
Abstract
We present historical accounts of congenital heart surgery since the early 1900s, as our specialty evolved from individual heroic efforts into an established and sophisticated surgical specialty with consistent and excellent results. We highlight colleagues and intrepid pioneers who have strived to solve seemingly insurmountable problems during this remarkable journey and celebrate continued success into the 21st century with surgical advances that have resulted in innovative operations, database inquiries, quality measures, new techniques of medical illustration, and the establishment of the Congenital Heart Surgeons’ Society, which has become the leading organization dedicated to congenital heart surgery in North America.
“Innovation doesn’t occur in a vacuum. Doers and thinkers from Shakespeare to Jobs, liberally ‘stole’ inspiration from the doers and thinkers who came before….‘If I have seen further,’ Isaac Newton wrote in a 1675 letter to fellow scientist Robert Hooke, ‘it is by standing on the shoulders of giants.’ It can be easy to look at great geniuses like Newton and imagine that their ideas and work came solely out of their minds, that they spun it from their own thoughts—that they were true originals. But that is rarely the case. Innovative ideas have to come from somewhere. No matter how unique or unprecedented a work seems, dig a little deeper and you will always find that the creator stood on someone else's shoulders. They mastered the best of what other people had already figured out, then made that expertise their own. With each iteration, they could see a little further, and they were content in the knowledge that future generations would, in turn, stand on their shoulders. Standing on the shoulders of giants is a necessary part of creativity, innovation, and development. It doesn’t make what you do less valuable. Embrace it.” From Farnum Street Blog. Standing on the shoulders of giants. https://fs.blog/shoulders-of-giants/
Introduction
In celebration of the 50th anniversary of the founding of the Congenital Heart Surgeons’ Society (CHSS), we note herein the many momentous contributions to our specialty both before and after the founding of CHSS. The particulars of the CHSS founding and subsequent interim advances are chronicled in two previously published articles,1,2 while we explore events and individuals who have established our specialty from the very beginning and into the era of CHSS. So, how did we get here? Who got us here? What did they do? Let's explore. The founding members of the CHSS, 1 along with subsequent members, played a major role in the development of our specialty of pediatric and congenital heart surgery.
Congenital heart surgery is a medical discipline that has been steeped in Aristotelean principles 3 that include courage, tenacity, intrepidity, justice, and practical wisdom. 4 Since the early 1900s, during many of our own lifetimes, we have witnessed the progression and evolution of pediatric cardiac surgery from epic efforts into an established and sophisticated specialty with excellent outcomes and few limits regarding complex cardiac pathology or patient age.
The beginnings and raison d’etre for cardiac surgery were primarily to treat pediatric congenital anomalies that were approached initially using closed extracardiac procedures and followed by intracardiac procedures when techniques were developed to support the patient's circulation by induced deep hypothermia, cross circulation, and cardiopulmonary bypass (Table 1). 4 These courageous, intrepid, and ingenious applications of technology and human technical skill paved the way for advances to treat adult-acquired heart disease. While the development of congenital heart surgery was a continuum of advances and discovery, some eras stand out including closed extracardiac operations, the subsequent era of closed or semiclosed intracardiac operations, the initial stages of complete intracardiac repair, the succeeding and most recent period that introduced new operations, the intensive care unit, cardioplegic arrest, expansion of the field to the correction or palliation of virtually any type of congenital heart disease, and ultimately, the era of advanced medical illustration that formed the basis of generalized surgical education. 5 The authors would like to note that much of this historical account is based on a previous publication regarding milestones of congenital heart surgery. 4
Chronological Sequence of Major Contributions to the Development of the Field of Congenital Heart Surgery.
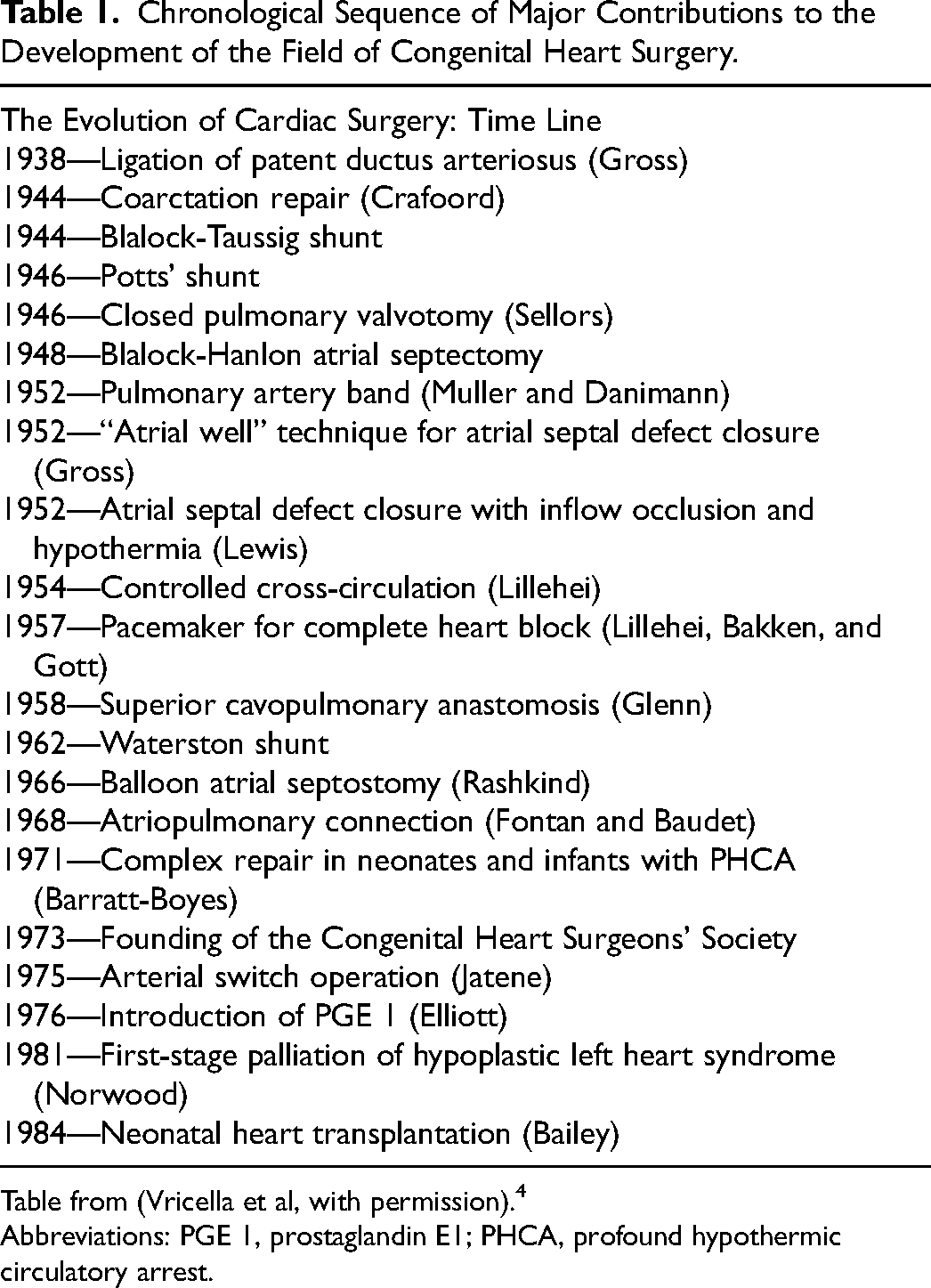
Table from (Vricella et al, with permission). 4
Abbreviations: PGE 1, prostaglandin E1; PHCA, profound hypothermic circulatory arrest.
The Beginnings of Cardiac Surgery
The early days of transthoracic procedures permitted exposure for surgeons to repair simple cardiovascular malformations and was a natural initial surgical entry into subsequent eras and frontiers of cardiac surgery.6,7 While these conditions were anatomically simple, patient selection complicated by extracardiac conditions often made the operations more complex and challenging. The threat of infection in the preantibiotic era as well as undiagnosed pulmonary hypertension often made these initial attempts unsuccessful. 8 These associated lesions were demonstrated in the first case of surgical ligation of a patent ductus arteriosus (PDA) in a 22-year-old patient with known bacterial endocarditis on March 6, 1937, in Boston by John Strieder. While the operation was initially effective with disappearance of the vascular thrill by palpation, the patient succumbed to generalized sepsis on the fourth postoperative day. Necropsy showed large septic vegetation, extending from the arterial duct to the level of the pulmonary valve. 8
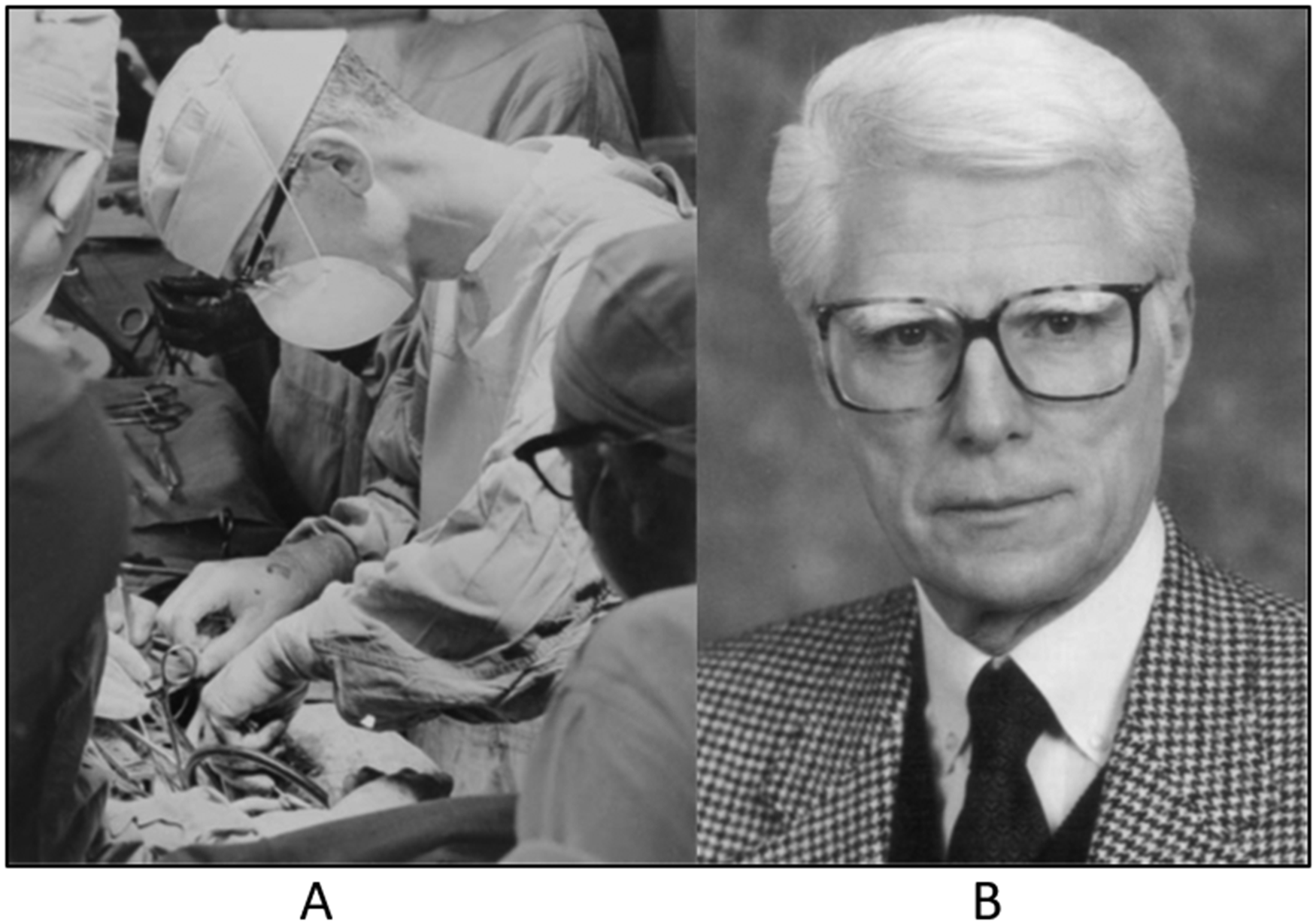
Gross (Figure 1A) is credited with the first successful congenital heart operation by ligating a PDA at Boston Children's Hospital on August 26, 1938.9,10 Interestingly, he was the chief resident at the time and was presented with a very sick seven-year-old child with pulmonary overcirculation. He performed the PDA ligation against the advice of his chairman William Ladd11,12 who was in Europe at the time. Nowadays, this act of insubordination would hardly be tolerated. However, the year was 1938. It was a different time. Physicians were observing multiple deaths caused by pathologic conditions that seemingly could be surgically approached with a reasonable chance of a lifesaving outcome. At least, that is the way that we might look at this in today's world. However, one must imagine the angst and uncertainty that Gross must have experienced knowing that failure might cause his patient's death and “bring hell down from on high” from Dr William Ladd upon his return from Europe. As it turned out, the patient had an uneventful recovery, was discharged in ten days, and survived for many years. Many years after this report, Kaemmerer and associates 13 discovered that Emil Karl Frey, a surgeon at the Medizinische Akademie in Düsseldorf, Germany, had already ligated a PDA successfully, but did not publish the results, wanting to gain more experience and report a series of patients and not just one case report. Nevertheless, Gross's landmark operation and contribution demonstrated that a curative intervention on the great vessels within the depths of the thoracic cavity was possible.
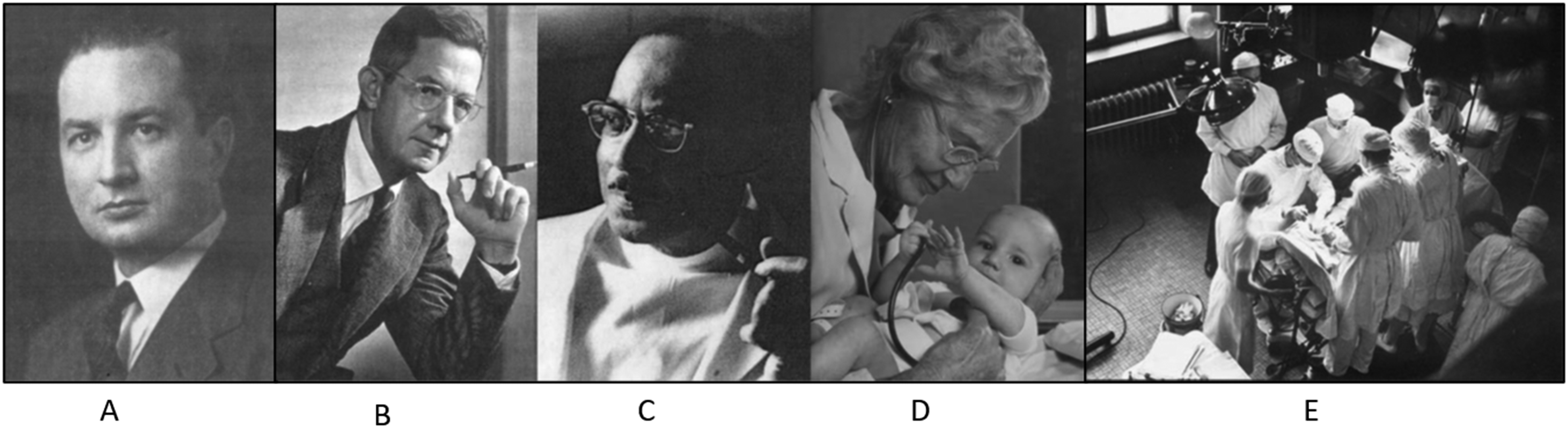
(A) Robert E. Gross (1905-1988), protagonists of the first systemic-to-pulmonary shunt on November 29, 1944, at the Johns Hopkins Hospital (From Westaby, with permission) 10 ; (B) Alfred Blalock (1890-1964) (Copyright estate of Yousuf Karsh, Courtesy of Johns Hopkins University Photographic Archives); (C) Vivien Thomas (1910-1985) (Courtesy of the Johns Hopkins University photographic archives); and (D) Helen Taussig (1898-1986) (Copyright estate of Yousuf Karsh, Courtesy of Johns Hopkins University Photographic Archives). (E) One of the first “blue baby” operations at the Johns Hopkins Hospital, circa 1945. In the center of the photograph, to the left of the operating table, Dr Alfred Blalock. Behind him, Vivien Thomas, and, to his left, the then chief resident Dr William Longmire. Standing as first assistant, opposite to Dr Blalock, is the assistant resident, Dr Denton Cooley (Courtesy of the Johns Hopkins University photographic archives).
Historically and anatomically, it made sense that the next challenge was repair of coarctation of the aorta. Blalock was the first to attempt correction of coarctation of the aorta in a canine model in 1944, by dividing the aorta in the presumed area of the isthmus and turning down the distally transected left subclavian artery and anastomosing the vessel to the proximal descending aorta (Blalock-Park procedure). 14 The experiments were conducted in Dr Blalock's laboratory in a comprehensive manner to include postoperative neurologic and hemodynamic results. The authors discovered an unfortunately high rate of paraplegia likely caused by long clamp times, which limited flow through a normal-caliber subclavian artery and poor collateral circulation. Nevertheless, the authors started the inquiry and hemodynamic approach to this significant problem.
In related inquiries and results, Crafoord and Nylin routinely clamped the aorta during ligation of the arterial duct, which emboldened him to move further with these results to perform the first reported coarctation repair with end-to-end anastomosis in two patients who were operated at the Karolinska Institute in 1944. 15 Gross et al reported a case of successful coarctation repair shortly thereafter in 1945 16 and was first in addressing this malformation with an interposition homograft in 1949. 17 While these initial interventions and contributions were thought to be curative, long-term outcomes were not assessed.
Scientific inquiries were expanded to include the dismal outlook for children with complex cyanotic congenital heart disease. Diagnostic tools in the middle 1940s other than clinical examination, the stethoscope, chest roentgenography, and electrocardiography were unavailable and added to the uncertainty of preoperative diagnosis and operative planning. At Johns Hopkins University (Figure 1B-D), Helen Taussig established the congenital heart service and with only the diagnostic tools available to her, she followed children in her clinic while administering to their needs as best that she could under the circumstances. When the children passed away from their disease process, she performed necropsies thereby completing the clinicopathologic analysis. She was able to characterize their anomalies into broad anatomic categories that offered a chance to consider methods for stable palliation for cyanotic patients. The idea of creating an “artificial ductus arteriosus” was appealing but was thought to be unrealistic by Gross. It remained for Taussig to approach Blalock, the newly appointed chief of surgery at the Johns Hopkins Hospital. Blalock had previously established an experimental animal laboratory at Vanderbilt University in Nashville with Vivien Thomas (Figure 1C), his laboratory technician who accompanied him to Baltimore. Blalock and Thomas established an experimental model of pulmonary hypertension that consisted of ligation of the left pulmonary artery and anastomosis between the left subclavian and left branch pulmonary arteries. 18 The idea was that increased pulmonary flow would cause reactive pulmonary hypertension. They were unable, however, to augment pulmonary pressure because of the low impedance of the pulmonary vascular bed. Unexpected and seemingly unwanted consequences proved to be a benefit for using this operative procedure to increase pulmonary artery flow in cyanotic children. The idea was introduced to a child with severe cyanosis on November 29, 1944, when Blalock successfully performed the first systemic-to-pulmonary artery shunt. This momentous clinical advance established the role of long-term palliation for cyanotic patients (Figure 1E).19,20 The patient, a 16-month-old with pulmonary stenosis, weighed only 4 kg having had a premature birth weight of 1.1 kg.
The following years ushered in several modifications of the systemic to pulmonary artery shunt and included an anastomosis of the descending aorta to the left pulmonary artery (Potts shunt) 21 reported in 1946 and of the ascending aorta to the right pulmonary artery (Waterston shunt) reported in 1962. 22 These approaches often proved to be unreliable in regulating pulmonary blood flow and were extraordinarily difficult to control at the time of late complete intracardiac repair. Consequently, these operations were eventually abandoned after the introduction of the modified Blalock-Taussig shunt by Marc de Leval, 23 which proved to be predictable and dependable. Initially, this shunt was employed for cyanotic patients who were better thought to be palliated owing to low-birth-weight individuals, abnormal coronary artery distribution, and complex anatomy; the idea being that the patient would be a more appropriate candidate for complete repair at a later date after weight gain. The shift toward neonatal complete repair in patients with two adequate ventricles resulted in fewer initial palliative procedures. However, the introduction of staged repair of univentricular heart disease depended on the temporary use of systemic to pulmonary artery shunts for decreased pulmonary flow (cyanosis)23–29 or pulmonary artery band for pulmonary overcirculation. Pulmonary artery banding had a similar historical development except that it was introduced for pulmonary overcirculation and not cyanosis. Patients with congenital anomalies characterized by left-to-right shunting, pulmonary overcirculation, and pulmonary hypertension were initially treated by pulmonary arterial banding, which was first introduced by Muller and Danimann in 1952. 24 Although rarely utilized in biventricular hearts nowadays, pulmonary arterial banding still has a role in the initial staging of cardiac malformations characterized by univentricular morphology and pulmonary overcirculation. Of some historical personal interest, Dr Muller was Chairman of Surgery at the University of Virginia School of Medicine at the time that one of us (CM) was a medical student there. Imagine being that close to history! Over the succeeding decades, systemic-to-pulmonary shunts became the basis of palliation for univentricular heart disease. Extracardiac palliative procedures are now generally performed as the foundational step toward the attainment of complete right heart bypass, the Fontan circulation (Figure 2).10,25–31
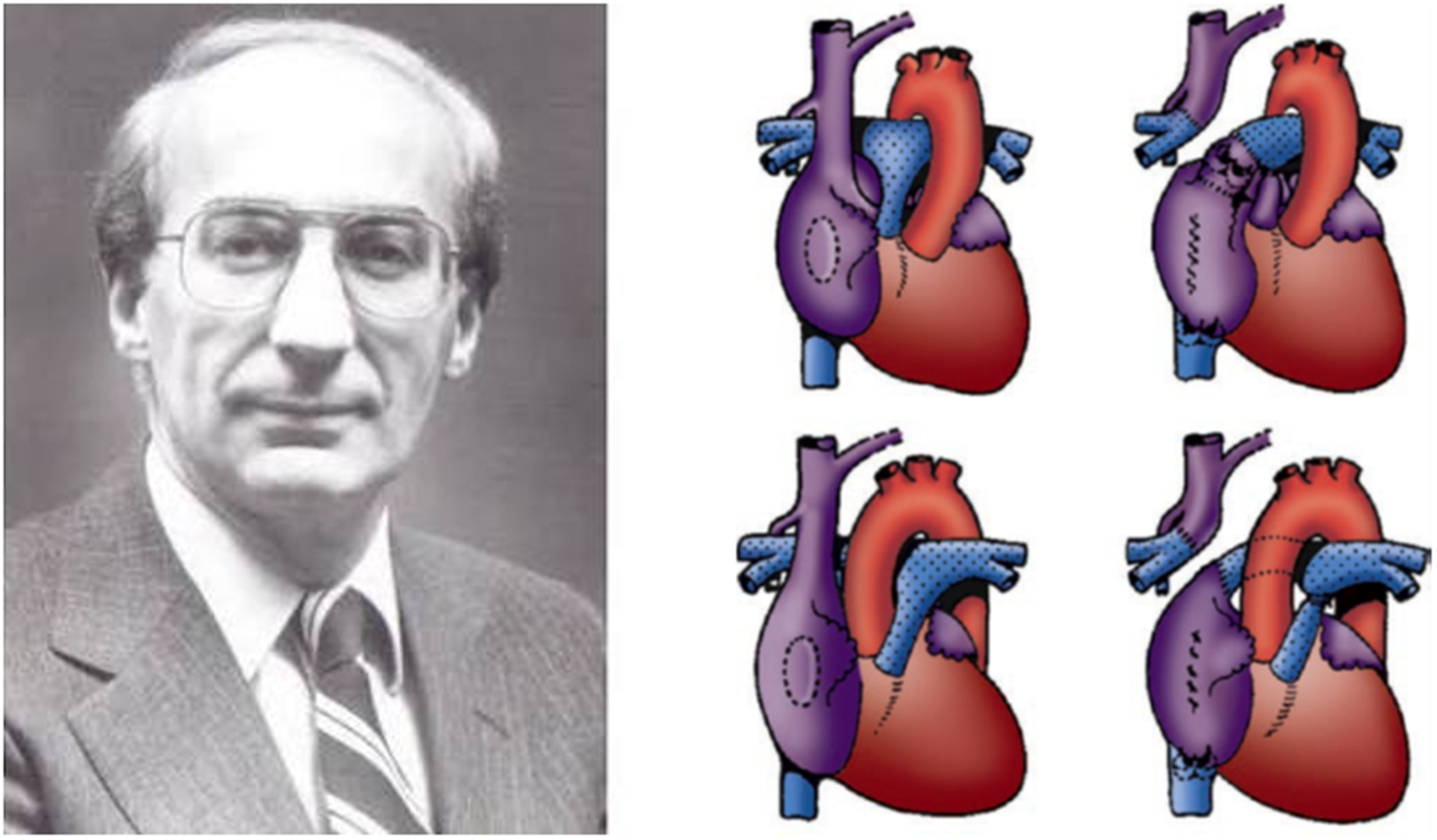
(A) Francis Maurice Fontan (Reproduced from Westaby, with permission). 10 (B) Illustration from the original 1971 article detailing a novel surgical approach to tricuspid atresia and univentricular heart disease. Atriopulmonary connection with (upper panel) and without (lower panel) interposition of a valved homograft (Reproduced from Fontan and Baudet). 26
Intracardiac Operations by Early Closed or Semiclosed Methods
The initial attempts at closed intracardiac intervention were performed for cyanotic patients with pulmonic stenosis. Sellors of London reported the first successful transventricular pulmonary valvotomy in December 1946. 32 His original intent at therapy was to perform a systemic-to-pulmonary shunt for his patient with tetralogy of Fallot, but the chronic sequelae of tuberculosis made this initial plan unachievable since pulmonary adhesions prohibited dissection of the brachiocephalic vessels. This novel approach was subsequently embraced by Lord Brock at Guy's Hospital and became the standard practice for pulmonic stenosis for much of the following decade. This procedure was later outdated and replaced by open valvotomy using cardiopulmonary bypass. Eventually, the more often utilized percutaneous balloon valvotomy, first introduced in 1982 by Jean Kan and colleagues at the Johns Hopkins Hospital became the procedure of choice. 33
The initial intrepid advances and successes with palliative and closed procedures resulted in improved survival and quality of life for those patients with certain types of congenital heart disease amenable to these innovative techniques. These patients who benefited would most likely have had early deaths. 34 These advances were followed by more creative techniques that addressed other lesions such as atrial septal defects (ASDs). Partially successful attempts for ASD closure with the external suturing technique were described by Murray in 1948. 35 In 1952, Gross and colleagues reported the creative use of an “atrial well” to close ASDs. 36 They temporarily attached a cone-shaped rubber funnel to the right atrial wall so blood could rise up into the rubber “well” (Figure 3A), 10 allowing the surgeon to find the defect by palpation and repair it by primary suture technique without direct visualization. Although the technique was quite rudimentary and imperfect, Kirklin and colleagues in 1956 reported a series of 29 patients undergoing successful ASD closure with the atrial well technique and without operative mortality. 37 Kirklin was one of the founding members of the CHSS. His numerous scientific inquiries would solidify his legacy as one of the founding fathers of congenital heart surgery (see article on Kirklin in this issue). In addition to ASD closure, the “atrial well” could also be employed to create an interatrial communication in patients with cyanotic lesions characterized by poor mixing. Another and more reliable method of atrial septectomy was described by Hanlon and Blalock in 1948, 38 a semiclosed technique that was performed by temporary occlusion of the right pulmonary artery and veins and applied with an appropriately designed clamp (Figure 3B and C)10,39 at Sondergaard's groove that isolated a portion of the right and left atria. The dorsal and right-lateral portion of the interatrial septum could then be excised, and the interatrial groove closed primarily. These technically challenging operations40,41 were eventually replaced by the introduction of balloon septostomy by Rashkind and Miller in 1966. 42
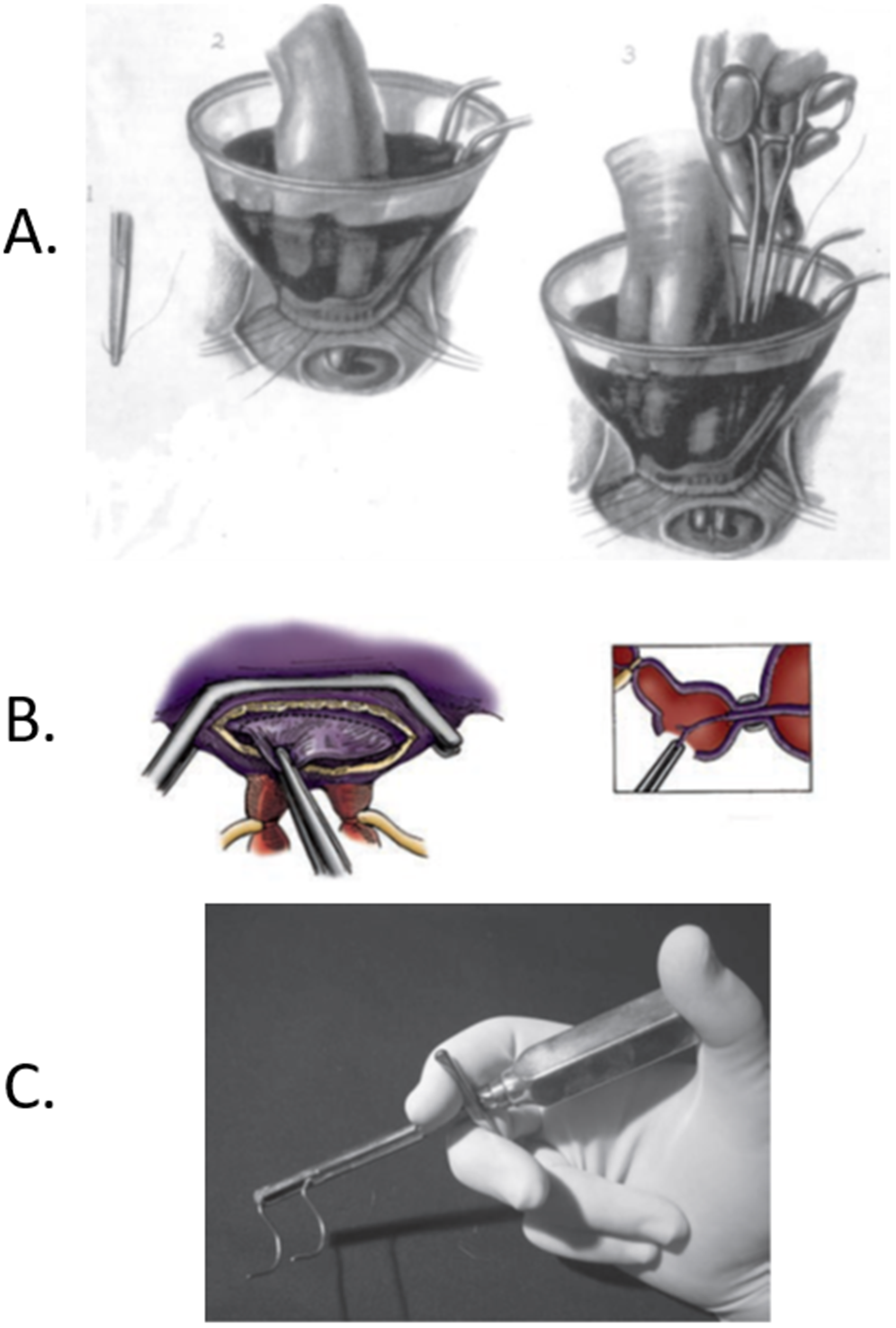
(A) The “atrial well” technique for closure of atrial septal defects, introduced by Robert E. Gross in 1952. A rubber cone is anastomosed to the convexity of the right atrium, and the defect is palpated by the index finger of the operator under the column of blood (2). An appropriately loaded suture (1) is then utilized to close the defect (3) (From Westaby, with permission). 10 (B)/(C) Blalock-Hanlon atrial septectomy. (B) Following isolation of the right pulmonary artery and veins, an incision is made in Sondergaard groove (left) and the dorsal and leftward portion of the interatrial septum is excised (right) (Reprinted with permission from Waldhausen and Pierce). 39 (C) Specially designed clamp, utilized by Alfred Blalock to perform closed atrial septectomy (Courtesy of Vivien Thomas, given to the Division of Cardiac Surgery, The Johns Hopkins Hospital).
Initial Phase of Complete Intracardiac Repairs
While closed or semiclosed operations were helpful for specific lesions amenable to creative exposure, they failed to address more complex morphologic problems, for which a true correction under direct vision was considered unachievable until the early 1950s. The parallel investigation of hypothermia by the pioneering work of Bigelow and colleagues, 43 the introduction and development of extracorporeal circulation by John Gibbon, 44 and the groups at the University of Minnesota and the Mayo Clinic made true and accurate intracardiac surgery attainable.
John Lewis performed the first closure of an ASD on September 2, 1952, under direct vision in a five-year-old child at the University of Minnesota.45,46 The procedure took advantage of the inherent organ preservation technique of surface cooling to achieve direct vision and access of the ASD. Surface cooling to achieve a core temperature of 28 °C, took 2 h and 10 min. This was then followed by a right thoracotomy, 5 min of inflow occlusion, right atriotomy, and primary repair of a 2-cm ASD. The entire procedure took 58 min. Progress was rapid and in just a decade, the mortality for ASD closure was lowered from 30.2% (Gross's original series on ASD closure using the atrial well) 36 to 12.1% (Lewis's inflow occlusion series). 47 Nevertheless, there were many impediments to using these techniques. The moderate hypothermia-inflow occlusion technique allowed only 10 min to repair the ASD to afford some degree of safety. Moreover, the time period did not account for a complex patch repair in the event that a large ASD was encountered. Clearly, new techniques would be necessary and were introduced by John Gibbon at Jefferson Medical College in 1953. 48 He was the first to report successful direct closure of an ASD with the assistance of extracorporeal circulation in an 18-year-old patient. The first extracorporeal circuits were undergoing rapid advancement with alternating success and failures. Two main techniques emerged: controlled cross-circulation and mechanical extracorporeal perfusion, advocated by the University of Minnesota and the Mayo Clinic, respectively. At one time in history, the only place where open heart surgery could be performed was in Minnesota. These intrepid surgeons performed preliminary experiments that led them to believe that their techniques would work in humans. Lillehei10,49 organized efforts to achieve intracardiac repair of complex cardiac lesions with the clinical introduction of controlled cross-circulation on March 26, 1954 (Figure 4A). 48 Warden et al pioneered this technique after extensive and comprehensive laboratory investigation in canines.50,51 The first patient, a one-year-old boy with an operative weight of 6.9 kg, was supported by his father during cross circulation (Figures 4B and C) 49 for 19 min during which time the ventricular septal defect was closed primarily. The patient died from pneumonia after 11 days. Clearly, there were lessons to be learned, but this outcome did not undermine the morale of the surgeons at the University of Minnesota. There was institutional bias against continuing with this avant garde therapy, but with the support of Owen Wangensteen, Chair of the Department (Figure 4D), 49 Lillehei closed the ventricular septal defect of a four-year-old girl two weeks later, achieving long-term survival. The long-term results were nothing short of spectacular. Lillehei and coworkers performed a total of 45 operations with controlled cross circulation. Among these operations were a number of firsts that included, the first successful repair of tetralogy of Fallot, ventricular septal defect, and atrioventricular canal.52–54 In this extraordinary series, operative mortality was 38%, and 79% of hospital survivors were alive at 30-year follow-up. 49 Of some interest, no operative deaths were directly attributable to extracorporeal perfusion. In those days, intricate knowledge of the intracardiac conduction system was waiting to be defined and postoperative heart block was most certainly implicated in several of the early failures. Because of this early, permanent, and often lethal complication, Lillehei and coworkers also developed, out of extreme necessity, the first temporary and, eventually, permanent implantable pacemakers.55,56 By the end of the 1950s, the University of Minnesota adopted circulatory support technology with the DeWall-Lillehei oxygenator 57 and abandoned controlled cross-circulation. Eighty-four miles away, in the same state of Minnesota, John Kirklin (Figure 5A) at the Mayo Clinic focused all his research efforts on cardiopulmonary bypass, developing the Mayo-Gibbon apparatus and its modifications. 44

(A) Clarence Walton Lillehei (1918-1999) (From Westaby, with permission). 10 (B) University of Minnesota, Operating Room B, March 26, 1954: the first case of controlled cross-circulation. Dr C. Walton Lillehei, to the right of the scrub nurse, is seen wearing a headlight. Opposite to Dr Lillehei is Richard Varco. The patient's father is in the right background, and visible is the femoral donor cannulation site. Morley Cohen and Herbert Warden are seen behind Dr Lillehei. Vincent Gott, the surgical intern on the cardiac service, is seen at the left upper corner of the picture, while assistant resident Norman Shumway is to his right (Image courtesy of the University of Minnesota photographic archives). (C) Schematic illustration of the first case of controlled cross-circulation, 1954. Original drawing by the intern on C. Walton Lillehei's service, Vincent L. Gott. (D) Note from Owen H. Wangensteen written to C. Walton Lillehei on March 25, 1954, the eve of the first parental cross-circulation: Dr Lillehei Dear Walt—By all means, go ahead! OHW (C and D from Lillehei, with permission). 49
(A) John Kirklin (1917-2004) (Courtesy of Dr. Joseph Dearani, Division of Cardiac Surgery, The Mayo Clinic. With permission). (B) Aldo Castaneda (1930-2021) (From Westaby, with permission). 10
In 1955, Kirklin reported on 38 patients with ventricular and other septation defects that were corrected with cardiopulmonary bypass techniques. 58 These initial contributions established the relative safety of mechanical extracorporeal circulation and would serve as the basis for the development of the field of pediatric cardiac surgery. These techniques, developed in Minnesota, would be the mainstay for repair of more complex anomalies that were approached in the early 1960s without excessive mortality.59–66 Seventeen years passed before John Kirklin joined others in the founding of the CHSS. 1 While the initial experience of congenital heart disease in older children proved promising, intracardiac repair remained a daring undertaking in neonates and infants, mostly because of the deleterious effects of cardiopulmonary bypass in children. 66 Inquiries into the complications associated with cardiopulmonary bypass revealed the importance of the size of the bypass circuits, crudeness of the materials, lack of advanced cardioplegia strategies, and underdevelopment of pediatric critical care. These deficiencies made correction of cardiac anomalies in early infancy prohibitive. Between 1955 and the middle 1960s, smaller patients underwent correction only after initial palliation by closed cardiac techniques.
Expansion of Congenital Cardiac Surgery
Sir Brian Barratt-Boyes was a very influential figure during this continued inquiry into solving the problems associated with cardiopulmonary bypass, which led to improved results. After spending two very informative years at the Mayo Clinic (1953-1955), he returned to Green Lane Hospital (Auckland, New Zealand) to pioneer and develop the concept of profound hypothermia and hypothermic circulatory arrest. 67
This method served to decrease the duration of exposure to extracorporeal surfaces and the subsequent inflammatory response pertaining thereto, by limiting the exposure to that needed for cooling and rewarming.
The actual intracardiac repair could then be carried out effectively, unconstrained by cannulas crowding an asanguinous field. This greatly facilitated exposure in neonates and small infants. In addition, systemic cooling permitted relatively reliable myocardial protection, based on hypothermia, before the routine introduction and use of cardioplegia.68–70 This revolutionary innovation allowed intracardiac repair of complex anomalies in neonates and infants, with excellent outcomes.67,71 In his original 1971 article, 67 Barratt-Boyes reported on 37 infants who underwent repair using these principles. Thirty-three had operative weight below 10 kg, and 25 patients were between 8 days and 12 months of age at the time of surgical correction. With increased experience, a gradual but steady shift toward early, complete one-stage intracardiac repair rather than initial palliation followed.72–76 Complex anomalies such as total anomalous pulmonary venous connection, transposition of the great arteries,75,76 complete atrioventricular canal,77–79 and aortic arch anomalies80,81 could be repaired in the neonatal period or in early infancy with much more acceptable morbidity and mortality as compared with the results of earlier corrective attempts. Universal recognition followed, and, for his pioneering efforts, he was appointed Commander of the Order of the British Empire in the 1966 New Year Honours, 82 and promoted to Knight Commander of the same order in the 1971 New Year Honours, further confirming an international prominence comparable to that achieved by René Favaloro in Argentina and Christiaan Barnard in South Africa. 83 Barratt-Boyes became a proponent of these techniques and shared the Green Lane experience at many international meetings as well as hosted workshops in Auckland. 83 Interest and acceptance quickly followed. This pioneering work was further developed by Aldo Castaneda (founding member of the CHSS) (Figure 5B),10,76,78 Jatene et al,84,85 Norwood et al,86,87 Ebert et al,88,89 Bailey et al,90,91 and others.92–95 This new era of deep hypothermia and circulatory arrest in neonates enhanced the development of complex open-heart repairs by Castaneda and Norwood at Boston Children's Hospital that resulted in the introduction of the Norwood operation and other one-stage complex repairs. Thanks to the vision and determined commitment of these contributors as well as to the exponential progress of perioperative care,42,96 the corrective congenital heart surgery evolved over a 25-year period from difficult attempts at palliation in older children to routine complete correction in neonates and infants.
Further Developments That Propelled Congenital Heart Surgery into the 21st Century
The students of the aforementioned notable intrepid surgeons 1 carried the innovative techniques into refined stages that improved clinical results; retrospective data analysis by the Society of Thoracic Surgeons Congenital Heart Surgery Database 97 ; prospective multi-institutional studies conducted by the data center of the CHSS1,2; inauguration of the American Board of Thoracic Surgery Congenital Heart Surgery certification 98 ; and establishment of the CHSS as the leading organization dedicated to congenital heart surgery in North America.1,2 The specialty of congenital heart surgery was maturing.
At the dawn of the 21st century, high mortality was still associated with the Norwood operation for hypoplastic left heart syndrome, common arterial trunk (truncus arteriosus) with interrupted aortic arch, severe neonatal Ebstein anomaly of the tricuspid valve, and ventricular septal defect with major aortopulmonary collateral arteries (MAPCAs).99,100 Moreover, long-term complications involving the Fontan operation led to high mortality involving Fontan revision, cardiac transplantation for Fontan patients owing to coexisting liver failure, cardiac arrhythmias, protein-losing enteropathy, and plastic bronchitis.101,102 Analytic and committed surgeons introduced and refined the Norwood operation86,87 that served to improve results. Individuals such as William Norwood, 103 Bove (past president of the CHSS),104–107 Thomas Spray, 108 David Bichell, 109 and Sano et al110–112 documented incremental technical advances that decreased circulatory arrest time, standardized neoaortic patch augmentation, introduced the ventricular-to-pulmonary-artery shunt, and emphasized postoperative management schemes including delayed primary chest closure. These innovations served to improve clinical results with the Norwood operation.
Owing to many advances, operations for common arterial trunk (truncus arteriosus) were being performed with a low mortality rate.113–116 However, those patients with associated interrupted aortic arch still had high mortality owing to anatomic variation, truncal regurgitation, and arch hypoplasia. 117 Prospective inquiries by CHSS members and the data center led to documentation of these results. 118 It was Edward Bove 119 who showed how improved results can be achieved by thoughtful application of myocardial preservation, systemic perfusion techniques, and stellar technical skill. 120 Improved results documented by others soon followed.115,116
Neonates with severe Ebstein anomaly of the tricuspid valve were particularly at risk in the immediate postnatal period owing to poor systemic perfusion, acidosis, and hypotension. Vaughan Starnes and colleagues introduced tricuspid isolation with a fenestrated patch and systemic to pulmonary artery shunt to stabilize these patients with remarkable success.121,122 Knott-Craig and colleagues 123 introduced the idea that even neonatal/infant repair of the tricuspid valve could be accomplished with favorable results. This strategy allowed for a biventricular repair in some patients, unlike the Starnes technique that largely steered the patient toward univentricular palliation.
Biventricular repair of ventricular septal defects, pulmonary atresia, and MAPCAs was challenging and limited by seemingly impossible unifocalization of the peripheral pulmonary artery segments into one pulmonary artery that could accept the pulmonary circulation without right ventricular hypertension. Hanley et al exercised the patience, courage, and technical ability to rehabilitate small peripheral MAPCAs into a unifocalized segment and accomplish biventricular repair with ventricular septal defect closure and right ventricular to pulmonary artery conduit. 124 Hanley et al shared his experience through national meetings, fellowship training, and invitations to his operating room. His educational style emphasized the technical aspects of pulmonary artery rehabilitation by using autograft material that would grow with the patient.
During this period, patients with univentricular anatomy who were palliated by the Fontan procedure were starting to show significant atrial arrhythmias, ventricular dysfunction, atrioventricular valve regurgitation, liver dysfunction, protein-losing enteropathy, and plastic bronchitis. 125 Early attempts to further palliate these patients with pacemaker therapy126–128 proved to be hazardous and were soon abandoned. Drs Constantine Mavroudis (past president of CHSS), Barbara Deal, and Carl Backer (past president of CHSS) used a systematic approach to introduce a new operation based on arrhythmia surgery, anatomic conversion to extracardiac connections, repair of associated lesions, and pacemaker therapy, 129 which was called Fontan conversion. Unfortunately, this operation could not be applied to all patients with failing Fontan physiology owing to severe ventricular dysfunction, protein-losing enteropathy, plastic bronchitis, and advanced cirrhosis. These unfortunate patients were too sick for this strategy and ultimately required cardiac transplantation. 130
Repair of aortic aneurysms owing to connective tissue disorders in children was pioneered by intrepid surgeons such as Vincent Gott, Duke Cameron, Luca Vricella, and colleagues.131–133 These surgeons took advantage of newly introduced synthetic grafts, 133 cardioplegic techniques, and advances in deep hypothermia circulatory arrest to visualize, plan, and execute safe operations for these unfortunate patients.
Advances with cardioplegia were attended by the sustained career-long efforts of Pedro del Nido who introduced and offered a well-accepted cardioplegic solution to extend the limits of myocardial preservation with less administration during the operation. 134 Surgeons now were able to concentrate efforts more on the operations and less on the frequent administration of cardioplegic solution. Other contributions included intraoperative transesophageal and epicardial echocardiography,135,136 first introduced by Ungerleider.
The aforementioned advances are but a few of the extraordinary innovations that inspired the continued development of congenital heart surgery (Table 1). 4 The future is bright and centers around improved cerebral protection, early extubation strategies, collaboration of pediatric cardiothoracic programs, and effective teaching techniques.
Medical Illustration in the Era of Congenital Cardiac Surgery
The era that spawned the advancement of congenital heart surgery was notable by those talented individuals who illustrated new techniques, documented the intricate educational parts of the operation, and introduced interrelational anatomic details of complex congenital heart disease. Illustrating these images was no small undertaking since both epicardial and endocardial anatomy had to be shown and interpreted. These complex details challenged the medical illustrator to use various techniques to show the anatomy and the stages of the operation.
Twentieth-Century Advances in Medical Illustration in the Era of Cardiac Surgery
The beginning of the 20th century laid the groundwork for medical illustration in North America that was foundational in introducing a new academic department that would chronicle, in exquisite anatomic detail, the advances of congenital heart surgery. Shortly after the inauguration and establishment of the Johns Hopkins University School of Medicine (1893) Max Brödel arrived in Baltimore in 1894.137,138 He was an art student who had been working at the Physiological Institute in Leipzig. He was recruited to Johns Hopkins University School of Medicine where he began illustrating for William Halsted, Professor of Surgery, and Harvey Cushing. The first Department of Art as Applied to Medicine with Max Brödel as director was established in 1911. 139
Brödel introduced the technique of “carbon dust drawing on Ross stipple board” that had the effect of creating medical, grayscale, tonal illustrations appear like living tissue. His teaching style was instrumental in producing many students who excelled in their own careers, and he is considered by many to be the father of medical illustration. Figure 6 shows Max Brödel shortly after his arrival in Baltimore.
Max Brödel shortly after he arrived in Baltimore. Brödel established the first Department of Art as Applied to Medicine in the United States at Johns Hopkins University (Reproduced with permission from the Max Brödel Archives of the Department of Art as Applied to Medicine).
Anatomic investigation into the particulars of congenital heart disease has been documented by individual reports since the Renaissance. However, the systematic inquiry of relating symptoms to specific anatomic lesions is thought to have been initiated by Maude Abbott, MD, a pathologist at McGill University in Montreal. She classified diseases by careful observation and correlation to the clinical course of patients. It became apparent that medical illustration would be important and imperative to explain anatomy and pathophysiology to interested students and faculty of this newly formed subspecialty. Maude Abbott published her Atlas of Congenital Cardiac Disease in 1936.140–143 The descriptions were accurate even by today's standards, the drawings were expertly rendered, and the technique of carbon dust was mastered by artists who studied with Brödel at Johns Hopkins. Figure 7A shows the exquisite anatomic detail of a patient with double inlet left ventricle and pulmonary stenosis.140–143
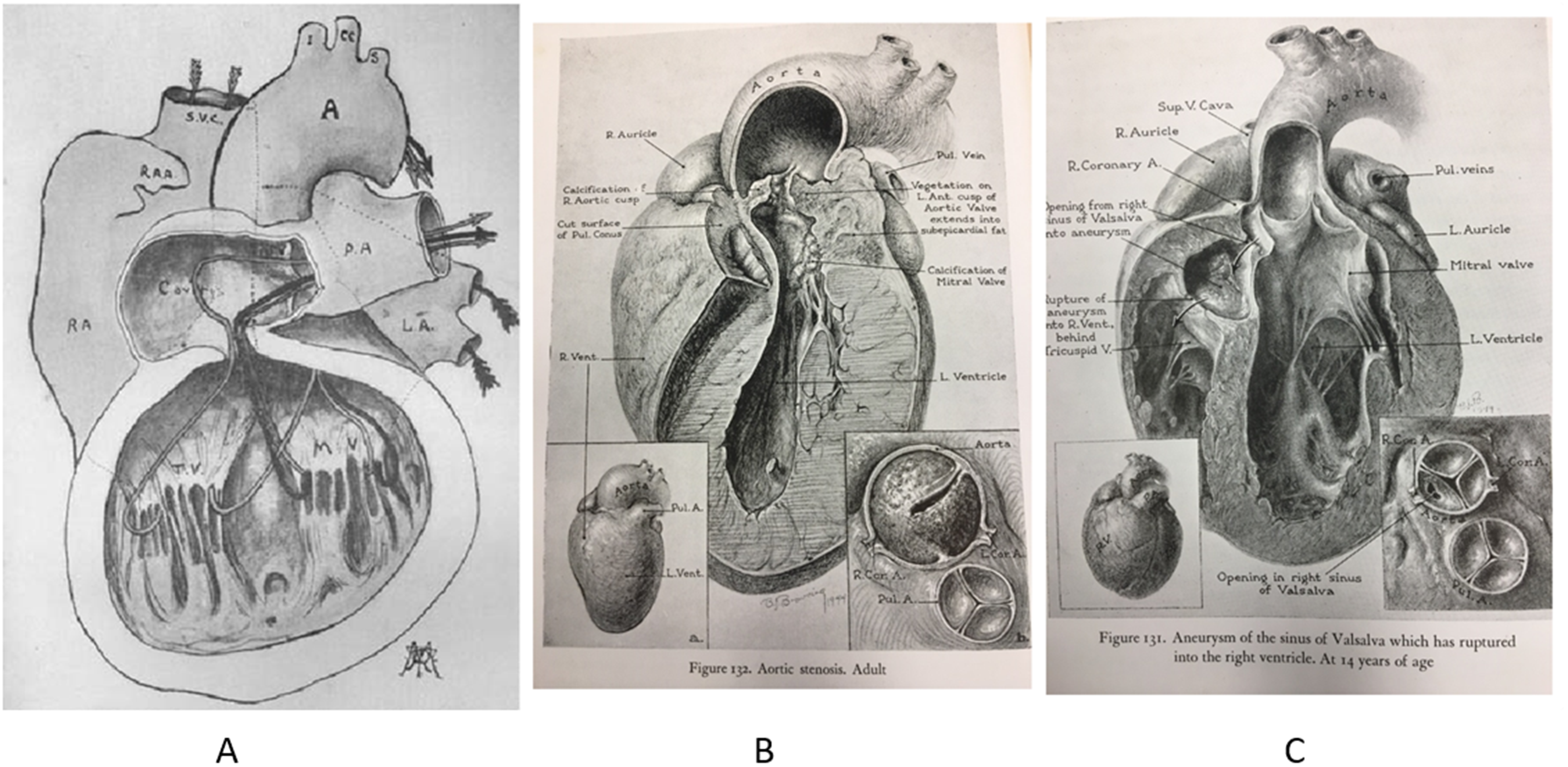
Double-inlet single ventricle with pulmonary stenosis (A) as demonstrated by Hortense Douglas Cantile. Hortense studied with Brödel at Johns Hopkins where she mastered the technique of “Carbon Dust.” She worked with Blankstock to illustrate Maude Abbott's treatise (Reproduced courtesy of the Maude Abbott Museum of McGill University, Canada). (B-C) Detailed coronal views of specimens of aortic stenosis (B) and Sinus of Valsalva Aneurysm (C) by Elizabeth Browning, also known as “BJ.” BJ used carbon dusting techniques with coronal sections (B and C Reproduced with permission from Taussig). 144
In parallel inquiries into the illustration of congenital heart lesions, Johns Hopkins would play a major role. Taussig would start the process. She was the daughter of a well-known Boston physician who urged her to pursue nursing as a career. She chose otherwise. After her rejection from Harvard Medical School, she applied to and was accepted to Johns Hopkins University School of Medicine where she excelled and became interested in congenital heart disease. She succeeded in correlating history, symptoms, and physical findings of her patients with their autopsy findings upon their death. Her excellent and comprehensive descriptions were illustrated by Elizabeth Browning, also known as “BJ.” BJ used carbon dusting techniques with coronal sections to show the intracardiac pathologic anatomy (Figures 7B and C). 144
Illustration for Cardiac Surgery Comes of Age
While Maude Abbot and Helen Taussig introduced the comprehensive and conscientious study of congenital heart disease, it was Crafoord and Nylin, 15 Gross and Hubbard, 9 and Blalock13,19,38 whose courageous efforts inaugurated the pathway to open heart surgery. While complex operations could be described in prose, complete understanding for teaching purposes and communication required illustration.
Brödel's introduction of the “carbon dust drawing on stipple board technique” to add depth and texture to the illustration was learned and practiced by Leon Schlossberg who worked closely with Blalock and many Johns Hopkins professors. Paul A. Ebert, a Johns Hopkins University School of Medicine alumnus of the residency program, published an Atlas of Congenital Heart Surgery that was illustrated by Schlossberg (Figure 8). 145 Other notable Brödel trainees included Ted Bloodgood and Gerald P. Hodge at the University of Michigan, Herb Smith and Barry Baker at Baylor College of Medicine in Houston, and Timothy Hengst at the Texas Children's Hospital in Houston.
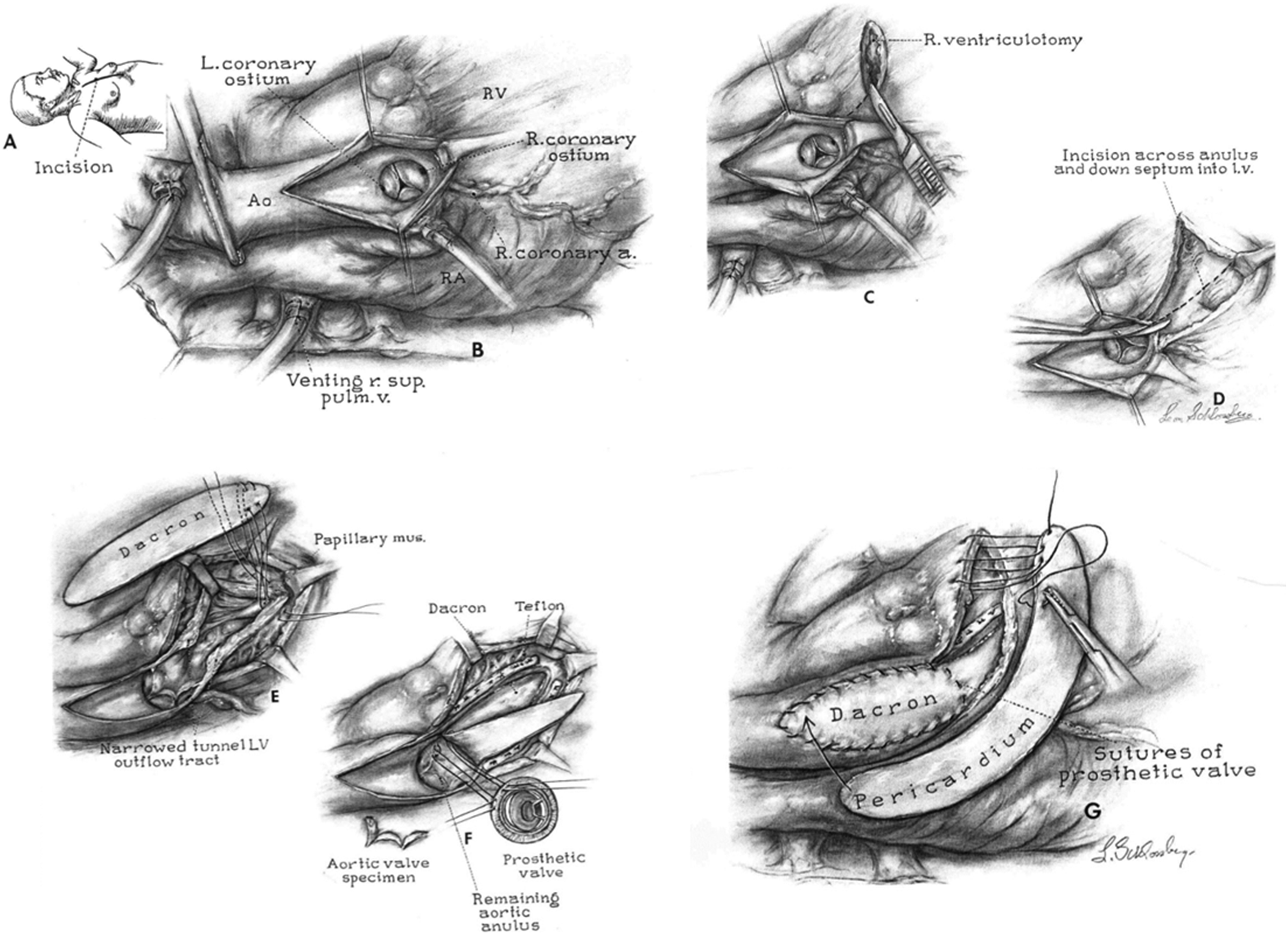
Dr Ebert communicated with Leon Schlossberg to produce a series of drawings that explained the Konno procedure, one of the more difficult procedures to master. He repeated the inset showing the median sternotomy and depicted the small aortic annulus, which is the reason for this operation. Reproduced with permission from Ebert. 145
Late 20th and Early 21st Century
The era that bridged the late 20th and early 21st centuries was notable for significant advances in surgical therapy for patients with transposition of the great arteries, functional single ventricle, left ventricular outflow tract obstruction, and tetralogy of Fallot, among others. Advanced and innovative operations such as arterial switch operation, Norwood operation, extracardiac Fontan, Fontan conversion with arrhythmia surgery, Ross-Konno, and pulmonary valve-sparing/restoration for tetralogy of Fallot repair have emerged.77,87,92,129,146 While there were many programs and associated medical illustrators who participated in and documented these advances, focused efforts were centered in Chicago at Children's Memorial Hospital starting first with Willis J. Potts whose pioneering efforts with the Potts’ shunt 21 and coarctation of the aorta were illustrated by Virginia Sampter, a very talented medical illustrator who graduated from University of Illinois Medical Illustration School in 1947. Her drawings emphasized the stepwise parts of the procedures of Dr Farouk Idriss, who succeeded Dr Potts at Children's Memorial Hospital as chief of Pediatric Cardiac Surgery, concentrated his research and clinical expertise on anatomic correction of transposition of the great arteries. The initial drawings of the arterial switch operation were illustrated by Virginia Sampter (Figure 9A-D top panel). 147 Subsequently, during the improved clinical experience with the arterial switch operation, it was Zelda Zelinsky who illustrated the progressive steps of the arterial switch operation (Figure 9 bottom panel). 148 In 1989, Dr Constantine Mavroudis succeeded Dr Farouk Idriss and brought his own vision of medical education through publication and illustration. It was, at this time, that Rachid Idriss, son of Dr Idriss, completed his education in medical illustration and associated with Drs. Mavroudis and Backer at Children's Memorial Hospital to publish numerous articles, textbooks, and atlases.148–153
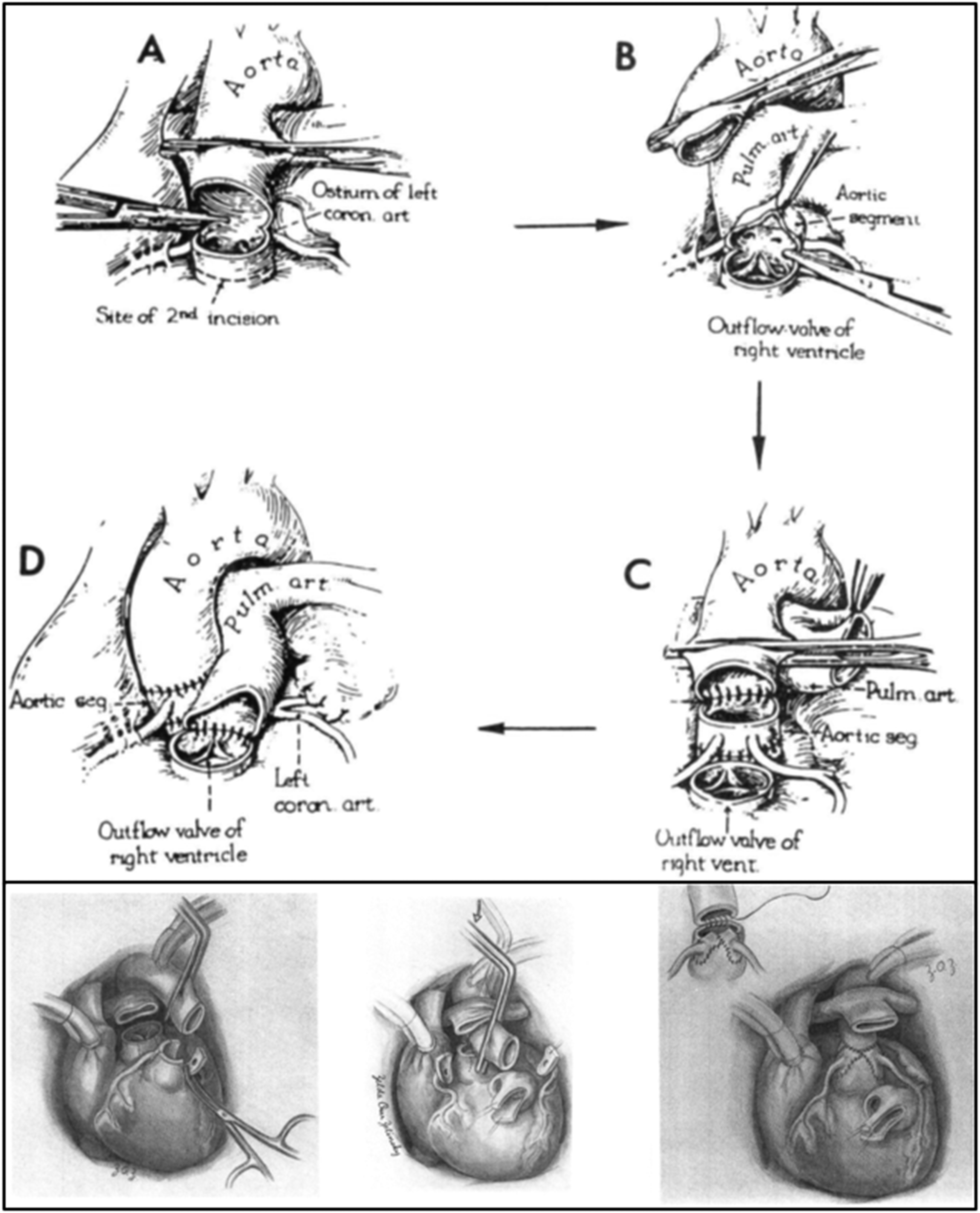
(A-D) Virginia Sumpter also worked with Dr Farouk Idriss, whose pioneering efforts to develop the arterial switch operation started in 1961. Her rendition of Idriss's notion of the arterial switch operation is shown in four drawings depicting the important steps of the procedure. Of some interest is that cardioplegia was not yet introduced and that arterial blood gas determination was not clinically available (Reproduced with permission from Mavroudis and Backer). 147 (E-G) Zelda Zelensky started to work with Farouk Idriss shortly after Virginia Sampter. Her style was tonal grades of grey and was depicted to give more texture to the illustration. Shown here are steps of the arterial switch operation, which were perfected after the introduction of cardioplegia, arterial blood gas determination, and fine suture techniques. The first drawing (E) shows the coronary artery dissection after great vessel transection. The second drawing (F) in Zelensky's rendition of the arterial switch operation showed the Maneuver of Lecompte portrayed by the “Ghost” clamp that was moved from the distal ascending aorta (ghosted clamp) to the proximal ascending aorta (actual clamp). The dissected coronary artery buttons are shown in preparation for the neoaortic reconstruction. The third drawing (G) in Zelensky's arterial switch shows the completed neoaortic reconstruction with the inset demonstrating the suturing technique that was introduced by Dr Idriss (Reproduced with permission from Dr Constantine Mavroudis who retains the copyright). 148
During the continued progression of medical illustration, several techniques were incorporated into the drawings that gave perspective, proportionality, and action to the design. The hovering technique (Figure 10A top row) 152 allows the observer to visually understand where the sutures are placed in each location while the patch or device floats over the area of eventual placement. Visualization of concomitant internal and epicardial anatomy can be expressed by techniques known as hidden anatomy, ghost views, or transparency (Figure 10B bottom row).149,153 Another aspect of illustration is the centrally focused perspective that allows the artist to deemphasize the periphery of the operative field and call attention to the important part of the operation at the center of the illustration. Other methods that artists use to emphasize activity in the drawing are action techniques that bring life and movement to the drawing. Another illustration technique is the use of insets. An inset is an illustration technique that directs a more exact and focused view of a drawing. Another technique that medical illustrators use to provide a sense of dimension and measurement is the detail of human proportionality in the drawing. This is a method to indicate the size relationship between the operative subject and the human. Perhaps, one of the most important illustration techniques of cardiac surgery is the step-by-step technique. This series of drawings depicts, in a coordinated instructive process, the important stages of an operation.
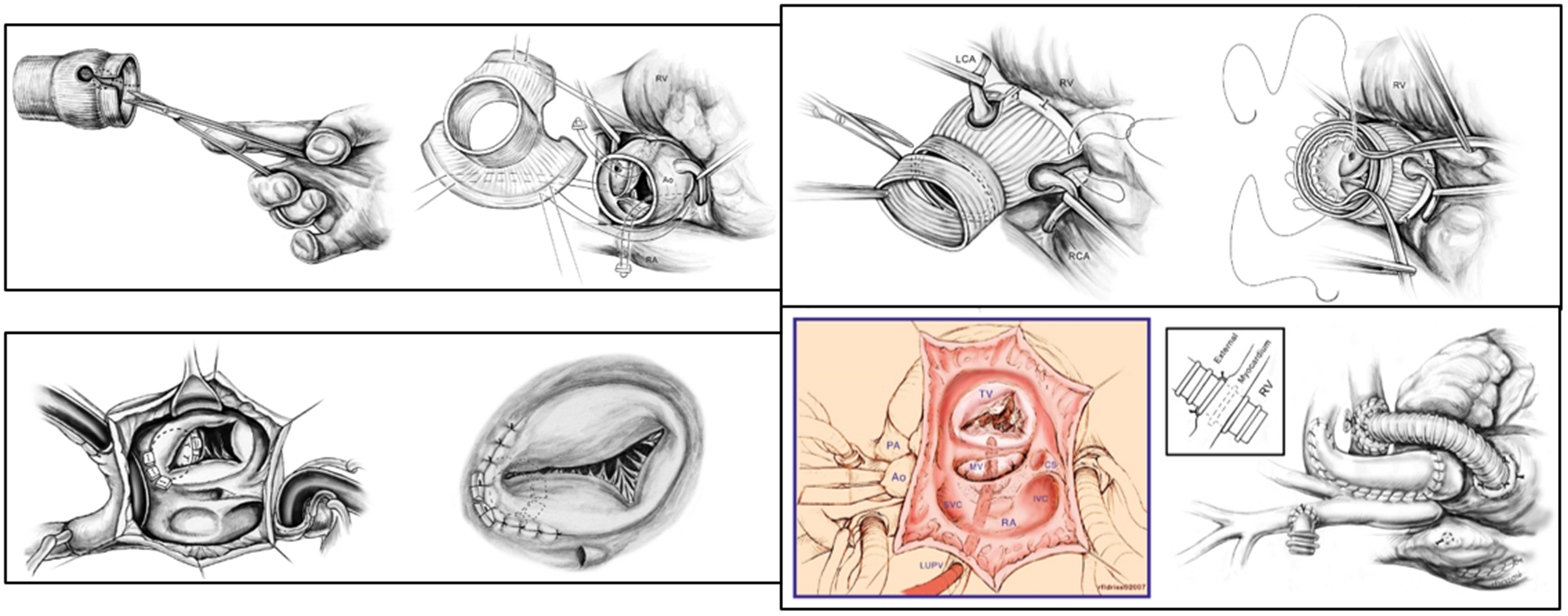
Various artists’ techniques to show proportionality, insets, and hidden anatomy. Top row: The graft is being prepared by incising the root of the graft to communicate with the “keyhole” for the coronary arteries (first panel). The artist shows human proportionality to demonstrate the relative size of the graft. There are two central focuses in this rendition: the graft and the hand. Both are important. Perhaps the most ingenious drawing in this series is in the second panel. Idriss shows a hovering view of the graft above the central figure, namely the aortic root. The pledgeted sutures are exactly placed to show how the graft will be engaged. The hovering graft is splayed open for the observer to see exactly how this graft will fit. The artist took the privilege of “seeing with the mind's eye” to demonstrate this complicated maneuver. In reality, this graft is not actually positioned in this manner. The image, however, tells the story of what needs to be done. In the third panel, The Florida Sleeve has been successfully placed around the aortic root with care to preserve the anatomic configuration of both coronary arteries. The focus is the aortic root; the action is shown by the tie in progress, and the scissors show how the graft can be shortened to fit the reconstruction. In the fourth panel, the top of the aortic root is being attached to the top of the Florida Sleeve graft using a piece of Dacron felt. The coronary arteries are shown with the central focus on the suturing technique, which shows the action of the repair. (From Mavroudis and Dearani, with permission). 152 Bottom row: These drawings show “Ghost” view techniques in the first three panels highlighting the ventricular septal defect patch behind the tricuspid valve; the ventricular septal defect patch behind the repaired tricuspid valve; and the left ventricular vent through the right superior pulmonary vein, into the left atrium, and then to the left ventricle. The fourth panel drawing shows how a Norwood operation can be simulated in a neonatal piglet as a teaching tool. The artist uses tones to demonstrate the externally supported ribbed right ventricular to pulmonary artery Gortex graft as well as an inset that shows how the ribbed graft can be placed into the right ventricular cavity to prevent anastomotic narrowing. This maneuver is called the “dunk technique.” (From Mavroudis and Backer, with permission and from Mavroudis et al, with permission).149,153
Modern Times and the Medical Illustrator
The history of medical illustration has mirrored, quite literally, the great advances in surgical procedures. This focused historical overview of medical illustrators in the era of congenital heart surgery emphasizes the contribution that medical illustrators have made in the educational process of learning complex open-heart procedures. To offer a closing note from our publications,4,5 “While new technologies of medical imaging are extant
154
and developing rapidly, these methods are the ‘cameras’ of anatomical reproduction. The camera, computed tomography scan, magnetic resonance imaging, reconstructed heart models, and arteriograms are clearly important for diagnosis, operative planning, and therapeutic interventions; however, they do not ‘illustrate’. Illustration focuses, interprets, emphasizes, directs, cautions, explains, and, in the most fundamental way, teaches. The association between medical illustrator and clinician has ancient roots. There is no substitute for human interaction, spatial interpretation, and medical education in its most robust form, illustration.”4,5
Summary
The historical account of congenital heart surgery is founded on ingenious ideas, clinical research, intrepid surgeons, thoughtful collaboration, and introduction of educational illustration techniques that were the foundations of sharing advances with the world. Imagine for a moment how, in the early 20th century, two visionary and inspired women, Maude Abbott and Helen Taussig, defined the study of congenital heart disease with collaborative illustrations that were instrumental in discovery and education. Anatomic atrial wells were created to close an ASD without cardiopulmonary bypass. C. Walton Lillehei used cross-circulation to perform open-heart surgery. John Kirklin perfected the heart-lung machine that John Gibbon introduced and when Dr Kirklin noted a high incidence of heart block with ventricular septal defect closure, he traveled to Chicago to collaborate with Maurice Lev, a pathologist, with whom he determined the conduction system and the method to avoid it during open heart surgery. And there was more. Creative surgeons introduced new operations; the intensive care unit was created; and myocardial preservation was perfected. Education became essential in the propagation of surgical techniques, physiologic advances, board certification, and resident education. Medical illustration was instrumental and essential during national meetings, focused manuscripts, and textbooks. As we celebrate the 50th anniversary of the CHSS, one must marvel at the advances that have shaped our specialty of congenital heart surgery and the enormous contributions of CHSS members relating thereto.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.