
Abstract
Left ventricular pseudoaneurysm (LV-PsA) is a critical finding that could result in a fatal outcome. It may complicate myocardial infarction, cardiac surgery, trauma, or endocarditis but rarely follows pericarditis. We report a case of infectious pericarditis complicated by pericardial tamponade in an infant. After effusion drainage and medical therapy, a large LV-PsA was detected. Successful closure of the pseudoaneurysm᾽s neck was accomplished using a Gore-tex patch.
Introduction
Left ventricular pseudoaneurysm (LV-PsA) is a critical finding that could result in a fatal outcome. 1 The primary pathogenesis of LV-PsA is ventricular wall rupture that is contained through adherence of adjacent pericardium or fibrous tissue. LV-PsA may be a complication of myocardial infarction, cardiac surgery, trauma, or endocarditis. 2 Although rare, it may follow infectious pericarditis. 3 We are unaware of the latter scenario having previously been documented in infancy. In the current report, we describe the successful repair of a large LV-PsA post-pericarditis in an infant.
Case Report
A nine-month-old female infant presented with a five-day history of high fever, not responding to ampicillin–sulbactam antibiotics, with rapid breathing and poor feeding. On examination, she was tachypneic, tachycardic, and hypotensive, with congested neck veins and distant heart sounds. Chest x-ray revealed an increased cardiothoracic ratio. Emergency echocardiography demonstrated pericardial effusion with right atrial collapse consistent with tamponade. Immediate echocardiography-guided pericardiocentesis drained 170 mL of nonbloody fluid. Small amounts were drained for another four days. Computed tomography scan after initial drainage showed pericardial effusion with consolidations and mild pleural effusion (Figure 1). Blood tests demonstrated leukocytosis (WBC 18,160/μL with neutrophilia 73%); and C-reactive protein 102 mg/dL. Pericardial fluid had purulent nature with WBC (26.600/μL), polymorphs (90%), high protein content (4.29 g/dL), and low sugar (18 mg/dL). However, blood and pericardial fluid cultures did not demonstrate bacterial growth. The patient clinically improved after receiving antibiotics (vancomycin and cefotaxime) and ibuprofen, with minimal effusion on the last echocardiography before discharge.
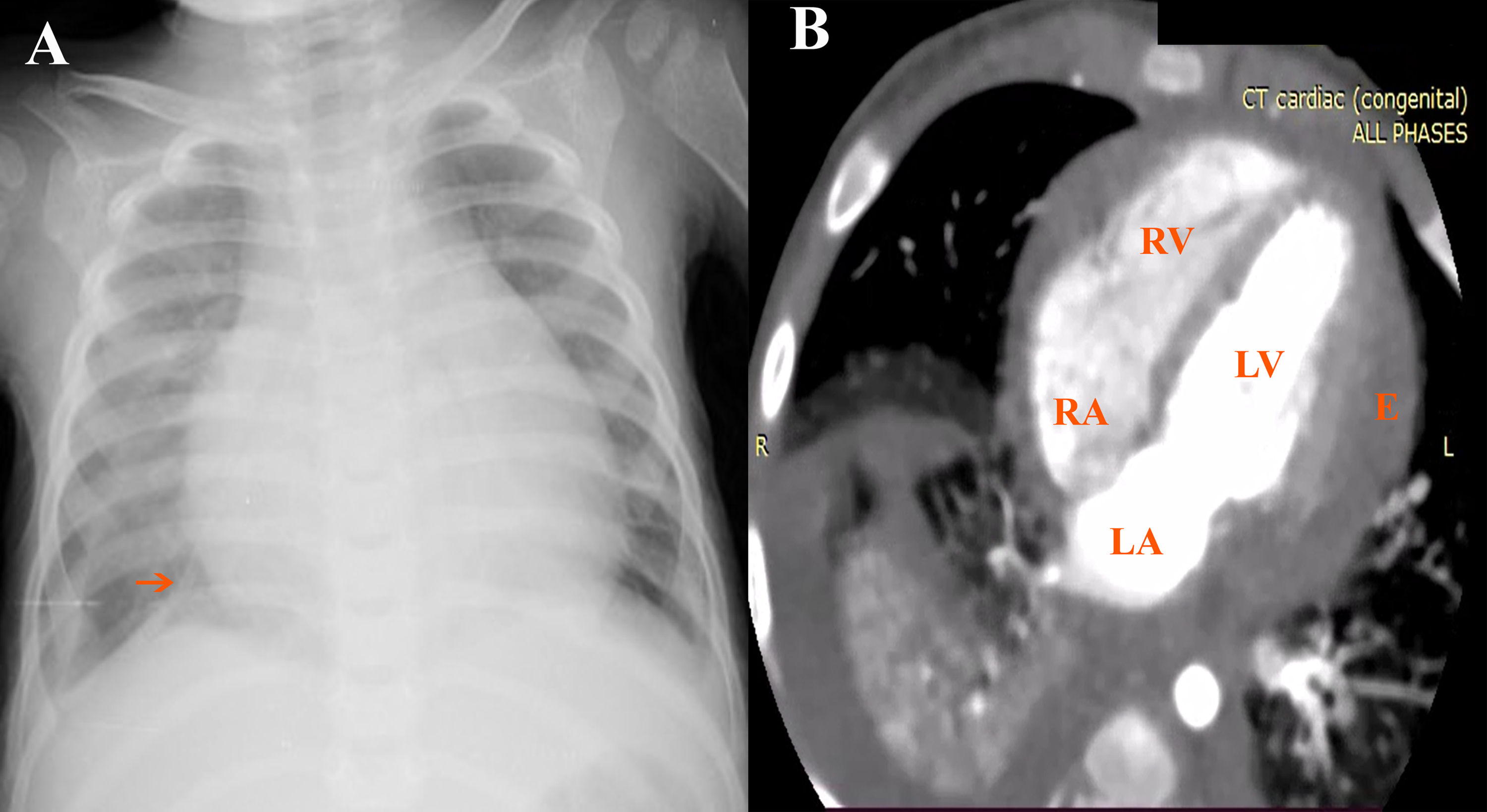
(A) Chest x-ray on initial admission revealed cardiomegaly, right lamellar effusion, and right lower segmental collapse (red arrow). (B) Computed tomography (CT) chest and heart axial view showing pericardial effusion and consolidations. E, effusion.
Two weeks following discharge, the effusion had completely resolved, and ibuprofen was stopped. However, follow-up echocardiography six weeks after pericardiocentesis revealed new moderate mitral regurgitation and an echo-free lesion posterior to the LV (Figure 2 and See Online Movie 1). Despite these new findings, the patient was asymptomatic. Cardiac magnetic resonance imaging (MRI) confirmed a large well-circumscribed pseudoaneurysm measuring 4.3 cm × 3.5 cm connected to the LV just below the mitral valve, with a 1.5-cm wide neck and without evidence of thrombosis. Delayed gadolinium peripheral enhancement was evident without myocardial continuity in the LV-PsA wall starting at the neck edges (Figure 3 and See Online Movie 2).
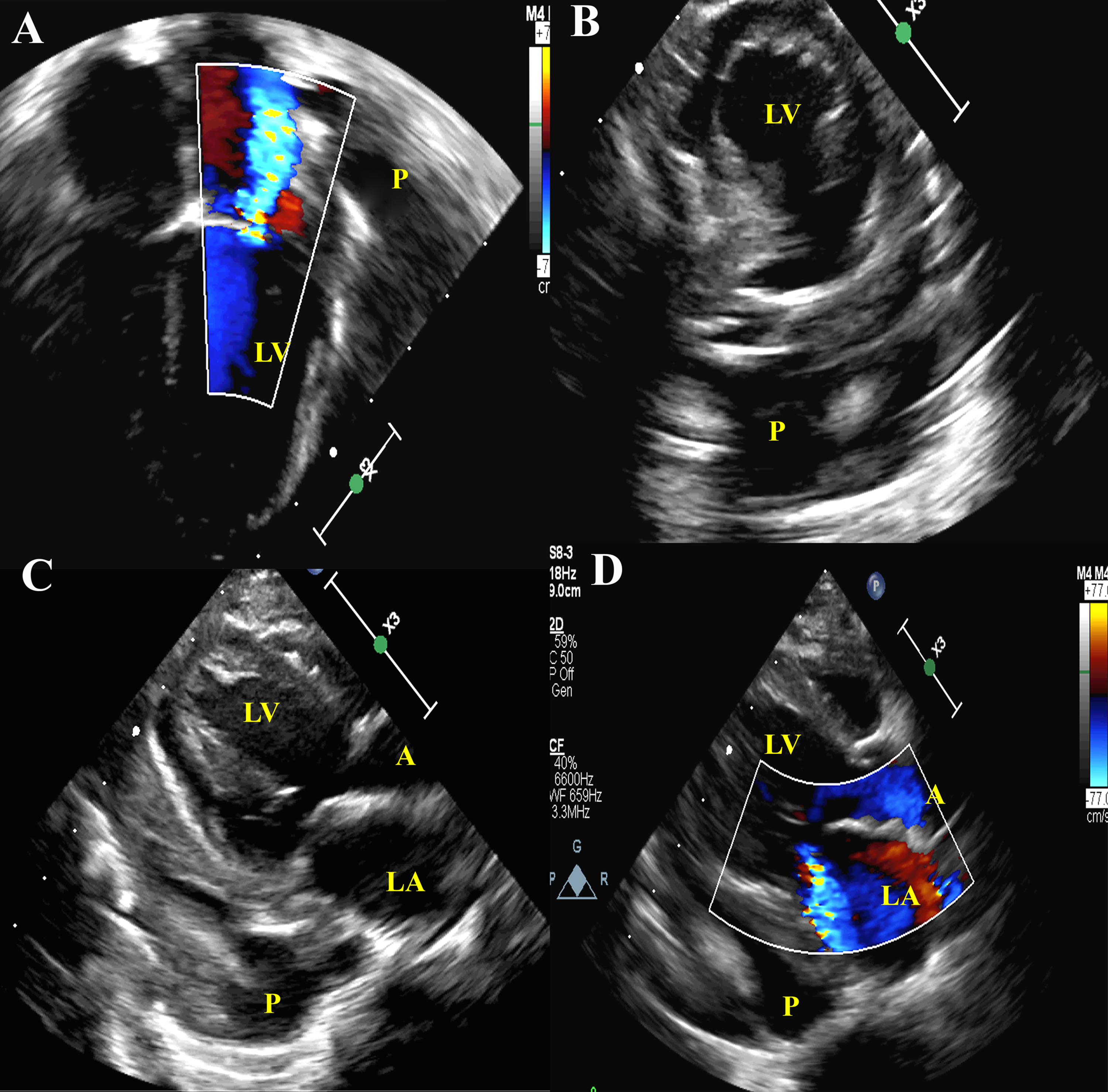
Transthoracic echocardiography (A) Color flow four-chamber view showing mitral regurgitation and echo-free area posterior to left atrioventricular junction. (B) Short parasternal view demonstrates pseudoaneurysm. (C and D) Two-dimensional and Color Doppler long parasternal view, showing mitral regurgitation and pseudoaneurysm posterior to left ventricle (LV). A, aorta; P, pseudoaneurysm.
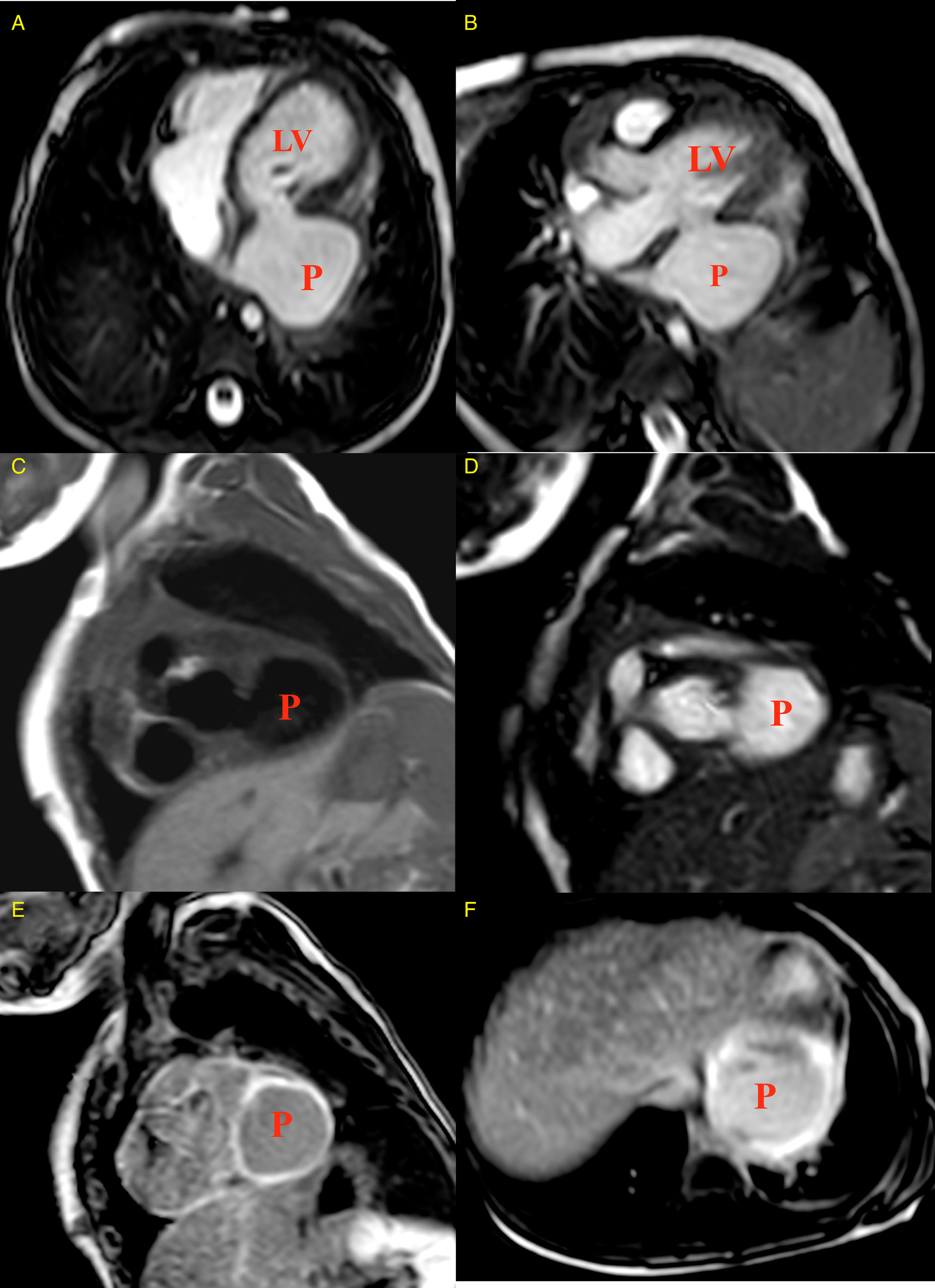
Cardiac magnetic resonance imaging (MRI). (A and B) Cine SSFP axial four- and three-chamber views show large saccular pseudoaneurysm arising posterolaterally below mitral apparatus. (C and D) T2 Black blood and Cine SSFP sequence of short-axis view demonstrate large pseudoaneurysm. (E and F) Gadolinium-enhanced MRI short-axis and axial views showing diffuse pericardial enhancement with the enhancement of pseudoaneurysm wall. P, pseudoaneurysm.
Regarding etiology of the pseudoaneurysm, the possibility of trauma during pericardiocentesis was considered. However, the drainage was echo-guided, and the wire was not advanced beyond the apex. Moreover, the absence of evident bleeding in pericardial fluid and the latent period between drainage and pseudoaneurysm detection do not suggest traumatic etiology.
The patient was operated through a median sternotomy. After the institution of cardiopulmonary bypass, extensive fibrous adhesions between pericardium and LV-PsA were dissected. The LV-PsA was opened with suction of contents. The neck was detected close to the posterior mitral leaflet. The sac was excised and the neck was closed using a patch of Gore-Tex (W. L. Gore and Associates, Flagstaff, Arizona) secured with pledgeted sutures of polypropylene (Figure 4 and See Online Movies 3-5). She was extubated on the day of the operation with a smooth postoperative course and discharged eight days later. Pathologic examination of the sac confirmed the absence of myocardial tissue with the fibrous nature of the pseudoaneurysm. One month postoperative, echocardiography revealed regressing mitral regurgitation with good systolic function. On the last follow-up at 12 months, the patient was stable with no recurrence and no residual mitral regurgitation.

Surgical repair of left ventricle (LV) pseudoaneurysm. (A) Large pseudoaneurysm related to posterior LV. (B) Pseudoaneurysm was opened, showing the neck communicating to LV. (C) Mitral papillary muscles could be seen from pseudoaneurysm's neck. (D) Gore-Tex patch was used to close pseudoaneurysm's neck.
Discussion
Pericarditis may lead to hemodynamic compromise and mortality. However, LV-PsA is a rarely reported complication of infectious pericarditis. Staphylococcus aureus was the commonest microorganism detected in 52% of previously reported LV-PsA postinfectious pericarditis cases. 4 Hypotheses suggested to explain the development of postinfectious pericarditis pseudoaneurysm include a direct spread of infection from the pericardium or myocardial abscess formation that gradually perforates the ventricular wall and is contained within thickened pericardium or fibrous tissue.3,5
Several reports describe post-pericarditis LV-PsA in adulthood and childhood. Juliana et al reported postinfectious pericarditis LV-PsA in a six-year-old girl. Accompanying literature review included 12 other cases of LV-PsA after purulent peri/pancarditis in children aged 1.5 to 13 years. All childhood cases reviewed were Staphylococcus aureus–related except two patients were Mycobacterium tuberculosis–related and another one was related to varicella-zoster, the latter being the only mortality among children in the reviewed reports. 4 A unique aspect of our case is the infantile presentation of postinfectious pericarditis LV-PsA following tamponade with successful surgery and no recurrence. In the current report, although cultures had no growth (likely related to antibiotics received before admission), the combination of fever, leukocytosis, high acute-phase reactant, the exudative nature of the pericardial effusion, and response to effusion drainage and antibiotics support infectious nature of the pericarditis.
Most reported instances of LV-PsA as a sequel of infectious pericarditis are located in the posterolateral (submitral) region. It was suggested that because hospitalized patients are usually in recumbent position, an inflammatory reaction of posterior pericardium may result in pericardial adhesions and a posterior LV-PsA formation. 2
Differentiation between LV-PsA and true ventricular aneurysm is challenging, yet it is mandatory to determine when a patient is eligible for surgery. For pseudoaneurysm, urgent repair for fear of rupture is the rule, while management of true aneurysm can be more conservative. LV-PsA is more likely when the neck is narrow, contains thrombus, and when MRI reveals pericardial enhancement without myocardial tissue, while thinned myocardium is detected in true aneurysm. Although conventional echocardiography is helpful in preliminary diagnosis, cardiac MRI is a superior confirmatory tool. 6
Surgical closure of the neck of an LV-PsA following infectious pericarditis can be performed in childhood using a Gore-tex patch 3 as in our case, or using autologous pericardium, 7 bovine pericardium, 8 or direct pledgeted suture in LV-PsA with very small neck. Despite the possible fatal outcome of postinfective endocarditis LV-PsA, the prognosis of LV-PsA secondary to pericarditis is more favorable without reported recurrences in cases with timely surgical management. 1
Conclusion
LV-PsA is a rare complication of infectious pericarditis that we have observed and managed in infancy. Timely surgical intervention with closure of the submitral pseudoaneurysm neck can result in a favorable outcome without recurrence.
Footnotes
Authors' Statement
Parental consent was obtained for submission and publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.