
Abstract
Background
The optimal approach to patent ductus arteriosus management during systemic-to-pulmonary artery shunt placement is currently unknown. The purpose of this study is to examine the outcomes of variable strategies for patent ductus arteriosus management during Blalock-Taussig-Thomas shunt surgery.
Methods
A retrospective cohort study of infants who underwent shunt placement was performed, comparing those who had the ductus ligated with those who had the ductus left open. Indicators of low cardiac output syndrome, development of necrotizing enterocolitis, and secondary outcomes such as resuscitation events were examined.
Results
Thirty-six infants were included all of whom had their shunt placed via median sternotomy. Twenty infants had their ductus ligated at the time of the shunt, and they were compared with 16 infants whose ductus was left open. There was no statistical difference in preoperative baseline characteristics, including corrected gestational age, age in days, weight, mechanical ventilation, vasoactive use, heterotaxy, and gastrointestinal anomalies. There was also no statistical difference in postoperative indicators of low cardiac output, including urine production, total fluids given, renal injury, maximum lactate, and vasoactive-inotropic score. Three patients had postoperative renal injury, and all were in the ligated duct group. There was also no statistical difference in any secondary outcomes, including the development of necrotizing eneterocolitis, resuscitation events, reinterventions, length of intubation, total length of stay, and mortality.
Conclusions
This study provides evidence that variable management of the ductus during shunt placement does not significantly impact outcomes. Leaving the ductus open allows for a potential rescue source of pulmonary blood flow and does not appear to increase the risk of postoperative low cardiac output.
Introduction
The modified Blalock-Taussig-Thomas shunt (BTT shunt) is constructed by placing a vascular graft between the innominate artery and a branch pulmonary artery (PA) to provide a stable and adequate source of pulmonary blood flow when one does not exist. 1 Two major types of complications with this connection are low systemic perfusion secondary to pulmonary overcirculation and insufficient pulmonary blood flow from shunt thrombosis.2,3 After a BTT shunt, there is typically one ventricular outflow tract supplying both systemic and pulmonary circulations, and the goal is to balance the perfusion to both circulations. Disruption of this balance can lead to morbidity and mortality, especially in the initial postoperative period. 2
Maintaining a patent ductus arteriosus (PDA), which supplies pulmonary blood flow preoperatively, is no longer required long-term after BTT shunt placement. Intraoperative management of the PDA is surgeon-dependent. It can be ligated if the surgical approach allows or be left patent to close more gradually once prostaglandin is discontinued. The postoperative impact of having the PDA ligated or left open is unclear. Theoretically, if a PDA is left patent with a BTT shunt, the two sources of pulmonary blood flow may result in pulmonary overcirculation. In addition to the associated pulmonary edema and venous congestion that could occur in an already inflamed postoperative state, this increased pulmonary perfusion could result in systemic underperfusion and end-organ damage, also referred to as low cardiac output syndrome (LCOS). Yet, if shunt occlusion occurs, the PDA may become lifesaving by providing an alternate source of pulmonary blood flow in the perioperative period.
The approach to PDA management during BTT shunt has been studied only to a limited degree, 4 and the best approach is unknown. The purpose of this study is to examine the outcomes of variable PDA management during BTT shunt placement.
Patients and Methods
Patient Population
In 2019, there was a programmatic shift to start leaving the PDA open in all patients undergoing BTT shunts at our institution. The reason for this decision was to give a potential rescue option (opening the PDA via prostaglandin infusion) if acute shunt thrombosis occurred in the immediate postoperative period. It was further hypothesized that a gentler transition to pure shunt physiology could be beneficial. After an extensive literature review, little information was found about this strategy, so it was decided to carefully evaluate the first cohort of shunts with the new strategy and compare them with the previous group to ensure that there were no unexpected complications due to potential competing blood flow. This was the only change in surgical management, and there was no change in surgical or intensive care unit (ICU) personnel during the study period. This provided the opportunity to have an historical control group.
A single center retrospective cohort study of all infants receiving a BTT shunt from 2016 through 2021 was thus performed to compare those who had the PDA ligated with those whose PDA was left open. Exclusion criteria included corrected gestational age less than 35 weeks, weight less than 2,000 g at the time of surgery, absence of a PDA preoperatively or the use of cardiopulmonary bypass (CPB) intraoperatively. Patients with multiple sources of pulmonary blood flow specifically from major aortopulmonary collateral vessels without confluent pulmonary arteries were excluded.
Patients with prematurity and small size were excluded due to the known increased surgical risk in those populations to limit confounding.5,6 Those without a PDA preoperatively were also excluded given the apparent lack of total reliance upon a shunt for pulmonary blood flow and because the PDA was neither ligated or left open. Patients on CPB for shunt placement were also excluded as all CPB cases had their PDA ligated and because the systemic inflammatory response induced by CPB results in increased pulmonary vascular resistance (PVR) as well as myocardial injury that can ultimately reduce cardiac output. 7
All shunts placed during the study period were 3.5 mm in diameter Gore-Tex grafts sutured in place with 8-0 prolene from the base of the innominate artery and into the midportion of the right PA distally. A dose of 400 U/kg of heparin was given prior to shunt placement and 10 U/kg/h was standardly infused postoperatively until the patient was on full feeds. All patients were then sent home on 41 mg of ASA daily. When the PDA was ligated it was done with a suture. Patients with left BTT shunts were excluded due to conflicting duct anatomy.
Patients were stratified to the PDA ligated group if PDA ligation was performed during the operation per the operative note or if a PDA ligation procedure code was entered in the BTT shunt operative note. Patients were stratified to the PDA left open group if it was reported in the operative note, postoperative echocardiogram report or postoperative progress note that the PDA was left open.
Baseline characteristics with potential impact on observed outcomes were collected, including corrected gestational age at surgery, age in days at operation, weight at operation, preoperative use of mechanical ventilation, use of preoperative vasoactives, heterotaxy, and gastrointestinal (GI) anomalies. PDA dimensions were taken from the suprasternal notch view on the echocardiogram done just prior to surgery.
End Points
Postoperative outcomes that indicated the presence of LCOS were collected, including the postoperative vasoactive inotropic score (VIS), lactate levels, and the presence of acute kidney injury (AKI). Vasoactive inotropic score was calculated using the equation, dopamine dose (µg/kg/min) + dobutamine dose (µg/kg/min) + 100*epinephrine dose (µg/kg/min) + 10*milrinone dose (µg/kg/min) + 10000*vasopressin dose (U/kg/min) + 100*norepinephrine dose (µg/kg/min). 8 The score was examined for the first 72 h postoperatively, and the maximum score determined. Every lactate level measured in the first 72 h postoperatively was further recorded. Acute kidney injury was defined as having a postoperative increase in creatinine of at least 0.3 µmol/L within a 48-h period and/or developing a decrease in UOP to less than 1 mL/kg/h in the first postoperative 48 h and 72 h. Total fluid volume per weight administered, lowest pH, maximum lactate, and lactate area under the curve during the first 72 h postoperatively were determined.
Documentation of the development of necrotizing enterocolitis (NEC) during the same hospitalization was noted. Necrotizing enterocolitis was defined as the presence of any symptoms with simultaneous radiographic evidence of NEC. Symptoms of NEC were defined as the presence of bilious gastric aspirate or emesis, abdominal distension, or occult/gross blood in stool. Radiographic evidence of NEC was defined as the finding of pneumatosis intestinalis, hepatobiliary gas, or pneumoperitoneum. Duration of NPO (nothing by mouth) status was noted, as well.
Other outcomes collected included whether a resuscitation event occurred in the first 72 h postoperatively, whether reintervention occurred during the hospitalization, length of intubation, length of cardiac intensive care unit (CICU) stay, total length of stay, and occurrence of mortality. A resuscitation event was defined as the need for chest compressions, administration of an epinephrine bolus or placement on extracorporeal membrane oxygenation (ECMO). Reintervention was defined as an unplanned cardiac surgery or cardiac catheterization.
Statistical Analysis
Continuous variables were compared using appropriate parametric and nonparametric testing after assessing for normality. For those continuous variables with a non-normal distribution, a median was calculated and compared among the two patient groups using a Mann-Whitney U test. For lactic acid levels measured in the first 72 h of life, an area under the curve was calculated for each patient and compared appropriately. Negative binomial regression was performed for continuous variables to adjust for potential confounders. Development of NEC and time to feed initiation were adjusted for GI anomalies. Mortality was adjusted for preoperative inotropic support. Length of intubation was adjusted for preoperative mechanical ventilation. Categorical variables were compared using a chi-squared test, and logistic regression was performed to find the odds ratio for the PDA ligated versus the PDA left open groups after assessing descriptively and adjusting for known confounders. P-values were assumed to be significant if less than .05. All statistical calculations was performed using SAS (SAS Institute).
Results
Baseline Characteristics
There were 48 infants who underwent BTT shunt placement during the study period. Of these, two were excluded due to absence of the PDA preoperatively, and ten were excluded due to use of CPB intraoperatively. In four of these cases, the shunt was initially done off pump, but following significant desaturations, it was felt that revision was necessary and the patient was converted to CPB because of instability. In the others, decompensation and desaturations during initial dissection led to the decision to go on CPB to provide stability. In all cases, CPB was initiated with a single aortic and single venous canula. The PDA was ligated in all of these patients on CPB.
In total, 36 infants remained and were included in the study. This included 20 patients who had their PDA ligated and 16 who had their PDA left open. Baseline characteristics are listed in Table 1. There was no significant difference in baseline characteristics (Table 1). Only one patient required mechanical ventilation preoperatively, and that patient was in the PDA ligated group. All patients requiring inotropic support preoperatively were on milrinone. None of the patients from either group required epinephrine, vasopressin, dopamine, dobutamine, or norepinephrine preoperatively.
Baseline Characteristics of the 2 Groups. a
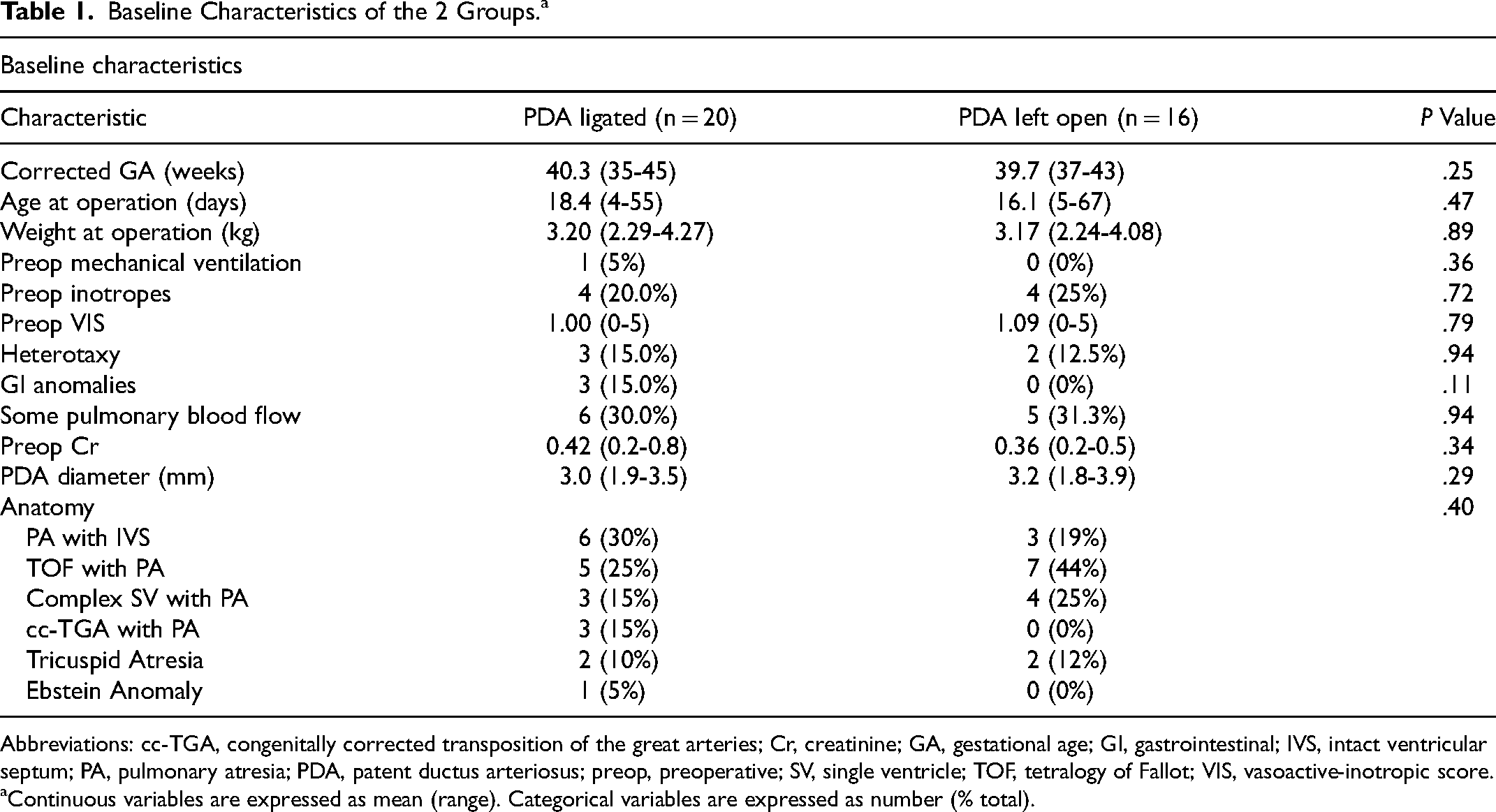
Abbreviations: cc-TGA, congenitally corrected transposition of the great arteries; Cr, creatinine; GA, gestational age; GI, gastrointestinal; IVS, intact ventricular septum; PA, pulmonary atresia; PDA, patent ductus arteriosus; preop, preoperative; SV, single ventricle; TOF, tetralogy of Fallot; VIS, vasoactive-inotropic score.
Continuous variables are expressed as mean (range). Categorical variables are expressed as number (% total).
Although the difference in the number of patients with GI anomalies between the two groups did not reach statistical significance, there were three such patients in the PDA ligated group and none in the PDA left open group. Of the three patients with GI anomalies, two had malrotation, and one had NEC with perforation requiring ileostomy prior to BTT shunt placement. One of the patients with malrotation developed NEC postoperatively. There were no patients in either group where the PDA was felt to be solely responsible for perfusion to an arterial segment that could not be achieved by a shunt.
Indicators of LCOS
There was no statistical difference in indicators of LCOS between the PDA ligated and PDA left open groups (Table 2). The mean maximum VIS did approach statistical significance with the PDA ligated group at 13.1 and the PDA left open group at 8.7 (P = .057). Mean UOP and mean total fluids given were not different between the two groups either in the first 48 h or 72 h postop. Three patients were found to have postoperative AKI, and all were in the PDA ligated group. All three cases of AKI were based on changes in creatinine rather than urine output. The mean maximum lactate was not different in the PDA ligated group (4.23) compared with the PDA left open group (2.7), P = .085.
Indicators of LCOS in the 72-h Postoperative Period Along With Secondary Outcomes. a
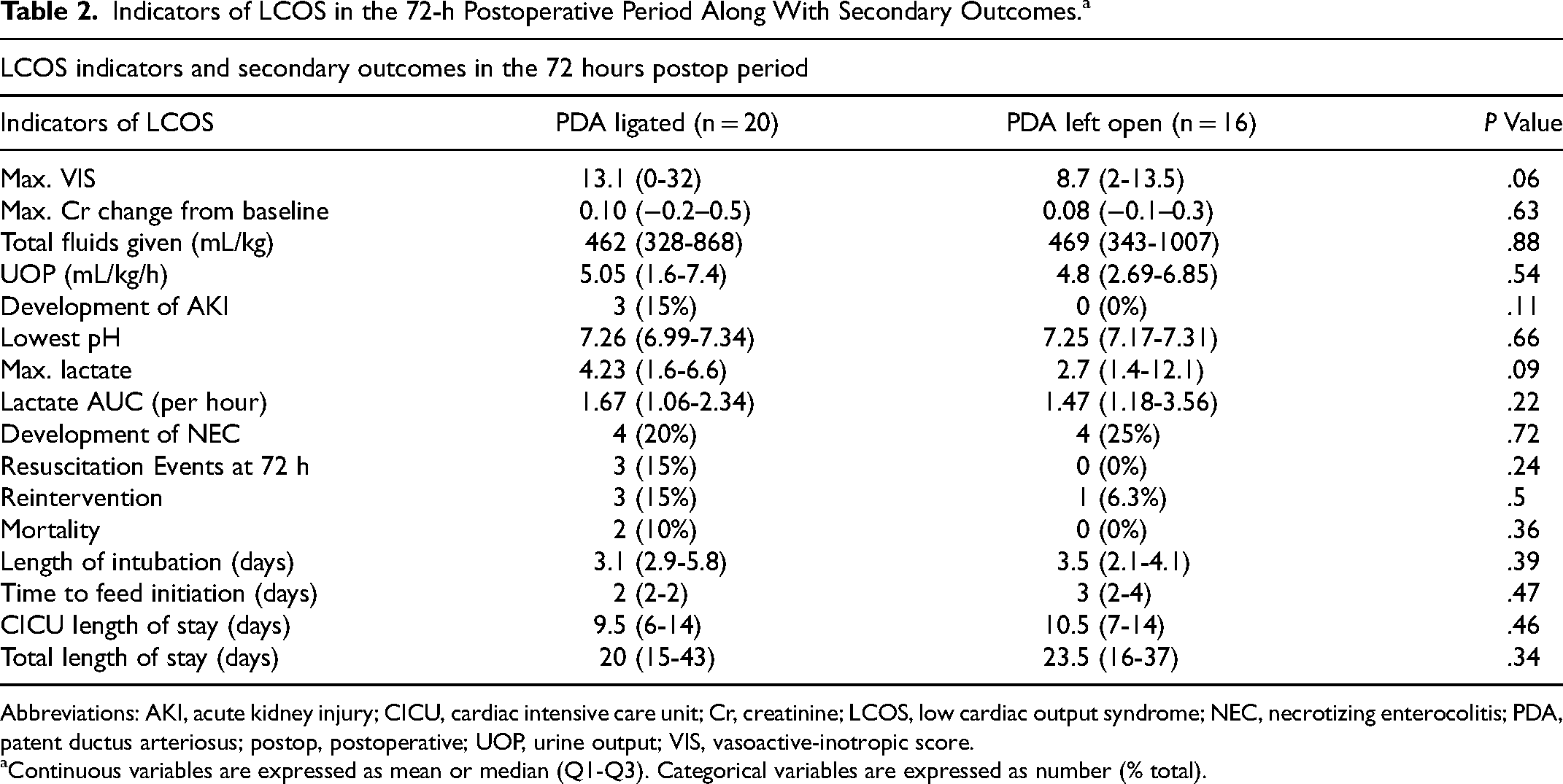
Abbreviations: AKI, acute kidney injury; CICU, cardiac intensive care unit; Cr, creatinine; LCOS, low cardiac output syndrome; NEC, necrotizing enterocolitis; PDA, patent ductus arteriosus; postop, postoperative; UOP, urine output; VIS, vasoactive-inotropic score.
Continuous variables are expressed as mean or median (Q1-Q3). Categorical variables are expressed as number (% total).
Secondary Outcomes
There was no statistical difference found between the two groups in any of the secondary outcomes (Table 2). Figure 1 shows the tendency for more adverse outcomes to occur in the PDA ligated group, although not to a significant degree. This is true except for NEC and time to feeding which occurred more often in the PDA left open group although again, not significantly more. There was one patient in the PDA left open group who required reintervention due to shunt occlusion, and that patient was placed on prostaglandin E-1 (PGE) until Sano shunt placement. Figure 2 shows the proportion of each group over time to remain intubated (Intubation time), remain NPO (Feeding time), remain in the CICU (CICU LOS), and remain in the hospital (Total LOS). Although there was no significant difference between the two groups, Figure 2 demonstrates that the PDA ligated group had more outliers on the longer end of all these outcomes.
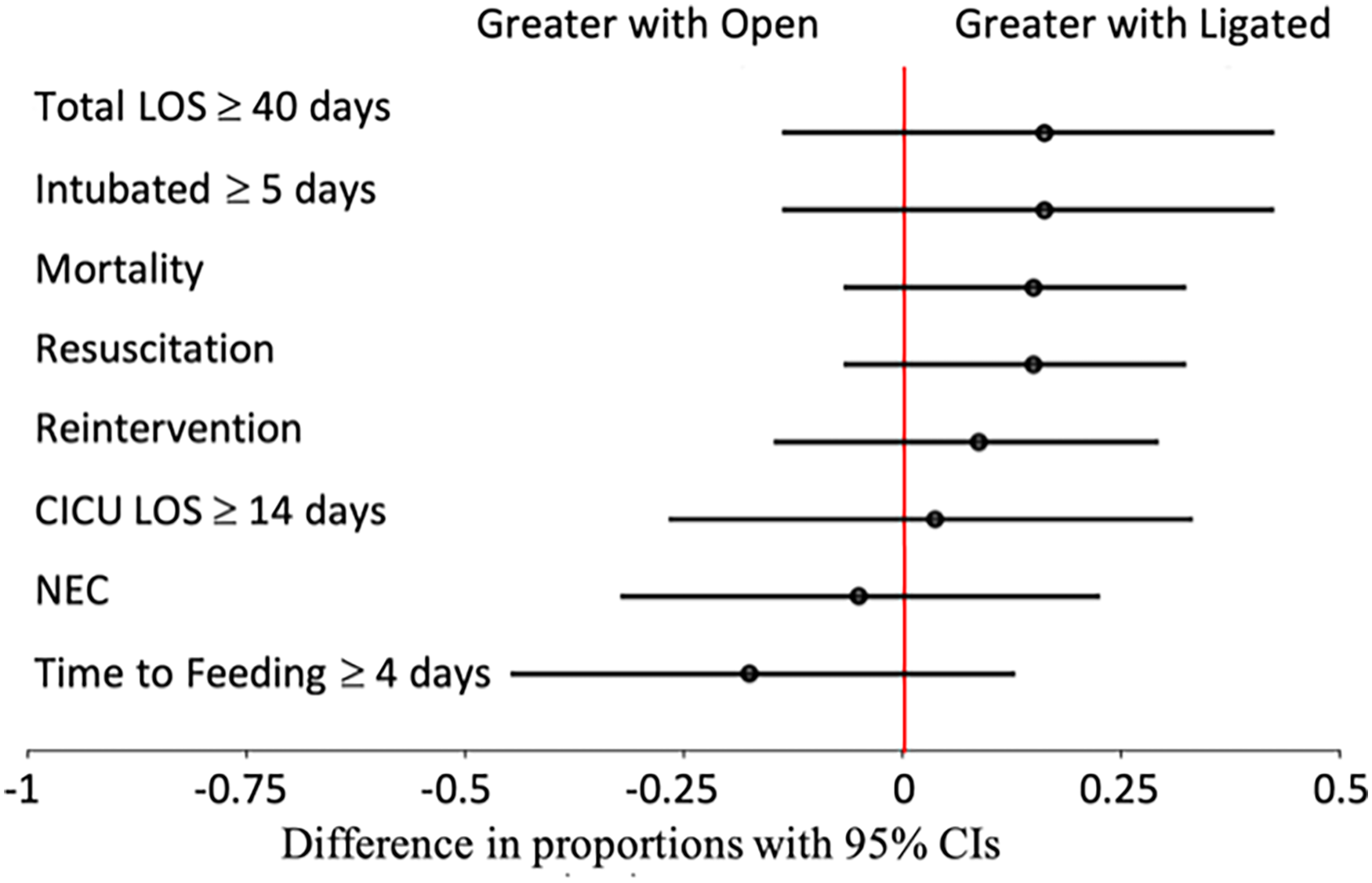
Difference in proportions for secondary outcomes of those with patent ductus arteriosus left open versus ligated.
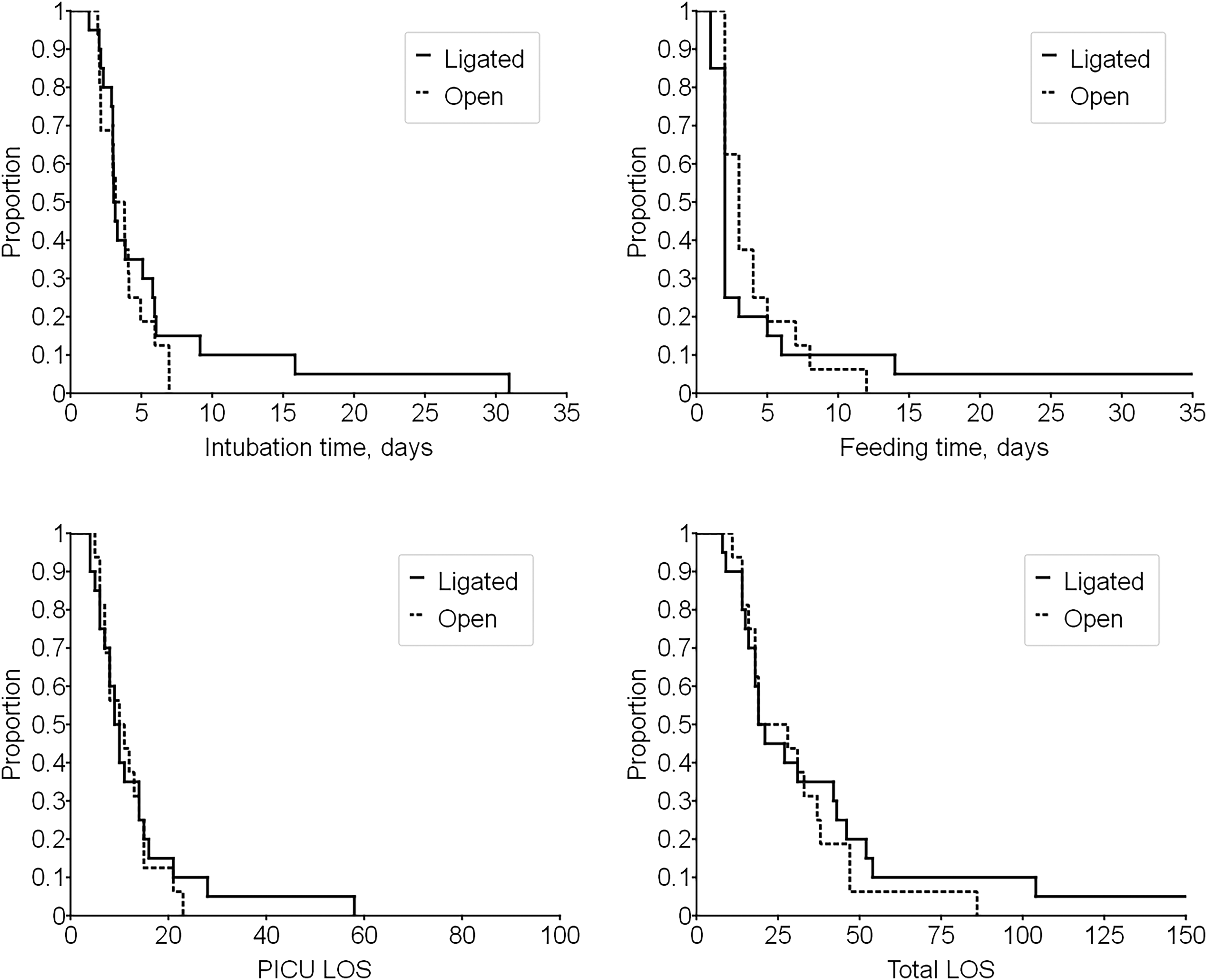
Intubation time, feeding time, CICU length of stay, and total length of stay of patients with patent ductus arteriosus left open (dash line) or ligated (solid line) over time.
Each group had four patients who developed NEC postoperatively. Two of the four in the PDA ligated group had GI anomalies. There were three patients with resuscitation events, all of whom were in the PDA ligated group. All three required epinephrine boluses and chest compressions, and two of the three required ECMO. None of the patients requiring resuscitation had a mortality. Four patients required reintervention during their hospitalization. One of these patients was in the PDA left open group and underwent right ventricle-to-PA conduit placement after cardiac catheterization revealed obstruction of the BTT shunt. The other patients were in the PDA ligated group. One patient had a thrombosis surgically removed from the BTT shunt the night after shunt placement. One patient required stent placement for BTT shunt occlusion. Another patient had a catheterization the day after shunt placement due to hemodynamic collapse, but no catheterization-based interventions were performed. None of the patients requiring reintervention had a mortality.
Of note, the number of patients undergoing PA interventions, either with cardiac catheterization or with surgery, within one year of BTT shunt placement was noted for each patient group. Of the 36 patients in the study, 25 (69%) had data available through one year after BTT shunt placement, including 14 patients from the PDA ligated group and 11 from the PDA left open group. Of these, three from the ligated group required PA intervention within a year of BTT shunt placement (3/14, 21%) and five from the left open group (5/11, 45%) All PA interventions were surgical and occurred along with the next planned surgery (such as Glenn or Tetralogy of Fallot repair) except for one patient in the PDA left open group who additionally required multiple catheterization-based interventions to address the pulmonary arteries. One of the patients in the PDA left open group requiring PA intervention was the same patient who benefited from restarting PGE when the BTT shunt occluded on postoperative day two.
There were two mortalities in the study population and both whom were in the PDA ligated group. Both patients were born at term and were over a week old at the time of surgery. The first patient began having seizures on POD 20 that progressed to status epilepticus and pulseless arrest. After a brief ECMO run, care was redirected due to a nonreassuring EEG. The second suffered an unexplained cardiac arrest on POD 14 while on step-down status and working on feeds. The cause of the arrest was unknown but was unrecoverable.
Comment
The results of this study demonstrated no significant difference in outcomes as to whether the PDA was ligated at the time of BTT shunt placement when CPB is not utilized. Mean maximum VIS, development of AKI, mean maximum lactate, resuscitation events, reintervention, and mortality were all higher in the PDA ligated group but not to a significant degree.
Low cardiac output syndrome is a decrease in cardiac output following surgery for congenital heart disease and is a commonly encountered postoperative problem. 7 It is associated with significant morbidity and mortality, 9 and for this reason, has been a frequently discussed and researched topic with the goal of predicting its occurrence and treating it most effectively when it does occur. In the patient with a BTT shunt and only one adequate great artery, low cardiac output has effects on both systemic and pulmonary perfusion. The goal of postoperative management is to maintain a balanced circulation, providing both adequate systemic perfusion and enough pulmonary blood flow for oxygenation to occur. There is concern that systemic and pulmonary blood flow are unbalanced when there are multiple sources of pulmonary blood flow such as a PDA and a BTT shunt, leading to low cardiac output.10,11 However, there has not been evidence to support this theory.
In addition, 19% of patients in the PDA left open group had pulmonary atresia with intact ventricular septum (PA/IVS). Individuals with this condition are prone to the development of coronary artery anomalies. 12 Having two sources of shunt blood flow with these individuals could theoretically further reduce diastolic pressure and cause coronary steal from an already fragile coronary vascular bed. 13 Despite this very real risk, none of the patients in this study with PA/IVS had signs of reduced coronary perfusion as indicated by sudden hemodynamic changes, ST segment changes or a higher incidence of LCOS compared with the control group.
To our knowledge, there has been only one prior study directly assessing the question of PDA management during BTT shunt placement. A single center retrospective observational study in Slovakia included 62 patients with pulmonary atresia undergoing BTT shunt and found that patients with a PDA left patent had lower rates of resuscitation events, reinterventions, and early mortality. 4 This study looked at data from a 13-year period, starting in 1997 and included the procedures of nine surgeons at that institution. Another study comparing surgical approach, sternotomy with PDA ligated versus thoracotomy with PDA left patent, found no differences in outcomes. 14 However, a case series of three PDAs not ligated described deaths in all three. 11 There is also a study that used 3D modeling to compare the predicted pulmonary circulation and thrombotic risk and found both pulmonary hyperperfusion and increased risk of shunt thrombosis in models with an open PDA. 10
This study provides a new comparison of PDA management styles. It includes data from nonsimulated clinical scenarios. All patients in this study underwent sternotomy, so there was no difference in surgical approach between the two groups. Further, all surgeries were performed by the same surgeons within a five-year period, potentially minimizing confounding factors such as surgical technique and post-surgical management. The results of this study are in keeping with the single prior similar study done in Slovakia. Overall, an intact PDA does not appear to pose a significant risk for excess pulmonary blood flow and subsequent systemic underperfusion. This is evidenced by the lack of difference in signs of low cardiac output such as AKI, need for inotropic support, and postoperative lactates. Prostaglandin E-1 was stopped postoperatively in all cases, allowing natural PDA closure in those with the PDA left open intraoperatively. Thus, the additional source of pulmonary blood flow from the ductus is only transient and occurs during a period when an elevated PVR is known to cause hemodynamic problems. 15
One patient from the PDA left open group suffered shunt occlusion. This patient was able to maintain pulmonary blood flow via the PDA by restarting PGE. Although the results of this study indicate that there is no significant difference in outcomes associated with PDA management in patients undergoing BTT shunt, this demonstrates a reason to leave the PDA open as the ability to reopen it postoperatively can be lifesaving in the event of shunt occlusion.
This study was limited by its small sample size and retrospective nature, both of which contributed to an inability to fully control for confounding factors. Analyzing the occurrence of some outcomes such as NEC was dependent upon the clarity of patient documentation. For those patients in the PDA left open group, it was not noted when the ductus closed on its own after BTT shunt placement as our center does not routinely do echocardiograms in the immediate (first 48 h) postoperative period unless there are hemodynamic concerns.
Variable management of the PDA during BTT shunt placement without the use of CPB did not significantly impact outcomes in our initial cohort. The findings of this study convinced our center to continue with this strategy as we had no issues with theoretical competing sources of pulmonary blood flow as evidenced by no significant increase in the risk of postoperative low cardiac output or widespread difficulty with the shunt from competing flow. In addition, leaving the PDA open allows for a potential rescue source of pulmonary blood flow as occurred in one of our patients. While these numbers are probably too small to draw definitive conclusions about the overall risk of competitive pulmonary blood flow, the results from this study were enough to convince our center to continue the strategy and demonstrates the need to perform a larger, probably multi-institutional, study to assess this potentially beneficial approach to shunt placement.
Footnotes
Abbreviations
Acknowledgments
The authors acknowledge the contribution of Dr Mark Conaway of the Division of Translational Research and Applied Statistics in the Department of Public Health Sciences at University of Virginia for performing the statistical analysis used in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.