
Abstract
Background
There are limited population-based studies on congenital heart disease (CHD) in the pediatric population in Africa. Technological advancements in diagnostic tools have resulted in multiple echocardiographic studies in hospital settings. We aimed to determine the prevalence of CHD in both settings (population-based and hospital based) followed by comparing the two estimates for a difference.
Methods
We systematically searched PubMed, Google Scholar, African Journals Online, and African Index Medicus for eligible studies from 1992 through 2022. We performed a meta-analysis using the random-effects model.
Results
We selected 42 studies; 10 population studies with 1,011,163 participants, and 32 hospital-based studies with 605,268 patients for the analyses. The population and hospital-based prevalence were 5.12 versus 12.63 per 1,000 population of children (P = .007). Ventricular septal defect was the most common type of CHD in both settings (0.61 vs 1.88 per 1,000), followed by atrial septal defect (0.26 vs 0.68 per 1,000). Tetralogy of Fallot was the most common cyanotic heart lesion in both settings (0.08 vs 0.52 per 1,000).
Conclusions
The population-based prevalence of CHD was significantly lower than the hospital-based prevalence (5.12 vs 12.63 per 1,000 population of children). Juxtaposing these two prevalence estimates against each other can be a reasonable alternative to quantifying the contemporary burden of CHD in the pediatric population of Africa. Moving forward, efforts should bolster awareness of CHD in Africa, and further advocacy for children with CHD should be a priority on the continent.
Introduction
Congenital heart disease (CHD) constitutes one-third of all congenital birth defects and is a leading cause of childhood mortality. 1 It is typically defined as a structural abnormality of the heart and/or great vessels present at birth with potential for actual functional significance. 2 The current literature shows that the burden of the disease is on the rise globally.3–5 This could be due predominantly to improved diagnostic imaging coupled with increased survival rather than notable increases in the true incidence of CHD. However, little is known about the burden of CHD in the pediatric population in Africa. In recent times, advances in healthcare technology have improved the accessibility to diagnostic tools such as handheld echocardiograms. 6 This has created research opportunities in regions like Africa. Examining prevalence studies on CHD could lead to a better overview of its burden, with positive implications on policymaking and planning for dedicated care and advocacy on the continent.
Current estimates of CHD in the pediatric population of Africa are 4.35 per 1,000 children. 5 This was computed from nine population-based studies. Population-based studies are the ideal methodology to estimate disease burden; however, in order to undertake these studies they require adequate resources. This can pose a challenge in low-income settings in undertaking many such studies to assess disease. We propose that finding hospital-based prevalence studies, which may include a diagnosis of CHD shortly after birth, are more feasible to conduct, and analyzing them in addition to the population-based studies could be a reasonable alternative to obtaining insight into the burden of CHD in Africa.
Our study seeks to derive updated population-based and hospital-based prevalence estimates in the current era for children under 18 years of age in Africa. Secondly, we intend to juxtapose the two prevalence estimates against each other to obtain a range for our commentary. Lastly, we hypothesize that the hospital-based prevalence estimate will be higher than the population estimate.
Material and Methods
The review was conducted and reported according to the PRISMA 2020 statement. 7 A review protocol was registered on PROSPERO (CRD42023428232). Changes were made to the review protocol after it was published. Thus, the present protocol on PROSPERO is not the current version. These changes included analyzing population-based studies separate from the hospital-based studies, and utilizing R statistical software version 4.4.0 Meta package instead of STATA software version 17 (Stata Corp V.17) due to software convenience.
Search Strategy
We conducted a database search of PubMed, Google Scholar, African Index Medicus, and African Journals Online on May 5, 2023. We used text words and Medical Subject Heading terms. Our key search terms on PubMed were: “congenital heart defects” or “congenital heart disease,” the name of every known anomaly of these abnormalities, and the individual country names for the 54 African countries as additional key search terms. The full search string was adopted from a peer-reviewed published systematic review and meta-analysis protocol on the same topic. The authors published the protocol in 2017. 8 However, after a thorough search, the authors never began the systematic review and meta-analysis. We set the limit for studies from 1992 through 2022. By the early 1990s, studies had correlated echocardiographic findings with morphology. 9 This informed the lower limit for our study period. No language restrictions were applied. We scrutinized references of relevant articles for additional data sources.
Data Review
Three authors independently conducted the review in three stages (titles, abstracts, and full texts). Rayyan online systematic review software was utilized to screen the combination of records from all the databases using their titles to remove irrelevant reports and duplicates. The abstracts were subsequently scrutinized to identify potentially relevant studies. Interrater agreement was not assessed. Discrepancies were resolved by team discussions, similar to previous studies.3–5 All relevant peer-reviewed observational studies conducted in Africa and reporting the prevalence of CHD in children from birth to 18 years, or at least providing the data to compute the prevalence, were included. Articles reporting the prevalence of acquired heart disease with coincidental and isolated findings on CHD were considered. Also, studies with data on patients up to 18 years of age distinct from the rest of the study population were considered. The hospital-based studies we included had their base population from overall general admissions. After exclusion based on the title and abstract, full-text articles were subjected to the inclusion/exclusion criteria. Studies lacking information on a total number of CHD cases, and studies with diagnoses not confirmed by echocardiography and/or autopsy were excluded. Hospital-based studies derived from only cardiology clinic attendance were excluded. Relevant articles retrieved after citation search of selected papers were also cross-checked with the same inclusion/exclusion criteria. All authors agreed on the final studies eligible for inclusion.
Data Extraction and Quality Assessment
Data from the selected papers were recorded independently on a Microsoft Excel spreadsheet. Discrepancies were resolved by team discussions. The following study characteristics were considered: the author, year of publication, country where the study was conducted, the study design, period of investigation, age range, number of CHD cases, total population size, and the various types of CHDs when available. The investigation period was taken as the time frame in which the study was conducted. We separated purely population-based studies from hospital-based studies. Two authors independently assessed the quality of the included studies using the Joanna Briggs Institute (JBI) quality appraisal checklist for prevalence studies. 10 The checklist comprised nine items; marks were awarded as yes (1), no (0), or excluded from the overall appraisal if it did not apply to the study. The final score was computed as a percentage of the proportion of the number of items judged “Yes” over the total number of applicable assessments. A JBI score higher than 70% was classified as high quality, between 50% and 70% as medium quality, and less than 50% as low quality. 11
Data Analysis
Data were analyzed using R statistical software version 4.4.0 Meta package. A random-effects meta-analysis model was used to obtain an overall summary estimate of the population and hospital-based prevalence, as we expected a highly heterogeneous dataset. The pooled estimates were represented with 95% confidence intervals. We used a P-value of .05 as the cutoff for a statistically significant difference. Studies were grouped into six groups of 5-year periods based on the year of publication from 1992 to demonstrate the changes in CHD population-based prevalence over time. The six groups were: 1992 to 1996, 1997 to 2001, 2002 to 2006, 2007 to 2011, 2012 to 2016, and 2017 to 2021. There were three additional hospital-based studies published after 2021.12–14 Forest plots were used to display the estimated sizes obtained from the meta-analyses, and a line graph for the time trend analyses. The “2002-2006”-year period was omitted from the line graph for population-based studies because no studies were recorded in that period. We performed leave-one-out for sensitivity analyses. Funnel plots analysis and Egger's test were performed to detect publication bias.
Results
Our systematic database search yielded 2,553 records. Two additional studies were obtained from other sources; one from the included studies of Liu et al 5 and the other from a Ghanaian pediatrician with a particular interest in cardiology. 14 After the removal of 100 duplicate records, two additional records were excluded based on numerical assumptions in the total number of CHD cases, 15 and similarity between a record 16 and another potentially relevant study. 17 Overall, 42 studies were selected for the meta-analysis (Figure 1); 10 population-based studies comprising 1,011,163 participants, and 32 hospital-based studies comprising 605,268 patients. Their ages ranged from birth to 18 years of age in both settings. The population-based studies originated from Kenya, 18 Egypt, 19 Mozambique, 20 Uganda, 21 Tunisia, 22 Senegal, 23 and Nigeria.17,24,25 One of the population-based studies originated from the small island state of Réunion. 26 The island's territory is not depicted in Figure 2A because it is located further east (680 km [420 miles]) from Madagascar. One of the hospital-based studies was a thesis for obtaining a medical doctorate in Morocco. 27 Figure 3 shows the number of studies recorded for the various publication year periods. After critical appraisal, the studies were judged to be of medium to high quality, ranging from 62.5% to 100% on the JBI score. Only two studies were of medium quality, with the lowest scoring of 62.5% for both.28,29 Echocardiography was the diagnostic tool used in all the studies, except one study from Nigeria, where CHD was ascertained during autopsy 28
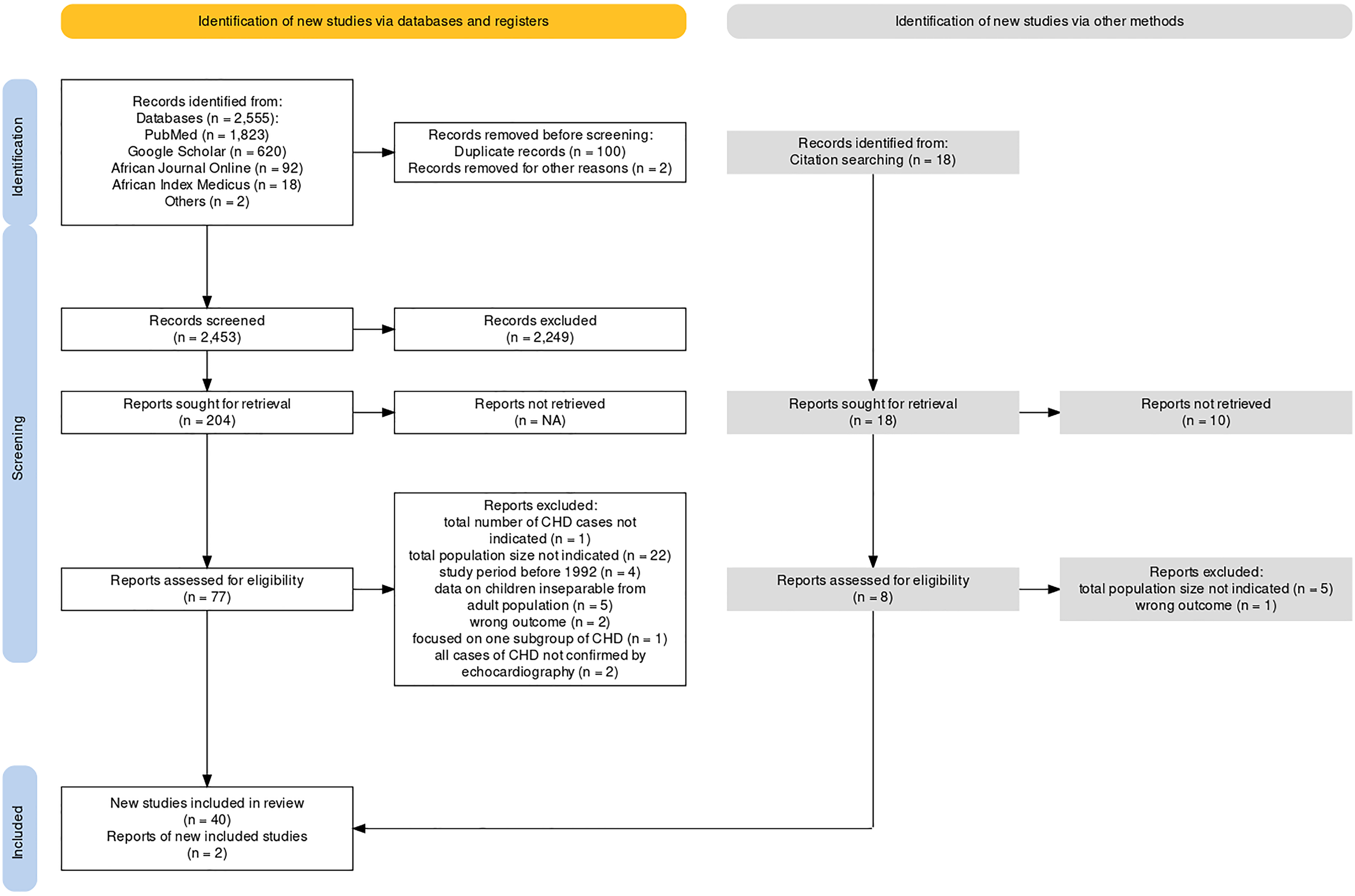
PRISMA flowchart showing the selection of studies for meta-analysis.
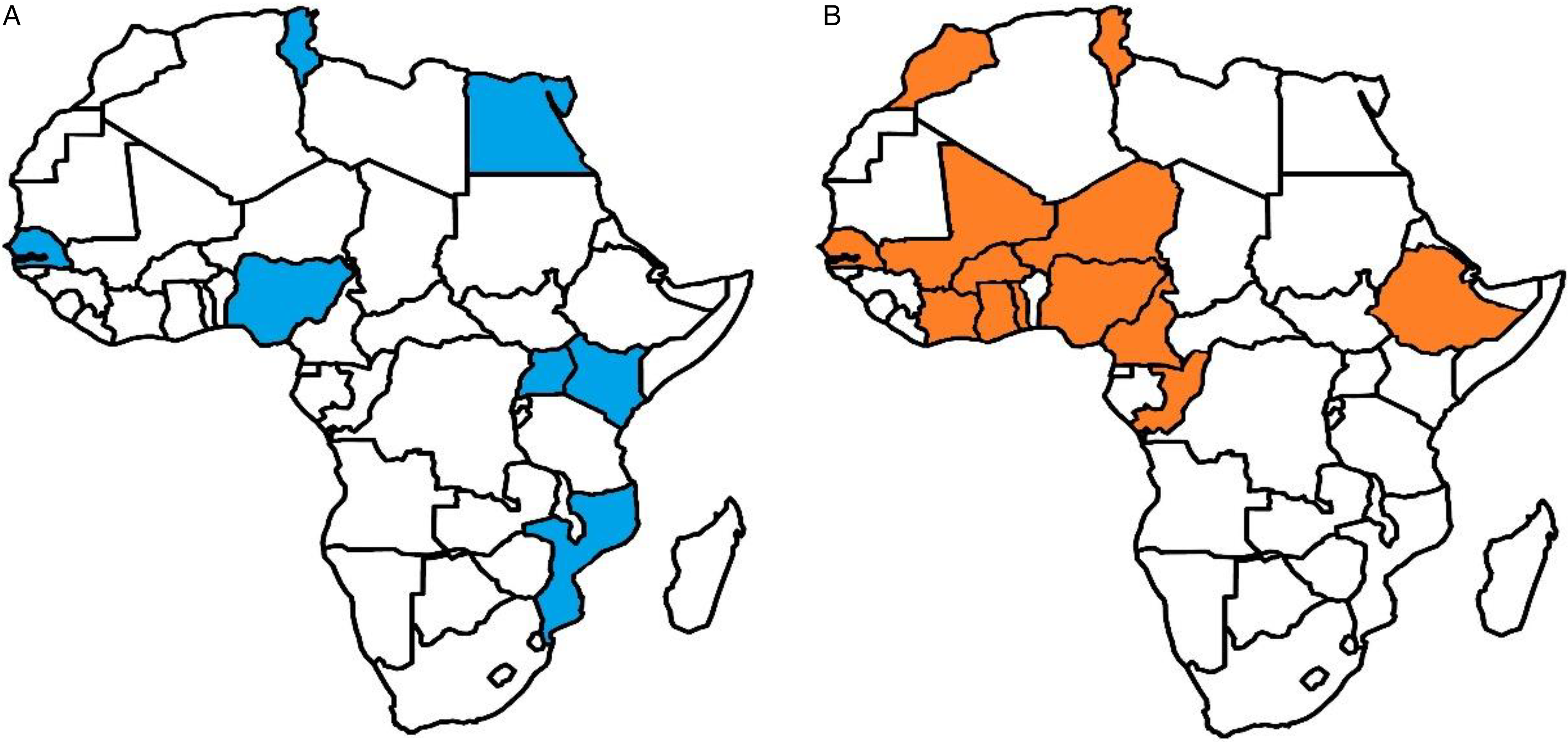
(A) African map showing the countries of origin of population-based studies. (B) African map showing the countries of origin of hospital-based studies.
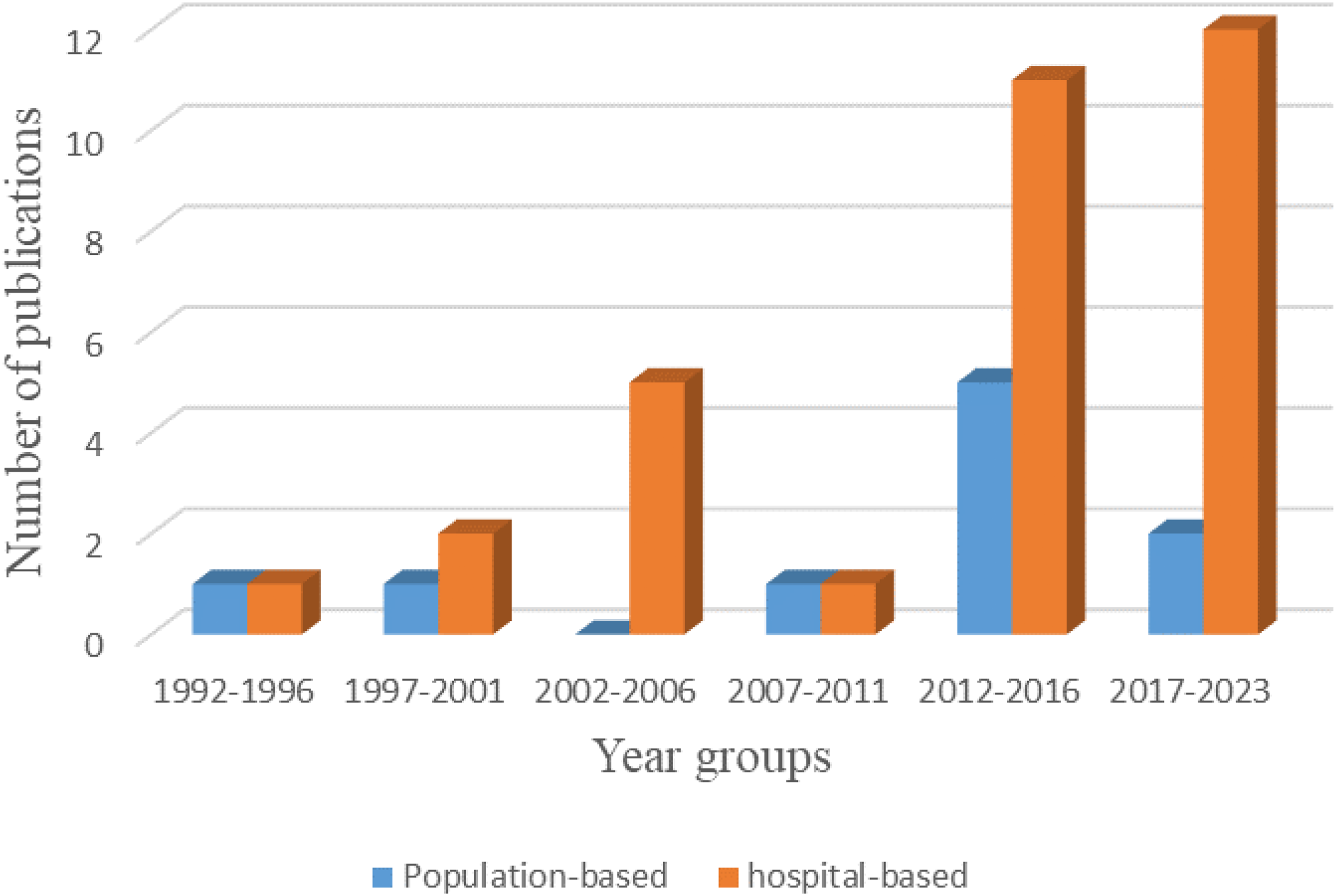
The number of included studies according to the publication year groups.
Population and Hospital-Based Prevalence of Congenital Heart Disease
The pooled population and hospital-based prevalence of CHD were 5.12 [2.77; 8.14], and 12.63 [8.02; 18.25] per 1,000 population of children, respectively (Figures 4 and 5)12–14,16,18–54 The statistical test for the difference between the two prevalence estimates was significant (P = .007). Over time, the population-based prevalence increased by 80%, from 1.79 to 9.97 per 1,000 population of children (Figure 6). Again, the “2002-2006”-year period was omitted from the time series for population-based studies because no studies were recorded in that period.
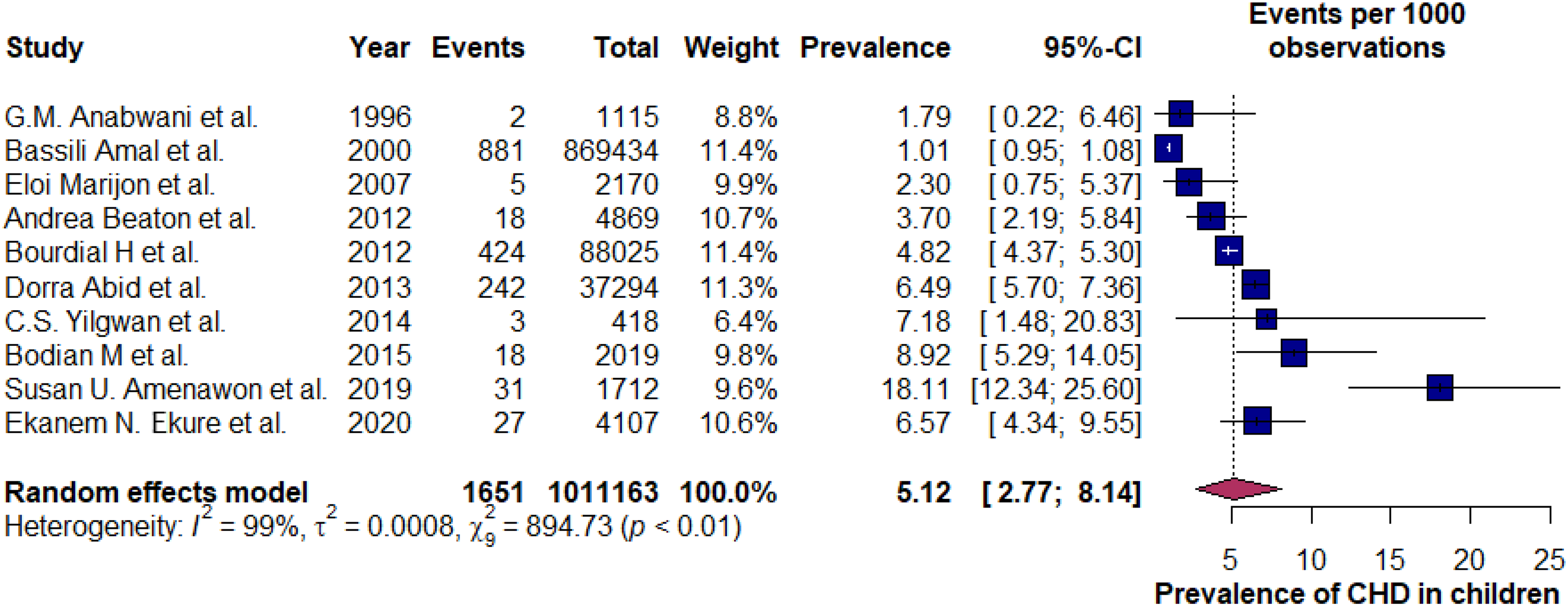
Forest plot showing the pooled population-based prevalence of CHD in children below 18 years of age in Africa. CHD, congenital heart diseases; CI, confidence interval.
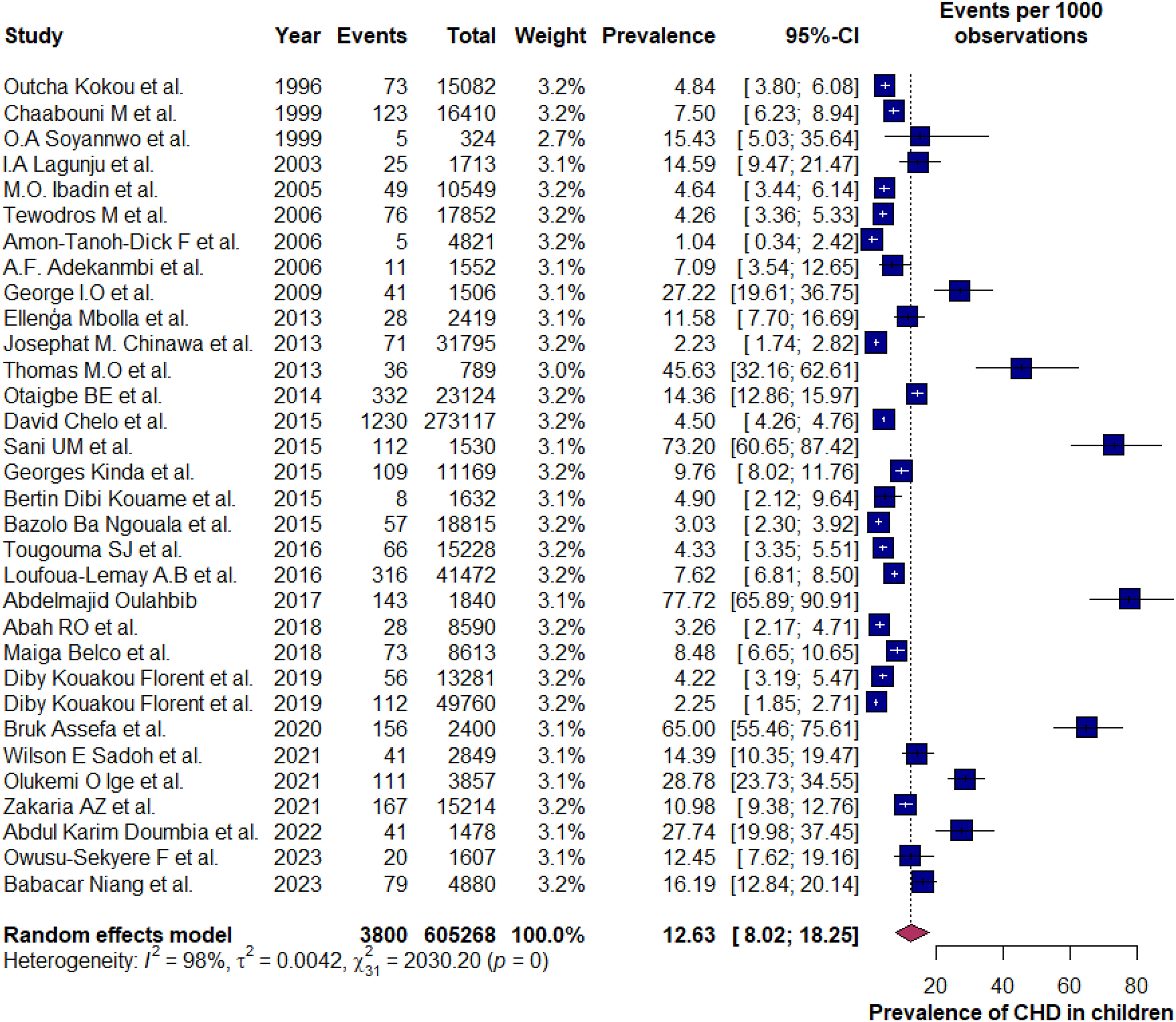
Forest plot showing the pooled hospital-based prevalence of CHD in children below 18 years of age in Africa. CHD, congenital heart disease; CI, confidence interval.
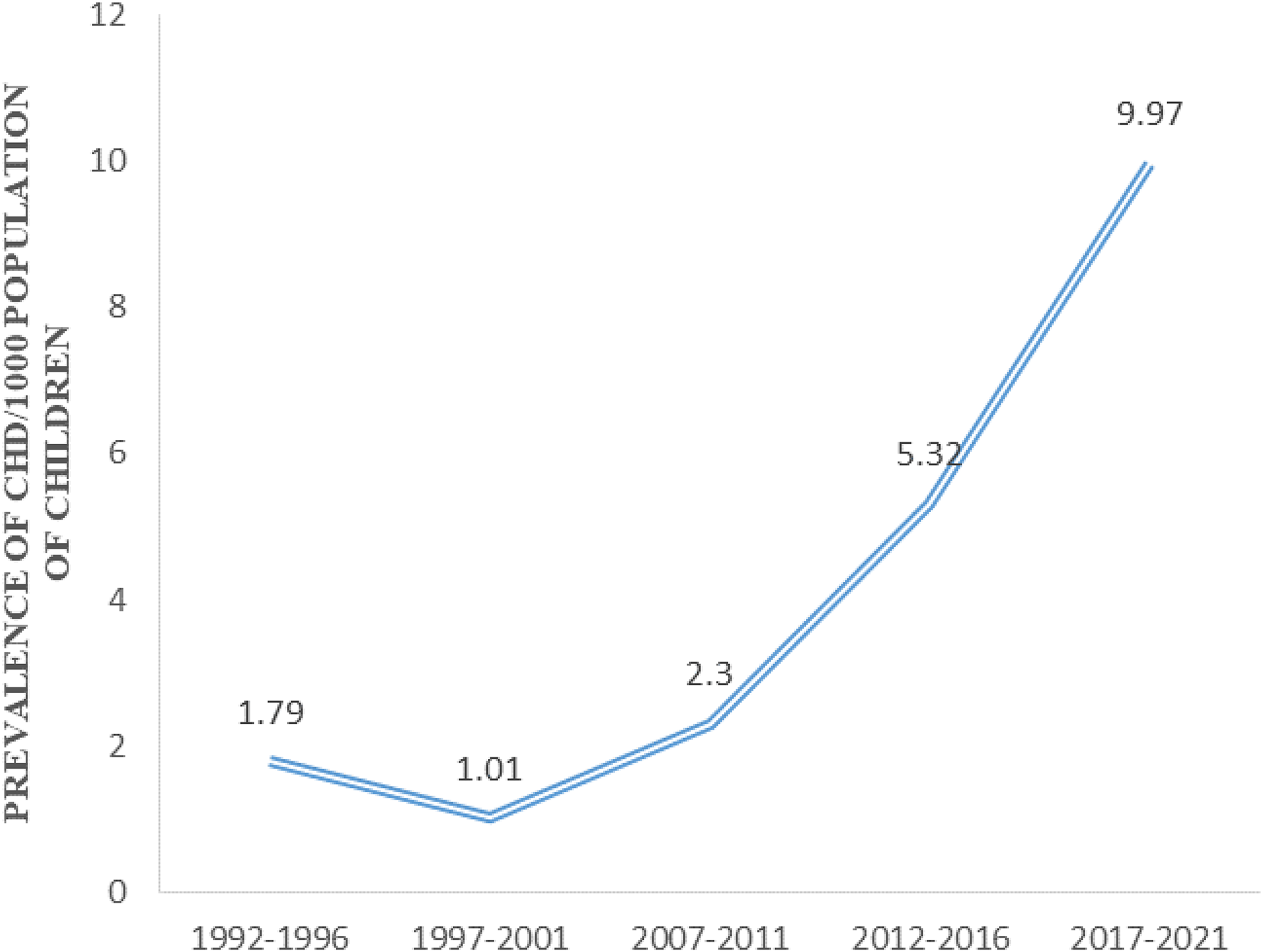
Time course of population-based CHD prevalence from 1992 through 2022. CHD, congenital heart disease.
Prevalence of the Top Five Types of Congenital Heart Disease
The reported prevalence of the most common types of CHD are shown in Table 1. Ventricular septal defect (VSD) and atrial septal defect (ASD) were the top two types of CHD in both study groups. Although the same entities, the order of the remaining three types differed in each group.
Prevalence of the Top Types of CHD Recorded From the Two Study Groups.
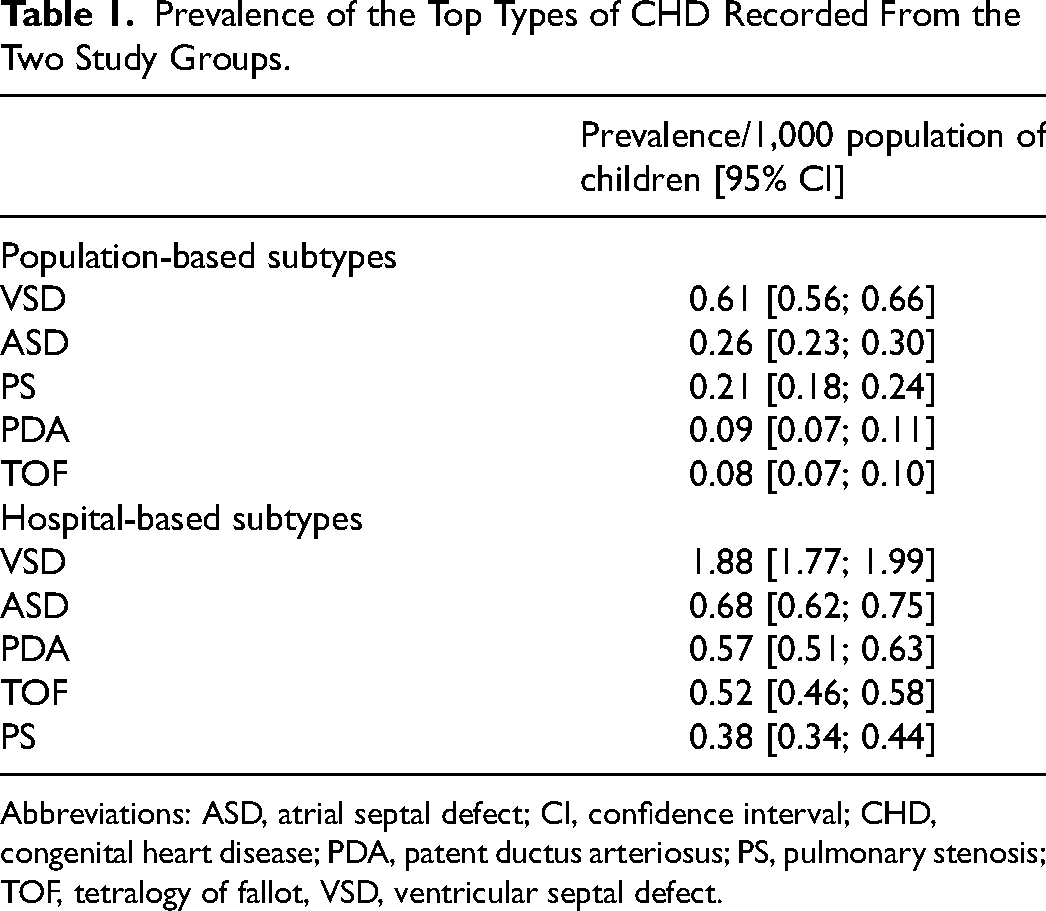
Abbreviations: ASD, atrial septal defect; CI, confidence interval; CHD, congenital heart disease; PDA, patent ductus arteriosus; PS, pulmonary stenosis; TOF, tetralogy of fallot, VSD, ventricular septal defect.
Subgroup Analysis, Heterogeneity, Sensitivity Analysis, and Publication Bias
We aimed to conduct subgroup analyses for the five subregions of the continent. However, not all the subregions were represented, especially in population-based studies. Hence, we changed our methodology. Significant heterogeneity (I2 > 98%) was observed among the two study groups. This could be due to the differences in the observational study methodologies. In the sensitivity analyses, the pooled prevalence for population-based studies remained uniform (Figure 7). The hospital-based prevalence was uniform except for these two studies27,30 (Figure 8). Omitting those studies, the updated hospital-based prevalence was 10.2 [6.9; 14.3] per 1,000 population of children. Funnel plots and Egger's test in both scenarios were asymmetrical with P-value below .10, indicating the presence of publication bias.
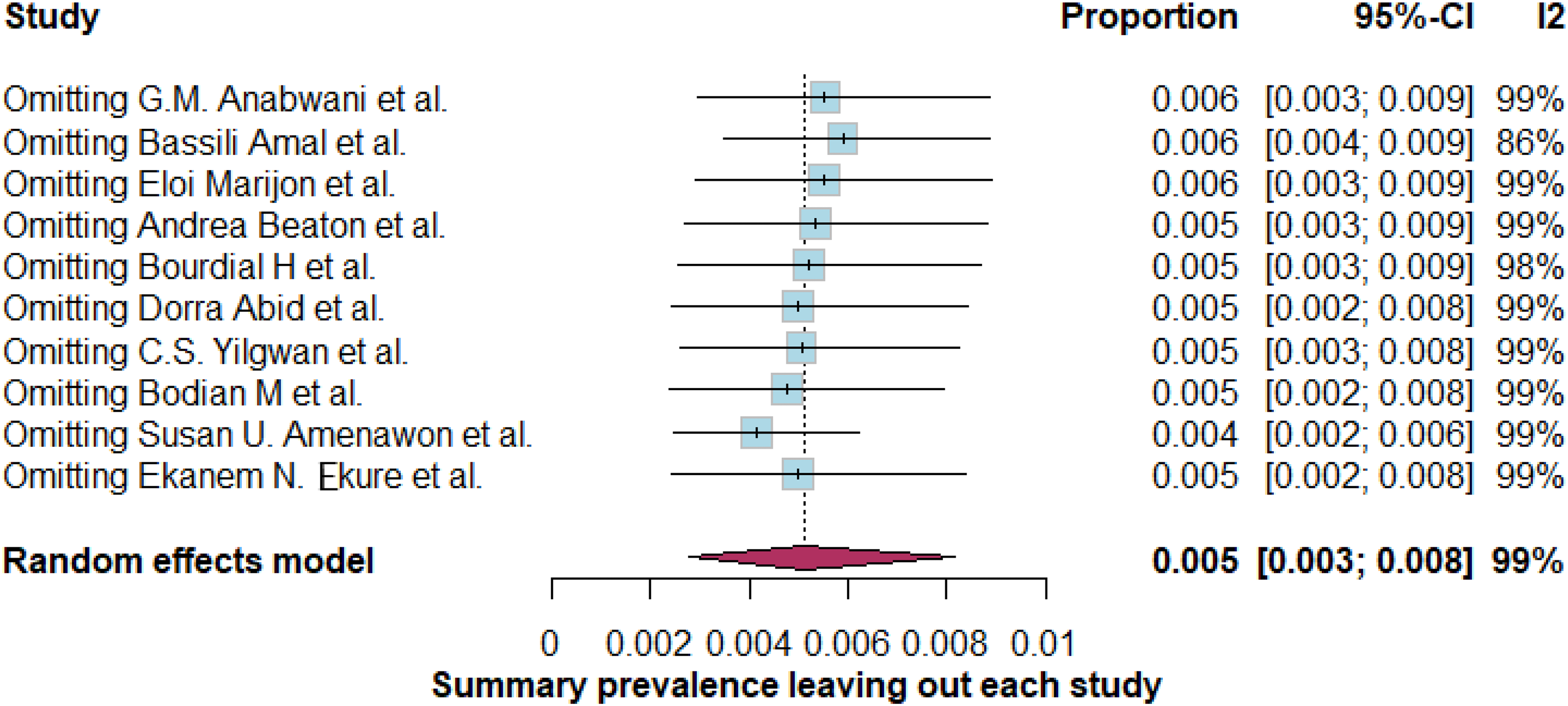
Leave-one-out test analysis for population-based studies. CI, confidence interval; I2, heterogeneity.
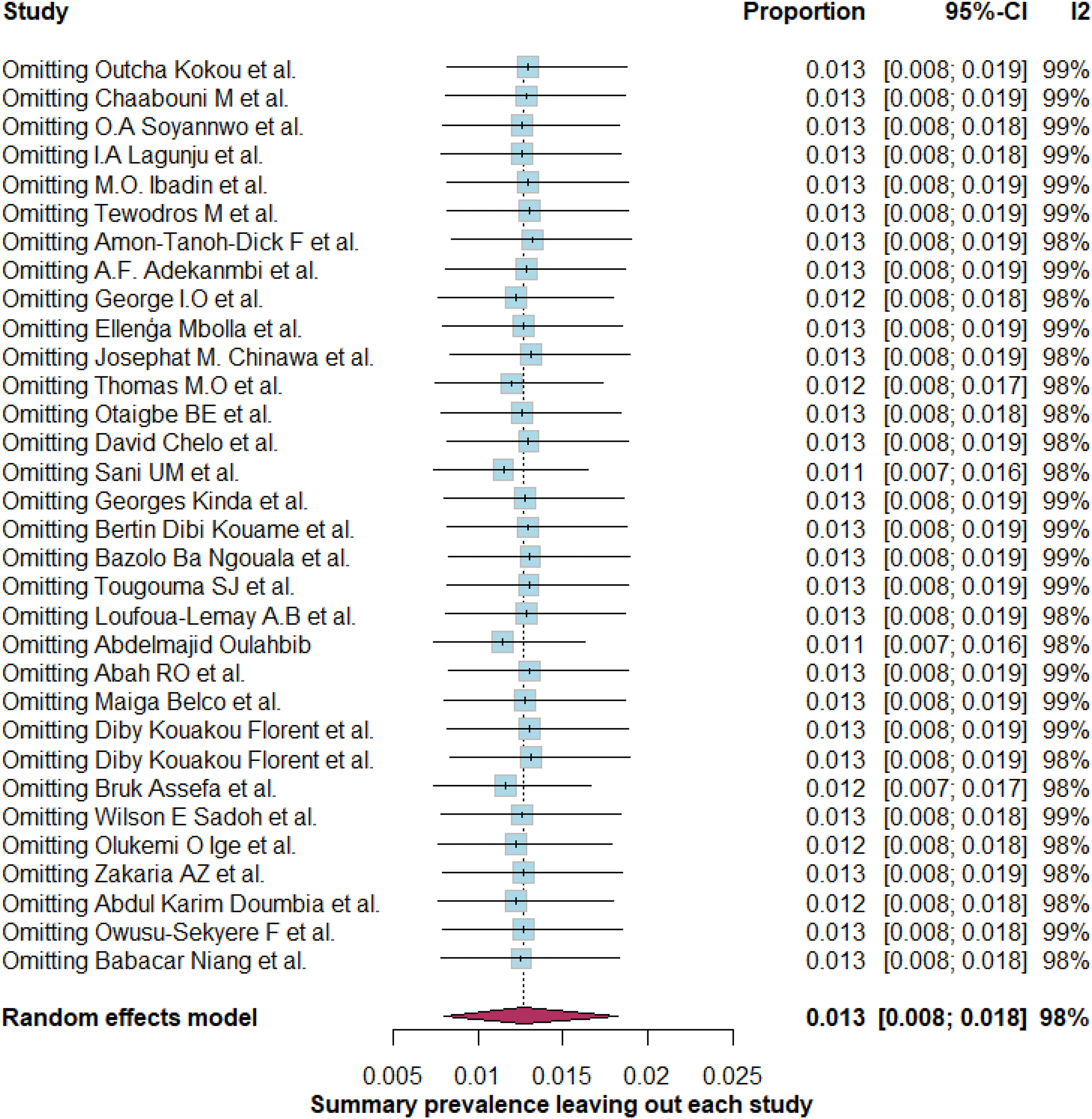
Leave-one-out test analysis for hospital-based studies. CI, confidence interval; I2, heterogeneity.
Comment
We have summarized contemporary data from 10 population-based and 32 hospital-based studies to derive separately, the population and hospital-based prevalence of CHDs in the pediatric population in Africa. The population-based prevalence of CHD was significantly lower than the hospital-based prevalence (5.12 vs 12.63 per 1,000 population of children; P = .007). From the leave-one-out sensitivity analysis, we can infer that the hospital-based prevalence ranged from 10.2 to 12.6 per 1,000 population of children. Juxtaposing the two major prevalence estimates against each other, a reasonable range of 5.12 to 12.63 per 1,000 population of children is a step toward improving the clarity of the conversations in policymaking to address the disease burden.
An upward trend in the population-based prevalence of CHD was discernible. We agree with Liu et al 4 that the low detection rate in Africa could be due to inadequate diagnostic tools and poor access to healthcare services. This was based on the significantly lower prevalence of CHD in Africa compared with other regions of the world in their studies. The increased use of echocardiography globally and improved echocardiographic techniques 9 have contributed to bridging this gap. Collaborative efforts between institutions from developed and developing countries20,21 can also be viewed as an additional contributor to addressing this gap. The upward rise in our study occurring after 2001 is similar to the reported global trend observed after 1995.3–5 The six-year lag could signify the buildup of accessible echocardiography services across Africa, resulting in increased research activities. This could more likely explain the upward trend we observed in the population-based prevalence over the study period, rather than representing a true prevalence increase. In spite of the challenges associated with conducting population-based screening due to limited resources, it can be perceived that the capacity buildup resulted in more hospital-based echocardiography studies, enabling us to identify 32 eligible hospital studies from the continent. The upward trend of such studies can also be appreciated in Figure 3. The difference between our population estimate of 5.12 per 1,000 and current data of 4.35 per 1,000 population of children 5 was minimal. We are optimistic that with more collaborative efforts between institutions in developed countries, passionate about global cardiovascular health, and African health institutions, as well as economic growth on the continent, more population-based studies would occur in the near future. Until then, an alternative to gaining insight into the current burden of CHD could be derived by viewing data from hospital-based assessments as complementary to the limited population studies.
To put this into context, the total population of children under 18 in Africa stands at 676,567,243; the sum of the population quotations displayed per country by the 2023 UNICEF data 55 Relating our population-based CHD prevalence of 5.12 [2.77; 8.14] per 1,000 population to the childhood population of Africa to estimate the burden of CHD, a hitherto unknown figure, corresponded to 3,464,000 (1,874,000-5,507,000) children. The computations for these figures are available in the research data file. A 2010 study estimated that 1 million children were living with CHD (operated and unoperated) in the United States 56 . The studies from which our meta-analyses were computed were reports of unoperated CHD. Thus, our study shows a clear need to bolster awareness of CHD in Africa, and further advocacy for children with CHD should be a priority.
Just as we found VSD and ASD to be the top two types of CHD in both study settings, this was consistent with previous findings.3–5 These lesions, when they exist in isolation, are typically of low to medium complexity, and compatible with survival into late childhood and adolescence without intervention. Regarding cyanotic CHD, tetralogy of Fallot (TOF) was the most prevalent type in both study settings. There were 84 and 312 population and hospital-based cases out of approximately 1 million and 605,000 participants, respectively. Transposition of the great arteries (TGA) was second to TOF with 46 population and 50 hospital-based cases, respectively, although it did not make it on our list of the top five types of CHD (Table 1). Future benefits, such as early diagnosis with positive repercussions on morbidity and mortality, could be achieved when advocacy efforts for public health initiatives, such as newborn screening using pulse oximetry, 57 are implemented and strengthened on the continent.
There are policy implications for the findings of our study. This includes—comprehensive newborn evaluation and pulse oximetry screening for critical CHDs to facilitate early diagnosis, as well as childhood screening in countries with large child populations; investment in diagnostic and treatment services/surgical interventions; and the need to build registries of children living with CHD. This would also help identify the age ranges at diagnosis. To meet the SDG 3.2 goal of reducing child mortalities, the prioritization of reducing premature deaths from heart disease in children under 5 years of age becomes essential. Health policymakers will need to develop specific measurable metrics that focus on barriers and improve access to care and treatment. Particularly important would be childhood screening, especially among preschool children, and mechanisms for pooled financing to replace out-of-pocket health expenditure for CHD care. In terms of human resources, as the specialist workforce is being built up, innovation and ingenuity will be needed to fill in the gaps. Task shifting is one of the viable means. 58 With handheld ultrasound devices allowing fundamental assessment of cardiac morphology,59,60 more community health workers and nurses should be trained in the use of these devices. As a political commitment to improving healthcare systems, private enterprises whose aim is to provide affordable access to quality healthcare should be encouraged. 58
Limitations
Hospital-based studies have their inherent limitations in providing population-based estimates—they can potentially underestimate or overestimate disease burden due to low coverage. Secondly, we excluded data on coexisting heart defects, such as VSD plus ASD, to avoid ambiguity. Nonetheless, such data were relatively small and the potential impact on the study findings is ostensibly marginal. Lastly, it is not unusual to find significant heterogeneity in meta-analyses of prevalence studies.2,3,5 However, we acknowledge the significant heterogeneity (I2 > 98%) in our study. A likely explanation in our meta-analysis could be the different age ranges of the individual study cohort. Nonetheless, the overall study population was under-18 years of age.
Conclusions
The population-based prevalence of CHD was significantly lower than the hospital-based prevalence (5.12 vs 12.63 per 1,000 population of children). Juxtaposing these two prevalence estimates against each other can be a reasonable alternative to quantifying the burden of CHD in the current era. Moving forward, efforts should bolster awareness of CHD in Africa, and further advocacy for children with CHD should be a priority on the continent.
Supplemental Material
sj-xlsx-1-pch-10.1177_21501351241299405 - Supplemental material for Prevalence of Congenital Heart Disease in Children and Adolescents Under 18 in Africa: A Systematic Review and Meta-Analysis
Supplemental material, sj-xlsx-1-pch-10.1177_21501351241299405 for Prevalence of Congenital Heart Disease in Children and Adolescents Under 18 in Africa: A Systematic Review and Meta-Analysis by Kwadwo A. Danso, Grace Appah, Rosemary S. Akuaku, Yaa S. Karikari, Annette K. Ansong, Frank Edwin and Nana-Akyaa Yao in World Journal for Pediatric and Congenital Heart Surgery
Supplemental Material
sj-docx-2-pch-10.1177_21501351241299405 - Supplemental material for Prevalence of Congenital Heart Disease in Children and Adolescents Under 18 in Africa: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-pch-10.1177_21501351241299405 for Prevalence of Congenital Heart Disease in Children and Adolescents Under 18 in Africa: A Systematic Review and Meta-Analysis by Kwadwo A. Danso, Grace Appah, Rosemary S. Akuaku, Yaa S. Karikari, Annette K. Ansong, Frank Edwin and Nana-Akyaa Yao in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Acknowledgments
The authors acknowledge Jeffery Osei, MBChB, MPH (Emory University Rollins School of Public Health, Atlanta, Georgia, USA) and Paa Kobina Forson, MBChB (Komfo Anokye Teaching Hospital, Department of Emergency Medicine, Kumasi, Ashanti Region, Ghana) for reviewing and revising the manuscript.
Data Accessibility Statement
All data available in research data file.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.