
Abstract
Circumflex aorta is described as a retroesophageal aortic arch, with opposite-sided descending aorta forming a true vascular ring with ligamentum arteriosum. We report two cases of right-sided circumflex aorta with varied clinical presentation. Computed tomography diagnosed this vascular ring anomaly. The patients were managed with the aortic uncrossing procedure as a primary surgical strategy. Preoperative diagnosis and thorough planning were essential for the successful outcome. The patients did not have any residual symptoms of tracheal and esophageal compression on follow up.
Introduction
Aortic arch anomalies constitute a wide array of variations resulting from irregularities in the embryogenesis of branchial arches. They can occur in isolation or in association with other intracardiac defects. Prevalence of aortic arch anomalies in the general population is approximately 1% to 2%. 1 Vascular rings account for 1% of all surgically operated cardiovascular malformations. 2 Circumflex aortic arch is characterized by retroesophageal crossing of the aortic arch with contralateral course of the descending aorta. Clinical presentation may vary from being asymptomatic to respiratory distress, stridor, or dysphagia. When symptoms occur, simple ligation and division of the ligamentum arteriosum may not be sufficient to relieve symptoms. We describe two cases of this anomaly with different clinical presentations that were successfully managed by the “aortic uncrossing procedure.” 3
Case Report
Case 1
A six-year-old girl (weight 13 kg) presented to us with dysphagia of one-year duration. Transthoracic echocardiography showed bicuspid aortic valve with no intracardiac defects. Computed tomography (CT) identified an ascending aorta passing to the right of the trachea and continuing as a retroesophageal segment behind the esophagus and trachea, emerging in the left thorax to descend to the left of the spine (Figure 1A). The branches from the circumflex arch in sequence were left common carotid artery, right common carotid artery (RCCA), with ectatic right-sided proximal arch followed by the right subclavian artery (RSA) and aberrant left subclavian artery (LSA) forming a Kommerell diverticulum (KD) (Figure 1B), exerting significant mass effect on the lower trachea and esophagus (Figure 1C).
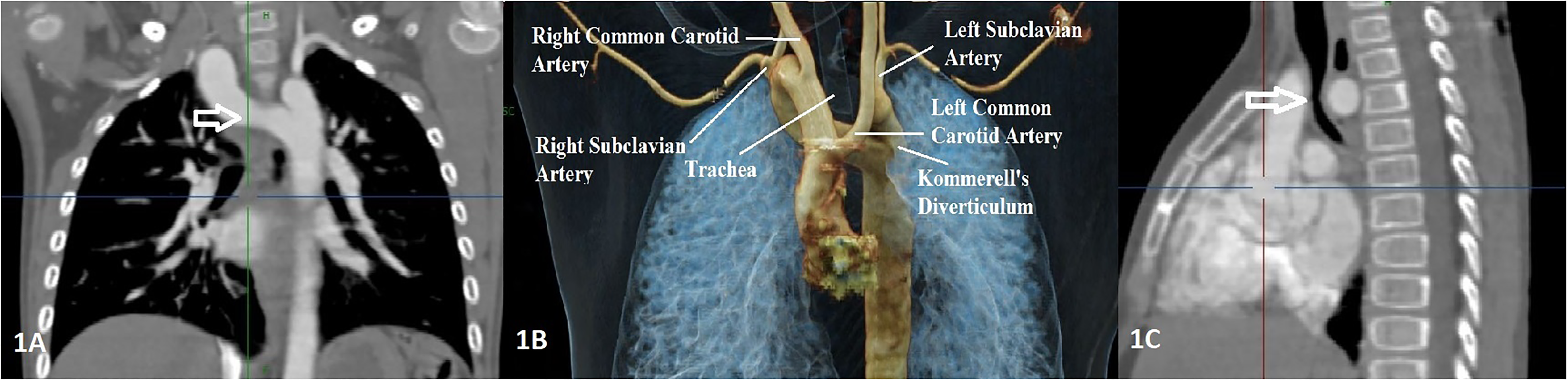
(A) Coronal section of computed tomography (CT) showing right aortic arch with left descending aorta. (B) 3D Reconstruction of CT image showing the aortic arch anatomy and its branches. (C) Sagittal section of CT showing tracheal compression by the aortic arch. CT, computed tomography.
Case 2
A seven-month-old girl (weight 4.7 kg) presented to us with respiratory distress and required mechanical ventilation in the emergency room. Chest x-ray showed marked cardiomegaly and increased pulmonary vascularity, along with pneumonic patches. Transthoracic echocardiography showed a large secundum atrial septal defect (ASD) and a large perimembranous ventricular septal defect (VSD) with severe pulmonary artery hypertension and right aortic arch. The inability to wean off ventilatory support and persistent consolidation in the lungs with high peak airway pressures led to the evaluation of the aortic arch. Computed tomography identified right-sided circumflex aorta. She had pneumonia and systemic sepsis, which was managed with appropriate antibiotics, anti-failure medications, and then taken up for surgery.
Surgical Technique
Both patients underwent the aortic uncrossing procedure as described by Russell and colleagues. 4 While dissecting all the vessels, bilateral phrenic and recurrent laryngeal nerves were carefully separated from the relevant structures. The ligamentum arteriosum was divided and both the stumps were transfixed (Figure 2A-C). Cardiopulmonary bypass was initiated via aortic cannulation to the base of the RCCA with bicaval venous cannulation and cooling to 22 °C. The VSD was closed in the second case while the patient was cooled. On reaching the desired temperature, selective antegrade cerebral perfusion was initiated by directing the aortic cannula further in the RCCA and snugging the neck vessels. The aorta was clamped between the RSA and LSA behind the esophagus and trachea. The remnants of the KD were excised, and the aberrant LSA was reimplanted. The proximal stump was doubly oversewn. The mobilized descending aorta was advanced anterior to the trachea and esophagus and anastomosed end to side to the ascending aorta. Complete closure of the ASD was done using autologous pericardial patch. Both patients were weaned off bypass uneventfully. Cardiopulmonary bypass, aortic cross clamp, and selective antegrade cerebral perfusion times in both patients were 61, 35, and 11 min and 114, 72, and 23 min, respectively. Both patients did not have any residual complaints and made an uneventful recovery.
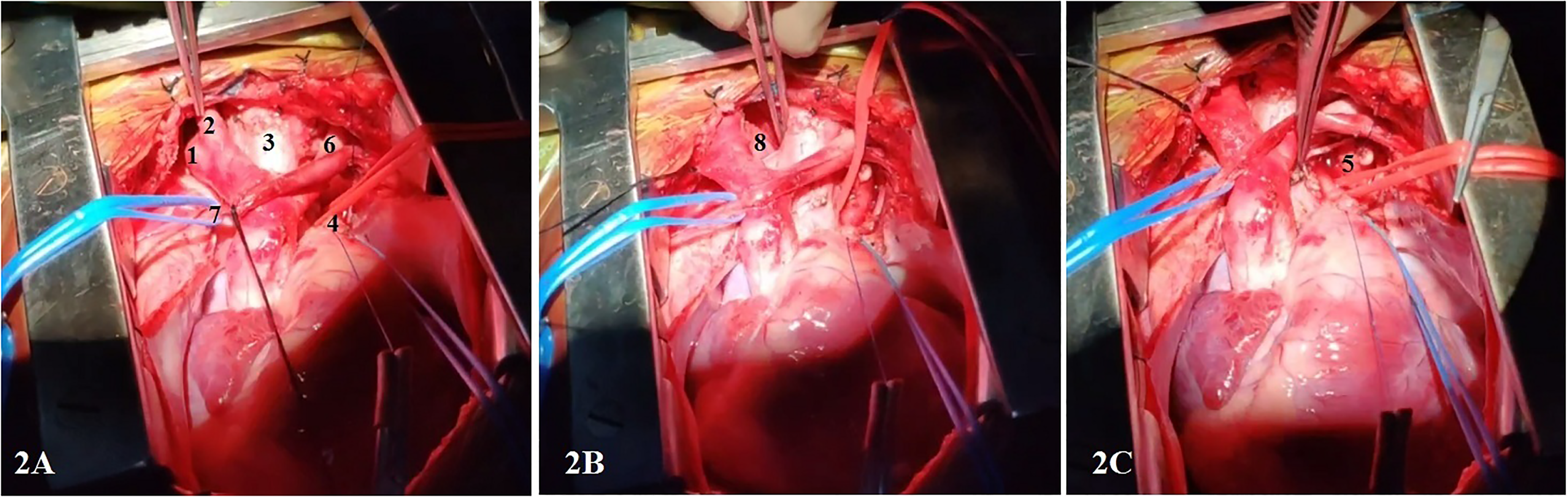
(A-C) 1: Right innominate artery; 2: Right common carotid artery; 3: Trachea; 4: Proximal ligamentum arteriosum stump after division; 5: Descending aorta; 6: left common carotid artery; 7: left innominate vein; 8: right arch going behind the trachea and esophagus.
Comment
The term, “circumflex aorta” is used for congenital aortic arch anomalies with high retroesophageal arch segment above the carina with both the proximal descending aorta and ligamentum arteriosum on the opposite side forming a vascular ring, while the distal descending aorta may or may not cross back to the other side of the spine. 5 A Kommerell diverticulum is invariably present. A left-sided ductus arteriosus or ligament arises from the main pulmonary artery and connects to the descending aorta; thus, completing a vascular ring. Right aortic arch with left descending aorta and left aortic arch with right descending aorta are termed as right and left circumflex aorta, respectively (right more common than left). Hypoplasia/coarctation can be associated with this anomaly. Embryology of circumflex aorta includes involution of the right sixth arch, left fourth aortic arch with persistence of the left sixth arch, and left dorsal aorta (contralateral side as compared with the same side of the dorsal aorta seen in normal development). 6 Both our patients had aberrant left subclavian arteries with nonobstructive arch causing significant symptoms due to tracheal/esophageal compression. Although echocardiography can detect aortic arch anomalies such as vascular rings, CT angiogram, or magnetic resonance angiogram are better diagnostic tools. Other studies have also reported similar results of the aortic uncrossing procedure.4,7,8
Currently, both patients are asymptomatic at six months and three months, respectively, after the surgery. Although the aortic uncrossing procedure provides total anatomical correction, it requires hypothermic circulatory arrest. The results of the procedure as a primary strategy even without aortic obstruction are promising with the advent of improved perfusion techniques to reduce perioperative morbidities and thus should be advocated.
Footnotes
Authors' Statement
Informed consent was taken from the patients’ guardians to publish this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.