
Abstract
Background
Infants represent a distinct subgroup within the field of pediatric heart transplantation, with greater rates of congenital heart disease (CHD), more organ dysfunction, and increased reliance on mechanical ventilation at the time of transplant than older children.1-3 Accordingly, infants experience the worst early post-transplant mortality of any pediatric age group, but those who survive beyond this early hazard period achieve greater long-term survival than all other children.2,4,5
Given the significant early post-transplant mortality burden in infants, and considering superior long-term survival among early survivors, it is imperative to identify risk factors that allow for pretransplant physiologic optimization and risk stratification for 1-year survival. Our group has previously shown that a compounding effect on post-transplant mortality exists depending upon the number of risk factors present. 6 Consistently reported independent predictors of post-transplant mortality in infants include both nonmodifiable (CHD) and modifiable risk factors (mechanical ventilation).1,3,6-10 Paralytic agents and total parenteral nutrition (TPN)-dependence are also commonly required by infants awaiting heart transplantation and are widely considered to be negative prognosticators, but their impacts on post-transplant outcomes remain understudied. In particular, some have questioned whether concomitant paralytic or TPN use (among other support modalities) in patients on mechanical has influenced and obscured the effects of mechanical ventilation itself reported by prior analyses. With this gap in the literature in mind, the present study sought to characterize the impacts of these 2 additional modifiable risk factors on post-transplant hospital outcomes, resource utilization, and 1-year mortality, both independent of and in addition to mechanical ventilation.
Methods
Patients and Data Acquisition
The present study was approved by the Cincinnati Children's Hospital Medical Center internal review board with a waiver of informed consent. The UNOS and Pediatric Health Information System (PHIS) databases were used to identify patients less than one year of age at the time of listing who received heart transplants between 2003 and 2020 in the United States. Data from both UNOS and PHIS were implemented. The UNOS database is predicated around organ utilization and, with mandatory reporting of all transplant listings in the United States, provides information about patients’ listing status, their transplant procedure, and post-transplant outcomes that are not available in PHIS. PHIS, on the other hand, is a hospital-based administrative dataset that includes 49 pediatric hospitals in the United States and, through ICD reporting and insurance billing information, allows for the analysis of day-by-day resource utilization (eg, mechanical ventilation, paralytics, TPN) that is not present (or unreliably recorded) in UNOS. Using the methodology previously described by the authors, patients present in both databases were identified and matched by variables present in both UNOS and PHIS: date of birth, gender, transplant center, date of admission, and date of transplantation. 11 Only patients present in both UNOS and PHIS were included in the analysis.
Support modalities of interest included mechanical ventilation, paralytic agents, and TPN-dependence. Patients were grouped into one of 6 mutually exclusive groups depending upon support requirement(s) at the time of transplant: none (“no-support”), mechanical ventilation only (“Ventilator-only”), Ventilator + Paralytics, TPN-dependence-only (“TPN-only”), Ventilator + TPN, and Ventilator + Paralytics + TPN (Table 1). Patients on extracorporeal membrane oxygenation (ECMO) at the time of transplant (per UNOS) were excluded from the no-support group.
Cohort.a
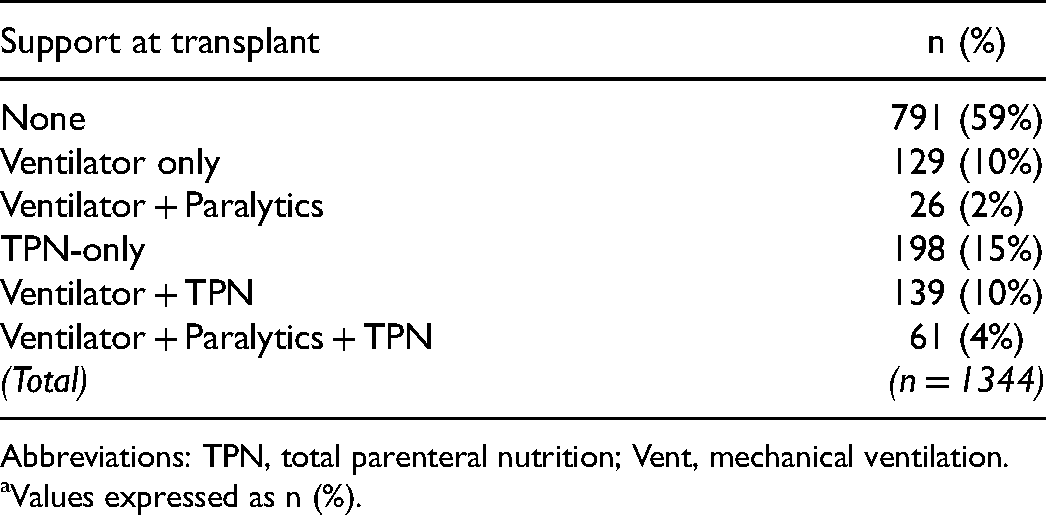
Abbreviations: TPN, total parenteral nutrition; Vent, mechanical ventilation.
Values expressed as n (%).
Paralytic use and TPN-dependence were determined using insurance charges from PHIS. Patients on paralytic agents were identified using pharmacy charges for atracurium, cisatracurium, rocuronium, or vecuronium for ≥3/5 pretransplant days. Only patients who received paralytic agents with concomitant mechanical ventilation were considered as part of the paralytics group (Ventilator + Paralytics). Since paralytic agents may be used transiently for diagnostic procedures in infants, requiring paralytic charges for at least 3/5 pretransplant days sought to increase the sensitivity of identification of patients who required paralytic agents for therapeutic purposes. Similarly, TPN-dependence at the time of transplant was determined by pharmacy charges for “fat emulsions,” “hyperalimentation solutions unspecified,” or “hyperalimentation solution and electrolyte combinations” for ≥3/5 pretransplant days without charges for oral nutrition for 5/5 pretransplant days. Those who received insurance charges for oral nutrition in addition to parenteral were not considered as part of the TPN-dependent group since such patients did not qualify as receiving total parenteral nutrition. The duration of 5 days was again chosen to increase the sensitivity of identifying TPN-dependent patients.
Although not one of the 2 primary support modalities of interest, mechanical ventilation was also included as a support modality. Mechanical ventilation is common among TPN-dependent patients and, for the purposes of this study, was required to define the paralytics group. Furthermore, it is the opinion of some (including the authors) that previous analyses reporting the detrimental effects of mechanical ventilation may have been influenced by concomitant paralytic and TPN use. Including mechanical ventilation-only as a support group in addition to other support groups with concomitant ventilation thus sought to shed light on this latter assumption. A major limitation of using UNOS alone to determine ventilatory status is that “ventilator-at-transplant” is listed as binary (yes/no) and therefore provides no context as to how long the patient was intubated. Therefore, PHIS was primarily used to define the ventilatory groups. Under the assumption that prolonged ventilation (>48 h) prior to transplant was very likely due to respiratory failure, patients in PHIS with insurance charges for mechanical ventilation for ≥2 continuous days pretransplant were considered “ventilated-at-transplant.” Patients with mechanical ventilation charges only on pre-transplant days one or 2 were included in the ventilated group only if UNOS also designated them as such. Seventy-two (20%) patients “on-ventilator” in UNOS could not be verified in PHIS and were therefore not included as part of the ventilator group.
Demographic (eg, gestational age, birthweight, gender, race/ethnicity) and cardiac diagnosis information were obtained from UNOS. Preterm birth was defined as gestational age <37 weeks and low birthweight was defined as <2.5 kg.12,13 Pretransplant clinical status data were obtained from UNOS as well, including listing UNOS status, renal and hepatic dysfunctions, ventricular assist device (VAD) utilization, inotrope and ECMO requirements, and waitlist durations. Renal dysfunction was defined as eGFR <60 mL/min/1.73 m2, calculated using the bedside Schwartz formula based upon creatinine and height at the time of transplant, as listed in UNOS. 14 Hepatic dysfunction was defined as total serum bilirubin >1.2 mg/dL at the time of transplant, as listed in UNOS. 15 Post-transplant ventilation durations, intensive care unit (ICU) lengths of stay, and ECMO requirements were calculated using PHIS insurance-charges data. Post-transplant dialysis requirements and mortality data were obtained from UNOS.
Statistical Analysis
Statistical analyses were performed using R (R Foundation for Statistical Computing, https://www.R-project.org/). Comparative analyses of demographics, pretransplant characteristics, and post-transplant outcomes were performed between groups, with post hoc pairwise analyses comparing each individual support group to the no-support group when significant (P < .05). Mood's median test was employed for continuous variables, and Pearson χ2 test with Yates’ continuity correction or Fisher exact test (for expected cell counts <5) were used for categorical variables. Kaplan-Meier analyses with the log-rank test were performed to determine one-year survival. Cox proportional hazards regression analyses were performed to identify predictors for mortality within the first year post-transplant, with variables with P < .1 on the univariable analysis used as covariables in multivariable analyses. ECMO requirement at transplant was not included in multivariable analyses due to significant collinearity with mechanical ventilation, thereby limiting the ability to differentiate the independent impacts of each.
Results
In total, 1344 infant heart transplant recipients were identified, 41% (n = 553) of whom required support at the time of transplant (Table 1). The cohort demographics are shown in Table 2. Rates of preterm birth (P = .449) and low birthweight (P = .985) were similar between all groups. White patients, in general, were more likely to require support, whereas Hispanic patients were less likely. CHD patients were also more likely to require support (all P < .05 vs. no-support except Ventilator + Paralytics [P = .466 vs. no-support]).
Demographics of Cohort.a
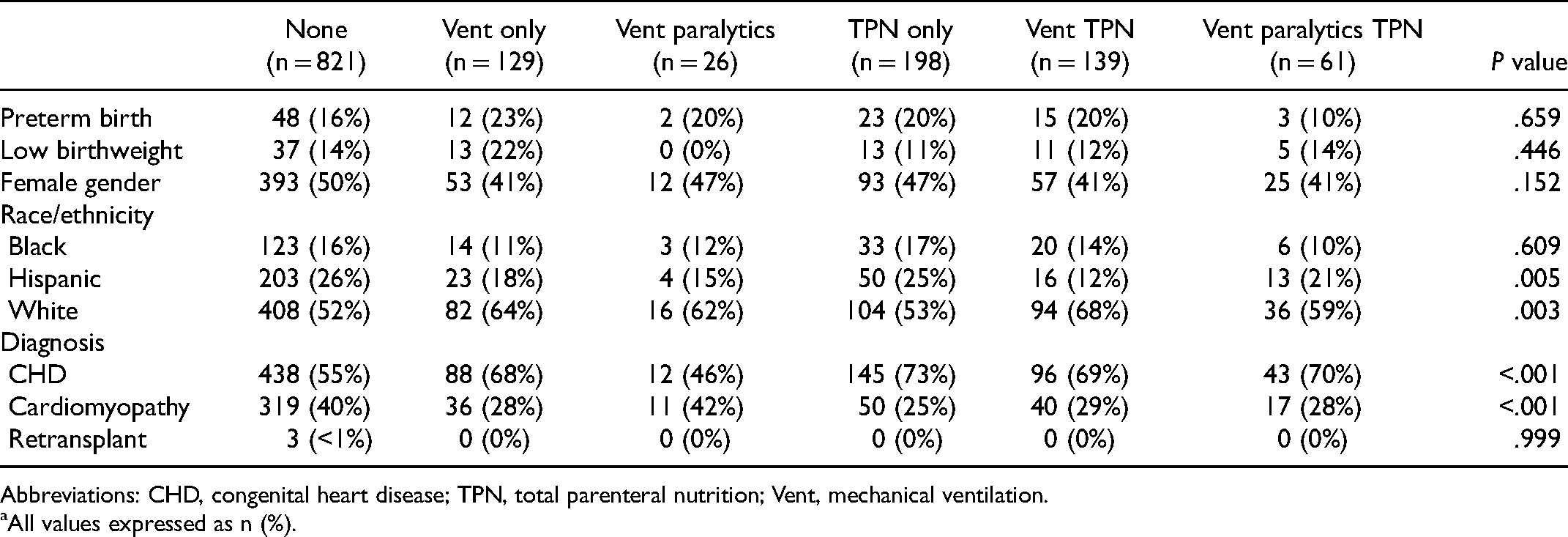
Abbreviations: CHD, congenital heart disease; TPN, total parenteral nutrition; Vent, mechanical ventilation.
All values expressed as n (%).
Infants who required support were, in general, more ill at the time of transplant, having greater end-organ dysfunction and inotrope requirements (Table 3). On pairwise analysis comparing supported patients to the no-support group, renal dysfunction was more common in the TPN-only, Ventilator + TPN, and Ventilator + Paralytics + TPN] groups (all P < .05 vs. no-support). Hepatic dysfunction was more common in all support groups (P < .05 vs. no-support) aside from Ventilator + Paralytics (P = .764). Inotrope requirements were greater in all support groups (all P < .01 vs. no-support). Supported patients were listed with higher UNOS statuses (P < .001 for all vs. no-support except Ventilator + Paralytics [P = .303 vs. no-support]). Clinically, waitlist durations were shorter in all support groups, although statistical significance was only seen in the Ventilator-only and Ventilator + Paralytics + TPN groups (both P < .01 vs. no-support). VAD utilization rates were 9% to 15% between groups and were similar between the support and no-support groups (P = .056).
Clinical Status at Time of Transplant.a
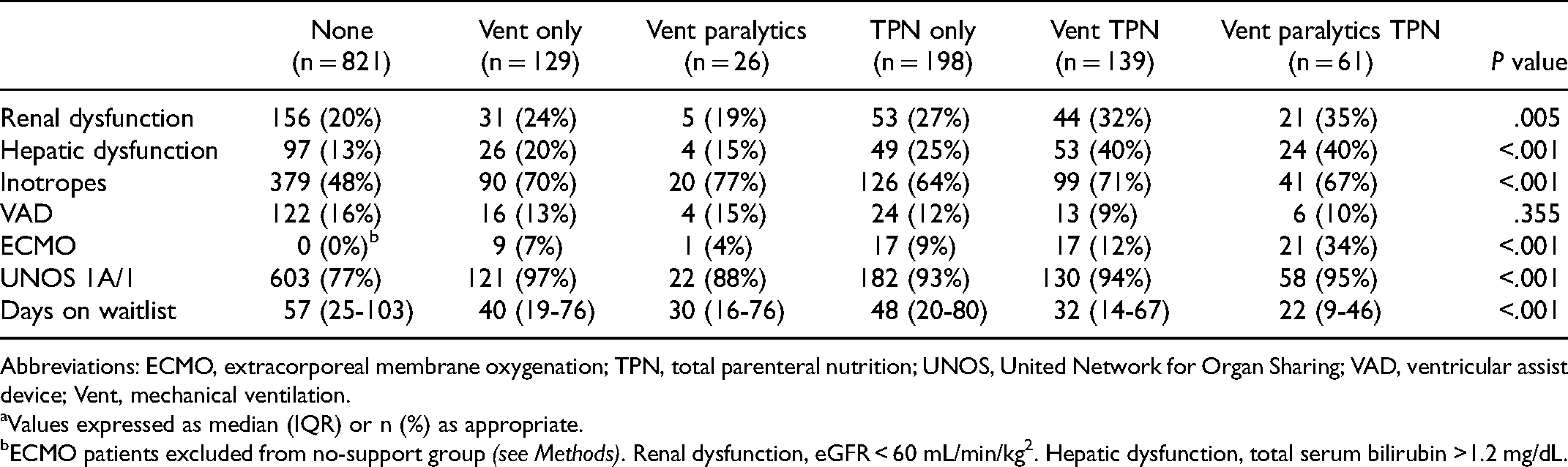
Abbreviations: ECMO, extracorporeal membrane oxygenation; TPN, total parenteral nutrition; UNOS, United Network for Organ Sharing; VAD, ventricular assist device; Vent, mechanical ventilation.
Values expressed as median (IQR) or n (%) as appropriate.
ECMO patients excluded from no-support group (see Methods). Renal dysfunction, eGFR < 60 mL/min/kg2. Hepatic dysfunction, total serum bilirubin >1.2 mg/dL.
Post-transplant hospital resource utilization was almost uniformly greater among patients who required pretransplant support (Table 4). Longer post-transplant mechanical ventilation durations were experienced by all supported patients (all P < .05 vs no-support). Supported patients also required longer post-transplant ICU and hospital lengths of stay (all P ≤ .001 vs no-support). Patients requiring Ventilator + TPN and Ventilator + Paralytics + TPN at transplant had greater post-transplant dialysis and ECMO requirements (both P < .05 vs no-support).
Post-transplant Hospital Outcomes.a
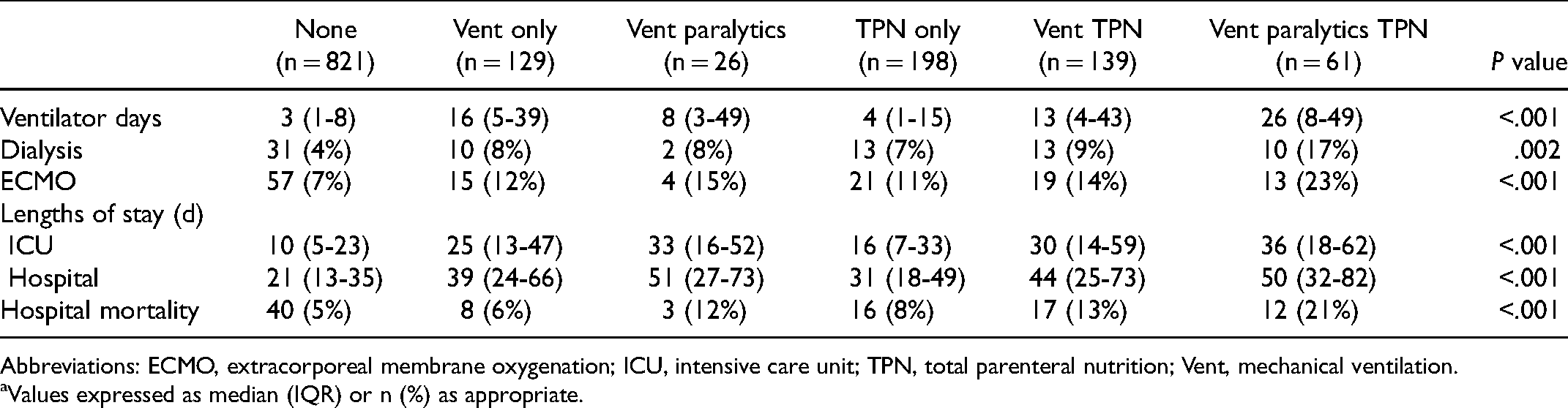
Abbreviations: ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; TPN, total parenteral nutrition; Vent, mechanical ventilation.
Values expressed as median (IQR) or n (%) as appropriate.
Supported patients, as a whole, experienced inferior survival. In-hospital post-transplant mortality occurred in 10% (n = 56) of supported patients compared to 5% (n = 40) of the nonsupported (P < .001). In-hospital death accounted for the majority of one-year mortalities in both groups—65% (56/86) in the support cohort and 57% (40/70) in the nonsupported group. The most common causes of in-hospital mortality included: cardiac event (eg, arrest, arrhythmia, ventricular failure; support—13%, no-support—18%), primary graft failure (support—13%; no-support—23%), respiratory failure (support—11%, no-support—13%), and non-cardiorespiratory end-organ failure (support—27%, no-support—20%).
By support group, rates of one-year survival were: 91% (no-support), 88% (Ventilator + Paralytics), 87% (Ventilator-only), 86% (TPN-only), 81% (Ventilator + TPN), and 73% (Ventilator + Paralytics + TPN), with significant differences between no-support and Ventilator + TPN (P = .006), no-support and Ventilator + Paralytics + TPN (P < .001), and Ventilator-only and Ventilator + Paralytics + TPN (P = .047). Upon multivariable analysis (Table 5), no-support was protective against one-year mortality (HR 0.66 [95% CI 0.48-0.91]), whereas requirement for each support modality independently predicted mortality (Ventilator + Paralytics vs. neither: 2.02 [1.25-3.27]; Ventilator-only vs. no-ventilator: 1.54 [1.10-2.14]; TPN vs. no-TPN: 1.53 [1.10-2.13]). Compared to no-support, Ventilator + TPN and Ventilator + Paralytics + TPN] also independently predicted mortality. Additional predictors of mortality for all patients, independent of other support requirement(s), included CHD and renal dysfunction. The most common causes of death postdischarge within the first year included: cardiac events (support—19%, no-support—4%), respiratory failure (support—29%, no-support—7%), infection (support—15%, no-support—22%), and rejection (support—10%, no-support—33%).
Cox Proportional Hazards Ratio for 1-Year Post-transplant Mortality.a
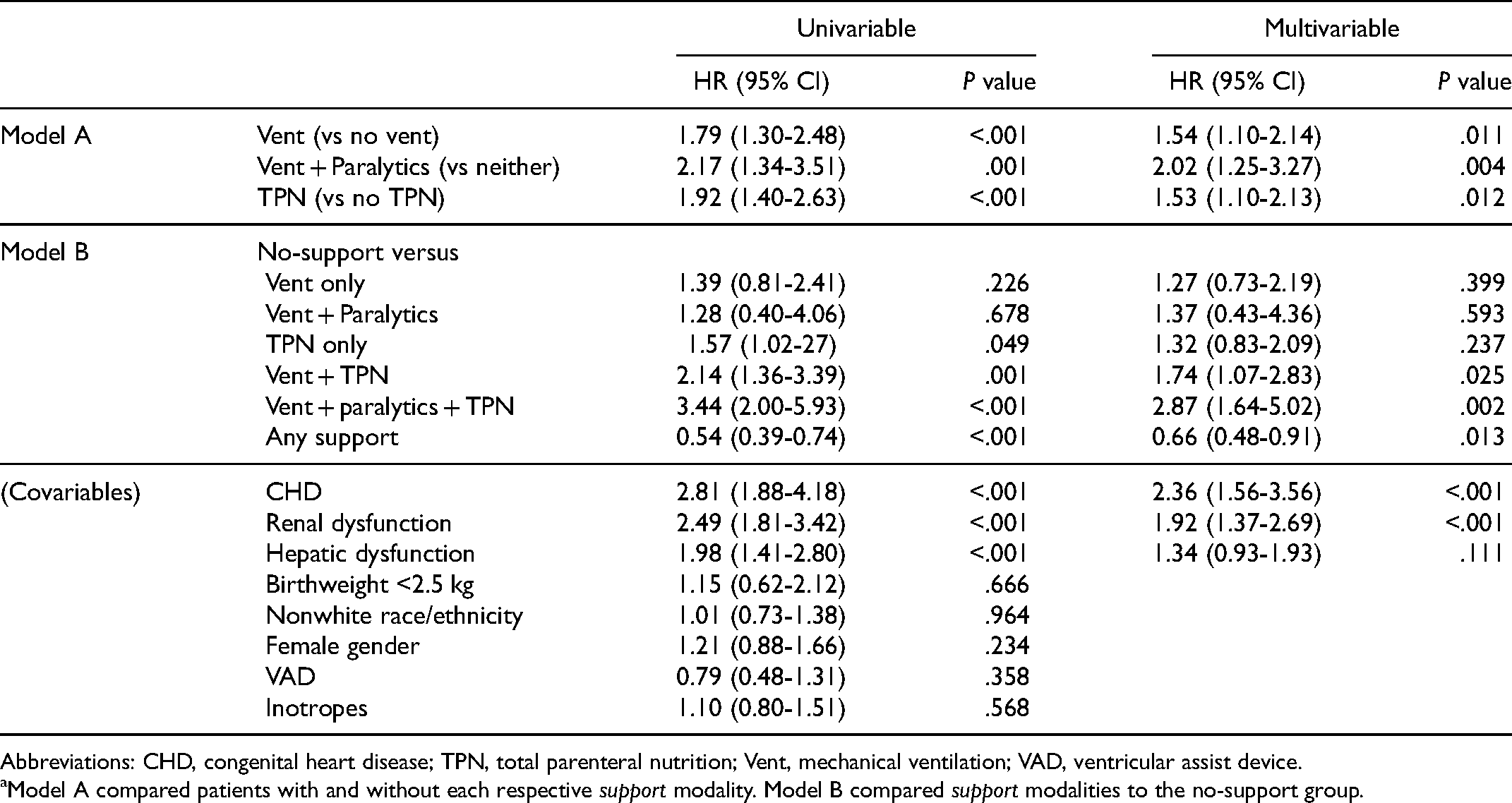
Abbreviations: CHD, congenital heart disease; TPN, total parenteral nutrition; Vent, mechanical ventilation; VAD, ventricular assist device.
Model A compared patients with and without each respective support modality. Model B compared support modalities to the no-support group.
Comment
The present retrospective, multi-institutional, national database study utilized UNOS and PHIS to identify over 1340 infants who received heart transplants in the United States between 2003 and 2020. The impacts of support requirements (paralytics and TPN-dependence, with and without concomitant mechanical ventilation) at the time of transplant on post-transplant hospital outcomes, resource utilization, and mortality were studied. Although pretransplant mechanical ventilator (MV) requirement is a well-established risk factor for post-transplant mortality, the independent effects of commonly co-utilized support modalities such as paralytics and TPN are unclear.1,3,5,6,10 In the present analysis, paralytic requirements and TPN-dependence at the time of transplant independently predicted one-year post-transplant mortality and were also associated with greater post-transplant hospital resource utilization.
Infants represent a distinct patient population within the field of pediatric heart transplantation and, therefore, warrant special consideration. By age group, infants comprise the largest proportion of children awaiting transplant in the United States (accounting for approximately one-third of all waitlist candidates) and, accordingly, experience the greatest waitlist mortality.1,4 Compared to other pediatric patients, infants are generally more ill at the time of transplantation, with greater rates of organ dysfunction and more MV and ECMO requirements.1,2,7,16 Infants have the worst one-year survival of any pediatric age group but, despite this, achieve long-term survival superior to all other children, with median survival exceeding 20 years.1,2,4,5,10,17 In light of these early hazards of mortality, the present study focused on mortality within the first year following transplant.
In addition to mechanical ventilation, other established risk factors for post-transplant mortality in infants include CHD, renal and hepatic dysfunction, and ECMO.1,3,5,8,17 Previous analyses have been limited by the inability to comment upon the impacts of paralytics and TPN-dependence, though, largely due to the difficulty of identifying these support modalities using oft-used datasets like UNOS. Concomitant paralytic utilization and TPN-dependence may have confounded the results of prior analyses, particularly those focusing on the “independent” impact of mechanical ventilation on post-transplant outcomes. In addition to UNOS, the present analysis also utilized PHIS, which, through daily insurance-charge information, allowed for the identification of patients receiving paralytics and who were TPN-dependent at the time of transplant.
Expectedly, infants who required support at the time of transplant were overall more ill at transplant (having greater degrees of other risk factors such as CHD, renal and hepatic dysfunction, and inotrope requirements). Accordingly, these patients required greater post-transplant hospital resource utilization and experienced inferior one-year survival compared to those patients who did not require support. Incorporation of PHIS data also allowed for the calculation of post-transplant MV durations and ICU lengths of stay (variables not present in UNOS). Although intuitive that pretransplant mechanical ventilation would also portend longer post-transplant ventilation, the fact that infants who required isolated mechanical ventilation (without paralytics or TPN) spent, on average, nearly 2 weeks longer on the ventilator after transplant than those not on pretransplant ventilation was surprising. Ventilated patients who also required paralytics and who were TPN-dependent experienced a median 26 days of post-transplant mechanical ventilation, compared to just 3 days in patients requiring no-support. Also interesting was the finding that patients who were TPN-dependent alone (no ventilation or paralytics) still experienced over 50% longer ICU and hospital lengths of stay than patients in the no-support group.
On multivariable analysis, the requirement for each support modality (mechanical ventilation, paralytics, and/or TPN-dependence) independently predicted one-year mortality, whereas no-support was protective. Noteworthy is that approximately two-thirds of one-year mortalities within the support cohort occurred prior to discharge, again confirming the early hazards of post-transplant mortality among infants and also alluding to the detrimental effects of pretransplant support of any kind on hospital outcomes. These in-hospital deaths occurred most commonly secondary to acute cardiac or other non-cardiorespiratory end-organ failure. The high rates of early mortalities among supported patients were most likely because these patients “limped” into transplantation while still requiring significant support requirements. Previous work by our group and others has highlighted the perils of pursuing transplantation in the presence of certain modifiable risk factors.5,6,17,18 It is important to always keep in mind that simply getting to transplant is not the goal—achieving long-term survival with a great quality of life is.
The ultimate goal of accurately identifying those patients who are simply “too ill” for transplantation remains somewhat elusive, but the present analysis highlights certain clinical factors that, when present, may prompt strong consideration for pursuing physiological optimization—possibly with mechanical circulatory support or even with temporary delisting and physiologic optimization (ie, weaning from support)—prior to transplantation. When pretransplant support is required, patients with CHD and those with impaired renal function should be considered very high risk. In the era of organ scarcity, equitable organ allocation (ie, ensuring that donor organs go to the patients who will benefit most) is imperative. The findings herein can assist in pre-transplant planning and post-transplant decision-making, informing clinicians and families alike of the expected course of patients who require support and highlighting the importance of risk factor modification whenever possible.
Limitations and Future Directions
While novel, the present study has several important limitations. First, the limitations inherent to all retrospective observational studies, as well as potential sampling and reporting biases, must be noted. The impacts of these shortcomings were somewhat abated by utilizing both UNOS and PHIS. As a comprehensive dataset with mandatory reporting of all transplants in the United States, UNOS is less subject to reporting bias. Only incorporating patients who could be identified in both datasets also served as a “safeguard” against these biases. The utilization of PHIS did result in a smaller patient population than using UNOS alone (619 patients [31% of all eligible UNOS patients] could not be identified in PHIS and were excluded). The most likely explanation for the failure to match these patients is simply that they received transplants at non-PHIS-affiliated centers—62 centers in UNOS performed infant heart transplants during the study period compared to 49 represented in PHIS. It is possible that the omission of these patients somehow influenced the results and conclusions, but the utilization and impacts of TPN use, paralytic administration, and pretransplant ventilation duration could not be determined for these patients.
The methodology devised to identify patients on paralytics and TPN warrants validation in further analyses, as the accuracy of the support variables ascertained using PHIS could not be directly validated using UNOS (as paralytics and TPN information are unavailable in UNOS). Future studies should also seek to address the impacts of ECMO specifically (which could not be fully assessed due to significant collinearity with ventilation), more prolonged support (eg, long-term TPN-dependence), partial (rather than total) parenteral nutrition, and other clinical support modalities like sedative agents. Attention should also be paid to the precise indications for support, the data for which was unavailable but might have important prognostic implications. Of note, CHD patients comprised over half of the cohort, yet specific morphologic (eg, hypoplastic left heart syndrome [HLHS]) could not reliably be determined from UNOS or PHIS. Work from the Pediatric Heart Transplant Society has shown that HLHS is the most common indication for heart transplantation in infants. 19 HLHS patients comprise a particularly high-risk cohort, with complex physiologic considerations (eg, Norwood or Glenn physiology) and high rates of concomitant organ dysfunction, often necessitating high levels of pretransplant support.19-21 A high incidence of HLHS in the study group may have accounted for the low rates of VAD seen in the study, although recent studies have shown single-ventricle VAD implantation to be both feasible and effective.22,23
Conclusions
A growing body of literature supports aggressive optimization of modifiable risk factors prior to pursuing transplantation, rather than simply “limping” to transplant. The end goal, then, should not simply be bridging patients to transplant but ensuring optimal post-transplant outcomes. The present analysis adds to this story by confirming that paralytic requirements and/or TPN-dependence at the time of transplant—or, more likely, the underlying organ dysfunction that necessitates their use—independently predict post-transplant mortality in infants. The findings herein suggest a role for aggressive weaning from mechanical ventilation, paralytics, and TPN-dependence before transplant, whenever possible. In some cases, the best management strategy may include delisting patients until they are physiologically ready for transplantation, although the precise group of patients who would benefit most from this strategy requires additional work. Although limited by small body habitus in infants, there may be a role for increased VAD implantation, which has been associated with improved pretransplant organ function, ventilatory weaning, and post-transplant outcomes, even in patients with single ventricle physiology. Continued quality improvement efforts and ongoing critical analyses of current clinical management strategies are necessary to improve the expectations and outcomes for the most vulnerable groups of transplant recipients.
Footnotes
Authors’ Note
All authors acknowledge full control of the study design, methods used, outcome parameters, data analysis, and production of the written report herein.
Declarations of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Morales is a consultant for Abbott, Inc., Azyio, Inc., Berlin Heart, Inc., CorMatrix, Inc., Syncardia, Inc., and Xeltis, Inc., and serves on the medical advisory board of Berlin Heart and Cormatrix. Dr. Chin is a consultant for Azurity Pharmaceutical, Inc. The remaining authors have no financial disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health; R01HL147957: “Novel Methods to Grow the Impact of Pediatric Thoracic Transplantation;” Principal Investigators: Farhan Zafar, MD, MS; David L. S. Morales, MD