
Abstract
A 13-month-old male sustained cardiac arrest under general anesthesia and was found to have left main coronary artery atresia with collateralization from the right coronary artery. After protracted recovery, the patient underwent coronary ostioplasty. Postoperative imaging confirmed patency of the newly established artery without stenosis. At 12 months, no changes in the vessel were noted. Ventricular function remains mildly decreased and stable.
Introduction
Left main coronary artery (LMCA) atresia is a rare anomaly in which the left main coronary ostium is absent, and the left anterior descending (LAD) and circumflex (Cx) arteries end blindly. We report a case of a 2.8-year-old male who at 13 months sustained sudden cardiac arrest while under general anesthesia and was found to have LMCA atresia. Antegrade coronary flow was reconstituted via coronary reconstruction and ostioplasty.
Case Report
The patient presented to our institution at 13.5 months of age for elective tear duct dilation. Under general anesthesia, the patient sustained sudden cardiac arrest and was placed on extracorporeal membrane oxygenation (ECMO) support. Cardiac catheterization revealed LMCA atresia with filling through poorly developed RCA collaterals (Figure 1). The patient experienced cerebral edema with evidence of herniation secondary to the original hypoxic–ischemic event. After expedient weaning from ECMO, he underwent emergent decompressing craniotomy with external ventricular shunt placement; this was converted to a ventriculoperitoneal shunt 1 month later. The patient remained hemodynamically stable and was started on a regimen of carvedilol, furosemide, and spironolactone, upon which his heart function improved to mild-to-moderate left ventricular (LV) dysfunction with moderate mitral regurgitation. His prolonged hospitalization was related to his neurologic injury and craniectomy. He was discharged home approximately 2 months post-event with significant seizures, jerking movements, and severe left-sided neurologic deficits leaving his neurological prognosis unclear. He underwent delayed cranial reconstruction 6 months after the initial event.
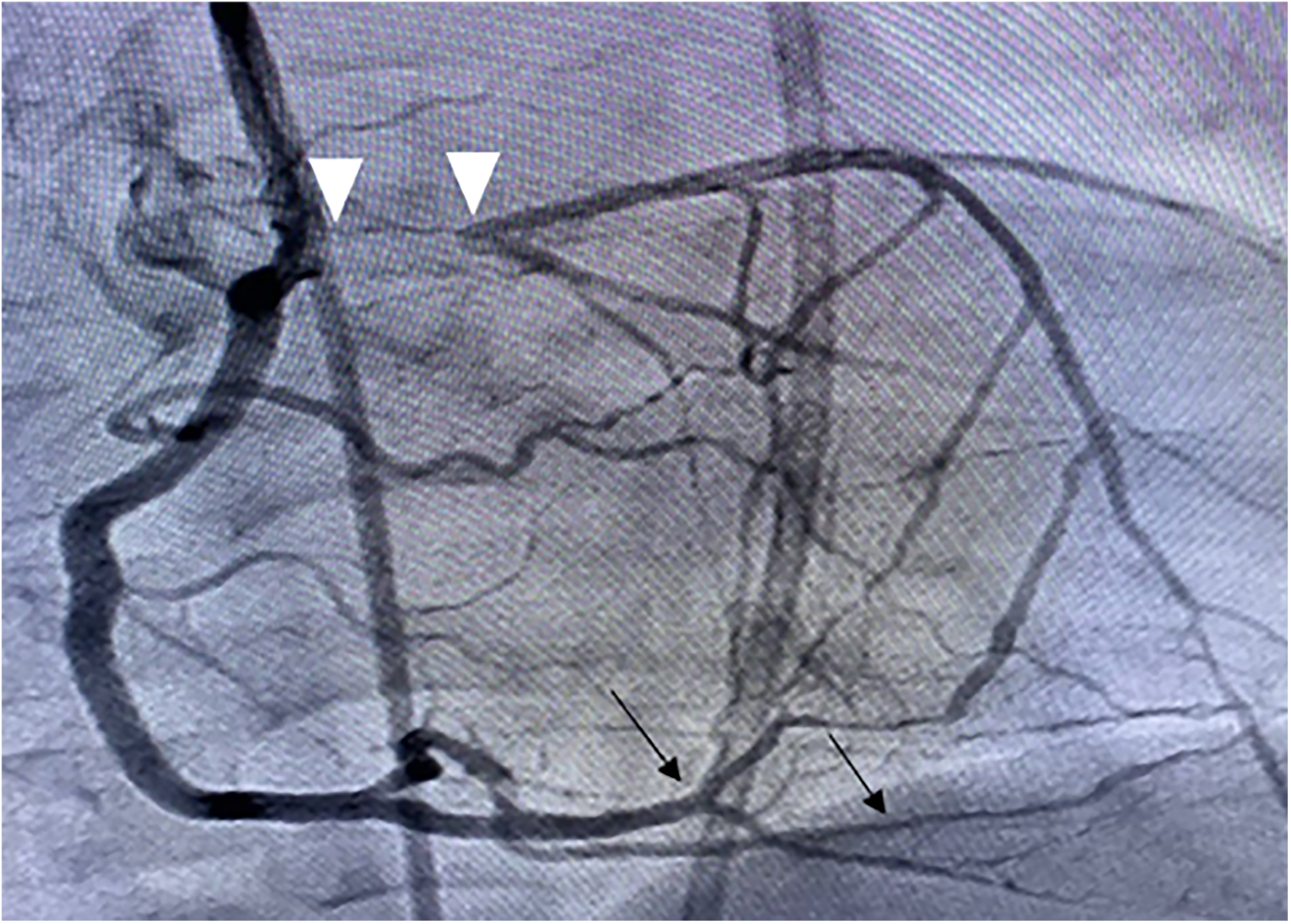
Blind-ending left main coronary artery (arrowheads) with filling from right coronary artery collaterals (black arrows).
Discussions regarding surgical intervention for his LMCA atresia were complex and involved input from neurology, cardiology, neurosurgery, and palliative care specialists. With stable cardiac status, coronary reconstruction was delayed in the setting of his unknown neurologic prognosis. His LV function and mitral regurgitation were monitored closely and continued to improve over time without evidence of ongoing ischemia. In addition, the patient tolerated multiple subsequent anesthetics.
The patient ultimately made a significant neurologic recovery, and by one-year post-event had returned to walking. With increased activity, the family reported intermittent symptoms of dyspnea and diaphoresis on exertion. Echocardiography showed a mildly dilated LV with an ejection fraction of 57% and trivial mitral regurgitation. Magnetic resonance imaging revealed moderate hypokinesia involving the mid-septal, apical, mid-anterior regions of the LV and a small apical subendocardial infarction. Based on his symptoms and after discussion with family, the decision was made to proceed with surgical revascularization.
After bypass and cardioplegia were achieved, the ascending aorta was transected. There was no ostium in the left aortic root sinus, and the proximal portion of the LMCA was found to be a fibrous cord connected distally to the patent junction of the LAD and Cx arteries (Figure 2A). The aorta was vertically incised to establish a left-facing ostium, and the incision was continued along the LMCA fibrotic cord and into the patent portion of the coronary bifurcation (Figure 2B). The aortic and coronary incisions were roofed with a decellularized bovine pericardial patch, establishing luminal continuity between the new left coronary ostium and junction of the LAD and Cx arteries (Figure 2C). The aorta was anastomosed to the root and the heart reperfused. Bypass was weaned without difficulty.
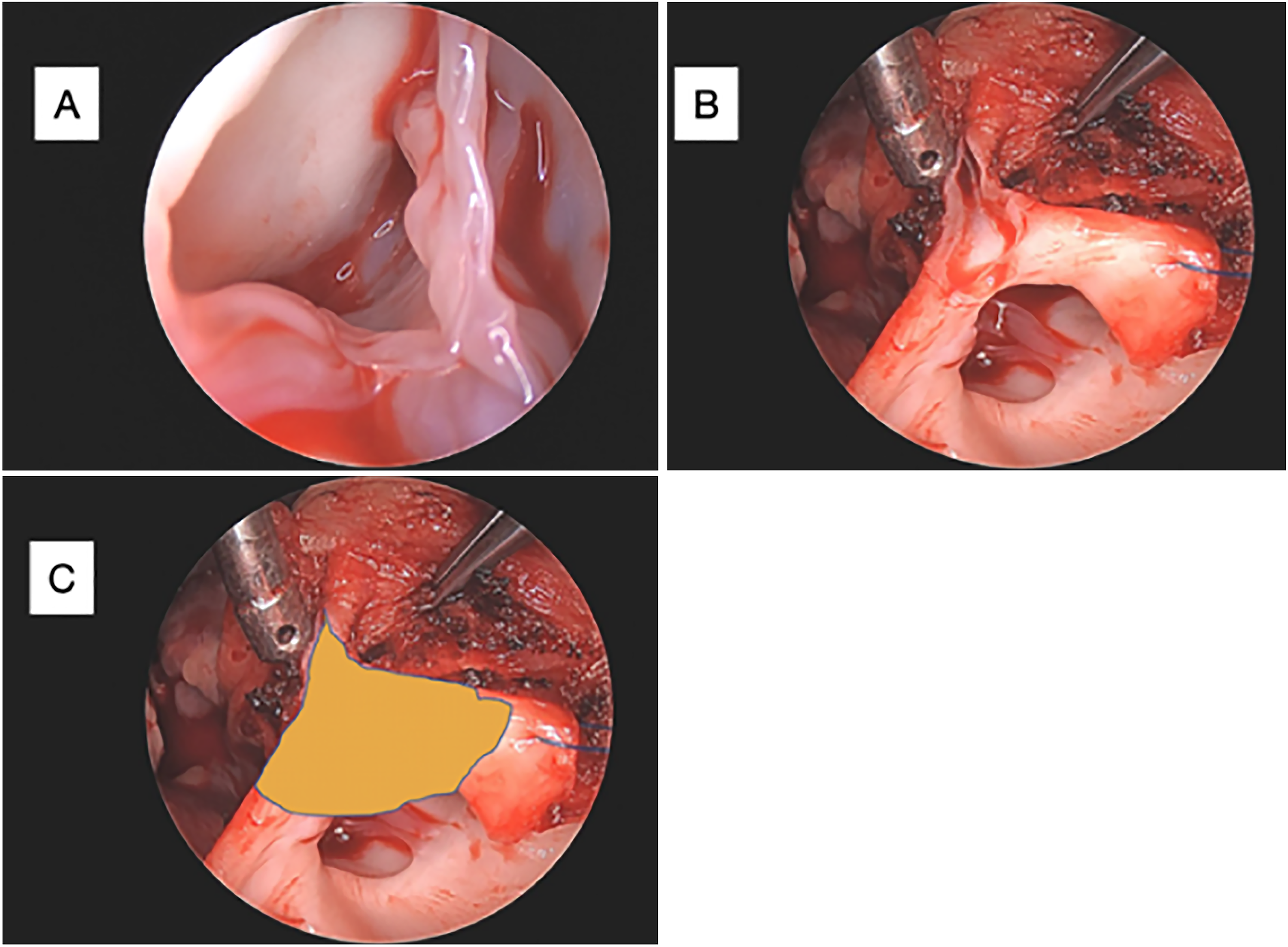
(A) Visualization of the defect showing absence of an ostium in the left coronary sinus. (B) Transected aorta and vertical incision of aortic root extending along the fibrous cord into the patent left anterior descending artery. (C) Schematic placement of the pericardial patch to roof the incision.
The patient’s postoperative course was uneventful. Echocardiography and CT angiography confirmed patency and antegrade flow in the newly established left coronary ostium (Figure 3). The patient was discharged on postoperative day 11. At 12-month follow up, echocardiography revealed anterograde flow through the LMCA with no stenosis, normal LV size, and only mildly decreased systolic function. Qualitative improvement of previously hypokinetic areas of the LV was noted. The patient is seen every 6 months in cardiology clinic and regularly in our multidisciplinary development clinic.
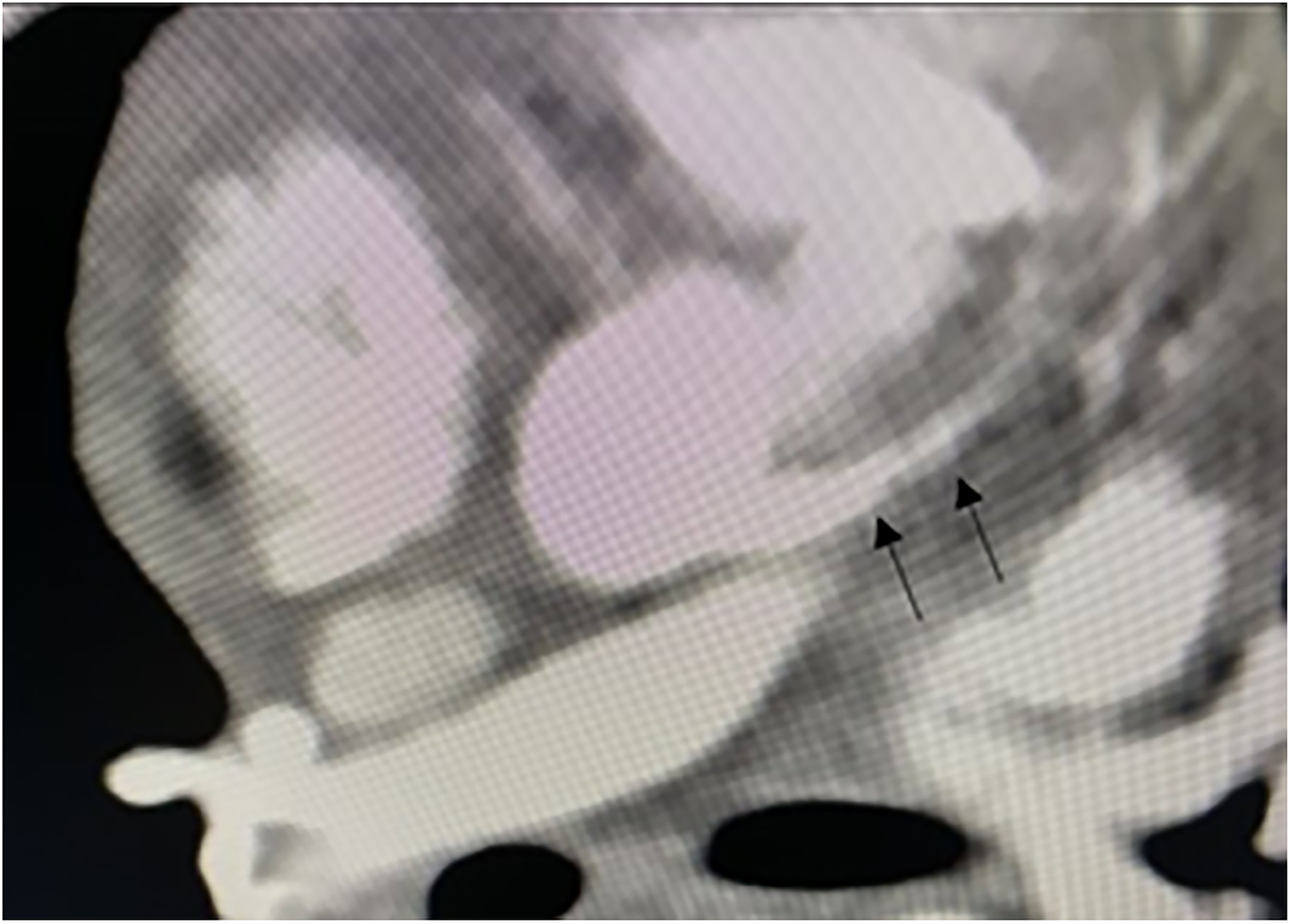
Postoperative computed tomography (CT) angiogram showing patency (black arrows) of the reconstructed left main coronary artery.
Comment
LMCA atresia is a rare condition with as few as 55 reported pediatric cases.1,2 Sudden cardiac arrest is reported in only 11% of pediatric LMCA atresia cases. 1 Our patient presented well below the median reported age (5 years) for repair of LMCA atresia, with only 8 ostioplasties having been performed in patients <3 years old. 1
Our technique followed the method presented by Albadi et al. 3 The fibrous cord lying between the sinus and coronary artery can be “opened” to provide a firm base on which to sew the ostioplasty patch. We utilized a bovine pericardial patch (Photofix, Artivion Inc). Henceforth, autologous pericardium may be preferable in view of a recent publication citing an incidence of degeneration of this bovine pericardial product.3–5
We prefer ostioplasty to CABG in these patients independent of age. The sustainability of the internal mammary graft in this setting remains concerning but could be used if, for some reason, ostioplasty could not be performed.
We elected to delay surgical repair due to the patient's incomplete post-arrest neurological recovery, stable ventricular function, and absence of evidence of ongoing ischemia. The later presentation of exertional symptoms and decreasing ventricular function prompted revascularization. If a decline in LV function or symptoms had occurred earlier in the post-arrest follow-up period, we would have certainly proceeded with revascularization at that time.
In conclusion, we found coronary ostioplasty to be a safe option for revascularization for LMCA atresia with good outcomes at an 18-month follow-up. We believe this technique should be considered a good option in pediatric patients regardless of age. Although reconstruction should normally be carried out as soon as possible after diagnosis, problems such as severe neurological injury (especially with the uncertainty of reasonable functional recovery) require close multidisciplinary management and surgical timing that optimizes the patient's condition and respects the family's wishes.
Footnotes
Author’s Statement
The authors thank the patient's parent for granting permission to publish this case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.