
Abstract
Kawasaki disease (KD), the leading cause of acquired heart disease in children in developed countries, merits conducting detailed studies in Arab countries. We introduce Kawarabi, as a multicenter research collaborative effort dedicated to improving diagnosis, care, and outcome of children and adults with KD in the Arab world. During the COVID-19 pandemic, there emerged a new multisystem inflammatory syndrome in children; a disease similar to KD. This highlighted the challenges that Arab physicians face in diagnosing and managing children with KD and KD-like illnesses. Kawarabi brings together experts in North America and Arab nations to study this family of diseases in a not-for-profit, voluntary scientific collaborative setting. Bylaws addressing the vision, objectives, structure, and governance of Kawarabi were established, and vetted by the 45 organizing members in 2021. An initial scientific publication showed evidence of a decreased level of awareness of the disease in the general population, as well as the lack of access to resources available for physicians caring for children with KD in Arab countries. Kawarabi has since held several educational webinars and an inaugural yearly meeting. The groundwork for future initiatives targeted at increasing awareness and understanding of the management and the long-term outcomes of children with KD in the region was established. Data on KD in the Arab world are lacking. Kawarabi is a multicenter research collaborative organization that has the unique resources, diversified ethnic makeup, and energy, to accomplish significant advances in our understanding and management of KD and its variants.
Introduction
Kawasaki disease (KD), a systemic vasculitis, is the leading cause of acquired heart disease in children less than five years of age in high-income countries. 1 These children are at risk of developing coronary artery aneurysms, leading to coronary artery stenosis, myocardial infarction, and death. 1 Morbidity and mortality in children with KD decreases significantly with timely diagnosis and prompt management using intravenous immunoglobulins (IVIGs 2 g/kg) within the first ten days of fever. 1
Kawasaki disease has been extensively studied in North America, Far East Asia, and Western Europe with an incidence as high as 308 cases per 10,000 children who were less than five years of age Japan. 2 This is 10 to 20 times the incidence rates reported in North America and Europe. 3 Robust nationwide data from low- and middle-income countries are lacking and rarely include Arab countries.4,5 The Arab world is comprised of 22 countries in the Middle East and North Africa.
The rates of KD in Arab countries are underestimated probably due to decreased awareness or underreporting of cases. Based on single center experience and case reports the incidence of KD is 2.5/10,000 to 7.4/10,000 in the Arab world with a reported 10-fold increase over the past decade in some countries.6,7 In Northern African Arab countries, it is 4 to 12 times lower compared with the relative incidence of KD among descendants of the same nations living in the province of Quebec in Canada. 8 In a single center study from Egypt, 40% of children with KD were treated more than ten days after fever onset. The rates of aneurysms were approximately 50%; half of those were large aneurysms associated with an exponentially high risk of coronary artery stenosis long term. 9 This would be 100 times the rate of large coronary artery aneurysms reported in Japan. 10 Furthermore, according to literature from Arab nations, there are limited data on the resources available for acute management and lifelong surveillance of KD.6,7,11,12
The Kawasaki Arab Initiative (Kawarabi) established in 2021 13 is a multicenter consortium that fosters collaboration between KD experts and maintains an active registry of KD patients to understand the epidemiology of KD and disease burden in the Arab world, including mortality and long-term morbidities in children and adults. This initiative also seeks to raise awareness of KD in the medical community and among the general population.
The aim of this article is to introduce Kawarabi to the international medical community and to discuss its vision, objectives, organizational structure, and future directions.
Methods
The COVID-19 pandemic and the emergence of the multisystem inflammatory syndrome in children (MIS-C), a disease similar in presentation to KD, led to faster virtual professional communication among those caring for children with KD. Webinars and ad-hoc web-based international meetings held by the International Kawasaki Disease Registry monitoring of COVID-19 pandemic and subsequently MIS-C shed light on the unique challenges faced by physicians in the Arab world caring for children with KD and MIS-C alike. Three pediatric cardiologists from North America, who are also coauthors of this paper (N.D. from St. Justine Children's Hospital, Montreal, Canada, A.S.H. from Children's National Hospital, Washington, DC, and N.C. from Icahn School of Medicine, Mount Sinai Kravis Children's Hospital, New York, NY, New York), initiated contact with colleagues from Arab countries, including the United Arab Emirates. (N.A., formerly Dubai) and Egypt (Cairo University Specialized Pediatric Hospital) as well as the then president of Pan Arab Congenital Heart Disease Association (PACHDA) (H.M.E). Discussions made it clear that a multinational registry of KD cases associating multiple Arab countries (all if at all possible) was imperative to collect robust data on KD and KD-related diseases and to understand the epidemiology of KD, the resources available for KD patients, as well as the long-term outcomes associated with KD in the region. This led to the establishment of the Kawarabi voluntary scientific collaboration, a not-for-profit consortium.
Results
Bylaws addressing the vision, objectives, structure, and governance of Kawarabi were presented and vetted by 45 members, on February 27, 2021.
Vision Statement
Kawarabi is a voluntary, not-for-profit scientific collaborative organization dedicated to improving diagnosis, care, and outcome of children and adults with KD across the Arab nations and ethnicities.
Objectives
The objectives of Kawarabi are the following:
Fostering research and multicenter collaboration between academic institutions in the Arab world in the field of KD and similar diseases. Improving accurate diagnosis, timely therapy, and reducing morbidity and mortality in patients with KD and similar diseases. Promoting cardiovascular surveillance and management of KD patients with coronary artery complications from onset throughout adult life. Maintaining a registry of children and adults in the Arab world with KD or similar diseases.
Structure
The consortium is governed by a steering committee (SC) that supervises the advocacy, research, and educational endeavors of Kawarabi (Figure 1). It builds bridges with other KD societies such as the International Kawasaki Disease Registry (IKDR) and Arab Medical bodies such as Pan Arab Congenital Heart Disease Association (PACHDA) to increase KD awareness. It reviews research proposals, supervises research projects, maintains the data quality of the registry, and meets quarterly with all members. It organizes in-person and virtual education webinars as well as a yearly scientific meeting.
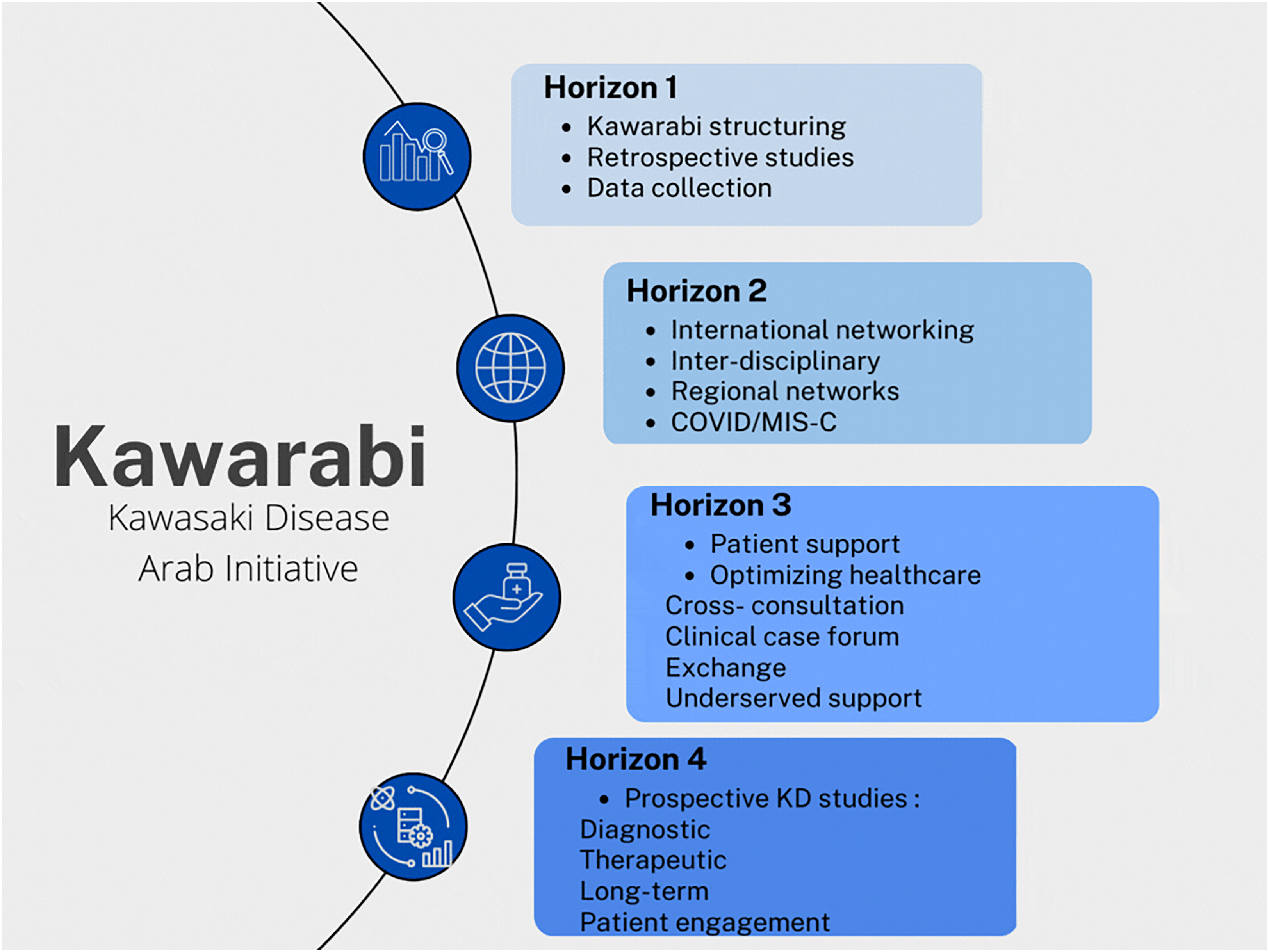
The development plan of Kawarabi divided in four horizons.
The SC is composed of founding members, a data center coordinator, a PACHDA liaison representative, and three regional lead representatives from the following three geographical regions: the West (Libya, Algeria, Tunisia, and Morocco), the Gulf (Kuwait, United Arab Emirates, Oman, Qatar, Bahrain, and Saudi Arabia), and the East (Egypt, Jordan, Lebanon, Palestine, and Syria). The lead representatives rotate every two years. The data coordinating institution (DCI) is St. Justine's Children's Hospital, Montreal, Quebec, Canada. English is the official language for all Kawarabi regulatory and educational publications and research-related documents and minutes.
Membership
Each medical institution in the Arab world caring for children with KD or similar illnesses can become a member by invitation from or by submitting a request to the SC. Currently, 24 centers from 15 Arab countries are fully onboard (Figure 2).
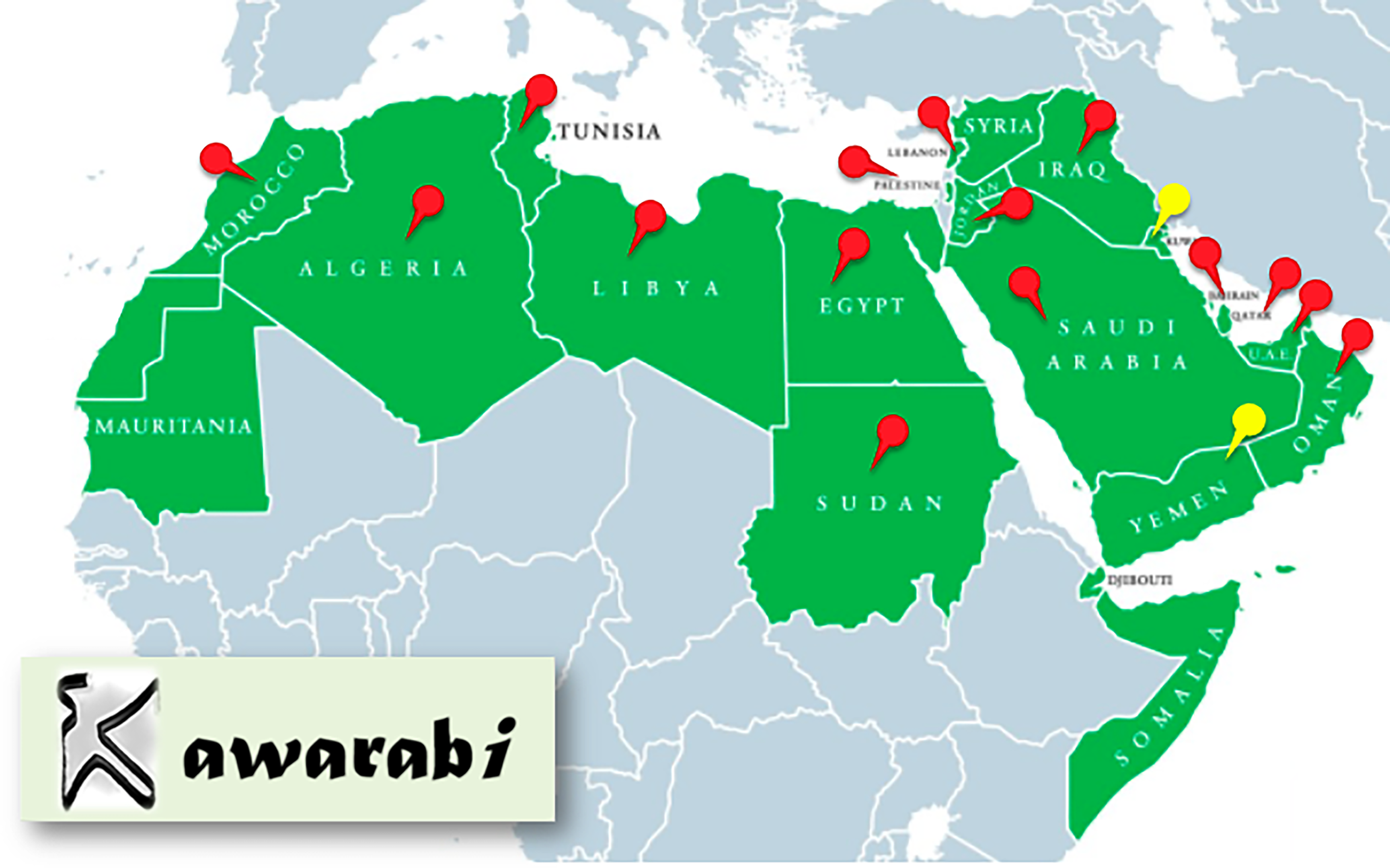
Countries that are part of Kawarabi. The red pins represent the 15 official members and the yellow pins represent two countries recruited (Kuwait and Yemen) still working on their onboarding.
Each institution identifies a primary site investigator (PI), secures an appropriate research infrastructure that abides by its regulatory board, and works directly with the DCI to maintain a high level of data quality.
Members will vote on all Kawarabi matters with one vote per institution. A quorum will consist of representation from 60% of the member institutions’ PIs, and 75% is the required quorum for changes to the bylaws. Institutions may designate a proxy for voting purposes.
Data Ownership, Management, and Analysis
Each site will sign a data sharing agreement with the DCI, obtain appropriate Institutional Review Board (IRB) approval before submitting any patient data, and arrange for consent of patients as required by their local IRB requirements. Each patient will be given a registry code. Deidentified data will be submitted using that code. Only collaborators within the center will have access to linking the registry code to the identity of the patient.
Member sites retain ownership of their own data that they submit to the registry. They may request that Kawarabi release their own data back to them (data export) so that they may collaborate with other investigators. These studies will not be considered “Kawarabi” studies. Research proposals are submitted to and approved by the SC. They include a brief description of the study, the expected involvement of each investigator, and a timeline for study completion.
Data analysis is performed by the DCI or another member site appointed by the SC. Only records validated by the DCI are considered in the data analysis.
First and senior authorship (+ DCI authorship) will be decided at project inception. Each institution nominates up to two primary authors to participate in the study. Order of primary authorship is decided using a point system: contribution to the manuscript (50 points), number of patients contributed to the registry (25 points), and quality and completeness of data (25 points).
Kawarabi members or sites who are not in the primary authorship group and who have contributed data to the analysis but did not meet authorship criteria will be listed alphabetically in the Kawarabi group appendix that will be submitted with each manuscript. This appendix will be searchable in PubMed.
Within 30 days of DCI receipt of a member site's written notification of withdrawal, data will be removed from the registry, returned to the member site, or destroyed, at member site's option and expense. This excludes data that have already been analyzed and/or published.
Research and Educational Activities
Two scientific articles have been published from Kawarabi since its inception. The first scientific publication from the Kawarabi collaborative in May 2022 13 found significant practice variation in KD management among Arab countries that resulted mainly from variability in the medical resources available as well as the low level of awareness in the general population. 13 The second article published in May 2023 showed that ease of access to care favored large and mid-size cities over rural areas in almost half of the surveyed member countries of Kawarabi. 14 Four virtual educational webinars moderated by national and international leaders in the field of KD have been held to address the epidemiology of KD and MIS-C in various Arab countries and were well attended by approximately 100 participants per webinar.
Kawarabi held its first in-person scientific meeting at the 11th International Pediatric Conference (https://kidsheart.ae/11-th-kidsheart-conference) in collaboration with Kids Heart Medical Center, November 11-13, 2022. Speakers from different Arab countries and from North America focused on sharing their institutional and regional experience in the diagnosis and management of KD and MIS-C and the challenges faced.
Discussion
We present the inception of the first regional initiative to study the epidemiology and long-term outcomes of KD in the Arab world. Consortiums and research collaboratives to study rare diseases or rare complications of diseases have been proven to be effective in improving our understanding of the disease process and have led to the development of new diagnostics and treatments.15,16 Specific to KD, the IKDR was established in 2013 along with those principles with the main aim to study the outcomes of children with KD and coronary artery aneurysms. It includes eight countries and more than 1,600 children with KD and coronary artery aneurysms. The majority of participants are from North America, Western Europe, and Taiwan. 17 Similarly, the Latin American Kawasaki disease network Red de Enfermedad de Kawasaki en America Latina (REKAMLATINA) established in 2013 with more than 100 centers from 20 countries focuses on assessing the disease burden of KD in Latin America. 18
The Arab world differs from other nations in its ethnicities and available resources. Consanguineous marriages are highly prevalent in parts of the Arab world: close to 50% in Jordan, 19 Qatar, 20 United Arab Emirates, 21 Saudi Arabia, 22 and Yemen. 23 This offers the perfect environment to study the genetic basis of KD. Data from Japan show that the rate of KD in a sibling one year after the index case is 2.1% which is 10 times higher than the general population in Japan. 24 Those statistics have been difficult to replicate in North America and Europe because of the ethnically diverse population.
Based on the two surveys published by Kawarabi, resources available for children with KD in Arab countries vary widely. There are significant practice variations in the management of KD, a low level of awareness of the disease in the general population, and access to care favors large to mid-size cities over rural areas in close to half of the participating countries.13,14 Ease of access to IVIG differs between institutions. 13 The lack of readily available IVIG combined with low awareness of the disease in the general population can potentially lead to underdiagnosis, delay treatment, and subsequently increase the risk of coronary artery aneurysms.
Those who develop large or multiple coronary artery aneurysms have a progressively increased risk of developing coronary artery stenosis and thrombosis up to 20% by ten years after the initial illness. Coronary artery revascularization for KD coronary lesions can be done with surgical coronary artery bypass grafting and percutaneous coronary intervention (PCI) procedures. 25 Access to coronary artery revascularization therapy in adults varies and remains suboptimal in some of the Arab countries despite having one of the highest mortality and morbidity rates from cardiovascular disease. 26 There are 1 to 5 adult cardiac surgeons per million population in Arab countries, a 10th or half of that seen in North America according to CTSNet. 27 In North African Arab countries, the use of PCI differs significantly between countries; only 2.5% of ST-segment elevation myocardial infarction (STEMI). are managed by early PCI in Algeria compared with 22% in both Morocco and Tunisia. Yemen and Oman have the lowest percentage of early PCI in the Middle East and North Africa. 28
Bylaws that cement the vision and objectives of a collaborative such as Kawasaki and that provide a solid infrastructure are vital for the success of the consortium. Bylaws were written and approved by members and participants. They serve as a set of rules to follow and to revert to in the event of a conflict. The Steering Committee is rotational and inclusive of regions as well as large and small institutions. Major decisions are suggested by members or by SC and voted for in order to be implemented. Votes are equal between large and small participating institutions (one vote per PI). The DCI at Saint-Justine Hospital in Canada will ensure that the data shared is of high quality, remains safe, and anonymous.
The active engagement of Kawarabi members during virtual webinars, the inaugural yearly meeting, as well as the publication of two manuscripts13,14 proves promising for the conduct of nested clinical trials on KD within the collaborative in the future. Clinical trials for rare diseases similar to KD and MIS-C require a collaborative multicenter approach as is evident in the trial investigating the role of etanercept and infliximab as an adjunct therapy for KD.29,30 Those endeavors will serve to educate physicians, collaborate on research work, and advocate for the care of children with KD by increasing awareness in the medical community.
Future plans are divided into several horizons as shown in Figure 1. Horizon 2 will permit the established initiative to participate in interdisciplinary and regional/international networks such as IKDR including data gathering on COVID-19 and MIS-C cases. Thus, horizons 1 and 2 will guarantee a solid foundation and visibility of the initiative and affiliated institutions. All efforts will permit moving into Horizon 3 with optimizing healthcare and patient support (cross-consultation, clinical case forum, interdisciplinary exchange, and underserved support). This will be in the form of a multidisciplinary health community with strong scientific ties that will link university-affiliated hospital centers to regional or rural hospital centers for continuous updates on clinical care and knowledge. A platform with resources readily available in Arabic, English, and French (two foreign languages commonly used according to specific countries) to patients and their families will be developed to improve their understanding of the disease and their access to medical care. This will finally lead to horizon 4; prospective KD studies will be designed to address diagnostic, therapeutic, and long-term patient engagement.
Conclusion and Future Directions
Kawarabi's first year since inception focused on structuring, recruitment of participating centers, and implementation of the first retrospective multinational KD study in Arab countries. Future plans include achieving local and international collaborations, optimizing healthcare and patient support, and developing providers and patients’ platforms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.