
Abstract
Background
The management of total anomalous pulmonary venous connection (TAPVC) in neonates and infants is resource-intensive. We describe early and follow-up outcomes after surgical repair of isolated TAPVC at a single institution in a resource-limited setting.
Methods
The data of 316 consecutive patients with isolated TAPVC undergoing repair (January 2010-September 2020) were reviewed. The study setting was a tertiary hospital in southern India that provides subsidized or charitable care. Standard surgical technique was used for repair, circulatory arrest was avoided, and suture-less anastomosis was reserved for small or stenotic pulmonary veins. Surgical and postoperative strategies were directed toward minimizing intensive care unit (ICU) stay.
Results
302 (95.6%) patients were infants and 128 patients (40.5%) were neonates; median weight was 3.3 kg (IQR 2.8-4.0 kg). Obstruction of the TAPVC was seen in 176 patients (56%) and pulmonary hypertension in 278 patients (88%). Seventeen (5.4%) underwent delayed sternal closure. The median postoperative ICU stay was 120 h (IQR 96-192 h), mechanical ventilation was 45 h (IQR 24-82 h), and hospital stay was 13 days (IQR 9-17 days). There were three in-hospital deaths (0.9%). Over a median follow-up period of 53.3 months (IQR 22.9-90.4), pulmonary vein restenosis was seen in 32 patients (10.1%) after a mean of 2.2 months (1-6 months). No perioperative risk factors for restenosis were identified.
Conclusions
Using specific perioperative strategies, it is possible to correct TAPVC with excellent surgical outcomes in low-resource environments. Late pulmonary vein restenosis remains an important complication.
Keywords
Introduction
The management of neonates and young infants with total anomalous pulmonary venous connection (TAPVC) is a challenge. Mortality for the repair of isolated TAPVC has steadily decreased over time to under 5% in the current era.1,2 However, outcome data from low- and lower-middle income countries (LMIC) are scarce. 1 In low-resource settings, early and accurate diagnosis, availability of neonatal cardiac surgical care, prompt transfer to these facilities, and the quality of postoperative care can pose specific challenges because of limitations in health systems.3–5 Funds available for treatment may be limited, both at the individual and government level.6,7 Limitations in funds available for individual patients impose constraints in operative management and postoperative care that include limited access to extracorporeal membrane oxygenation (ECMO) and inhaled pulmonary vasodilator therapy. Additionally, the problems related to the patient population such as undernutrition, small for gestational age status, and neonatal sepsis in the perioperative period pose additional challenges.
Morbidity after surgery for isolated TAPVC includes arrhythmias, pulmonary hypertension, and residual pulmonary vein obstruction. Restenosis of pulmonary veins after a repair has been reported in 11% to 21% of cases1,2,8 and often requires reoperations. Lower weight at surgery and younger age has been described as risk factors for restenosis. 1 Yet again, information on mid-term data from LMICs on the incidence of restenosis is sparse, especially in the context of neonates and infants that are born with lower birth weight. 9
We describe the results of TAPVC repair at a single institution in southern India in consecutive neonates and infants over a 10-year period. The aim of this study was to describe early and follow-up outcomes after surgical repair of isolated TAPVC and identify the factors affecting the outcomes.
Methods
Design and Study Setting
The study is a retrospective cohort study conducted at a tertiary cardiac center in the state of Kerala in southern India. The pediatric heart program caters to a population of 34 million and seeks to provide care to all patients irrespective of their economic condition. An organized state-wide referral network was established in the region in 2018 and a well-developed system for neonatal transport was established in 2019. 6 Funds are made available for operations through a variety of sources that include contributions from charitable foundations, public insurance, and out-of-pocket expenditure, and they are often finite for individual patients. Because of the absence of trained pediatric intensivists, postoperative intensive care is jointly delivered by a team of three to four staff anesthesiologists supplemented by two to three trainees. For an annual surgical caseload of 600 to 700 cases, there are five staff pediatric cardiologists and three surgeons. Surgical trainees are shared between the adult and pediatric cardiac surgery services. Turnover of nursing staff is high, and the average nurse has a cumulative experience of under 12 months in pediatric postoperative care. Limitations in material resources included the absence of ECMO until 2015 and its relatively limited availability thereafter and limited availability of single-use items in cardiac surgery and intensive care.
Patient Data
All consecutive patients with a diagnosis of isolated TAPVC who underwent surgical repair from January 2010 through September 2020 were included in this study. A detailed review of these patients is available from the patient records and institutional surgical database that is maintained as a part of the International Quality Improvement Collaborative for Congenital Heart Disease (IQIC). 10 Since 2010, key preoperative, operative, and postoperative variables have been collected in the IQIC database with an annual audit to ensure accuracy. Prior permission to access the hospital database to analyze and publish these data were obtained from the Institutional Ethics committee. In view of the retrospective nature of the study, the need for informed consent was waived.
Patients were defined as “isolated” TAPVC if there were no associated cardiac anomalies that needed to be addressed (excluding patent ductus arteriosus and atrial septal defect).
A complete clinical assessment followed by standard diagnosis through echocardiography was done for every patient. Computed tomography (CT) for delineation of pulmonary veins was reserved for cases where echocardiography was deemed unsatisfactory.
Demographic variables collected included age at surgery, gender, anthropometric measurements, prematurity, and nutritional status. Weight <2.5 kg was taken as low birth weight (LBW) and prematurity was defined as gestational age < 37 weeks. Preoperative variables included type of venous connection, presence of obstruction or pulmonary artery hypertension (PAH), and preop stabilization. PAH was assessed by right ventricular systolic pressure (RVSP) measurement from the tricuspid regurgitation jet (TR). In absence of a reliable TR jet, the end-systolic septal position was used to obtain an estimate of RVSP. If the calculated pulmonary artery (PA) systolic pressures were above 60 mm Hg, the patient was defined as having PAH. Obstruction was defined as the presence of a continuous monophasic signal across the vertical vein or evidence of restriction of the patent foramen ovale in the form of turbulent flows from the right to left atrium. Preoperative stabilization included mechanical ventilation and identification and management of sepsis.
Operative variables included the duration of cardiopulmonary bypass and cross-clamp times. Operative findings that were noted included size of individual veins and location and extent of stenosis. The early outcomes included 30-day mortality, duration of mechanical ventilation, intensive care unit (ICU) stay, incidence of surgical site infection, and postoperative bloodstream infection. Late outcomes (>30 days) included pulmonary vein restenosis, reoperation, and late mortality.
Follow-up was at one month, three months, six months, and yearly thereafter. Any patient with follow-up records not available beyond 1-month post-procedure was deemed as lost to follow-up and censored.
Operative Strategies
Cardiopulmonary bypass (CPB) was instituted with minimal handling of the heart. Bicaval cannulae were used. Patients were cooled to 22 °C to 24 °C. The incision on the common pulmonary venous chamber was extended into individual pulmonary veins if they were stenotic or less than 2 mm in size, or if they did not have direct drainage into the common chamber. The anastomosis between the common chamber and LA was modified in certain situations to incorporate a partial sutureless technique or even opt for a complete primary sutureless technique. We used partial suture-less anastomosis over those segments of the pulmonary venous system which were stenotic or small in size and complete primary sutureless technique if the pulmonary veins and common confluence were diffusely small and/or fibrotic (Figure 1). In the coronary sinus (CS) type of TAPVC, coronary sinus cutback technique was used with the patient cooled to only 28 °C. However, if the common pulmonary venous chamber drained to CS via a restrictive opening, we divided this junction and closed the cardiac end. The common vein was then opened widely into the individual pulmonary veins and anastomosed to left atrium through a separate incision in left atrium. The ASD was closed with a large patch of the treated autologous pericardium. The vertical vein was ligated just before complete separation from CPB in all cases of supracardiac TAPVC. In infracardiac TAPVC, the vertical vein was left alone and not interrupted or divided.

Diagram of surgical repair of infracardiac type of total anomalous pulmonary venous connection showing technique of suturing. (A) Primary sutureless repair for small caliber veins. (B) Direct anastomosis between common pulmonary venous confluence and LA with switching over to incorporate primary sutureless repair over areas of stenosis/small individual veins. Ao, aorta; IVC, inferior vena cava; LA, left atrium; LIPV, left inferior pulmonary vein; LUPV, left upper pulmonary vein; PA, pulmonary artery; RA, right atrium; RLPV, right lower pulmonary vein; RPA, right pulmonary artery; RUPV, right upper pulmonary vein; RV, right ventricle; SVC, superior vena cava; VV, vertical vein.
We endeavored to primarily close the chest in all patients. Optimization before separation from CPB and MUF was important in this regard. Patients were fully rewarmed to 36 °C rectal temperature and arterial blood gas (ABG) was corrected. Modified ultrafiltration (MUF) was used in all patients for 10 to 15 min.
Postoperative Management
Standard monitoring included invasive arterial blood pressure, central venous pressure, continuous electrocardiography monitoring, pulse oximetry, and temperature. Insertion of transcutaneous pulmonary artery (PA) or left atrial lines was not a routine part of our practice. Stable preoperative patients with no pulmonary venous obstruction received dopamine at 2.5 to 5 µ/kg/min. Critically ill patients with pulmonary venous obstruction, PAH, and RV dysfunction were typically administered epinephrine and milrinone. Postoperative fluid administration was typically conservative and it was routine to use diuretic infusions in the first days after the procedure. In addition to continuous fentanyl infusions, the sickest strata of neonates such as those with preoperative obstruction or infracardiac phenotype also received adjunct neuromuscular blockade in the first few hours after surgery. Since 2016 we have supplemented fentanyl with dexmedetomidine infusions and introduced sedation-free periods closer to weaning from mechanical ventilation. Those with residual pulmonary hypertension or precarious preoperative presentation received additional measures such as physician-supervised endotracheal toilet or care, and sedation boluses to prevent pulmonary hypertension crisis triggered by stimulation. Readiness for extubation was assessed based on multipronged assessment ranging from acuity of presentation, pulmonary venous anatomy, bedside echocardiograms, and clinical assessment of the adequacy of gas exchange and hemodynamics. It was routine in our unit to transition neonates through a period of nasal continuous positive airway pressure or high-flow nasal cannula oxygen therapy post weaning and extubation of the trachea.
Data Analysis and Statistics
The outcomes in neonates were compared with infants and older children. They were also compared between those who had obstructed venous drainage at presentation versus those who did not. Comparisons were made to study the era effect, before and after 2018, when a statewide referral system was established by the government. Categorical variables are presented as number and percentage. Normally distributed continuous variables are presented as mean with standard deviation (SD). In situations where the continuous variables were skewed, we presented median and interquartile range (IQR). Pearson χ2 test or Fisher exact test was used to compare the categorical variables. Independent sample t test or Mann-Whitney test was used to compare the continuous variables.
The Cox-regression model was used to estimate proportional hazards of risk factors for restenosis. Kaplan-Meier analysis was used to estimate the survival functions of mortality and restenosis on follow-up. Statistical analyses were conducted using SPSS Version 20.0 for Windows (IBM Corporation).
Results
In the study period, 316 patients underwent isolated TAPVC repair. Baseline demographics and clinical variables are shown in Table 1. More than 95%of patients were infants and the median weight was 3.3 kg. Forty two patients weighed less than 2.5 kg at operation, and the smallest baby weighed 1.4 kg.
Baseline Clinical and Demographic Variables in 316 Patients With Total Anomalous Pulmonary Venous Connection (TAPVC).
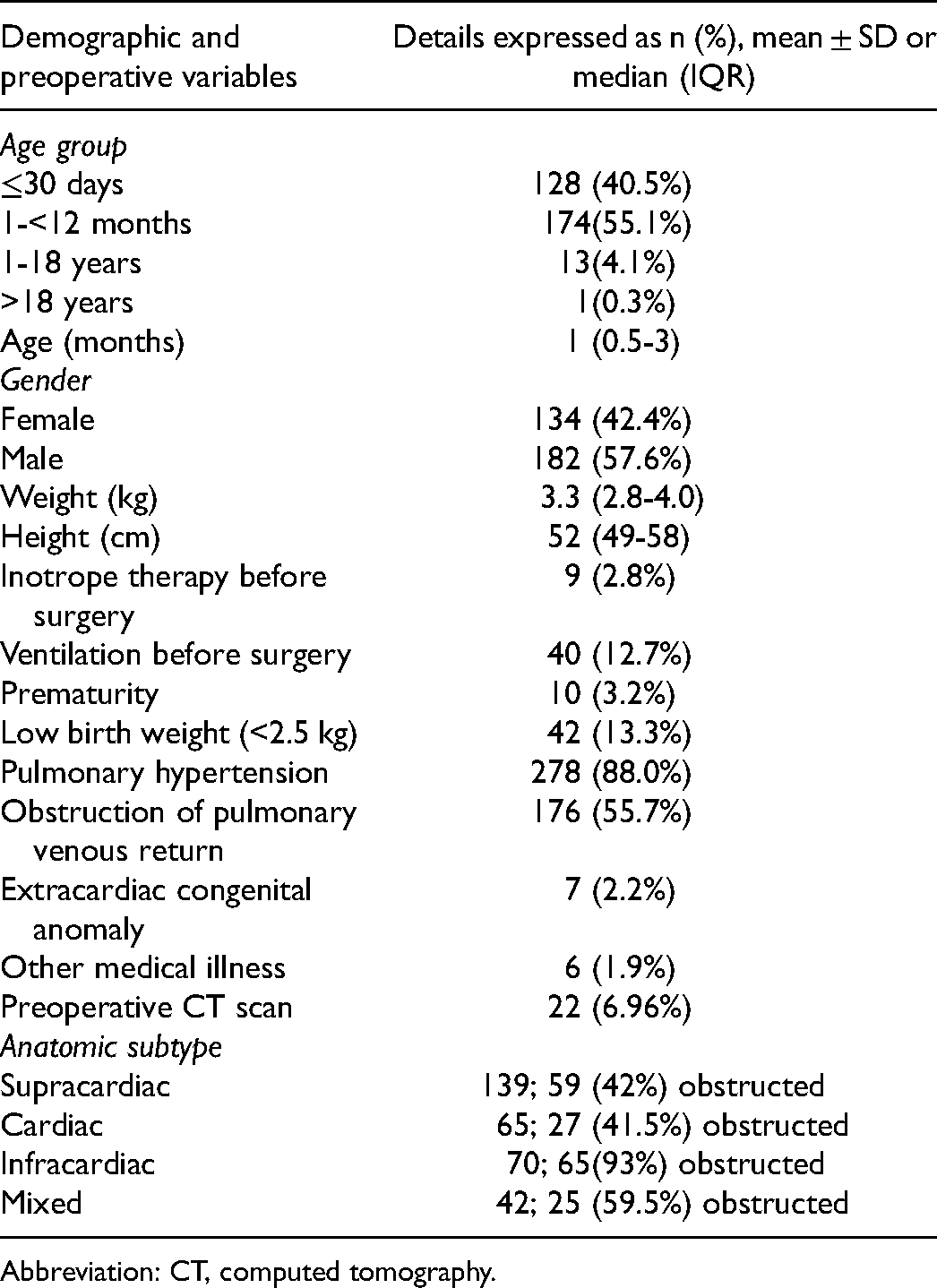
Abbreviation: CT, computed tomography.
Baseline pulmonary artery hypertension (PAH) as a result of obstruction or overcirculation was noted in 88% (n = 278). Five patients had extracardiac anomalies, namely cleft palate (1), developmental delay with hypotonia (1), left-side multiple ribs absent (1), preauricular tag (1), and VACTERL anomaly (1). The mean cardiopulmonary bypass time was 123.9 ± 58.9 min and the mean aortic cross-clamp time was 46.5 ± 26.6 min. There were no instances of total circulatory arrest.
The results of specific subgroup analyses have been summarized in Tables 2 to 4. Early postoperative results are shown in Table 2. The table also compares these outcomes between neonates and infants beyond 30 days of age (referred to as infants henceforth). The median postoperative ICU stay was 120 h (IQR 96-192 h), and the duration of mechanical ventilation was 45 h (IQR 24-82 h). Delayed sternal closure was needed in 17 (5.4%) patients. The hospital stay was 13 days (IQR 9-17 days). Bloodstream sepsis occurred in 9.2% (n = 29) and 11 (3.5%) had surgical site infection. There were three in-hospital deaths (0.9%). One neonate succumbed to refractory nephrotic syndrome. The other deaths were due to sepsis and pulmonary hypertensive crisis.
Early Postoperative Results in 316 Patients Operated for TAPVC.
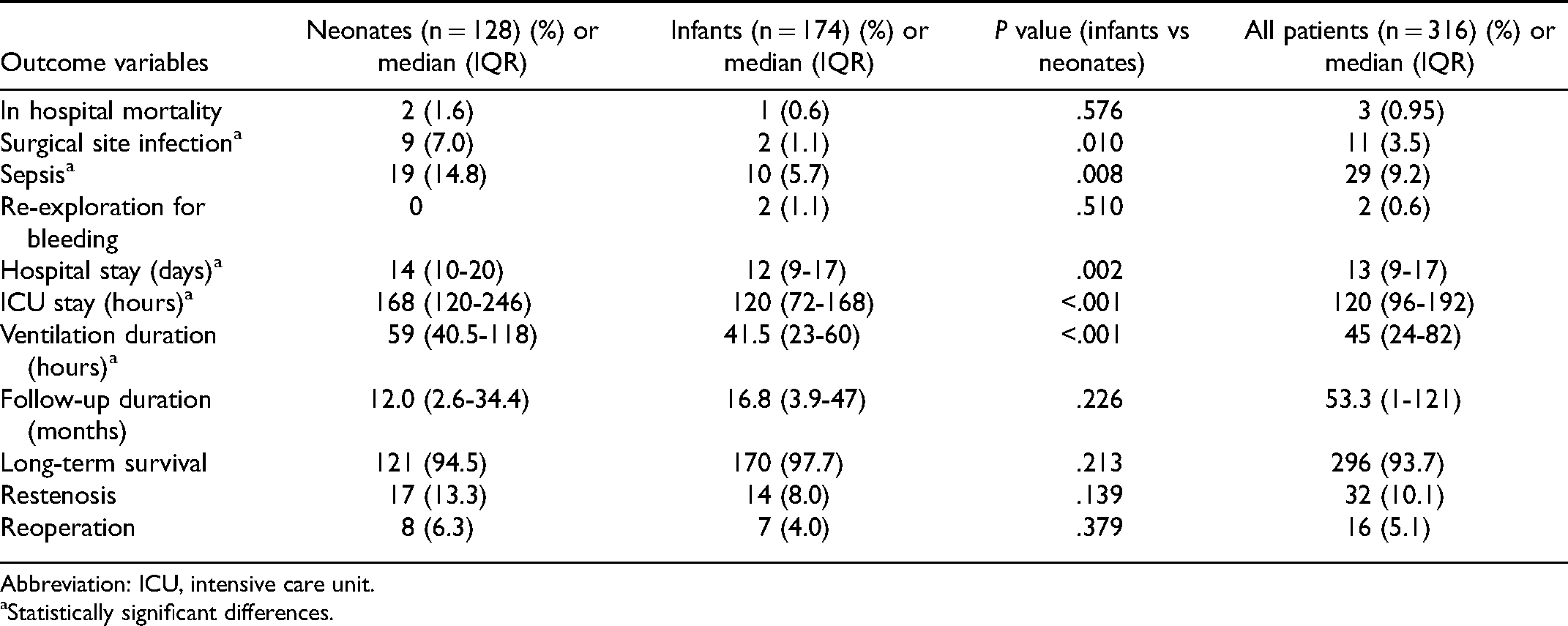
Abbreviation: ICU, intensive care unit.
Statistically significant differences.
Comparison Between Selected Pre- and Postoperative Variables in Patients With and Without Preoperative Obstruction.a
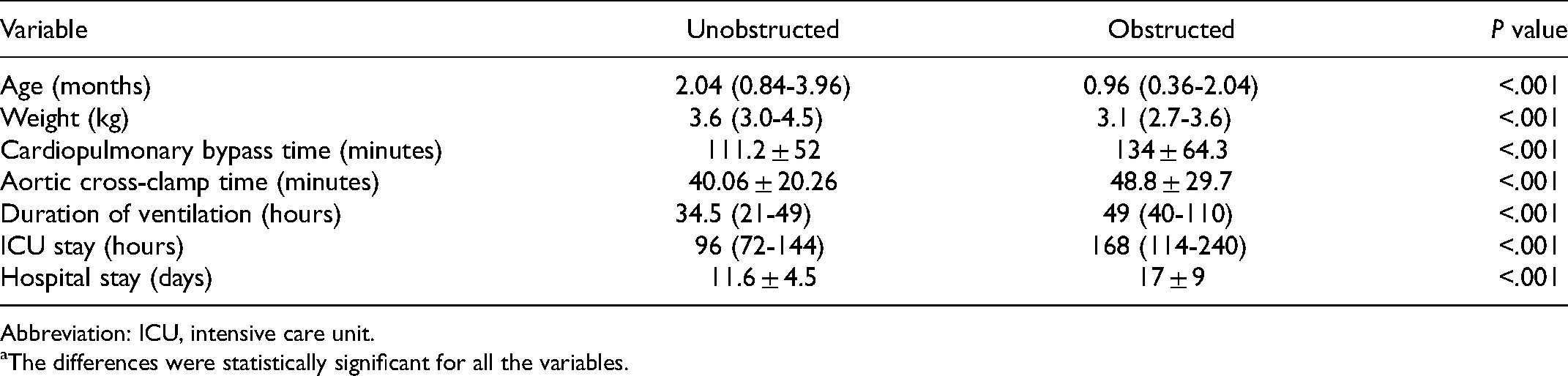
Abbreviation: ICU, intensive care unit.
The differences were statistically significant for all the variables.
Comparison Between Two Study Periods Before and After the Establishment of a Statewide Referral Network in 2018.
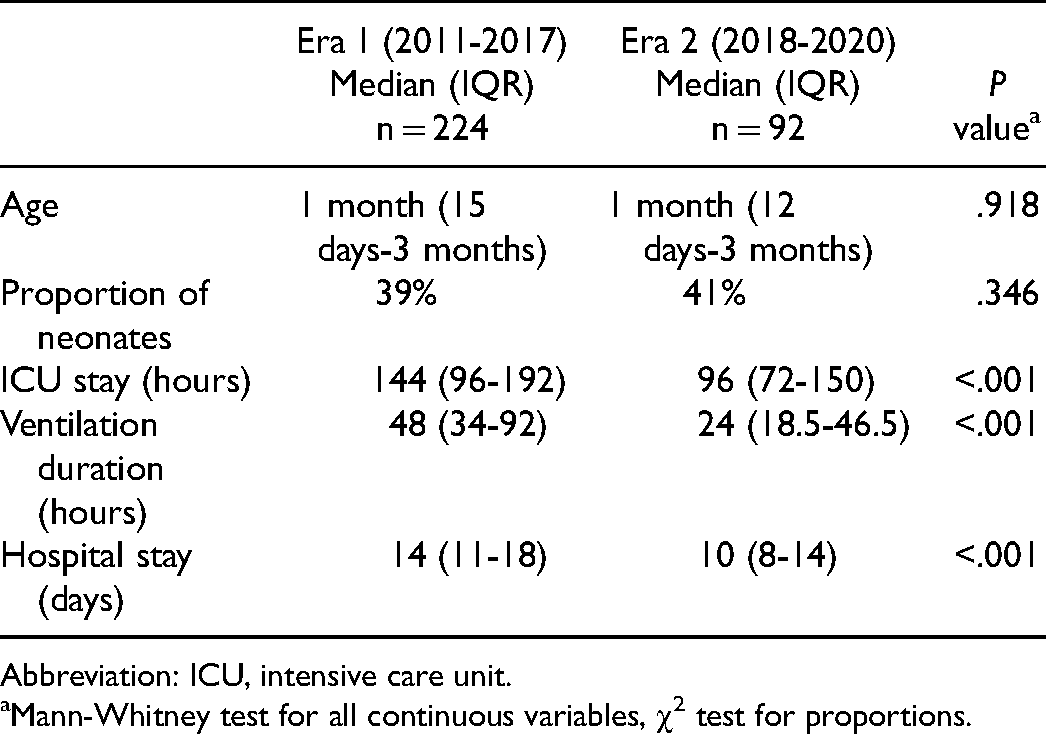
Abbreviation: ICU, intensive care unit.
Mann-Whitney test for all continuous variables, χ2 test for proportions.
Secondly, we sought to compare outcomes between obstructed and unobstructed TAPVC. Table 3 shows a comparison between those with preoperatively unobstructed versus obstructed pulmonary venous drainage. As would be expected the patients with obstructed drainage were younger, smaller, and required longer aortic cross-clamp (ACC) and CPB times and postoperative recovery times.
Lastly, we compared outcomes before and after 2018, when a state-wide referral network was established (Table 4). The referral pattern seemed similar, in that the age of children referred and the proportion of neonates was the same. However, it was found that immediate postoperative outcomes, namely ventilation hours and duration of ICU and hospital stay, were all significantly lower in the latter era.
Late Outcomes
Over a median follow-up period of 53.3 months (22.9-90.4), restenosis was seen in 32 patients (10.1%) at a mean of 2.2 months (range: 1-6 months) after surgery (Figures 2 and 3). The relative frequencies of restenosis were 5% for supracardiac, 12.3% for cardiac, 12.9% for infracardiac and 8% for mixed variants (P = .064).
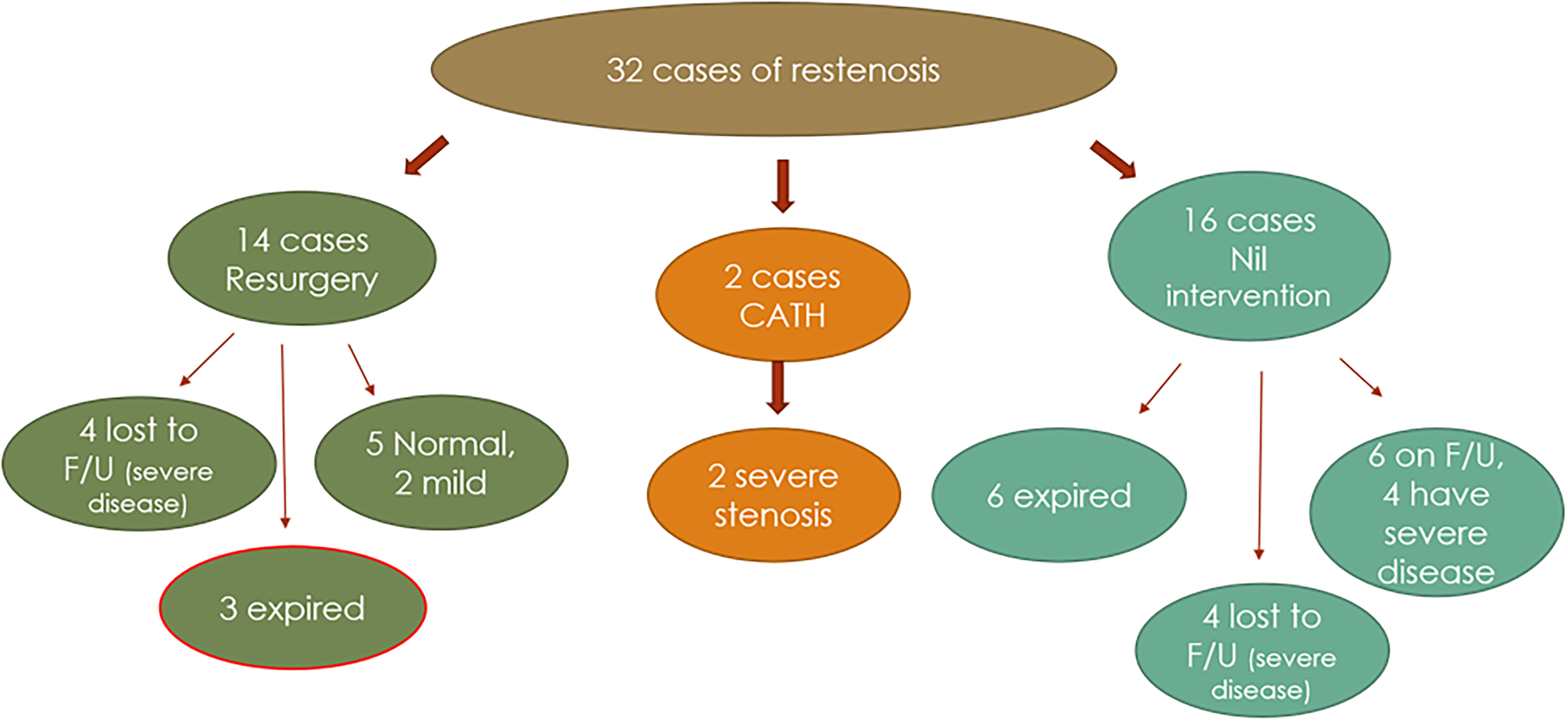
Outcomes in the 32 patients who had restenosis.
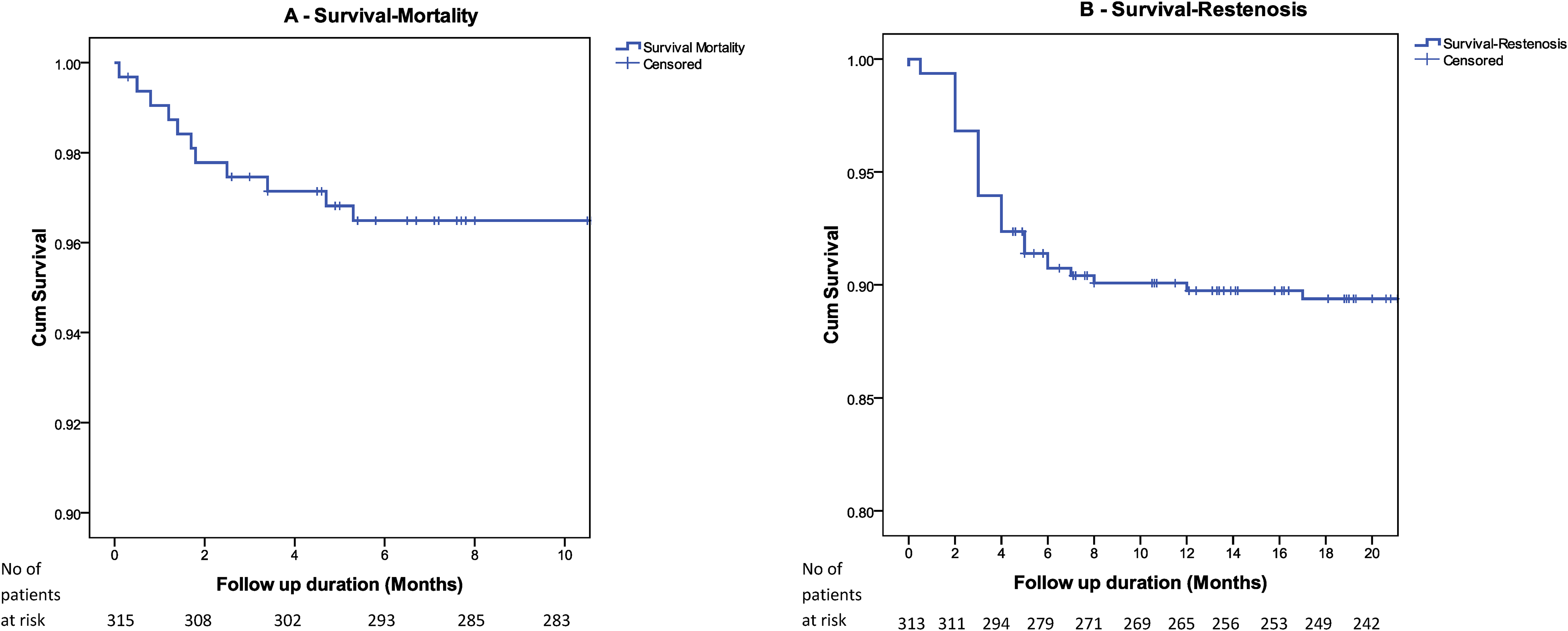
Survival (A) and restenosis (B) in 316 operated patients. Late mortality (>30 days post procedure) was documented in 2.8% (n = 9) patients. Restenosis free survival is 89.4%.
Of the 32 patients, one or more small individual pulmonary veins (<2 mm) were seen in eight patients during the operation, six were identified by preoperative imaging. The echocardiogram at the time of discharge after the operations was reported normal in 25 (69.4%) of these patients.
The cohort of 32 patients who had restenosis was further analyzed (Figure 2). Restenosis was deemed to be severe in 29 patients. Severe restenosis was defined as those with continuous monophasic Doppler signals with a mean gradient of >10 mm Hg; moderate restenosis 5 to 10 and mild as <5. Sixteen patients underwent reintervention; 14 patients underwent surgery, and two patients underwent catheter intervention. Successful reoperation was defined as unobstructed nonturbulent flows with complete resolution of pulmonary hypertension. Surgical re-repair was successful in seven of the total 14 patients, who were normal or had mild stenosis with no symptoms on follow-up. Two patients expired and five patients were lost to follow-up after the second surgery. Catheter interventions (balloon alone in one, stenting in one) were unsuccessful in relieving the obstruction in spite of multiple attempts, and both patients on follow-up were noted to have severe RV hypertension.
Of the 29 patients who had severe restenosis, those who had diffusely small pulmonary veins in CT scan were not offered surgery. Six of these children expired and four were lost to follow-up. A further three are on follow-up. One patient with mixed TAPVC had severe obstruction of the cardiac TAPVC (to CS) but normal drainage of the left upper pulmonary vein to LA anastomosis, was advised surgery, but lost to follow-up. Child was seen again after eight years and has a gradient of 22/8 at the common chamber-LA junction. One child with supracardiac TAPVC had small pulmonary veins on the left side and severe PAH and was advised surgery. Patient relatives refused surgery, but the child is on medical follow-up. Latest echo shows only mild turbulence at anastomotic site and small left-sided pulmonary veins. One patient was a cardiac TAPVC to CS, underwent CS cutback technique of repair. On follow-up, the child presented with severe PAH and CC-CS turbulence and small left-sided pulmonary veins and was followed-up medically. Latest echo shows moderate PAH and 12/6 mm Hg gradient across anastomotic site with LUPV anomalously draining into innominate vein.
In summary, of the 16 cases that were not intervened upon because of a poor anatomic substrate or mild disease, six patients expired and four patients, all having severe RV hypertension, were lost to follow-up. Of the remaining six patients on follow-up, four patients continued to have severe stenosis.
On univariable analysis, factors that had a statistically significant association with re-stenosis included lower weight at surgery and preoperative medical illness. On multivariable analysis, none of the variables were found to be significantly associated with restenosis. Patients who developed restenosis also had a longer duration of CPB and ACC times, hospital and ICU stay, and ventilation hours.
Discussion
Surgical repair of isolated TAPVC has been achieved with documented improvement in surgical outcomes with every passing decade.11–14 These outcomes are likely due to parallel improvements in the care continuum: surgical expertise, anesthestic practices, perfusion practices, and postoperative critical care. Surgical correction of TAPVC offers the prospect of a single corrective operation for a condition that is almost universally fatal. However, in low- and lower-middle income regions, provision of timely attention and achievement of consistently good outcomes may be a challenge.
Our report is, to our knowledge, one of the largest series of this condition reported from lower-middle income countries. It demonstrates the feasibility of excellent short-term outcomes and mid-term outcomes that are comparable with those achieved in better resource-endowed health systems from high-income countries. It seeks to extend the literature for lower resource settings in an effort to validate recent efforts to improve the health of children born with critical congenital heart disease.
The inherent limitations that exist from health system challenges and shortfalls in material and human resources were overcome through a variety of means. These included prudent use of preoperative imaging modalities such as CT and application of surgical strategies directed toward enabling early postoperative recovery. We also sought to tailor postoperative ICU management based on the preoperative condition and perceived risk. For example, neonates, those with obstructed forms of TAPVC, severe preoperative pulmonary hypertension, and right ventricular dysfunction were electively ventilated for longer periods of time. During the latter part of the study, (since 2018) we also sought to address the health system challenges in the region through the establishment of a regional network in partnership with the government and other pediatric heart programs in the region. Although there was no demonstrable decrease in the age of referral, there was a demonstrable improvement in outcomes after 2018 (Table 4). The postoperative duration of ventilation, ICU stay, and hospital stay was all significantly lower.
The incidence of postoperative restenosis in our series was 10.1%. Other series have reported this complication to occur at rates between 8% and 21%.1,2,8,14,15,16 The median time of presentation of restenosis was two months (1-6) after discharge replicating the timelines of another cohort. 15 Several factors have been found to be predictive of restenosis in isolated TAPVC. In a recent report (n = 768) from China, Shi et al 1 have found predictive factors to be preoperative pulmonary venous obstruction, mixed or infracardiac connections, and longer CPB time. Lower weight,14,16 younger age at operation, 16 mixed connection,8,13 preoperative hypoplastic pulmonary veins or absent confluence, 15 and postoperative PA crises 14 are the other factors found to have an association with restenosis. In our series, age at surgery was not associated with the risk of restenosis. The presence of preoperative medical illness and lower weight at surgery was the only significant associations found but none of these associations were detected to be independent predictors of stenosis. The overall long-term restenosis free survival was constant after the initial presentation of restenosis and was 89.4%, comparable to other studies.
Study Limitations
Our study has inherent limitations. It is retrospective and limited to a single center, where the practice has clearly evolved over time. We also acknowledge the possibility of a selection bias that may have prevented the sickest patients from reaching us. However, because of the health system challenges in the region, it is also possible that some of our patients may have actually been sicker on arrival because of delayed and suboptimal transport. Since 2018, universal neonatal screening has been introduced in the region. The age at referral and proportion of newborns has not changed since 2018 (Table 4). This argues against the possibility of a selection bias.
Conclusion
Our study demonstrated the feasibility of correcting TAPVC with excellent early surgical outcomes in low-resource environments with inherent challenges using specific perioperative strategies in a large retrospective cohort. We were unable to identify specific factors that were associated with restenosis that remains an important late complication in a significant percentage of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.