
Abstract
This manuscript will provide information about hypoplastic left heart syndrome (HLHS) and related malformations, including definitions, morphology, and classification, based on the 2021 International Paediatric and Congenital Cardiac Code (IPCCC) and the Eleventh Revision of the International Classification of Diseases (ICD-11). HLHS is defined as “a spectrum of congenital cardiovascular malformations with normally aligned great arteries without a common atrioventricular junction, characterized by underdevelopment of the left heart with significant hypoplasia of the left ventricle including atresia, stenosis, or hypoplasia of the aortic or mitral valve, or both valves, and hypoplasia of the ascending aorta and aortic arch.” Functionally univentricular heart is defined as “a spectrum of congenital cardiac malformations in which the ventricular mass may not readily lend itself to partitioning that commits one ventricular pump to the systemic circulation, and another to the pulmonary circulation.” The Norwood operation is synonymous with the term “Norwood (Stage 1)” and is defined as (1) creation of an aortopulmonary connection and neoaortic arch construction resulting in univentricular physiology and (2) creation of a controlled source of pulmonary blood flow with a calibrated systemic-to-pulmonary artery shunt, a right ventricle to pulmonary artery conduit, or rarely, a cavopulmonary connection. The goals of the Norwood (Stage 1) Operation are creation of (1) unobstructed systemic blood flow via aortopulmonary connection and neoaortic arch construction, (2) unobstructed coronary blood flow, (3) unobstructed flow across the atrial septum, and (4) controlled pulmonary blood flow.
Keywords
Definitions
The 2021 International Paediatric and Congenital Cardiac Code (IPCCC) and the Eleventh Revision of the International Classification of Diseases (ICD-11) provide the following definition for hypoplastic left heart syndrome (HLHS):
Hypoplastic left heart syndrome (HLHS) is defined as “a spectrum of congenital cardiovascular malformations with normally aligned great arteries without a common atrioventricular junction, characterized by underdevelopment of the left heart with significant hypoplasia of the left ventricle including atresia, stenosis, or hypoplasia of the aortic or mitral valve, or both valves, and hypoplasia of the ascending aorta and aortic arch.”1–4 Functionally univentricular heart is defined as “a spectrum of congenital cardiac malformations in which the ventricular mass may not readily lend itself to partitioning that commits one ventricular pump to the systemic circulation, and another to the pulmonary circulation.”1,2,3,5 Atrioventricular septal defect with ventricular imbalance with dominant right ventricle and hypoplastic left ventricle Tricuspid atresia with transposition of the great arteries (TGA) Double inlet left ventricle with transposition of the great arteries (DILV + TGA) “Atrioventricular septal defect with ventricular imbalance with dominant right ventricle and hypoplastic left ventricle” is defined as “a congenital cardiac malformation that is a variant of an atrioventricular septal defect (atrioventricular canal defect) with the right ventricle significantly larger than the left.”1–3 Tricuspid atresia is defined as “a congenital cardiovascular malformation with absence of the tricuspid valvar annulus (connection/junction) or an imperforate tricuspid valve.”1–3 Transposition of the great arteries is defined as “a congenital cardiovascular malformation in which the morphologically right ventricle connects to the aorta and the morphologically left ventricle connects to the pulmonary trunk.”1–3 Double inlet atrioventricular connection is defined as “a congenital cardiovascular malformation with a univentricular atrioventricular connection wherein both atria connect to one ventricle either via 2 separate atrioventricular valves or a common atrioventricular valve, such that all or nearly all of the total atrioventricular junctional (annular) area is committed to one ventricular chamber.”1–3 Double inlet left ventricle is defined as “a congenital cardiovascular malformation with a univentricular atrioventricular connection wherein both atria connect to a morphologically left ventricle either via 2 separate atrioventricular valves or a common atrioventricular valve, such that all or nearly all of the total atrioventricular junctional (annular) area is committed to the left ventricular chamber.”1–3 The Norwood operation is synonymous with the term “Norwood (Stage 1)” and is defined as (1) creation of an aortopulmonary connection and neoaortic arch construction resulting in univentricular physiology and (2) creation of a controlled source of pulmonary blood flow with a calibrated systemic-to-pulmonary artery shunt, a right ventricle to pulmonary artery conduit, or rarely, a cavopulmonary connection. The goals of the Norwood (Stage 1) Operation are creation of (1) unobstructed systemic blood flow via aortopulmonary connection and neoaortic arch construction, (2) unobstructed coronary blood flow, (3) unobstructed flow across the atrial septum, and (4) controlled pulmonary blood flow. use of homograft patch to reconstruct the aortic arch and the opened ascending aorta, and bring them over the divided proximal pulmonary trunk,7,8 use of complete tube from the proximal pulmonary trunk to the aortic arch,
7
techniques of direct reconstruction of the aortic arch and ascending aorta without prosthetic material,9–11 and direct anastomosis between the proximal pulmonary trunk and the aortic arch, augmented distally with a small homograft patch.
4
HLHS is a form of “functionally univentricular heart.” IPCCC and ICD-11 provide the following definition for functionally univentricular heart:
Many patients with functionally univentricular circulation are born with ductal-dependent systemic circulation or ductal-dependent pulmonary circulation, and these patients typically require surgical or transcatheter palliation in the neonatal period. Although the most common form of functionally univentricular heart with ductal-dependent systemic circulation is HLHS, neonates with several other forms of functionally univentricular hearts also have ductal-dependent systemic circulation, including some variations of the following congenital cardiac malformations:
Because some variations of these three congenital cardiac malformations are treated with the same treatment strategies as HLHS, the definitions from IPCCC and ICD-11 for these physiologically equivalent “HLHS-related malformations”1–5 are therefore also provided below:
Finally, the most common initial palliation for neonates with functionally univentricular heart with ductal-dependent systemic circulation is the Norwood (Stage 1) Operation. The following definition of the Norwood (Stage 1) Operation is used by most international registries and databases:
The first patient with HLHS successfully to undergo and survive the Fontan-type operation was reported by Norwood and colleagues in 1983.
6
This landmark publication finally offered hope for those born with this previously lethal cardiac malformation.
4
Since the early 1980s, there have been several modifications to Norwood's initial operation, including the following
4
:
The idea of placing a conduit from the right ventricle to the pulmonary artery during the first stage of palliation dates back to the earlier work of Norwood, who used valved Hancock and non-valved polytetrafluoroethylene 12 millimeter conduits.9,12,13 The fact that these early right ventricle to pulmonary artery conduits had a diameter of 12 millimeters was probably the cause of the negative outcome for this initial experience, and the technique was abandoned for years,4,12 with most surgeons using a systemic-to-pulmonary artery shunt as the source of pulmonary blood flow during the 1980s and 1990s. In 1993
14
and again in 1999,
15
the Japanese surgeon Kishimoto described performing the Norwood operation with a conduit placed from the right ventricle to the pulmonary artery. In fact, in 1999 and 2001, a few reports, mostly from Japanese cardiac surgical centers (Kishimoto, 1999,
15
Imoto, 2001,
16
and Sano, 2001
17
) revisited the use of conduits placed from the right ventricle to the pulmonary artery, either a xenopericardial conduit containing a bicuspid valve 6 millimeters in diameter,
15
or polytetrafluoroethylene tubes of 4, 5, and 6 millimeters in diameter.16,17 In 2003, Malec and colleagues also reported favorable experiences with the Norwood (Stage 1) Operation with a conduit placed from the right ventricle to the pulmonary artery.
12
Despite these earlier experiences, it is Sano who is usually credited for the spread in popularity of the use of the right ventricle to pulmonary artery conduit during the Norwood operation,
4
and this technique is frequently described in Europe and North America as the Sano modification.17,18
Morphology
Figures 1, 2, and 3 provide examples of the morphology of HLHS.
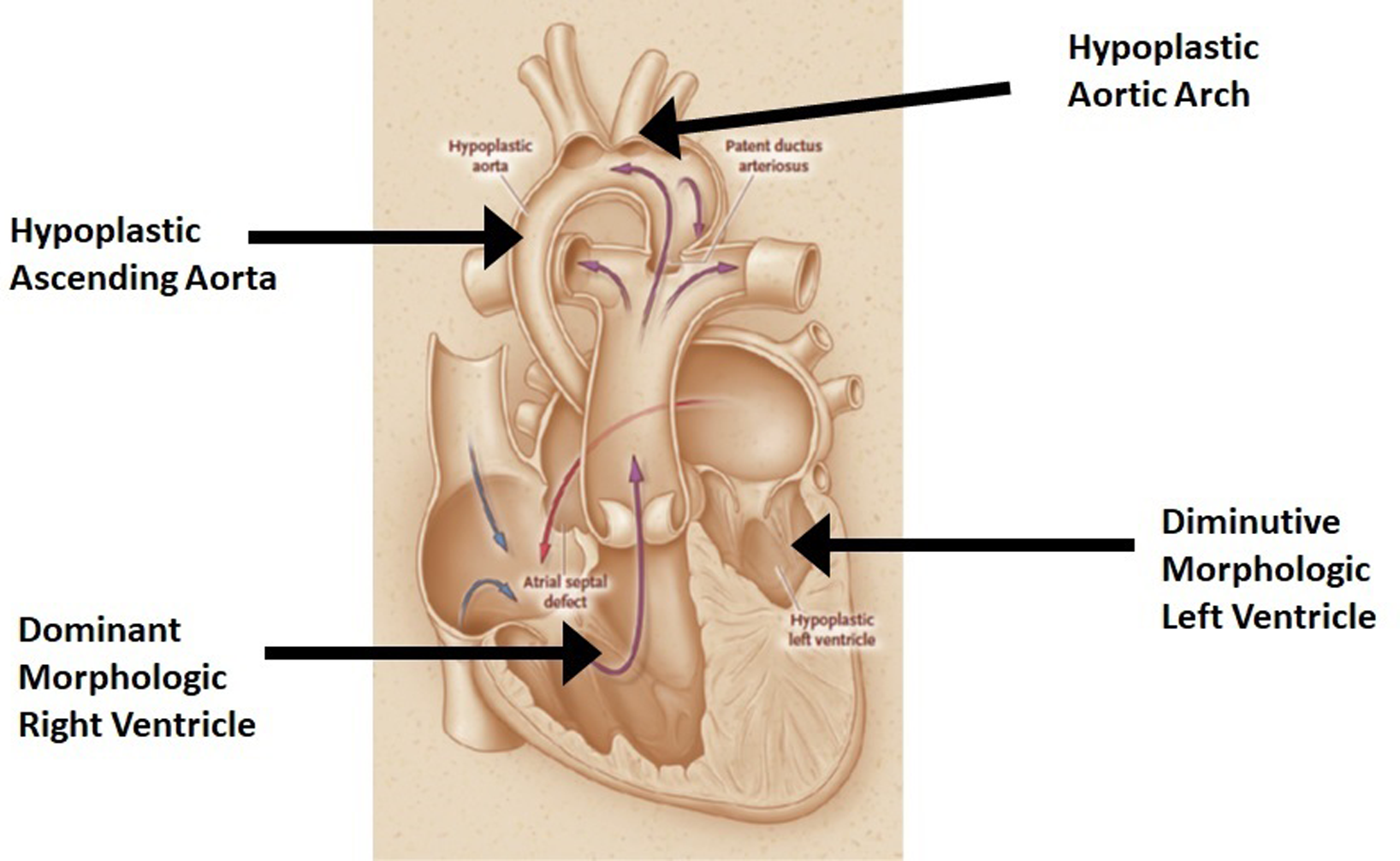
The common morphology of a typical heart with HLHS. 19 This figure is reproduced with permission of The New England Journal of Medicine. The left ventricle is severely hypoplastic. The ascending aorta is diminutive, often only 1 millimeter to 3 millimeters in size. (It is notable that in an analysis of 549 infants with a diagnosis of HLHS or a related single morphologic right ventricular anomaly and a planned Norwood procedure, the size of the ascending aorta [mean + /− standard deviation] was reported as 4 + /− 2 millimeters. 19 While the size of the ascending aorta is often only 1 to 3 millimeters in patients with HLHS and aortic atresia, the size of the ascending aorta is more than 3 millimeters in most patients with HLHS and aortic stenosis.) The aortic arch is small, with associated coarctation of the aorta, and the right ventricle is the only functional ventricle.
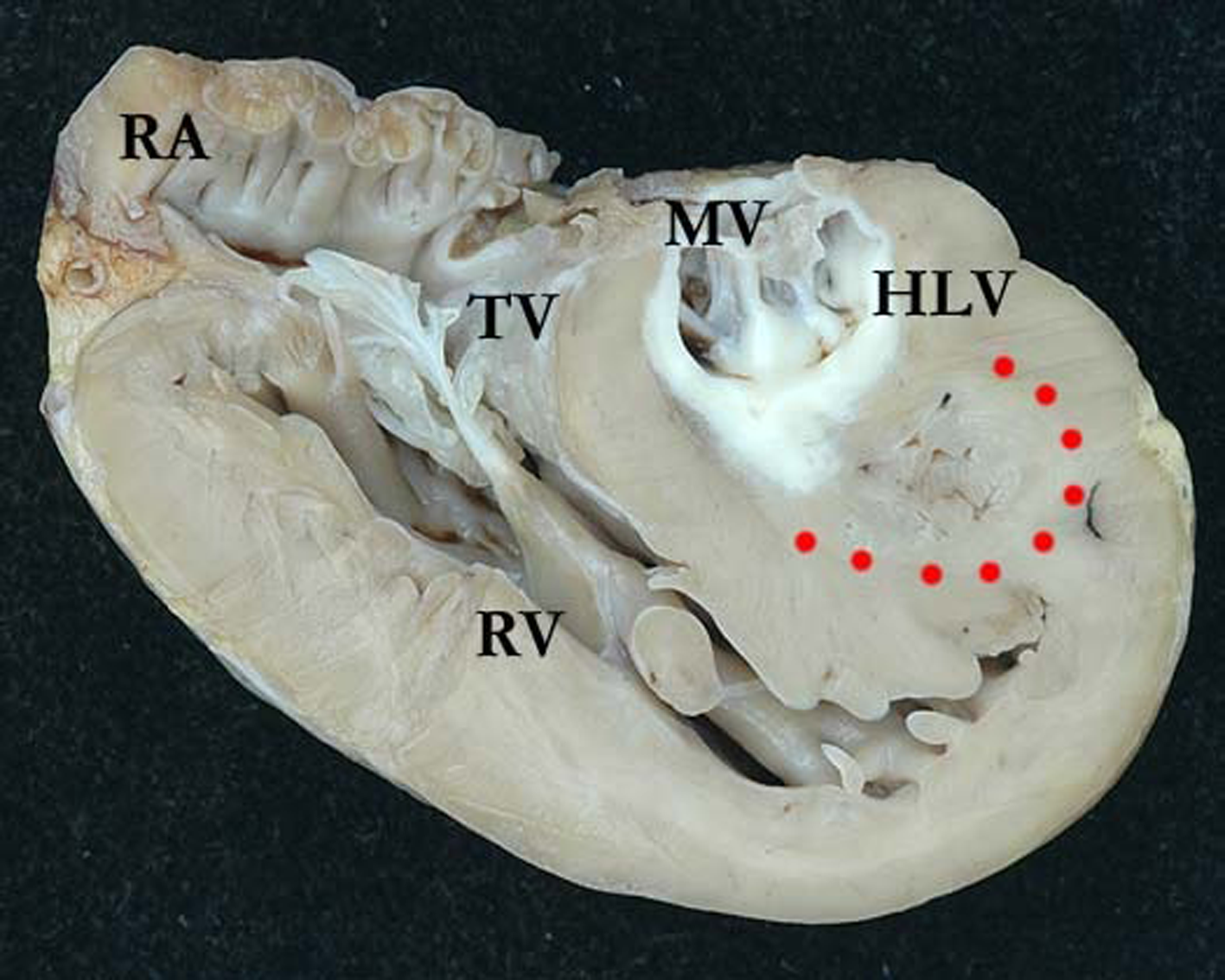
An anatomic specimen from the Van Mierop Archive at University of Florida, Gainesville, FL, USA, reproduced with permission of The International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD) [https://ipccc.net/awg/HLHS/HLHS_AA_MS_01_01_09/HLHS_AA_MS_01_01_09.html], accessed November 28, 2021. This photograph documents a 4-chamber view, viewed from the front of this heart that was removed when the patient underwent cardiac transplantation and shows a hypoplastic, fibroelastotic left ventricle (HLV). The apical portion of this globular left ventricle demonstrates remnants of the trabecular component, which are an unusual feature in HLHS (red dots). The mitral valve (MV) is severely stenotic, with short, fused tendinous cords. There is right ventricular hypertrophy and the right ventricle (RV) forms the apex of the heart. This image also illustrates endocardial fibroelastosis. (TV, tricuspid valve; RA, right atrium). (See full color image in online version).
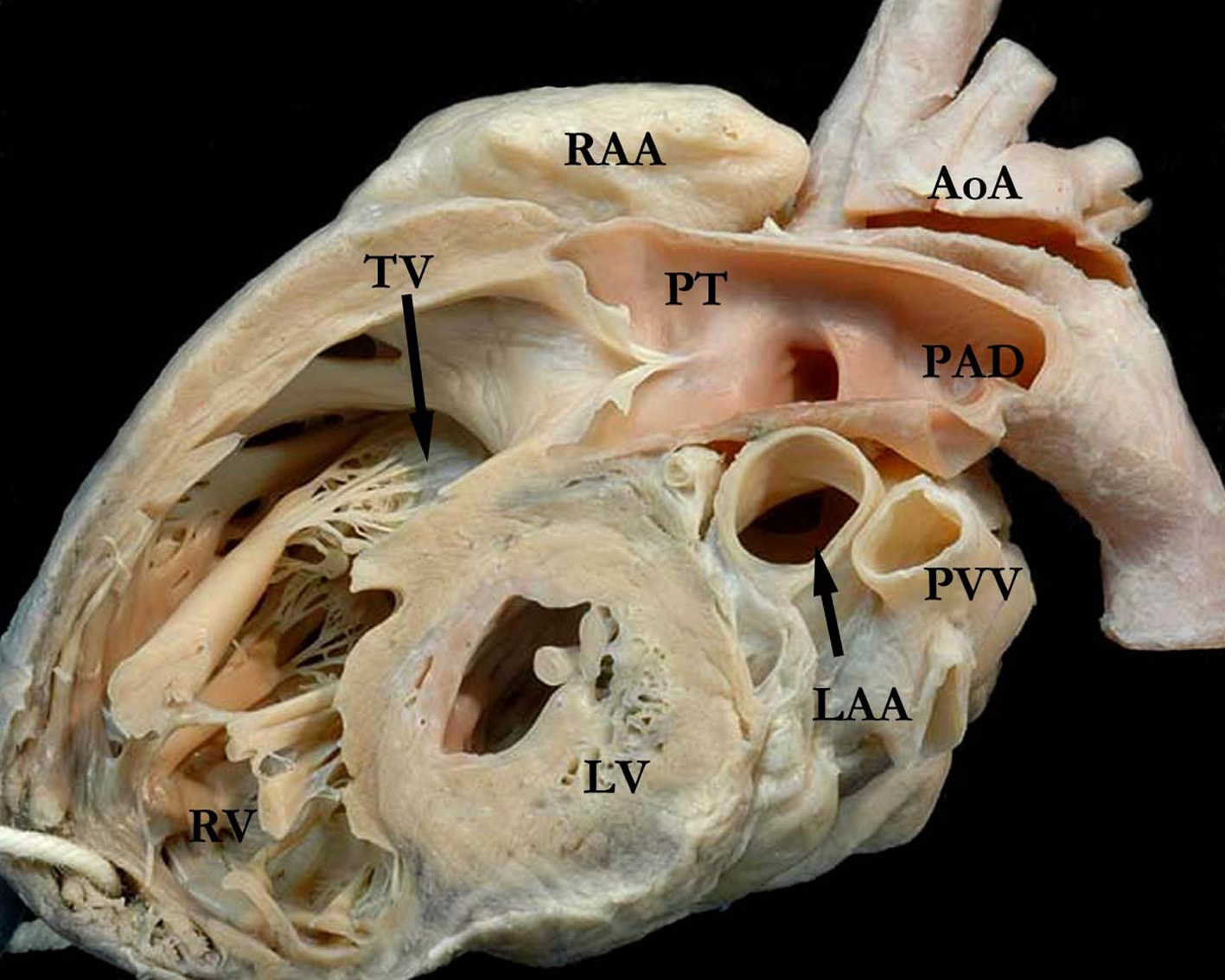
An anatomic specimen from the Van Mierop Archive at University of Florida, Gainesville, FL, USA, reproduced with permission of The International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD) [https://ipccc.net/awg/HLHS/HLHS_AA_MS_01_01_09/HLHS_AA_MS_01_01_09.html], accessed November 28, 2021. This photograph documents a simulated right ventricular long axis echocardiographic view, cut from a different heart, and illustrates a globular, hypoplastic left ventricle (LV). The right ventricle (RV) forms the apex of this heart, with the tricuspid valve (TV) in the inlet portion and a large pulmonary trunk (PT) forming the outlet component. The arterial duct is widely patent (PAD). The ascending aorta and aortic arch (AoA) are hypoplastic. Although not easily seen in this image, this left ventricle did have fibroelastotic changes. (RAA, right atrial appendage; LAA, left atrial appendage; PVV, pulmonary vein).
Figure 1 provides an illustration of the common morphology of a typical heart with HLHS.
19
As shown in Figure 1:
The left ventricle is severely hypoplastic. The ascending aorta is diminutive, often only 1 millimeter to 3 millimeters in size. It is notable that in an analysis of 549 infants with a diagnosis of HLHS or a related single morphologic right ventricular anomaly and a planned Norwood procedure, the size of the ascending aorta (mean + /− standard deviation) was reported as 4 + /− 2 millimeters.
19
While the size of the ascending aorta is often only 1 to 3 millimeters in patients with HLHS and aortic atresia, the size of the ascending aorta is more than 3 millimeters in most patients with HLHS and aortic stenosis. The aortic arch is small, with associated coarctation of the aorta. The right ventricle is the only functional ventricle.
Figure 2 is an anatomic specimen from the Van Mierop Archive at University of Florida, Gainesville, FL, USA, reproduced with permission of The International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD) [https://ipccc.net/awg/HLHS/HLHS_AA_MS_01_01_09/HLHS_AA_MS_01_01_09.html], accessed November 28, 2021. This photograph documents a 4-chamber view, viewed from the front of this heart that was removed when the patient underwent cardiac transplantation, and shows a hypoplastic, fibroelastotic left ventricle (HLV). The apical portion of this globular left ventricle demonstrates remnants of the trabecular component, which are an unusual feature in HLHS (red dots). The mitral valve (MV) is severely stenotic, with short, fused tendinous cords. There is right ventricular hypertrophy and the right ventricle (RV) forms the apex of the heart. This image also illustrates endocardial fibroelastosis (TV, tricuspid valve; RA, right atrium).
Figure 3 is also an anatomic specimen from the Van Mierop Archive at University of Florida, Gainesville, FL, USA, reproduced with permission of The International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD) [https://ipccc.net/awg/HLHS/HLHS_AA_MS_01_01_09/HLHS_AA_MS_01_01_09.html], accessed November 28, 2021. This photograph documents a simulated right ventricular long axis echocardiographic view, cut from a different heart, and illustrates a globular, hypoplastic left ventricle (LV). The right ventricle (RV) forms the apex of this heart, with the tricuspid valve (TV) in the inlet portion and a large pulmonary trunk (PT) forming the outlet component. The arterial duct is widely patent (PAD). The ascending aorta and aortic arch (AoA) are hypoplastic. Although not easily seen in this image, this left ventricle did have fibroelastotic changes (RAA, right atrial appendage; LAA, left atrial appendage; PVV, pulmonary vein).
Classification
HLHS may be subclassified into the following 5 subtypes:
Hypoplastic left heart syndrome (HLHS), Aortic atresia + Mitral atresia Hypoplastic left heart syndrome (HLHS), Aortic atresia + Mitral stenosis Hypoplastic left heart syndrome (HLHS), Aortic stenosis + Mitral atresia Hypoplastic left heart syndrome (HLHS), Aortic stenosis + Mitral stenosis Hypoplastic left heart syndrome (HLHS), Without intrinsic valvar stenosis or atresia (Hypoplastic aortic valve + mitral valve + left ventricle) = Hypoplastic left heart complex = HLHC “Atresia” is defined as the congenital absence or closure of a normal body orifice or tubular organ. It is derived from the Greek and Latin bases, where “a” means without, and “tresis” is the word for perforation. Thus, aortic valvar atresia can be defined as either absence or closure of the orifice of the aortic root. “Stenosis” is narrowing or stricture of a duct or a canal. Aortic stenosis, for example, is a broad term encompassing the supravalvar, valvar, or subvalvar variants. More specifically, aortic valvar stenosis is a narrowing of the orifice of the aortic valve due to fusion of the zones of apposition between the leaflets, or the inability of the valve to open adequately because of thickening or calcification of the leaflets, causing obstruction to the flow of blood. “Hypoplasia” is the incomplete development or underdevelopment of an organ or tissue. For example, a hypoplastic aortic valve can cause obstruction to the flow of blood simply because of its inadequate size. “Obstruction” is the act of blocking or clogging, or the state or condition of being blocked or clogged. Obstruction to the flow of blood, therefore, may be caused by atresia, stenosis, or hypoplasia of a given structure. “Hypoplastic left heart syndrome without intrinsic valvar stenosis or atresia is synonymous with the term hypoplastic left heart complex (HLHC) and is defined as a cardiac malformation at the milder end of the spectrum of hypoplastic left heart syndrome with normally aligned great arteries without a common atrioventricular junction, characterized by underdevelopment of the left heart with significant hypoplasia of the left ventricle and hypoplasia of the aortic or mitral valve, or both valves, in the absence of intrinsic valvar stenosis or atresia, and with hypoplasia of the ascending aorta and aortic arch.”
4
The following previously published definitions
4
are critical to understanding and applying this system of classification:
It is particularly important to differentiate the meaning of the terms “stenosis” and “hypoplasia.”
4
Although atresia and stenosis are mutually exclusive terms, hypoplasia may be present with atresia or stenosis, or can exist in isolation. Hypoplasia simply implies that the organ or tissue is less than its normal size.
4
Through the application of the above definitions, one may accurately describe the morphology and classify all hearts that exist in the spectrum of congenital cardiovascular malformations known as HLHS.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.