
Abstract
Different surgical techniques have been described for the primary repair of anomalous left coronary artery arising from the pulmonary artery (ALCAPA); however, very few techniques are described for management of coronary artery occlusion following ALCAPA repair. We present a case of a 7-year-old girl with left main coronary atresia status-post left coronary button transfer for ALCAPA in infancy. She underwent redo-sternotomy and left subclavian artery-to-left main coronary artery bypass plus mitral valve repair and had an uneventful postoperative course.
Introduction
Restoration of dual-coronary system is considered as the primary therapeutic goal in repair of anomalous left coronary artery arising from the pulmonary artery (ALCAPA). Coronary button transfer is the preferred technique. Alternative techniques like Takeuchi repair are reserved for special circumstances. However, very few techniques are described for coronary artery occlusion following ALCAPA repair. We describe a case of left main coronary atresia, years after coronary button transfer for ALCAPA, who underwent a successful left subclavian artery (LSCA)-to-left main coronary (LMCA) bypass grafting with mitral valve (MV) repair.
Case Report
A 7-year-old girl presented with a chief complaint of easy fatigability and shortness of breath on minimal exertion (NYHA/Modified Ross heart failure—Class III). She was diagnosed with ALCAPA at 3 months of age, at a different hospital, where coronary button translocation was done. The initial postoperative course was uneventful with good left ventricular (LV) function and mild mitral regurgitation (MR). However, over the course of 4 to 5 years, her condition gradually worsened with increasing MR and shortness of breath.
Her echocardiogram revealed severe MR along the coaptation margin of the MV leaflets (Figure 1A). The leaflets were abnormal with redundant tissue resulting in bileaflet prolapse. Chordae were elongated with patches of calcification. The LV ejection fraction was normal. Coronary angiography revealed atretic LMCA with retrograde filling of left anterior descending (LAD) and left circumflex (LCx) artery from the right coronary artery (RCA) and mild stenosis at the origin of LCx (Figure 1B).
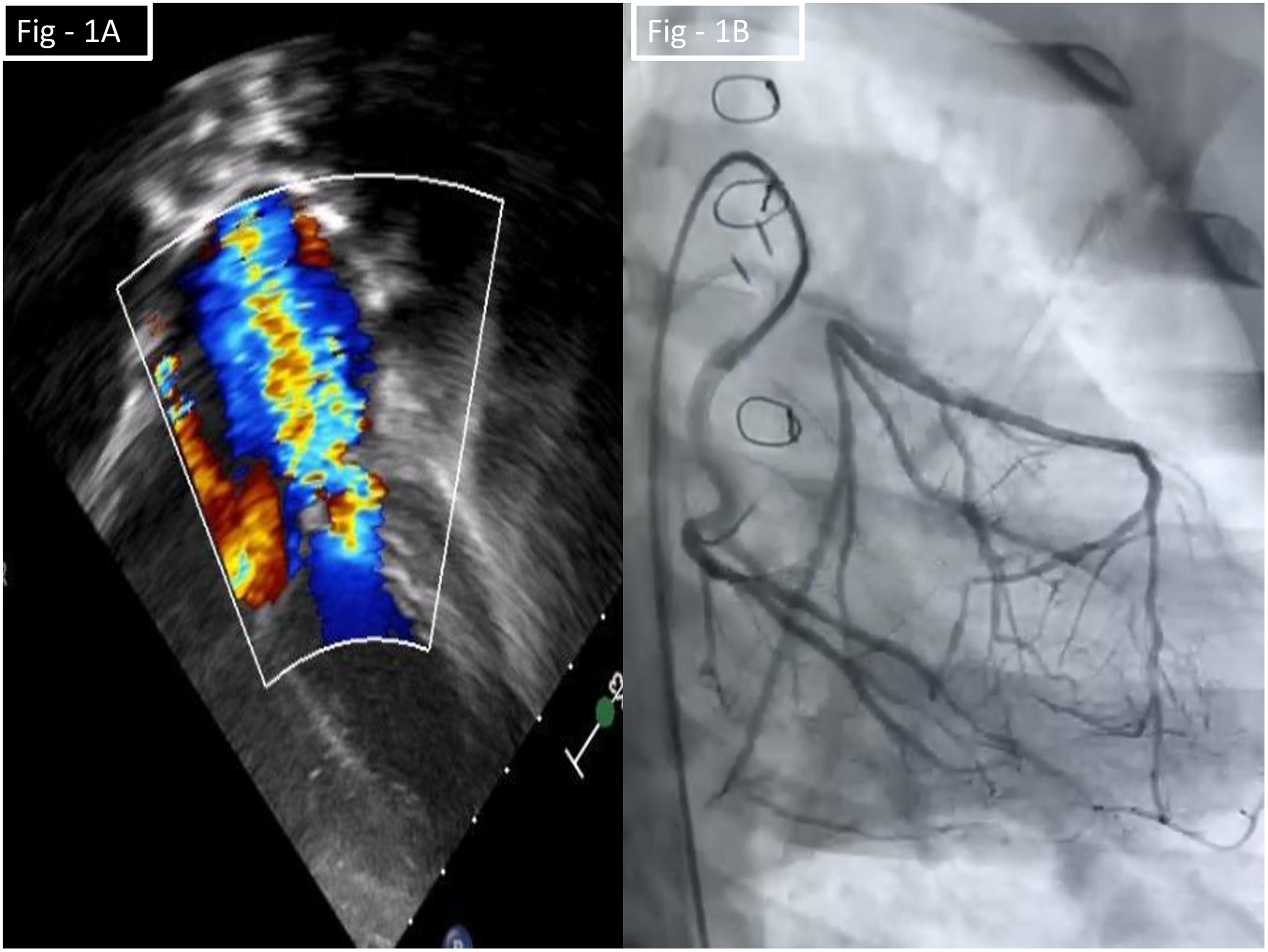
(A) Preoperative echocardiogram—severe mitral regurgitation; (B) Preoperative coronary angiogram—left main coronary atresia with retrograde filling of left anterior descending and left circumflex artery from the right coronary artery.
Surgical Technique
After redo-sternotomy and mediastinal dissection, proximal LSCA was looped and dissected to its branches. Continuous pulse-oximetry monitoring on the left index finger showed good pulsations on test clamping of the LSCA. Cardiopulmonary bypass (CPB) was instituted with aorto-bicaval cannulation. The space between the proximal aorta and main pulmonary artery (MPA) was dissected. The MPA was transected after arresting the heart with antegrade cardioplegia. The previously implanted left coronary button was identified. The atretic proximal LMCA was ligated near the aortic root and divided. No clear lumen of LMCA was identified distal to the division, as it was all fibrosed and possibly dissected. Hence, proximal LAD was opened and the incision extended proximally across the LMCA stump, identifying the LCx ostium posteriorly. The LSCA was clamped distally, divided, turned down, and the posterior aspect was anastomosed to the LMCA stump with a 7-0 polypropylene continuous suture. A small autologous MPA patch was harvested and used to augment the anastomosis anteriorly, extending into the LAD (Figure 2). MV repair was performed through a right atrial transseptal approach. There was bileaflet prolapse; anterolateral segment more than posterior-medial. The papillary muscles and the chordae tendinae were thickened, fibrosed and elongated, suggesting an ischemic etiology. Anterolateral papillary muscle splitting and sliding plasty were done along with P2 resection and sliding plasty and chordal translocation from P2 to A2. The MPA anastomosis was shifted to the right side, to avoid LSCA compression by the LPA and the anterior defect augmented with autologous pericardial patch. Patient weaned gradually from CPB. After satisfactory epicardial echo, standard sternal closure was done and the patient transferred to intensive care unit receiving milrinone 0.5 μg/kg/min. CPB time was 313 min and aortic cross-clamp time was 175 min. The postoperative course was uneventful and patient was and extubated the next day and discharged on postoperative day 7. Echocardiogram showed good biventricular function, trivial MR (Figure 3), and good flow in branch pulmonary arteries. Computed tomography (CT) scan showed good patency of LSCA-to-LMCA bypass and good flow into the LAD and the LCx (Figure 4).
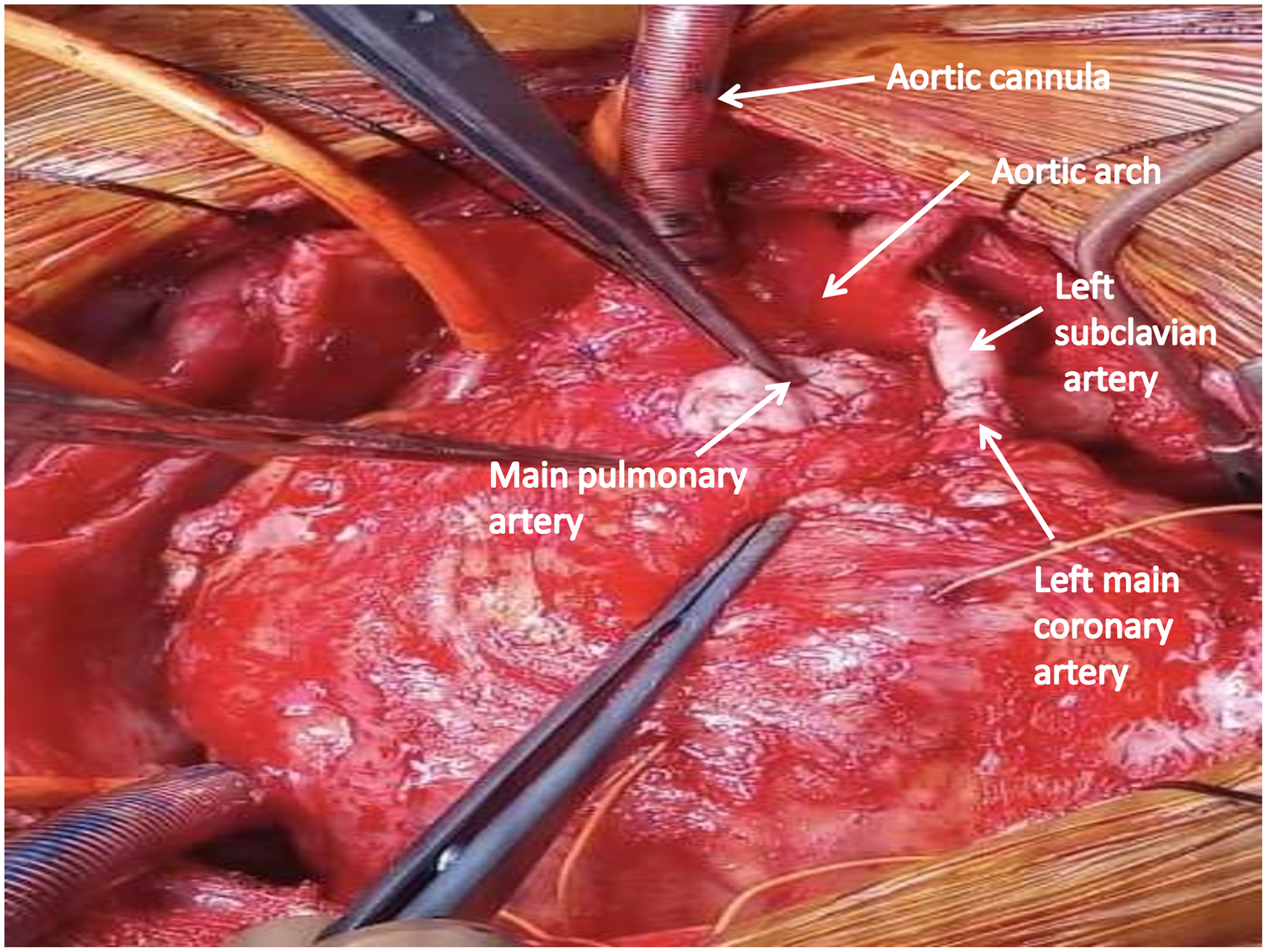
Intraoperative photograph.
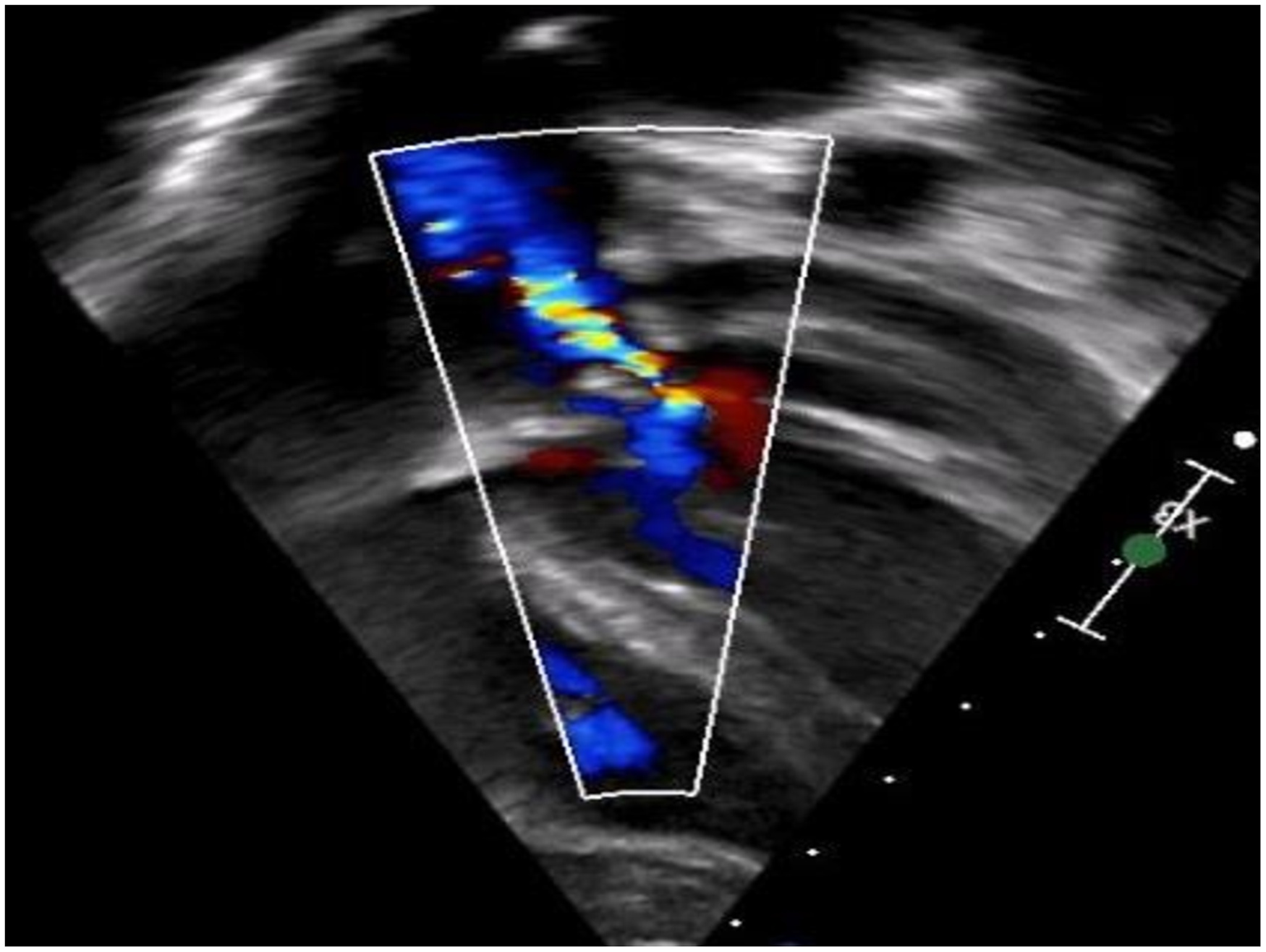
Postoperative echocardiogram—trivial mitral regurgitation.
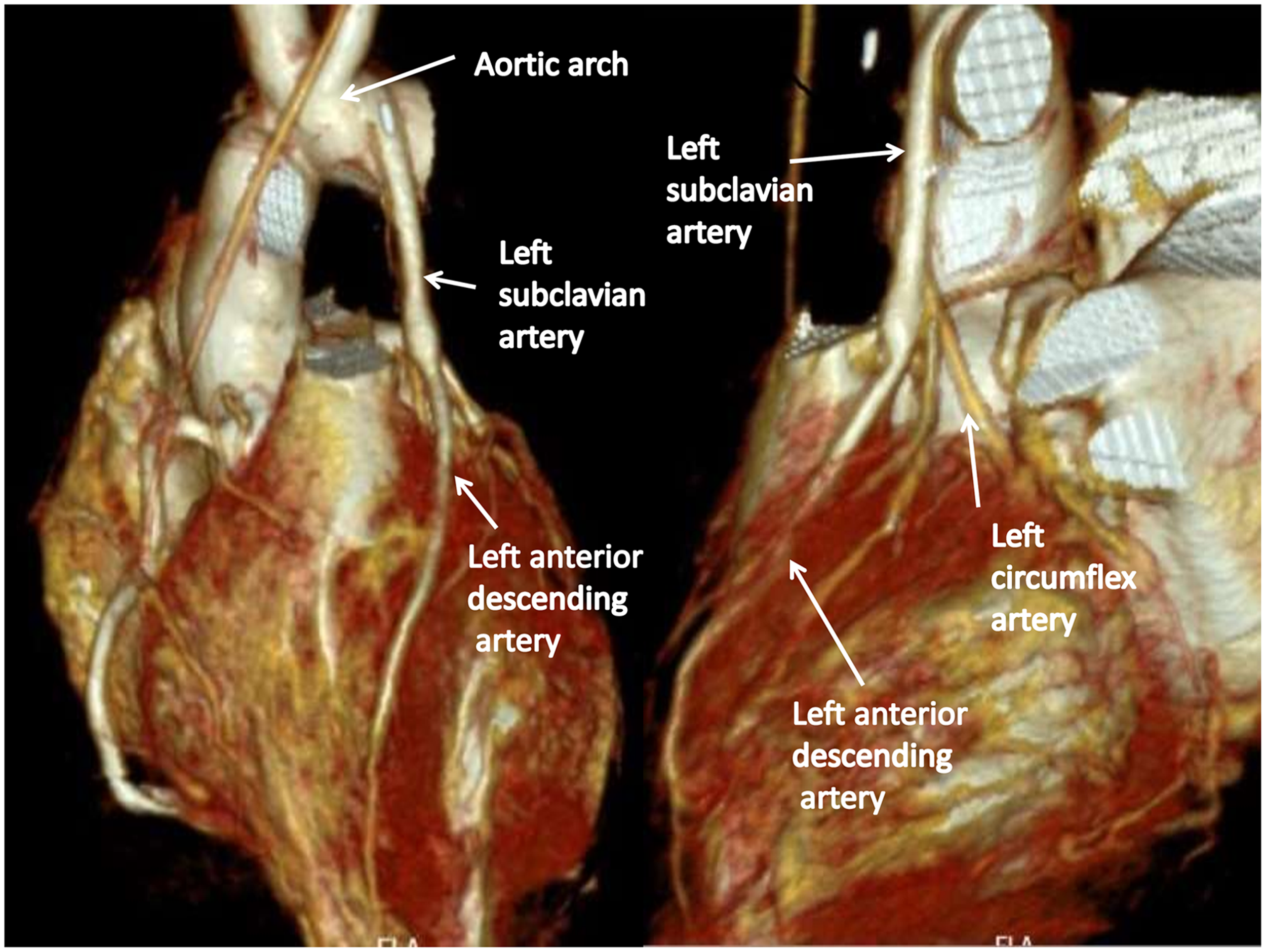
Postoperative computed tomography (CT) angiogram 3D reconstruction.
Comment
Different techniques have been described for ALCAPA repair with the aim to restore the dual-coronary artery system. Coronary button transfer is the most widely used technique, whereas the Takeuchi repair is reserved for special circumstances. Simple ligation of anomalous LCA was practiced previously but largely abandoned now in favor of procedures restoring “dual-coronary” supply. Collateral supply, however robust, may be inadequate at times of stress or during exercise. LSCA-to-LMCA bypass for ALCAPA repair was first described by Apley et al
1
in 1957 and first successfully performed by Meyer and coworkers in 1968.
2
The LSCA-to-LMCA bypass or the “Meyer operation” establishes a two-coronary-artery system, has growth potential, requires one vascular anastomosis, and results in improvement of LV contractility.
3
Different studies4,5 in the literature have shown that the LSCA-to-LMCA bypass is a valid option for primary ALCAPA repair and can be done without CPB. Drawbacks of using LSCA include left arm ischemia and asymmetric arm growth but were not seen in our case.
The exact etiology of atresia of the coronary button and LMCA post-ALCAPA repair was unknown in this case. Failure to add the Lecompte maneuver, as stressed by some investigators 6 to prevent stretching of LMCA by the pericardial patch used to close the defect in MPA, could be one of the reasons. A pledgeted hemostatic stitch used at the base of MPA posterolaterally in the primary surgery could also have caused compression and later occlusion of the LMCA. In our case, the LAD was filling retrogradely and its size was small; hence, we chose LSCA-to-LMCA grafting to achieve antegrade perfusion of both left coronary branches (LAD and LCx) and to achieve good quality anastomosis between two good-sized vessels.
Any worsening of MR after ALCAPA repair should be thoroughly evaluated by coronary angiography to rule out coronary button occlusion. Free right subclavian artery graft has been used to bypass LMCA occlusion, 7 but the length of the conduit is limited and there is a need for two anastomoses. Surgical patch angioplasty has been described in children with coronary occlusion, 8 and different patch materials have been used but were not feasible in our case due to the long length of occlusion.
Thus, we conclude that in-situ LSCA-to-LMCA bypass is technically feasible and can be a good option for coronary bypass in children with proximal coronary lesions. The quality of the conduit is good with potential for growth and requires only one anastomosis.
Footnotes
Authors’ Statement
Parents of the child consented to the publication of the case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.