
Abstract
Background
The repair of certain types of complex congenital cardiac defects may require a right ventricle-pulmonary artery (RV-PA) conduit. Using the Ozaki Aortic valve neocuspidization (AVNeo)technique, a valved RV-PA conduit was constructed with an Ozaki valve inside a Dacron graft. This study aims to evaluate the short-term outcome of the Ozaki valved RV-PA conduit.
Material/Method
A total of 22 patients received the Ozaki valved RV-PA conduit from November 2019 until December 2023. The median age was 12 years (interquartile range [IQR], 5.5-21), median body weight was 35 kg (IQR, 15.8-48.5). The conduit was used in 16 patients (72.7%) under 18 years of age. Indications for conduit placement included: anatomic repair of corrected transposition of the great arteries, ventricular septal defect/pulmonary stenosis, conduit replacement, pulmonary atresia with associated anomalies, pulmonary artery aneurysm with dysplastic pulmonary valve, tetralogy of Fallot with coronary artery crossing the right ventricular outflow tract, bioprosthetic pulmonary valve regurgitation, and rheumatic heart disease. Native pericardium was used for the Ozaki valve in 12 patients and bovine pericardium for 10 patients. Conduit sizes ranged from 18 mm to 30 mm.
Result
The median intensive care unit stay was 4 (IQR, 2-6) days and the median hospital stay was 9 (IQR, 5.5-13.5) days. There were two perioperative mortalities (9.1%) both unrelated to the conduit. The median follow-up was 12.3 (IQR, 4.43-21.2) months. There was no infective endocarditis of the conduit. The median peak gradient across the conduit was 22 mm Hg (range 0-44 mm), and all were competent with trivial regurgitation on follow up.
Conclusion
Creation of an Ozaki valved conduit is an attractive option due to low cost, reproducibility, and excellent hemodynamics. Longer-term studies are needed to confirm the durability.
Introduction
Biventricular repair of many complex congenital heart defects requires a valved right ventricle to pulmonary artery (RV-PA) conduit. Due to associated pulmonary regurgitation and its impact in the early perioperative period, nonvalved conduits are not optimal. Homografts, Xenografts, and synthetic valve grafts are often used in the developed world with good short and long term results. However, there are limited conduit options available in the developing world with minimal homograft availability at most centers. Commercially available synthetic valved conduits or xenografts such as bovine Jugular vein grafts are quite expensive. Pediatric cardiac caregivers in the developing world need less expensive and easily available RV-PA conduits. Many centers in developing nations use handmade RV-PA conduits with native pericardium, 0.1-mm expanded polytetrafluoroethylene (ePTFE) membrane, and bovine pericardium, within a pericardial tube. However, very few techniques using Dacron or PTFE grafts1–5; have been reported. In 2019, we reported our early experience with a handmade trileaflet valved conduit whereby autologous pericardial leaflets were sutured inside a Dacron graft using the Ozaki AVNeo technique. 6 Herein, we report an extension of our experience using this technique in patients undergoing complex congenital heart surgery and RV-PA conduit placement.
Material and Methods
This is a descriptive study done at G. Kuppuswamy Naidu Hospital, Coimbatore, Tamil Nadu, India. We included all patients who had an Ozaki valved RV-PA conduit at the time of biventricular repair from November 2019 to December 2023 in the study. Patients who were receiving repair without a conduit, nonvalved conduits, or commercially available conduits were excluded from the study. The demographic details of the patients, preoperative diagnosis, surgical procedure details, conduit sizes, material used for the valve leaflets, function of the valved conduit including gradient across the valve and regurgitation of the valved conduit in the operating room and the immediate postoperative period, perioperative events including mortality and morbidity and the function of the valved conduit during follow-up were collected retrospectively and analyzed. All the patient data were collected from outpatient medical records, operative notes, inpatient medical records, postoperative follow-up records, and direct telephonic interviews. We maintained confidentiality and privacy of all patients’ data throughout the study. All patients and their families consented to this study. The Institutional Ethics Committee approved the study.
Conduit Preparation and Operative Technique
After midline sternotomy, the pericardium was opened. The main pulmonary artery and both branch pulmonary arteries were dissected. The size of the pulmonary arteries was visually confirmed. The anterior pericardium in the primary cases or the available pericardium in the redo cases was harvested. The conduit is generally prepared after sternotomy and before going on cardiopulmonary bypass. The average time taken for conduit preparation was about 45 min. The operative technique for making the Ozaki valved conduit is described in our earlier publication. 6 Briefly, the harvested pericardium was cleaned and fixed to the stainless steel plate with multiple sutures. After cleaning and stretching, the pericardium was treated with 0.6% glutaraldehyde for 2 min and then washed with normal saline for a total of 18 min with three separate rinses at 6-min intervals. The primary surgeon created the Ozaki Valve inside the Dacron graft. However, the preparation of the native pericardium with glutaraldehyde and washing of the pericardium is done by a qualified assistant. Dacron grafts (Intergard Woven Grafts, Straight, Maquet) were used in all patients (Figures 1 and 2).
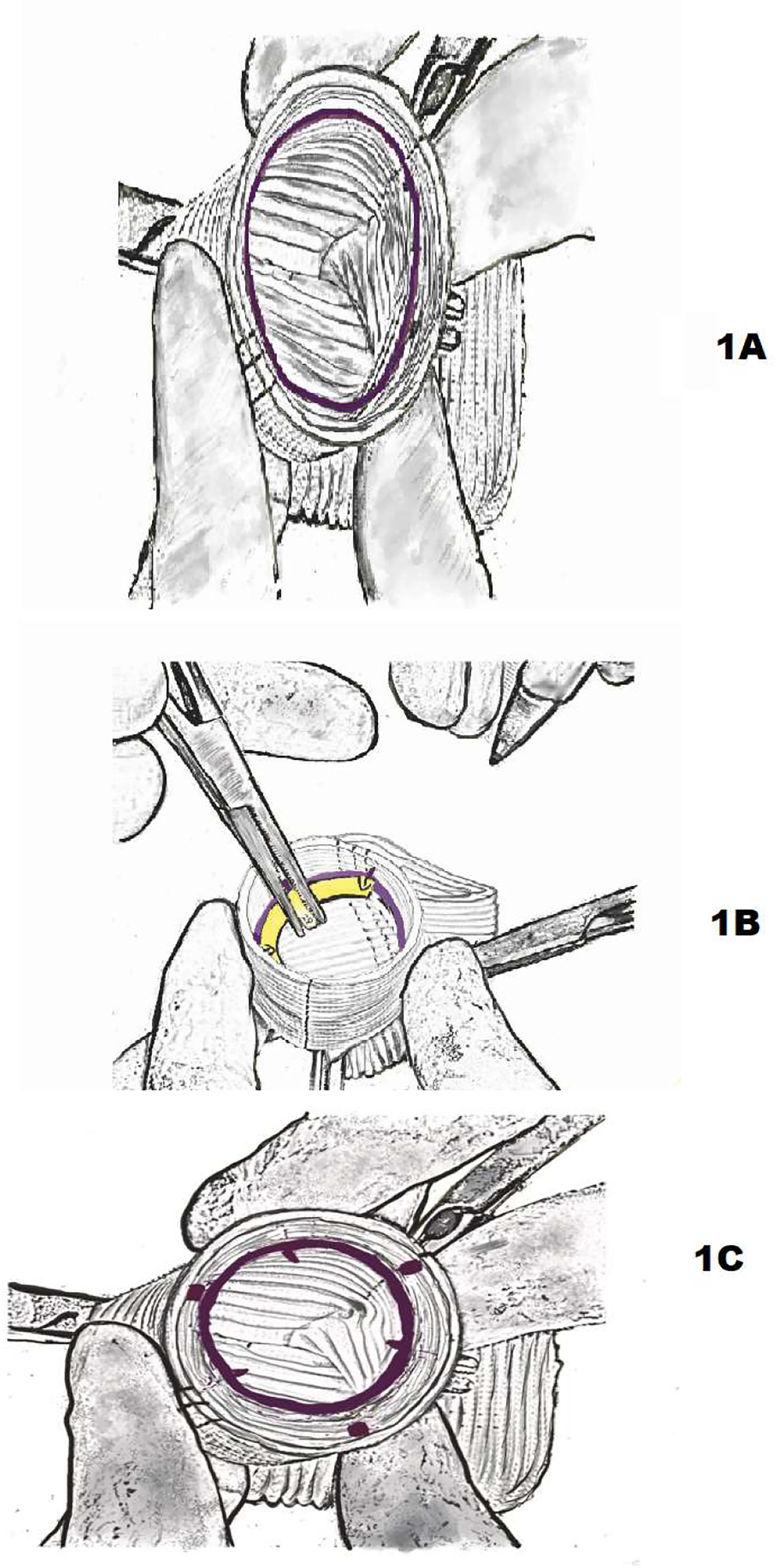
(A) Stabilization of Dacron graft on the operating table with a vascular clamp and marking the circle (mimicking annulus) about 1 cm from the edge of the Dacron graft using a marking pen. (B) Marking all the commissuresdd and centering each cusp within the graft with the Ozaki AV Neo valve sizer (Ozaki AV neo sizer is always one size larger than the size of the graft). (C) Dacron graft with all three commissures and center of each cusp are marked. Graft is ready with all the markings necessary for suturing the Ozaki valve cusps.
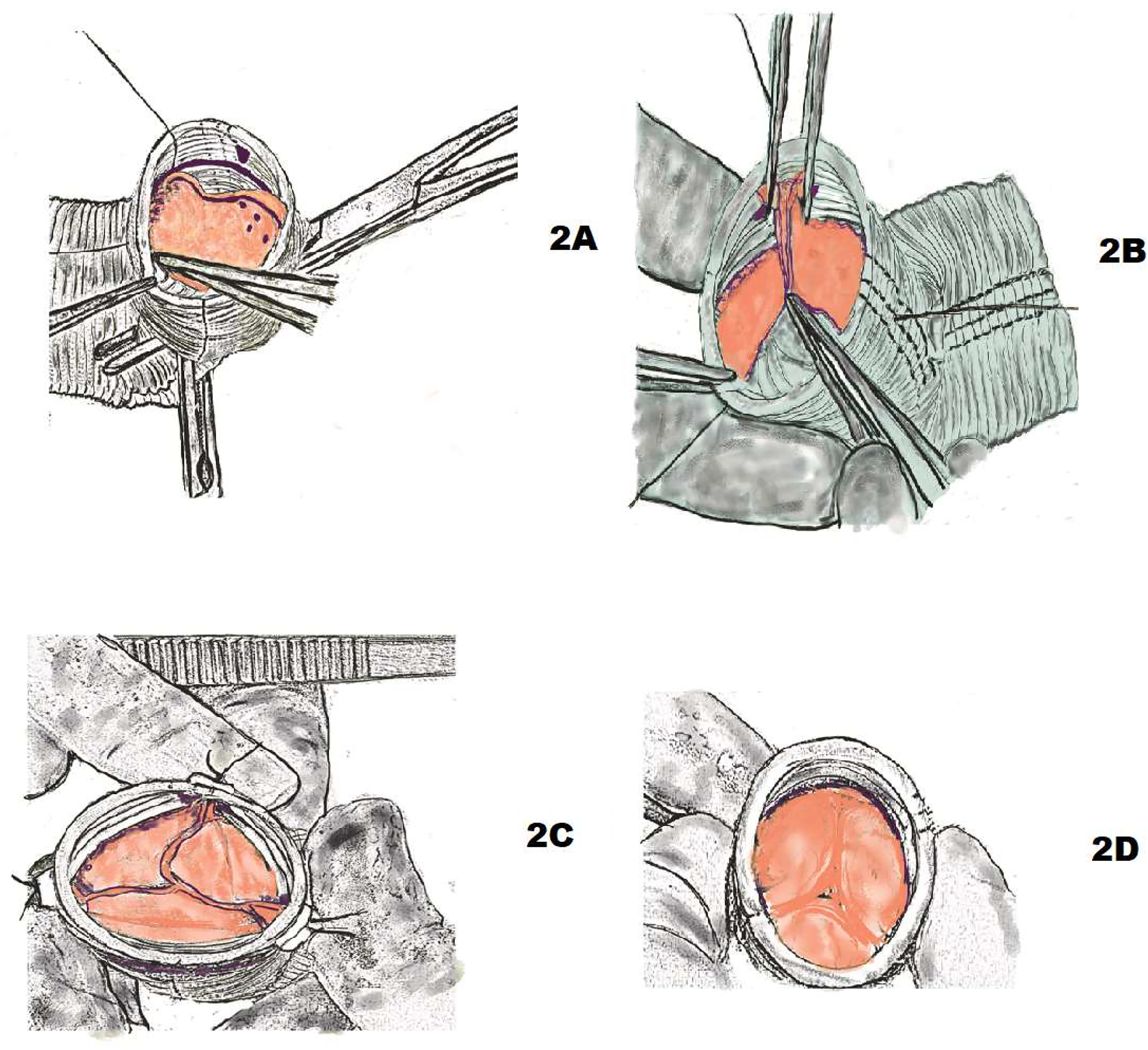
(A) Suturing of first leaflet. Starting from the middle of each cusp, suturing continues until it reaches the commissures on either side. At the middle of each cusp, the distance between the bites in the leaflet and the annulus should be 3:1, and closer to the commissure, 1:1. (B) Completed suturing of two leaflets. Commissural fixation between adjacent leaflets is usually done with additional 4-0 polypropylene suture by taking bites on the wing of leaflets on either side and brought outside through the graft and tied down over the Teflon pledget. (C) The Ozaki valved graft appears after all three leaflets have been sutured. The three leaflet heights and commissural heights should be identical. (D) Internal view of the Ozaki valved conduit with good coaptation of all three leaflets.
As a rule, the leaflet size is one size larger than the graft size. After choosing the graft and leaflet size, three appropriately sized pericardial leaflets were prepared from the treated pericardial patch based on the Ozaki templates. The leaflets were marked as per the templates. Usually, the annulus was marked with a marking pen inside the Dacron graft for about 1 cm from the edge. The annulus is circular and follows one particular ring of the graft. The appropriate Ozaki annulus sizer was taken, and all three commissures and the midpoint of each cusp were marked using the Ozaki sizer. Each pericardial leaflet was sutured to the marked annulus within the graft using 4-0 or 5-0 polypropylene sutures starting at the midpoint of each cusp. The suturing between the neo-cusp and annulus was done similarly to the technique originally described by Ozaki for aortic valve replacement. The only way to obtain a competent valve inside the graft is by strictly following the standardized suturing technique described by Ozaki et al. 7 Suturing begins at the midpoint of each cusp and extends on both sides. Correct bite selection is the most important part of valve competency. Correct bite selection requires a consistent distance in the leaflet as defined by Ozaki et al. When commencing the suture, the distance between the bites in the leaflet and the annulus at the midpoint of each cusp should be 3:1, but as the surgeon gets closer to the commissure, the disparity decreases. The last suture was taken outside of the graft and supported with Teflon pledgets. Particular attention was given to the commissures; all the commissures were suspended to the graft with an additional 4-0 or 5-0 polypropylene suture. These sutures were also brought through the graft and supported with the previously placed Teflon pledget. Next, all three commissures were suspended to the graft by tying these sutures outside the graft over Teflon pledgets. All three commissures were further reinforced with additional fine polypropylene sutures if required. This suturing design increases the cusp's resilience to stress at its middle part and also increases the coaptation along with the free margin of the cusp. The coaptation height in all types of Ozaki neocupidization will be usually about 8 to 10 mm. After commissural fixation, the degree of coaptation can be predicted by visually assessing the heights of all three leaflets and all three commissures. Our goal is to keep all leaflet heights and the commissural heights at the same level. The competency of the valved graft was also assessed by instilling the graft with saline.
The conduit is usually stored inside an empty sterile container. We do not recommend storing the prepared conduit in saline solution to avoid diffuse ooze from the graft after completion of the procedure. The end of the graft-carrying valve was sutured to the pulmonary artery end, and the other end of the graft was sutured to the right ventricular outflow tract (RVOT) either directly or with ringed GORE-TEX graft as a hood to avoid sternal compression. All patients were discharged on aspirin.
Echocardiography
Intraoperative transesophageal echocardiogram (TEE) and direct needle pressure measurements across the conduits were obtained in all patients to assess conduit competency and gradients. Transthoracic 2D-echocardiograms were obtained at discharge, one month, six months, and annually. Conduit regurgitation was graded as none, trivial, mild, moderate, or severe as per the standard echocardiographic criteria. Peak gradients across the conduits were graded as trivial (0-10 mm Hg), mild (11-20 mm Hg), moderate (21-40 mm Hg), or severe (>40 mm Hg).
Statistical Analysis
Statistical analysis was carried out using the Statistical software Jamovi version 2.3.21. Descriptive statistics for continuous variables with normal distribution was represented as mean and standard deviation and those with skewed distribution as median and interquartile range. All categorical variables were represented as frequency and percentage.
Results
Between November 2019 and December 2023, 22 consecutive patients underwent Ozaki RV-PA conduit implants. Among these, 16 patients (72.7%) were between 1 and 18 years, and 6 (27.2%) were older than 18 years of age. The median age was 12 years (interquartile range [IQR] 5.5-21), and the median weight was 35 kg (IQR 15.8-48.5) (Table 1). Indications for RV-PA conduit included: anatomical repair for corrected transposition of the great arteries (TGA), ventricular septal defect/pulmonary stenosis (VSD/PS) (n = 8), replacement conduit (n = 6), pulmonary atresia with associated anomalies (n = 3), pulmonary artery aneurysm with dysplastic pulmonary valve (n = 2), tetralogy of Fallot with coronary crossing RVOT (n = 1), bioprosthetic pulmonary valve regurgitation (n = 1), and as double Ozaki with rheumatic aortic and pulmonary disease (n = 1). Seven patients had prior palliative procedures. Redo sternotomy was required in 14 patients (63.6%). The glutaraldehyde-treated native pericardium was used in 12 patients (55%) and bovine pericardium in 10 patients (45%). Conduit sizes included: 18 mm (n = 1), 20 mm (n = 5), 24 mm (n = 6), 26 mm (n = 1), 28 mm (n = 4), and 30 mm (n = 1) (Tables 1 and 2).
Preoperative Demographic and Intraoperative Details.
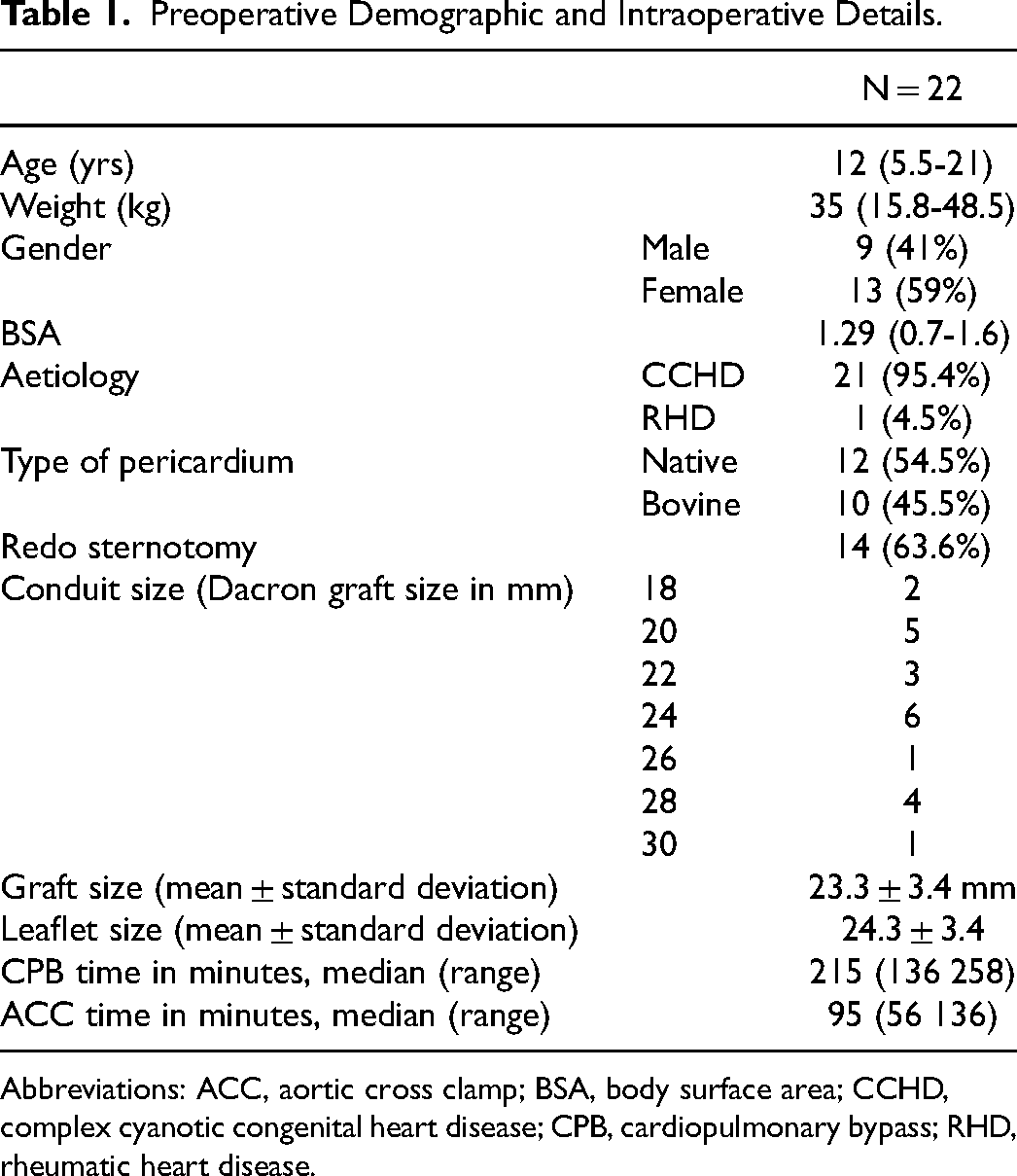
Abbreviations: ACC, aortic cross clamp; BSA, body surface area; CCHD, complex cyanotic congenital heart disease; CPB, cardiopulmonary bypass; RHD, rheumatic heart disease.
Patient Details, Diagnosis, and Size of Ozaki Valved RV-PA Conduits.
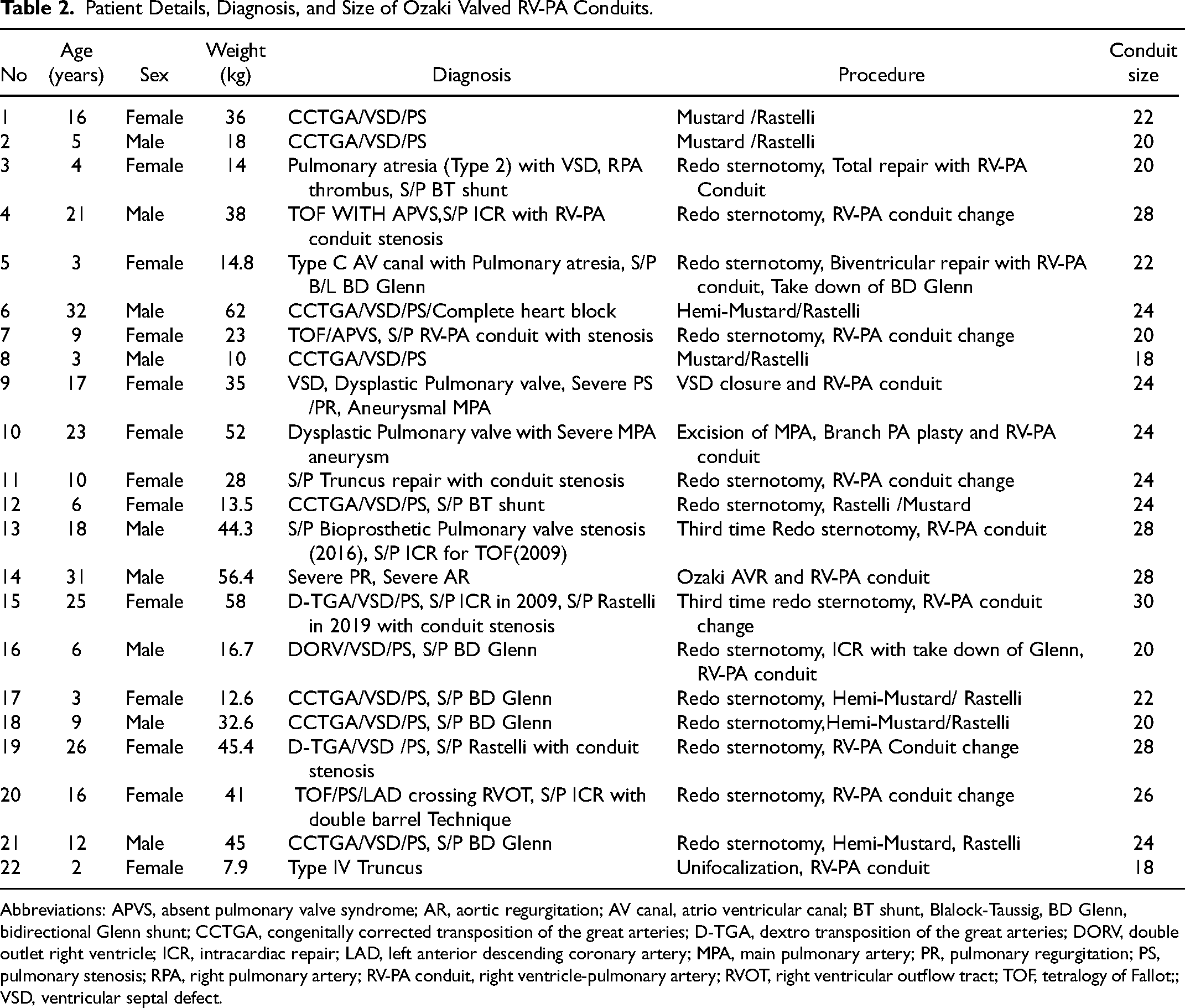
Abbreviations: APVS, absent pulmonary valve syndrome; AR, aortic regurgitation; AV canal, atrio ventricular canal; BT shunt, Blalock-Taussig, BD Glenn, bidirectional Glenn shunt; CCTGA, congenitally corrected transposition of the great arteries; D-TGA, dextro transposition of the great arteries; DORV, double outlet right ventricle; ICR, intracardiac repair; LAD, left anterior descending coronary artery; MPA, main pulmonary artery; PR, pulmonary regurgitation; PS, pulmonary stenosis; RPA, right pulmonary artery; RV-PA conduit, right ventricle-pulmonary artery; RVOT, right ventricular outflow tract; TOF, tetralogy of Fallot;; VSD, ventricular septal defect.
Intraoperative TEE showed moderate conduit regurgitation in two patients but at discharge, both were reduced to mild. One patient had an intraoperative conduit gradient of more than 40 mm Hg, which was early in the experience and likely related to an undersized conduit. The median ICU stay was 4 (IQR 2-6) days, and the median hospital stay was 9 (IQR 5.5-13.5) days. In the immediate postoperative period, surgical reintervention was required in three patients (pleural hematoma evacuation in one, pericardial effusion drainage through a subxiphoid incision in one, and tracheostomy in another). To coil the major aortopulmonary arteries (MAPCAs) one patient required percutaneous intervention. One patient required conservative management for chylothorax. The overall surgical mortality in this group was 9.1%. There were two perioperative mortalities after about a week following surgery but the death was unrelated to the conduit.
The first patient was a six-year-old male child with a case of double outlet right ventricle with remote VSD and pulmonary atresia. He had a BD Glenn operation elsewhere as initial palliation surgery. The child underwent redo sternotomy, take down of the BD Glenn, routing of VSD to the aorta after VSD enlargement and RV-PA Ozaki valved conduit.The child did well initially but in the second week of the postoperative period, developed low cardiac output and very low platelet count. Blood culture was positive for gram-negative bacteria and the child finally succumbed. The other patient was a 12-year-old male child, with a case of congenitally corrected transposition with VSD and severe PS. This child also had a BD Glenn as initial palliation at the age of two elsewhere. Heunderwent redo sternotomy, hemi-Mustard, and Rastelli operation with the Ozaki valved conduit. Postoperatively the child developed acute renal failure and was supported with hemodialysis for up to 14 days. His kidneys did not recover and he finally died of sepsis.
None of the conduits had any evidence of infective endocarditis. Survival at discharge was 90.9%. The median follow-up was 12.3 (IQR, 4.43-21.2) months. There was one sudden death at four months after surgery of unknown cause in a four-year-old who had a Mustard/Rastelli operation for situs inversus, dextrocardia, bilateral superior vena cava, corrected TGA, VSD, and PS. The survival was 86.4% at follow-up. At last follow-up, all valved conduits were competent with trivial regurgitation at 12 months (n = 14) and 24 months (n = 9) (Table 3). No patient had increased gradients from discharge (Table 4). The patient discharged with a peak gradient of more than 40 mm Hg remained asymptomatic with a similar gradient on follow-up. There was no evidence of infective endocarditis of the conduits, and no patient required conduit replacement.
Ozaki Valved Conduit Regurgitation Based on the 2D-Echocardiography.

Ozaki Valved Conduit Gradient Based on the 2D-Echocardiography.

Discussion
Establishing RV-PA continuity is an essential part of anatomical correction in complex congenital heart disease. The first valved aortic homograft was used in the repair of pulmonary atresia by Ross in 1966 8 and popularized by Rastelli 9 in patients with transposition of the great arteries with ventricular septal defect with severe pulmonary stenosis. The use of a homograft in the pulmonary region does not guarantee long-term performance. The homograft in the pulmonary location worked better in Ross procedure patients, with 90% freedom from reintervention at five years. 10 However, homografts function quite poorly in non-Ross surgeries. 11 Homograft shrinking is induced by annulus thickening and fibrosis rather than the patient's somatic growth. Furthermore, when used in young individuals, aortic homografts are prone to rapid fibrocalcification. Blood type incompatibility is one of the most important risk factors for calcification in cryopreserved homografts. 12 Homografts are not readily available in the developing world due to the investment necessary in procurement, preservation, and the cost involved in the maintenance of homograft banks. As a result, very few centers have access to a homograft bank. In addition, despite good infrastructure in some countries such as Japan, certain cultures and people's beliefs have made homograft unavailable.
Xenograft valved synthetic grafts of varying sizes gained popularity in the 1970s.These were expensive and readily available in the developed world. However, studies have shown a very high (approximately 30%) incidence of failure with xenograft valved grafts at six years. 13 Contegra bovine jugular vein conduits have become more popular worldwide in recent years. They are considered to be an alternative to homografts in the pulmonary position in newborns and infants. Sierra et al reported 90% freedom from reintervention at seven years. 14 Contegra, on the other hand, is not widely available in developing nations and is quite expensive. Due to the scarcity of homograft and expensive cost of xenografts, surgeons in developing countries are constantly looking for alternative options for RV-PA conduits. The majority of the centers in the developing world use an indigenous method to make conduits.
Handsewn valved conduits for establishing an RV-PA connection was first introduced by Schlichter et al 1 with autologous pericardium and PTFE conduits. These handsewn valved PTFE grafts worked very well in the native RV-PA position with freedom from reoperation was 100% at one year and two years, 96% at five years, and 80% at ten years. 1 A long-term follow-up study from Japan by Koh et al 2 with handmade trileaflet conduits employing pericardium and 0.1-mm PTFE membrane inside the PTFE graft in the pulmonary position are almost equal to the usage of a pulmonary homograft. This study showed the freedom from reoperation was 84% to 94% at five years, 80% at eight years, and 58% at ten years. Another study from Japan by Ando and Takahashi with handmade trileaflet valved conduits using the 0.1-mm GORE-TEX membrane and Dacron graft showed very good long-term results with freedom from conduit replacement at 97.8% ± 1.6% at three years, 93.5% ± 4.4% at five years, and 88.0% ± 6.8% at ten years. 3 A study from China by Zhang et al compared the handsewn trileflet conduit using 0.1-mm GORE-TEX membrane inside the GORE-TEX graft with bovine jugular vein. The freedom from reoperation at seven years for handmade conduit was 83.6%versus 62.1% for bovine jugular vein. The study concluded that compared with bovine jugular vein grafts, handsewn grafts appear to be associated with a lower incidence of perioperative complications, graft failure, and early-phase mortality. 4 There is currently no single approach that works for all centers to make handmade conduits; instead, each center has its own unique process.
In 2008, Ozaki et al15,16 developed a technique for aortic valve reconstruction using trileaflet neocuspidization with glutaraldehyde-treated autologous pericardium or bovine pericardium showing good mid-term results in the aortic position in adults. The Ozaki technique is better suited for patients in developing countries. The technique avoids the use of expensive commercially available bioprosthetic or mechanical valves and avoids anticoagulation. This operation can be taught in a short period of time due to the high reproducibility and simplicity. Because the original surgical method was highly standardized, this operation can be performed with minimal training. The technique is simple to duplicate with readily available sizers and templates.
In 2019, we began using Ozaki's technique of neocupidization for the aortic valve in children and young adults with congenital and chronic rheumatic aortic valve disease with good early success. So far we have done close to 50 cases of Ozaki aortic neocuspidization including one Ozaki Bentall procedure and five cases of Ozaki neocuspidization in the pulmonary position. Our mid-term results are very satisfactory. Based on this experience, we began to create conduits for both the right and left ventricular outflow tracts using Dacron grafts and glutaraldehyde-treated autologous pericardium. 5 Our preferred leaflet material is native pericardium treated with glutaraldehyde. As a result, even in a redo situation, wealways strive to obtain native pericardium. The native pericardium is very supple and gives good coaptation. It is also freely available. In this study, 55% (12/22) of our patients received native pericardium. If no native pericardium is available, we will use bovine pericardium (10/22, 45%). In the current literature, most of the centers preferred 0.1-mm of ePTFE as a leaflet material in the conduits. The ePTFE membrane is not freely available in developing nations, and they are more expensive than bovine pericardium. We do not have any experience with ePTFE membrane as a leaflet. The bovine pericardium is thicker and less pliable than the native pericardium and ePTFE membrane. None of our patients with bovine pericardial leaflets have required any further surgery yet. However, we are concerned about the premature valve cusp regeneration in bovine pericardial leaflet compared with native pericardium.
Dacron grafts are the least expensive, among all the currently available synthetic grafts. The conduits can be constructed before commencing cardiopulmonary bypass; thus, limiting cardiopulmonary and ischemic times. As long as the conduits are appropriately sized and follow the standardized method of suturing the leaflet to the graft, the Ozaki valved conduit yields excellent hemodynamics with very little regurgitation or gradients across the valve. The valve leaflets are sutured directly to the Dacron graft without a stented frame, allowing them to move freely during systole and providing excellent hemodynamics. During diastole, all three cusps have very large coaptation, which precludes significant regurgitation.
Selecting theappropriately sized Dacron graft is crucial for optimal RV-PA conduit hemodynamics. Z-scores of the pulmonary valve, main and branch pulmonary arteries are used to determine graft size. We aim to increase the graft size from +1 to +3 on the Z score if the main and the branch pulmonary arteries are of normal size. We aim to achieve a graft size up to +3 of Z score for children under five years given high growth potential, +2 for children between 5 and 15 years of age, and +1 for anyone above 15. In cases when the Z-score of the branch pulmonary arteries is less than −2, a smaller size graft will be used. In patients with small-sized branch pulmonary arteries, graft oversize can cause branch pulmonary stenosis, especially at its origin. With the currently available Ozaki sizer, creating the Ozaki valved conduit as small as 12 mm up to the maximum of 34 mm is possible. It is difficult to create a trileaflet valve in a graft size smaller than 16 mm. Thus, one should consider constructing bicuspid valves in graft sizes smaller than 16 mm. Generally, the templated leaflet sizes are one size larger than the selected graft size but can be confirmed using the sizers. Smaller size grafts and the use of bovine pericardium might increase the conduit gradient.
This technique has a few limitations and several significant advantages. Additional operative time is required to construct the valved conduit. Although the conduit is frequently constructed before commencing cardiopulmonary bypass, once on bypass and if the heart is arrested, it might not be feasible to resize and construct another conduit. The tissue matching of the Dacron graft to hypoplastic, thin branch pulmonary arteries is poor, occasionally making the distal suture line less optimal and although we have not seen neo-intimal proliferation occur within the Dacron graft, it has been reported.17,18 If smaller conduits (<16 mm) are used in growing children, conduit replacements will be likely. Advantages include a well-standardized surgical technique, freely available reusable sizer and templates, a well-described suturing method, and minimal training required to reproduce the valved conduit with excellent hemodynamics. This conduit also avoids use of anticoagulation, as all our patients are only on aspirin. And by creating the conduit using native pericardium within a Dacron graft, one can save nearly US $2000 per patient in the developing world. Transthoracic echocardiogram with 3D reconstruction is very helpful in assessing the valve function inside the conduit on follow-up. 19
Limitation
There are three limitations. This is a single-center study, and all surgeries were performed by a single surgeon. Second, it is a descriptive study including a small number of patients with very short follow-up, and finally, there is no comparison group with homograft or bovine jugular conduit.
Conclusion
Creation of an Ozaki valved RV-PA conduit is an attractive option in the developing world due to its affordable cost, reproducible technique, and excellent hemodynamics. Results of the Ozaki valved RV-PA conduit are encouraging on short-term follow-up. This technique provides an extra surgical tool in the surgeon's arsenal for patients requiring an RV-PA conduit irrespective of age. Longer-term studies are needed to confirm the durability of the conduit.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.