
Abstract
Background
Recipients of transcatheter pulmonary valve replacement (TPVR) have shown increased risk of infective endocarditis (IE). Little is known about the outcomes of different management strategies, particularly surgery, for IE after TPVR.
Methods
We queried the Pediatric Health Information System database for cases of IE after TPVR performed from 2010-2020. We described patient demographics, hospital courses, admission complications, and treatment outcomes based on therapy offered, surgical or medical only. We compared outcomes of initial therapy. Data are expressed as median or percent.
Results
Sixty-nine cases of IE were identified, accounting for 98 related hospital admissions; 29% of patients recorded IE-related readmissions. Of those readmitted after initial medical therapy only, 33% had relapse IE. Rates of surgery were 22% during initial admission and 36% overall. Likelihood of surgical intervention increased with each subsequent admission. Renal and respiratory failure were more common in those given initial surgery. Mortality rate was 4.3% overall and 8% in the surgical cohort.
Conclusion
Initial medical therapy may result in relapses/readmissions and possible delay of surgical therapy, which appears to be most effective for treatment of IE. For those treated only medically, a more aggressive course of therapy may be more likely to prevent relapse. Mortality following surgical therapy for IE after TPVR appears higher than reported for surgical pulmonary valve replacement generally.
Introduction
Transcatheter pulmonary valve replacement (TPVR) has become an important therapy for right ventricular outflow tract pathologies since the Food and Drug Administration humanitarian device exemption of the first implant, the Medtronic Melody™ valve, in 2010. Patients with surgically corrected congenital heart disease (CHD) are key beneficiaries. Infective endocarditis (IE), however, has increasingly been recognized as a serious long-term complication of TPVR. Patients with CHD in general have an increased risk of IE, with an incidence 15 to 140 times greater than that of the general population.1,2 Risk is also increased with prosthetic heart valves, which account for a disproportionate 10% to 30% of all IE cases. 3 The combination of these risk factors in TPVR recipients therefore increases their susceptibility to IE. Annualized risk of IE after TPVR has been reported as 1.5% to 4.8% with a cumulative risk from 3% to 25%, which is perhaps a higher incidence compared to surgical pulmonary valve replacement (SPVR) that has an annual risk of 0.5% to 1.5%.4–12 As many of these patients require surgery, understanding treatment options is critical.
The role and timing of surgery for TPVR recipients with IE remains poorly understood. While findings suggest that the importance of early surgical intervention for cases with confirmed pulmonary valve involvement (ie, valve dysfunction) or minimal clinical improvement on antibiotics, the results are limited by sample size.13,14 For left-sided IE, current guidelines recommend earlier surgical management for cases with increased complications.15–18 In the general population, about 50% of IE cases—whether native or prosthetic valve—receive surgery, with preference given to high-risk groups and patients with poor recovery on medication only.19,20 Earlier surgical intervention has been linked to better outcomes such as reduced valve damage, shortened hospital stay, and improved long-term survival.17,21–23 While a recent study involving 11 patients with Melody valves suggested early surgical intervention is safe and effective for IE after TPVR, 24 it remains unclear how such results translate to larger cohorts of TPVR patients and whether management strategies for left-sided IE (eg, early surgical intervention) equally apply for these patients.
To address this knowledge gap, we used the Pediatric Health Information System (PHIS) database, which draws data from 49 tertiary pediatric institutions. The use of this database allowed us to track patients across multiple hospital admissions and gain granular insight into management strategies, ultimately allowing us to clarify patient characteristics and describe characteristics of isolated medical therapy versus surgical management.
Patients and Methods
We obtained approval from the Institutional Review Board of Washington University in St. Louis for this retrospective analysis (IRB #: 202006099).
We queried PHIS data for discharges from January 1, 2010 to September 30, 2020. International Classification of Diseases 9th and 10th Revision (ICD-9/10) procedure codes were used to extract all TPVR procedures (Supplement A). As noted in previous literature, ICD-9 code 35.26 in PHIS has been used for both SPVR and TPVR. Following the protocol described by Daily et al, code 35.26 cases were assumed to be TPVR procedures if no Operative Room Charge Flag was present and procedure code 37.23—combined right- and left-sided cardiac catheterization—was also used. 25 We then used ICD-9/10 diagnosis codes to identify all cases of IE following TPVR.
Primary data extracted included patient demographics, hospital and service dates, TPVR procedure codes and date, intensive care unit (ICU) stay, and mechanical ventilation status. For each case of IE, we identified the treatment modality using ICD-9/10 procedure codes and Clinical Transaction Classification billing codes. Hospital admission and discharge dates were used to calculate length of stay (LOS).
We extracted ICD-9/10 codes for procedures and diagnoses both before and after the index TPVR procedure from 2004 to the present. Diagnosis codes were used to identify underlying chromosomal anomalies, patient's primary CHD, risk factors for relapse, IE complications, and patient's immune status (Supplement A). We considered patients immunodeficient if diagnosed with a condition that predisposes for infection, as cataloged by the American Academy of Allergy Asthma and Immunology. 26 If no such diagnosis was made, patients were otherwise labeled as immunocompetent. We considered patients to have a history of a risk factor (eg, prior IE) if related diagnosis codes were assigned prior to their first IE-related admission.
IE-related hospital admissions were evaluated for indicators of true IE. Cases that did not have evidence of administration of empiric IE therapy or peripherally inserted central catheter (PICC) or long-term line placement prior to discharge, or lacked significant hospital stays and had diagnosis codes indicating other causes of admission, were considered admissions with uncertain IE. To perform a more conservative analysis, we thus excluded these cases from analysis. Internal validation was performed by comparing billing codes used against known IE cases at our institution. Additionally, we considered readmission after the typical window of antibiotic administration (ie, 8 weeks after IE diagnosis) to be a relapse admission.
We performed statistical analysis as follows: demographic and clinical characteristics were analyzed using mean ± standard deviation for normally distributed continuous variables and median and interquartile range (IQR) for skewed continuous variables, and counts (percentage) for categorical variables. The differences between comparison groups were assessed using 2 sample t statistics for normally distributed continuous variables and 2 sample Wilcoxon rank sum test for skewed continuous variables, and chi-square test statistics for categorical variables. We adjusted for the multiple comparisons using the false discovery rate method. Analyses were performed in SAS® version 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Cohort Admissions Overview
Our PHIS query revealed a total of 98 IE-related hospital admissions associated with 69 unique pulmonary valves (in 68 patients) after TPVR over the study period. Of the 98 total admissions, 29 were readmissions associated with IE. Fifty-four of the 69 index admissions (78%) were treated with medical therapy only and 15 (22%) received surgical intervention (Figure 1); 20/69 (29%) recorded a second admission. Among the initial 54 treated with antibiotics only and no surgical intervention, 18 (33%) were readmitted within a median 23.5 days (IQR: 12-36), with 7/18 (39%) receiving surgery during that second admission. Thirteen patients had continued medical treatment only during their second admission.
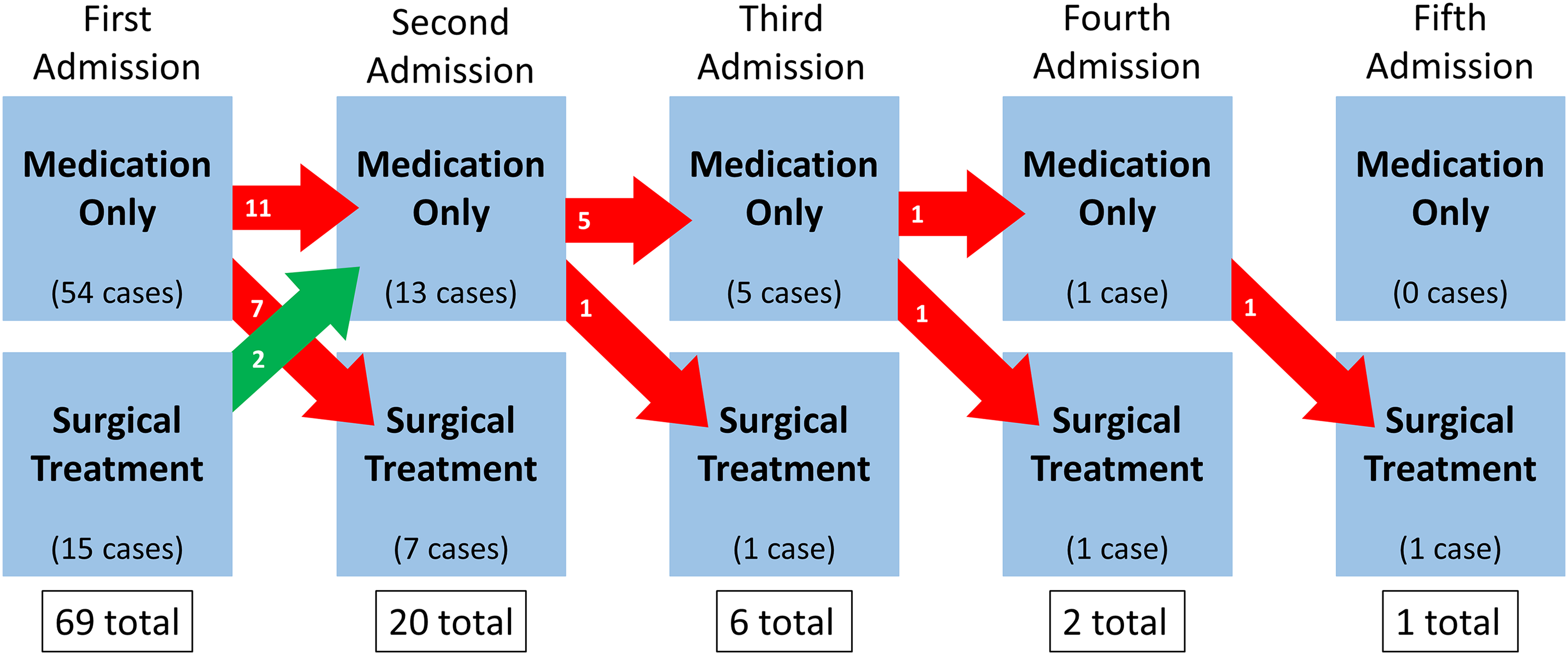
Within this cohort, 6/13 (46%) patients had a third admission, with 5 receiving medical therapy and 1 undergoing surgery; 2/5 (40%) with medical treatment during their third hospital stay went on to require a fourth admission, with 1 treated surgically. One patient recorded a fifth admission wherein he/she was treated surgically.
A single catheter-based intervention, a pulmonary valve dilatation, was performed on one patient during their index admission; however, 23 days later during the same admission, the patient received surgery.
Cohort Characteristics
Table 1 outlines characteristics of the entire cohort consisting of 69 TPVR patients who developed IE. Median patient age was 16.8 (13.2-20.9) years old, with a median valve age (time since TPVR) of 1.4 (0.4-3.2) years at the time of IE diagnosis. Fifty patients (72.5%) were male and a majority identified their race as White (41 patients, or 59.4%). Tetralogy of Fallot was the most common congenital diagnosis (27/69, 39.1%), followed by transposition of the great arteries (TGA) (10/69, 14.5%). Nineteen (27.5%) patients were immunodeficient, 14 of them had 22q11.2 deletion syndrome. Among past medical diagnoses analyzed, a history of IE in a prior valve—native or prosthetic—and gastrostomy were the most common, with 10 (14.5%) and 9 (13%), respectively. Median total hospital LOS was 13 (7-27) days, with initial admission lasting a median 9 (6-19) days. Three (4.3%) patients died across all admissions.
Cohort Characteristics.
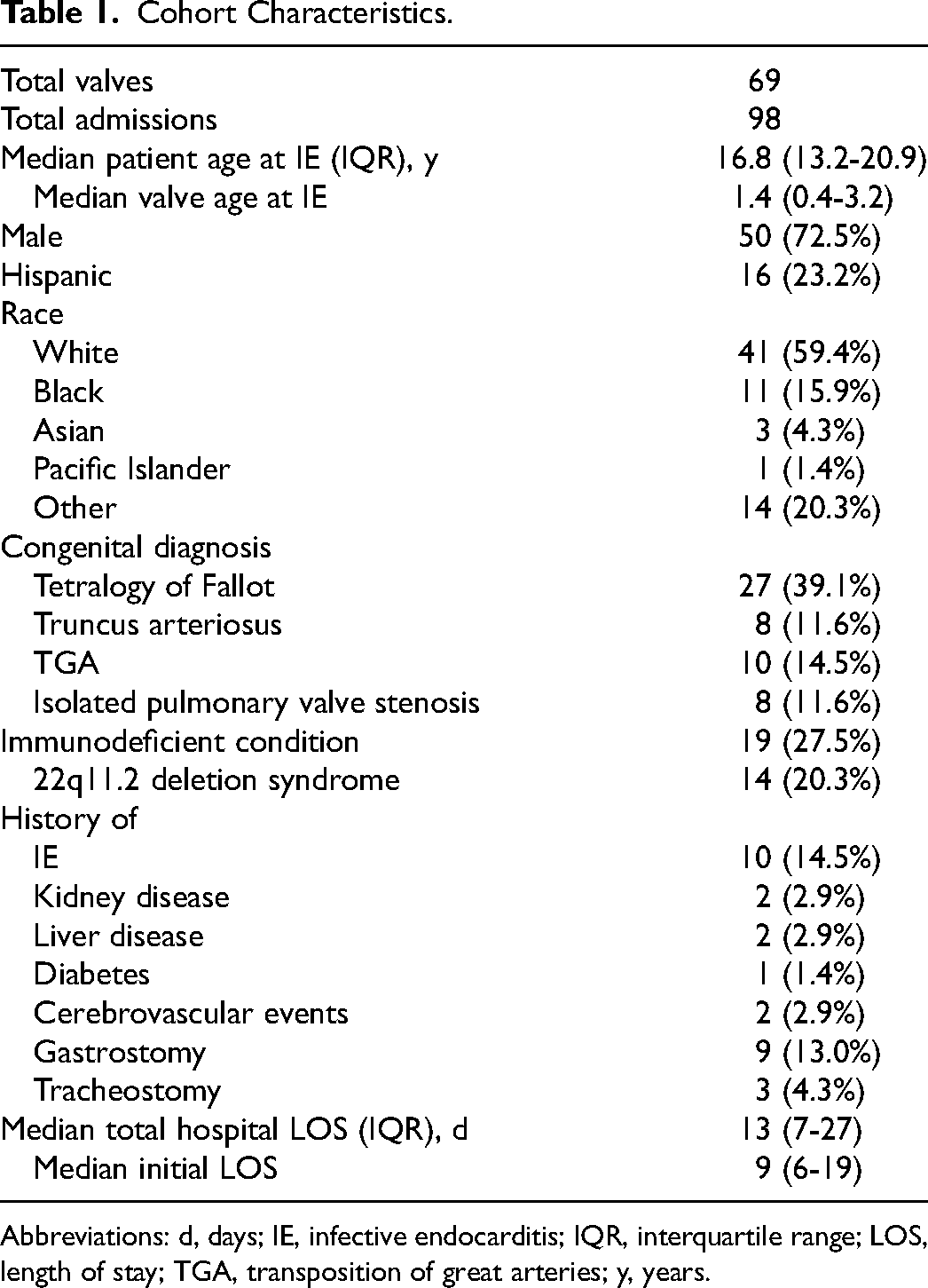
Abbreviations: d, days; IE, infective endocarditis; IQR, interquartile range; LOS, length of stay; TGA, transposition of great arteries; y, years.
Forty-five of the 69 IE cases (65.2%) had blood culture data reported the initial admission. Of those 45, 21 (46.7%) were Staphylococcus positive: 16 (35.6%) methicillin-susceptible Staphylococcus aureus (MSSA), 3 (6.7%) methicillin-resistant S aureus, and 2 (4.4%) undefined. Seventeen of 45 (37.7%) were of undefined Streptococcal origin with one specified group A and 2 (4.4%) were Enterococcus species. Of the remainder, there was 1 each of Coxiella burnetti, Haemophilus influenzae, Bartonella species, unknown Gram negative, and unknown anaerobic species. Only 13 of 29 readmissions had culture results, all of which speciated organisms consistent with previous admissions aside from 2 cases: one reported group A Streptococcus initially, then MSSA 5 months later, and the other showed an undefined Gram-negative organism followed by group A Streptococcus, a subsequent admission, notably over 4 years later.
We also considered characteristics from the 98 IE-related hospital admissions, including readmissions (Table 2). Seventy (71.4%) patients were initially admitted to the hospital floor, while 28 (28.6%) were admitted directly to the ICU. The most common admission complications were acute kidney injury (AKI) (28/98, 28.6%), respiratory failure (21/98, 21.4%), and noncerebrovascular embolism (19/98, 19.4%). Mechanical ventilation was required in 26 (26.5%) admissions for a median duration of 2 (1-4) days, while 45 (45.9%) required ICU stays lasting a median of 3 (1-8) days. Twenty-eight admissions (28.6%) resulted in further readmissions, while 67 (68.4%) did not; 3 patients died. The majority of patients, 68 (69.4%), were discharged home.
Admission Characteristics.
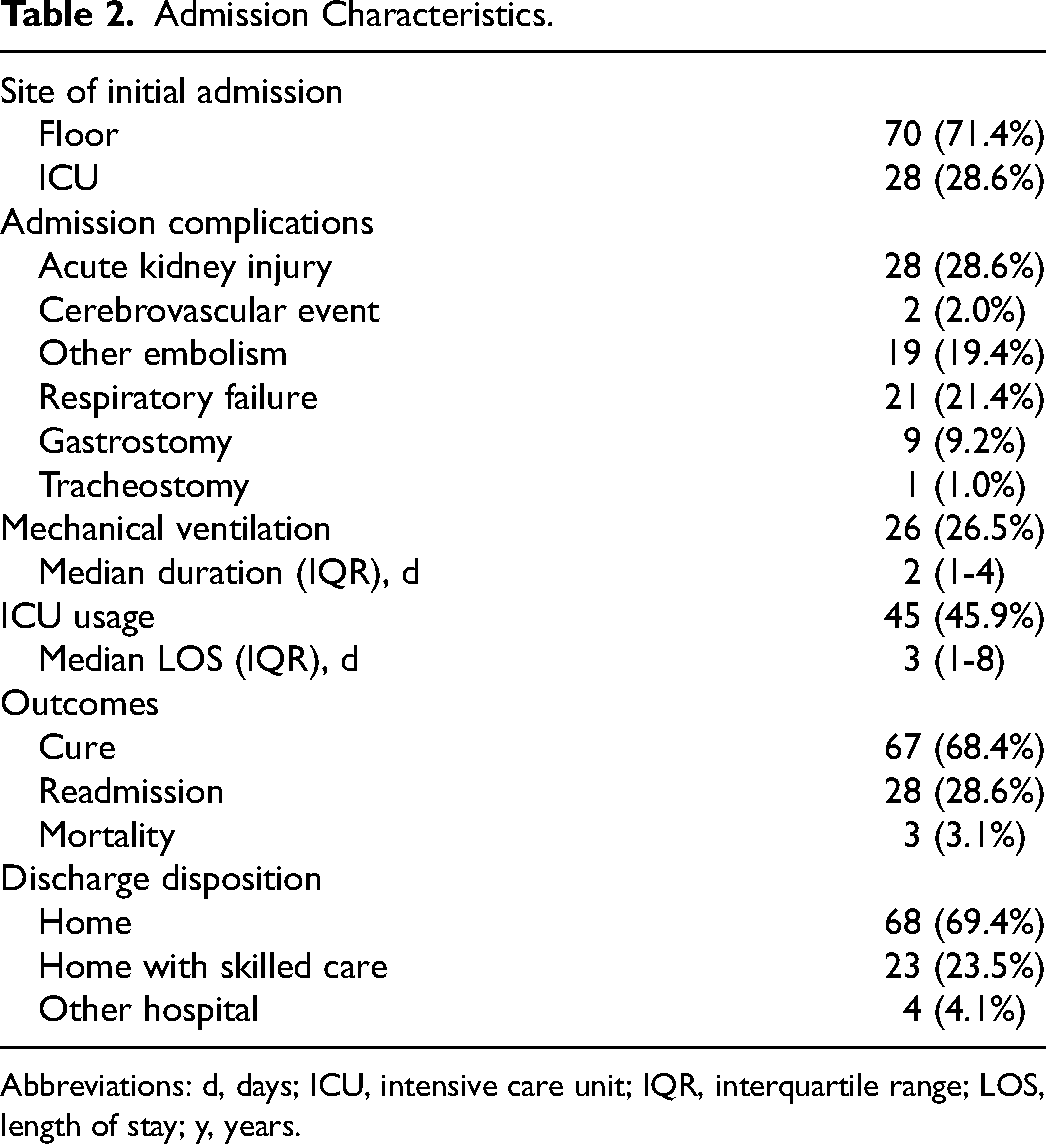
Abbreviations: d, days; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; y, years.
Comparison of Initial Therapy
We compared characteristics and outcomes of therapy offered during index admissions, shown in Table 3. The following data is described in relation to the 69 total patient cases. 54 patients received medical therapy only and 15 received surgical treatment initially. There was no statistically significant difference between the groups’ baseline characteristics of age, sex, ethnicity, or race. Although patients treated surgically during first admission had higher rates of TGA (5/15, 33.3% vs 5/54, 9.3%) than the medical therapy cohort, no significant difference existed in rates of other congenital heart diagnoses or immunodeficiency between groups. When adjusted for multiple comparisons, median total and initial hospital LOS were not significantly longer for the surgical group. Both AKI (11/15, 73.3% vs 15/54, 27.8%, P = .01) and respiratory failure (9/15, 60% vs 11/54, 20.4%, P = .02) were higher in the surgical group following adjusted analysis, likely reflective of why surgery was chosen as first-line treatment for these patients. Compared to those treated medically only, patients in the surgical group required mechanical ventilation (9/15, 60% vs 10/54, 18.5%, P = .01) and were admitted to the ICU (15/15, 100% vs 28/54, 51.9%, P = .02) more often. Notably, there was no significant difference in final discharge disposition between groups.
Comparison of Initial Therapy.
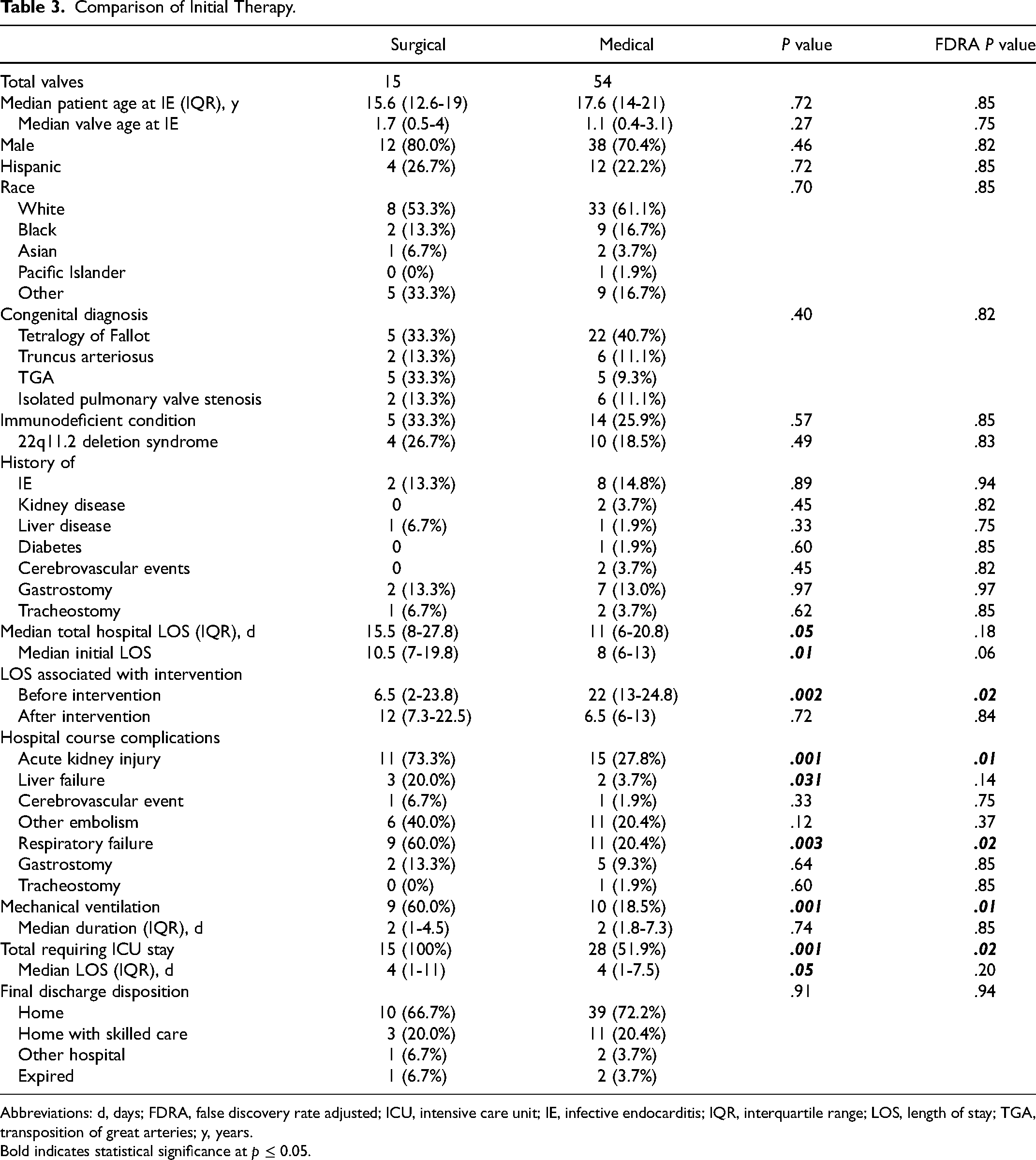
Abbreviations: d, days; FDRA, false discovery rate adjusted; ICU, intensive care unit; IE, infective endocarditis; IQR, interquartile range; LOS, length of stay; TGA, transposition of great arteries; y, years. Bold indicates statistical significance at p ≤ 0.05.
Relapse After Initial Medical Therapy Only
Out of 18 patients with readmissions after initial medical therapy, 6 (33.3%) met criteria for relapse (Supplement B) and accounted for 14 readmissions. The remaining 12 (66.7%) patients who did not meet criteria for relapse recorded 13 readmissions. Median age at IE was 19.9 (12.6-21.4) years among patients who relapsed, compared to 15.6 (10.5-19.8) years for those who did not. Details of the initial IE-related admissions compare as follows: Median hospital LOS of 6 (5.5-7.3) days for relapses compared to 11.5 (6.8-20.8) for nonrelapses; 1 (17%) patient required an ICU stay of 1 day in the relapse cohort versus 4 (33%) for nonrelapses, with a median LOS of 2 (1-7.5) days; an average of 3.5 ± 0.5 versus 5 ± 1.9 unique antibiotics administered to relapses and nonrelapses, respectively. Antibiotic regimens are detailed in Supplement B. 3/6 (50%) of the relapses and 7/12 (58.3%) of the nonrelapses went on to undergo surgery a subsequent admission.
Surgical Group
Table 4 details the characteristics, hospital course, and outcomes of the 25 valves (in 25 patients) treated surgically during any admission, described in reference to patient cases. These patients accounted for 44 total admissions. Median patient age was 15.6 (12.3-20.8) years old at the time of IE diagnosis, with a median valve age of 1.6 (0.5-3.5) years following TPVR. The majority of patients, 17 (68%), were male, and 16 (64%) identified their race as White.
Surgical Cohort.
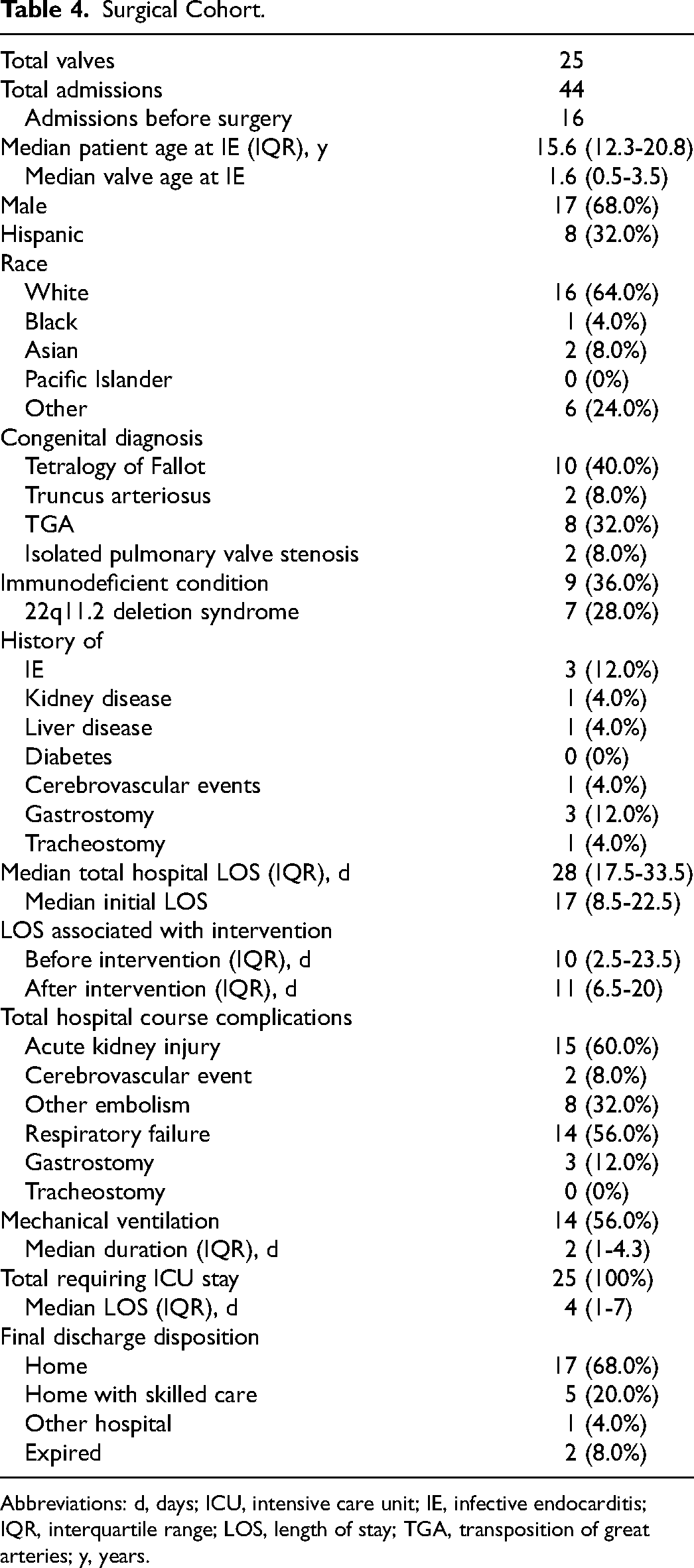
Abbreviations: d, days; ICU, intensive care unit; IE, infective endocarditis; IQR, interquartile range; LOS, length of stay; TGA, transposition of great arteries; y, years.
The most common congenital heart defect in the surgical cohort was tetralogy of Fallot (10/25, 40%) followed by TGA (8/25, 32%). Nine (36%) patients had immunodeficiencies; of them 7 (28%) had 22q11.2 deletion syndrome. Additionally, a history of IE and gastrostomy (3/25, 12% each) were the most common past medical diagnoses of relevance. Median hospital LOS was 28 (17.5-33.5) days, with a median 17 (8.5-22.5) days during the initial admission. These patients had a median LOS of 10 days prior to their surgery and 11 days after intervention.
All patients required at least 1 day of ICU stay during their hospital course, with a median of 4 days. Fourteen (56%) patients required mechanical ventilation, with a median duration of 2 days. The most common complications were as follows: 15 (60%) AKI, 14 (56%) respiratory failure, and 8 (32%) noncerebrovascular embolic events of which 7 were septic pulmonary emboli and 1 an undefined arterial embolus.
Most patients, 17 (68%), were discharged home after their final IE-related admission. Six (24%) were discharged with skilled care or to another institution and 2 (8%) died.
Comparison of Time to Surgery
Evaluating the surgical cohort based on time of surgery from IE diagnosis reveals a distribution shown in Supplement C, showing 13 patients receiving surgery before 20 days and 12 patients after 20 days, labeled ‘early’ and ‘late’ surgery, respectively. Comparison of early versus late surgery (Supplement C) demonstrates no statistically significant differences in hospital course characteristics and complications. However, the early surgical group tended toward the following: more direct admissions to ICU (46.2% vs 25%), longer LOS after surgery (13 days [8.5-28] vs 7.5 days [6-13]), increased discharges to locations other than home (38.5% vs 16.7%), and increased hospital complications including a higher average burden of the select complications evaluated (2.3 vs 1.5).
Medical Therapy Only Group
Of the 69 valves in the overall cohort, 44 (63.8%) received medical therapy only throughout their entire hospital course (Table 5). These patients accounted for a total of 54 hospital admissions. Described in relation to patient cases, median patient age was 18.3 (14.5-20.9) years, with a median valve age of 1.2 (0.3-3.1) years; 33/44 (75%) patients were male, and 23 (52.3%) identified as White.
Medical Therapy Only Cohort.
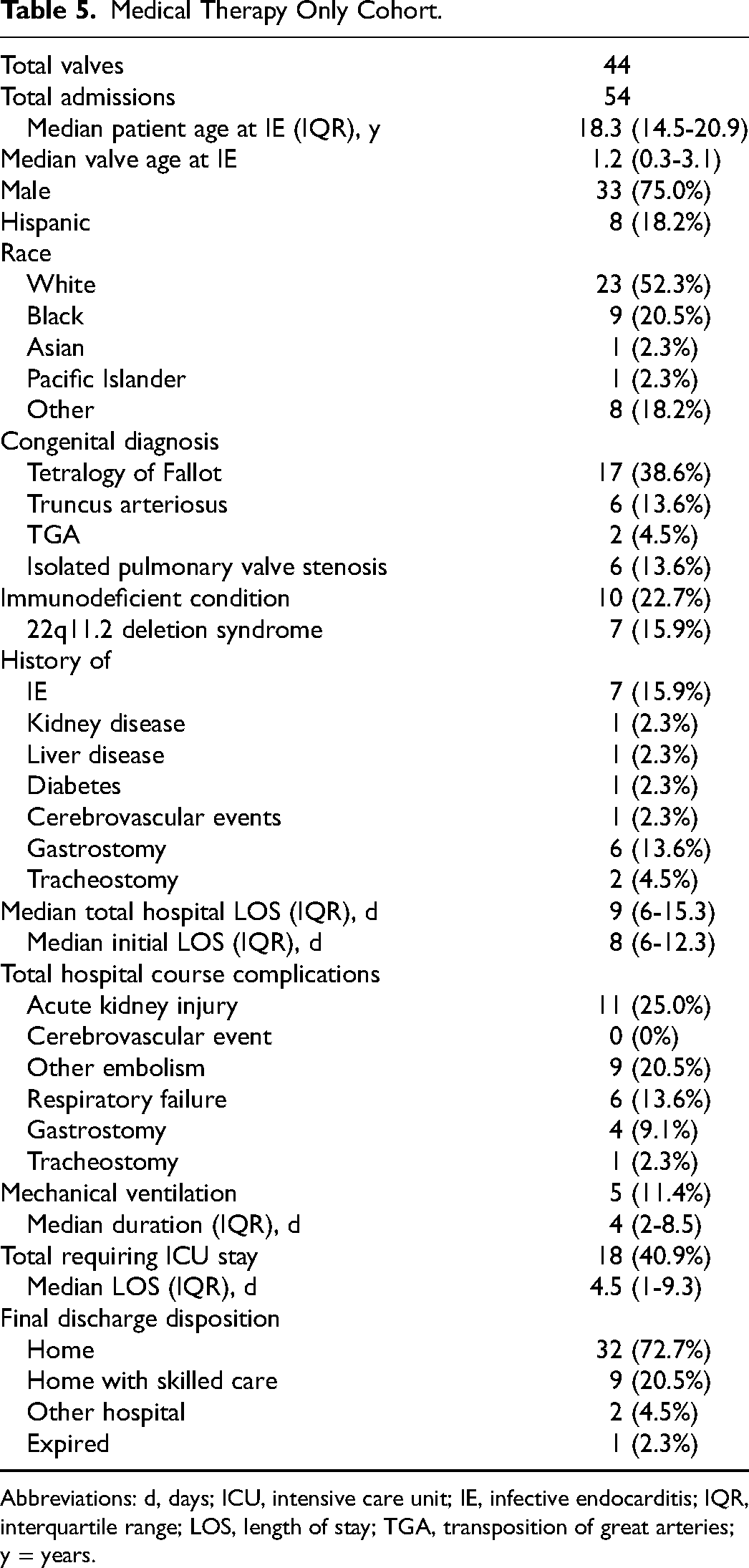
Abbreviations: d, days; ICU, intensive care unit; IE, infective endocarditis; IQR, interquartile range; LOS, length of stay; TGA, transposition of great arteries; y = years.
The most common congenital heart defect was tetralogy of Fallot (17/44, 38.6%), followed by TGA and pulmonary valve stenosis/atresia at 6 (13.6%) each. Additionally, 10 (22.7%) had conditions causing immunodeficiency, including 7 (15.9%) with 22q11.2 deletion syndrome. Seven (15.9%) had a history of IE in a previous valve prior to TPVR, and 6 (13.6%) had a history of gastrostomy.
Median total hospital LOS was 9 (6-15.3) days, with a median 8 (6-12.3) days during the initial admission. Eighteen (40.9%) patients required ICU stay for a median 4.5 days. Only 5 (11.4%) patients required mechanical ventilation, for a median of 4 (2-8.5) days. Additional notable complications included AKI in 11 (25%), respiratory failure in 6 (13.6%), and noncerebrovascular embolism in 9 (20.5%) patients of which 8 were septic pulmonary emboli and 1 an undefined arterial embolus.
Cohort Mortalities
We identified 3 mortalities. Two received medical therapy only and 1 underwent surgery during their index admissions. The first was a 20-year-old female who died during her second IE-related admission. She received medical treatment only during her initial admission of 12 days, which was devoid of recorded complications, ICU stay, and mechanical ventilation. Culture was positive for group A Streptococcus. Twenty-seven days after discharge, she was readmitted and within 24 h underwent combined emergent aortic root and SPVR with concomitant ventricular septal defect repair. This relapse was complicated by sepsis, disseminated intravascular coagulation, liver failure, kidney failure requiring dialysis, unspecified gastrointestinal bleeding, pneumonia and respiratory dysfunction requiring mechanical ventilation, cerebrovascular events requiring ventricular drain placement, and central line-associated venous thrombosis. Repeat surgical intervention involving mediastinal inspection with chest wall and diaphragm reconstruction was noted on admission day 5. Extracorporeal membrane oxygenation (ECMO) of unknown duration was also required. In total 45 days of ICU and 33 days of mechanical ventilation were recorded during LOS of 89 days. She passed away 88 days after surgery.
The second mortality was a 19-year-old male positive for DiGeorge syndrome who died after his initial IE-related hospital stay of 13 days, during which he received medical therapy only. Blood cultures were positive for MSSA. He was admitted directly to the ICU and remained there the entirety of the stay. His course was complicated by septic shock, disseminated intravascular coagulation, cardiac arrest, and multiorgan dysfunction including kidney and respiratory failure. He required dialysis and was mechanically ventilated starting day 3 of admission.
The single mortality among patients initially treated surgically was an 11-year-old DiGeorge-positive male who died within 6 days of admission. This patient had MSSA-associated IE and was admitted to the ICU within 24 h of admission. He suffered septic shock, cardiac arrest, and ventricular tachycardia during his course. He required mechanical ventilation and ECMO beginning on day 4 of admission, then received surgery the next day. He also suffered from liver and kidney failure, requiring dialysis postoperatively, and died 1 day after surgery.
Comment
In this study we describe patient characteristics, hospital courses, and treatment outcomes for cases of IE after TPVR. In a cohort of 69 patients over 98 admissions from the PHIS database, we found that over one-third (25/69, 36.2%) required surgical intervention at any time, 15 of them receiving surgery during their initial admission. 29% of patients recorded readmissions, with relapse IE being found in 33% of those patients readmitted after initial medical therapy only. There were 3 in-hospital deaths in the cohort.
Comparing initial surgical versus medical therapy revealed higher rates of AKI, respiratory failure, mechanical ventilation, and ICU usage in the surgical cohort. This suggests, perhaps intuitively, that those in the surgical cohort were sick patients experiencing more complicated hospital courses. No demographic differences were noted between groups. Interestingly, while not achieving significance, the surgical cohort also tended toward increased rates of TGA (33.3% vs 9.3%). Further studies may elucidate specific congenital heart diagnoses that predispose to severe TPVR-associated IE infections necessitating surgical intervention.
Our findings indicate that readmission is common following isolated medical therapy. After medical therapy alone, 33% of the patients experienced readmission associated with relapse IE (as defined by being outside the typical antibiotic treatment period). These patients tended to be older (19.9 vs 15.6 years), have shorter initial admissions (6 vs 11.5 days), required fewer ICU admissions (17% vs 33%), and received fewer antibiotic types (3.5 vs 5) than nonrelapse readmissions. While these findings did not reach statistical significance, likely due to the limited sample size, they perhaps suggest that patients initially receiving less aggressive antibiotic therapies—possibly due to lower disease severity on presentation—are more likely to relapse. However, it is difficult to discern elective readmission (such as for planned surgical intervention) from non-elective given the nature of the PHIS dataset. Additionally, several initial admissions were shorter than expected (eg, 3 or 4 days), which is unusual given the workup typically required for IE; all these patients were discharged home to skilled care, conceivably enabling their shortened stays. Alternatively, perhaps their workups were initiated at outside hospitals prior to transfer to an institution captured in the PHIS database.
For admissions with bacterial culture data, the findings indicate persistence of the same organism in readmissions in all but 2 cases, potentially corroborating the hypothesis that readmitted patients received insufficient antibiotic therapy initially. Additionally, the 2 instances of different bacterial species upon readmission may show that these valves are a nidus for infection from a variety of organisms, and treating one does not necessarily preclude future infection with other species.
Evaluating the impact of time to surgery on hospital course and outcomes, while failing to reach statistical significance, suggests those with earlier surgery (<20 days from diagnosis) tended to be sicker: more admitted to ICU directly, longer LOS after surgery, more discharged to skilled care or other institutions, and more complications during hospital course. Also, importantly, frequency of surgery in our cohort tended to increase with each subsequent IE-related admission aside from third admissions: 22% during first, 35% during second, 17% during third, 50% during fourth, and 100% during fifth admission. It is also notable that 5 patients were recorded for 3 admissions or more prior to surgery, perhaps highlighting less complicated disease courses or hesitancy toward invasive intervention, or else indicating an elective/semi-elective procedure down the road.
The finding of only one recorded transcatheter intervention in the setting of IE is somewhat surprising given that conduit stenosis is frequently implicated in IE.10,13,27,28 It is conceivable that our methodology of data abstraction did not capture all catheter-based interventions. Alternatively, there may indeed be some overall reluctance to proceed with catheter interventions in the setting of an infected conduit (despite presence of hemodynamic significant right ventricular outflow tract obstruction) with the potential for further embolization of infected materials into the lung.
Our cohort's overall mortality of 4.3% is less than but similar to recent data from results from McElhinney et al's cohort of 2476 TPVR patients, where the overall IE-related mortality rate was 6.6%. 9 We found a mortality rate of 8% (2 of 25 patients) in the surgical cohort, which is significantly higher than those reported for pulmonary valve or conduit replacement in the Society of Thoracic Surgeons (STS) Congenital Database STAT categories, which reports as follows: regular SPVR as STAT 1 with an average mortality of 0.2% (0.0%-0.4%), and full conduit replacement as STAT 2 at 1.6%-1.7% mortality. 29 Future analyses could indicate whether risk of SPVR is indeed much higher given the diagnosis of IE and whether such SPVR would be better suited to listing under different STAT categories.
Given the growing body of evidence suggesting an increased risk of IE after TPVR and the important role surgical therapy for IE plays, it would be worthwhile to establish a multi-institutional database to track cases and outcomes. The STS registry is a potential site that could facilitate such an endeavor. Medtronics (Dublin, Ireland), the maker of Melody™ valve, had multiple postmarket studies with the most recent ending in 2020; however, none specifically tracked outcomes of IE treatment but rather disease incidence, among other outcomes. Edwards Lifesciences (Irvine, CA), maker of the Sapien™ valve, has ongoing studies but does not appear to be specifically capturing IE treatment outcomes. Given increasing use of TPVR, capturing this data would be beneficial for clinicians and patients alike.
Limitations
Use of the PHIS database has several limitations. First, the data is derived from billing codes and relies on accurate submission by the billing coders and physicians. As such, the data may be vulnerable to coding errors and variability between institutions, which must be considered when interpreting results. 30 Second, the database is limited to all procedures and diagnoses submitted from participating pediatric institutions only, thus restricting the generalizability of the results. Third, as the database only includes administrative codes reported by constituent hospitals, it lacks clinical data such as imaging or laboratory findings; resultantly, we could not be absolutely certain a patient's source of IE was the TVPR and not other intracardiac structures or confirm the extent of valvular damage. The Exact nature of the surgical operation performed and type of prosthesis used for replacement similarly could not be verified. Additionally, the database precludes tracking patients who switch hospitals, and only accounts for mortalities occurring during patients’ hospital stay. Thus, the mortality rate for patients in our cohort is likely lower than the true mortality, as deaths occurring outside the hospital would not be captured. Lastly, it is conceivable that we missed patients who did not receive the IE ICD diagnoses yet and had clinical features of IE; hence, our estimates are likely an underestimate.
Conclusion
IE continues to be a vexing problem following TPVR. Initial medical therapy appears to result in relapses/readmissions and delay of surgical therapy, which appears to be the most effective treatment for IE. For those treated only medically, a more aggressive course of therapy may be more likely to prevent relapse. Mortality following surgical therapy for IE of infected TPVR appears to be higher than reported for SPVR. Further studies, including dedicated registries of IE cases following TPVR, would help us better understand the natural and modified history of treatments for affected patients.
Supplemental Material
sj-docx-1-pch-10.1177_21501351221129194 - Supplemental material for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement
Supplemental material, sj-docx-1-pch-10.1177_21501351221129194 for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement by J. Chancellor Fox, Horacio G. Carvajal, Fei Wan, Matthew W. Canter, Taylor C. Merritt and Pirooz Eghtesady in World Journal for Pediatric and Congenital Heart Surgery
Supplemental Material
sj-xlsx-2-pch-10.1177_21501351221129194 - Supplemental material for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement
Supplemental material, sj-xlsx-2-pch-10.1177_21501351221129194 for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement by J. Chancellor Fox, Horacio G. Carvajal, Fei Wan, Matthew W. Canter, Taylor C. Merritt and Pirooz Eghtesady in World Journal for Pediatric and Congenital Heart Surgery
Supplemental Material
sj-xlsx-3-pch-10.1177_21501351221129194 - Supplemental material for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement
Supplemental material, sj-xlsx-3-pch-10.1177_21501351221129194 for Outcomes of Treatment for Infective Endocarditis Following Transcatheter Pulmonary Valve Replacement by J. Chancellor Fox, Horacio G. Carvajal, Fei Wan, Matthew W. Canter, Taylor C. Merritt and Pirooz Eghtesady in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH T35 NHLBI Training Grant Fellowship (grant number 5 T35 HL007815).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.