
Abstract
A 12-year-old with a history of critical pulmonary stenosis and moderate right ventricular hypoplasia underwent neonatal pulmonary valve dilation, an aortopulmonary shunt, and an infant cavopulmonary anastomosis with aortopulmonary shunt takedown. During a diagnostic cardiac catheterization at 12 years of age, angiography showed interruption in the midportion of the coronary sinus, which required no intervention.
Introduction
Although coronary sinus abnormalities are rare, they usually result in no significant physiological consequences. Nevertheless, some require diagnostic imaging as they may complicate electrophysiological, surgical, or other interventional procedures. Coronary sinus atresia is a described anomaly, which results in discontinuity with the right atrium. We report a case of atresia of the midportion of the coronary sinus, resulting in coronary venous collateralization.
Case Report
A 12-year-old boy was born with critical pulmonary valvar stenosis and moderate right ventricular hypoplasia, He underwent balloon dilation of the pulmonary valve at one day of age, placement of a 3.5 mm aortopulmonary shunt at four weeks of age, and a cavopulmonary anastomosis with a takedown of the aortopulmonary shunt at six months of age. A diagnostic cardiac catheterization was performed at 12 years of age to assess potential candidacy for a transcatheter pulmonary valve. The right ventricular size appeared normal, and the tricuspid valve annulus Z-value was 0.6. There was no pulmonary stenosis. Pulmonary regurgitation was severe. Coronary angiography was performed to rule out significant coronary to right ventricular connections and to ensure suitability for transcatheter pulmonary valve placement. Right coronary angiography showed coronary venous drainage to the distal coronary sinus and then into the right atrium. Left coronary angiography revealed a venous return to two different portions of the coronary sinus. The majority drained into the proximal coronary sinus and then filled a left superior vena and the innominate vein, suggesting an abnormality of the coronary sinus. Selective angiograms in the left superior vena cava (Figures 1 and 2A) revealed atresia of the mid-portion of the coronary sinus with venous collateral flow from the proximal coronary sinus through the left superior vena cava and also through cardiac veins connecting into the distal coronary sinus and right atrium (Figure 2A and B). No intervention was undertaken.
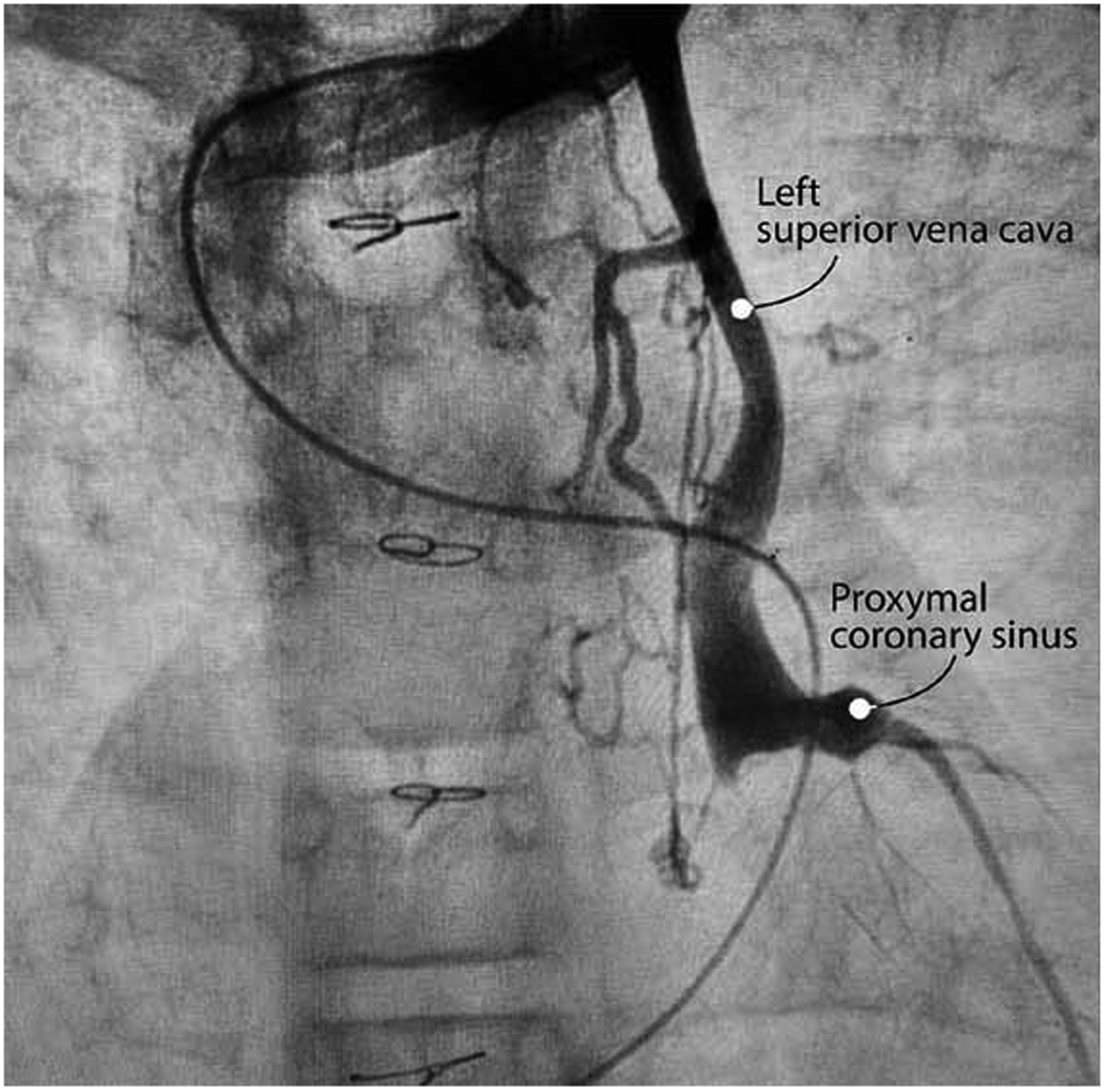
Left superior vena cava angiogram shows flow into the innominate vein. Contrast courses in retrograde fashion filling the proximal coronary sinus and a left ventricular cardiac vein.
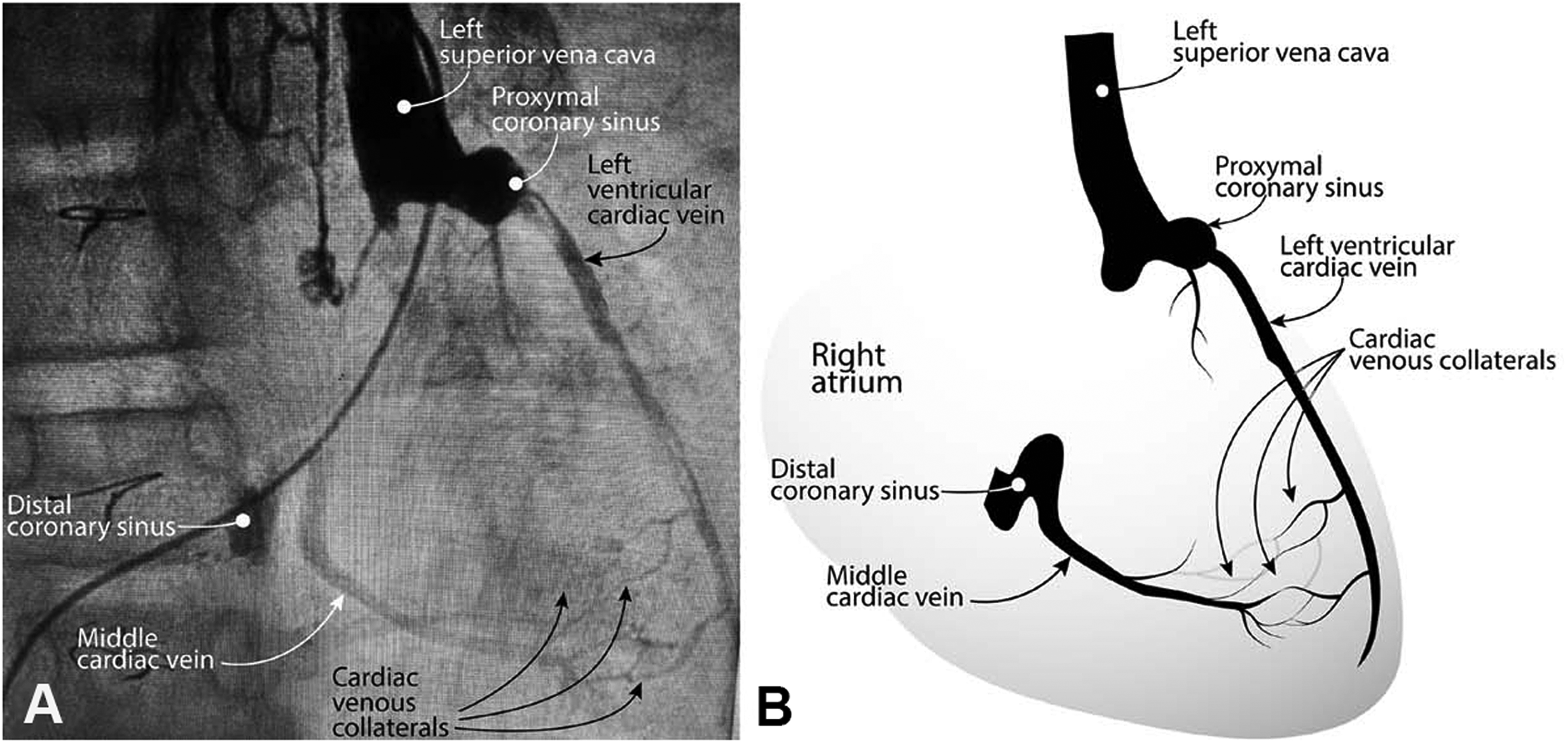
(A) Distal left superior vena cava angiogram demonstrates atresia of the coronary sinus between the proximal and distal coronary sinus. Contrast fills a left ventricular cardiac vein in retrograde fashion, with filling of cardiac venous collaterals that eventually connect with a middle cardiac vein, which in turn drains into the distal coronary sinus and right atrium. (B) Diagrammatic representation of pertinent cardiac venous anatomy.
Discussion
The coronary sinus runs along the left posteroinferior atrioventricular groove. It consists of a large vein and two valves: the Thebesian valve, which partially covers the ostium and the valve of Vieussens. 1 The veins that supply the coronary sinus are the oblique vein of the left atrium, additional left and right atrial veins, the great cardiac vein, the posterior vein to the left atrium, the left marginal vein, and the posterior interventricular vein. 2 The Thebesian valve is located in the right atrium at the orifice of the coronary sinus. 3 The valve of Vieussens is located at the junction of the great cardiac vein and the coronary sinus. 4 When the coronary sinus is stenotic or atretic, the following veins may drain the coronary venous return: left superior vena cava, Thebesian veins, innominate vein, and right-sided superior vena cava, all of which eventually drain into the right atrium. 5
Coronary sinus stenosis or atresia may occur at the distal end, in the middle or at the origin of the coronary sinus. Coronary sinus atresia implies a congenital origin; however, the lesion can also be acquired or iatrogenic. Other coronary sinus abnormalities include (a) absence of the coronary sinus, in which case blood flows directly into the left ventricle via Thebesian veins, 6 (b) unroofed coronary sinus in which there is a partial or complete absence of the roof of the coronary sinus, (c) coronary artery to coronary sinus fistula, (d) anomalous systemic or pulmonary venous return to the coronary sinus, and (e) coronary sinus diverticulum, in which there is a posteroseptal accessory atrioventricular connection consisting of a venous pouch within the left ventricular wall that has an opening to the coronary sinus. 7
It is important to recognize coronary sinus anatomy and abnormalities because an increasing number of procedures have been utilizing the coronary sinus. These include pacing of the left ventricle, mapping and ablation of arrhythmias, retrograde cardioplegia, mitral valve regurgitation interventional devices, targeted drug delivery, stem cell therapy, and resynchronization therapy. The course of the coronary sinus is often anomalous in patients with congenitally corrected transposition of the great arteries. 8
This case report describes atresia of the midportion of the coronary sinus. The proximal coronary sinus is drained by two pathways: the left superior vena cava and small cardiac venous collaterals connecting a left ventricular cardiac vein with a middle cardiac vein, eventually draining into the distal coronary sinus and right atrium. Persistence of the left superior vena cava in our patient is very suggestive of embryonic maldevelopment. However, the patient had a previous cardiac catheterization and two surgical procedures, which raises the possibility, albeit less likely, of thrombosis secondary to injury to the coronary sinus. The patient has had no symptoms or adverse consequence from this abnormality and has therefore required no treatment. He will continue to be watched closely.
This case highlights the need to be aware of and recognize coronary sinus abnormalities, particularly in patients that are candidates for electrophysiologic, surgical, or other therapeutic procedures.
Footnotes
Authors’ Note
The authors had full control of the study's design, methods used, outcome parameters, analysis of data, and production of the written report.
Acknowledgments
The authors thank Dr Ruben Acherman for creating the anatomic diagram.
Authors’ Statement
The patient's parents granted permission for publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.