
Abstract
We describe a simple and reproducible technique for neonatal peritoneal dialysis catheter insertion following cardiac surgery which prevents the catheter from becoming blocked by the omentum.
Introduction
Peritoneal dialysis (PD) is an established component in postoperative care of critically ill infants after cardiopulmonary bypass (CPB) for congenital heart disease and aids in the management of postoperative kidney injury, fluid balance and electrolyte disturbance. 1 A recent article by Namachivayam and colleagues 2 has shown that early commencement of PD irrespective of kidney function or volume status is associated with reduced incidence of adverse events such as death, cardiac arrest, emergent chest opening, or requirement for extracorporeal membrane oxygenation. This is postulated to be due to the modulation of post-CBP inflammatory response and its negative consequences by PD.
Peritoneal dialysis requires a functional PD catheter, which is usually inserted in neonates and infants at the conclusion of CPB if hemodynamic or renal compromise is anticipated postoperatively. Numerous techniques have been described to achieve this. 3 A significant limitation of these techniques is the potential for obstruction of the PD catheter by the omentum, limiting its utility. We describe a technique for placement of the catheter on the right side of the falciform ligament, which helps to prevent this problem.
Technique
At the conclusion of the procedure on CBP via median sternotomy, the patient is weaned from bypass, and modified ultrafiltration is commenced. Electrocautery is used to expose the peritoneum below the diaphragmatic attachments to the xiphisternum. A transverse incision is made in the peritoneum and a right angle clamp is used to facilitate a midline incision in the skin above the umbilicus, anterior to the omentum. A 14F silastic catheter is trimmed and brought through this incision (Figure 1A).
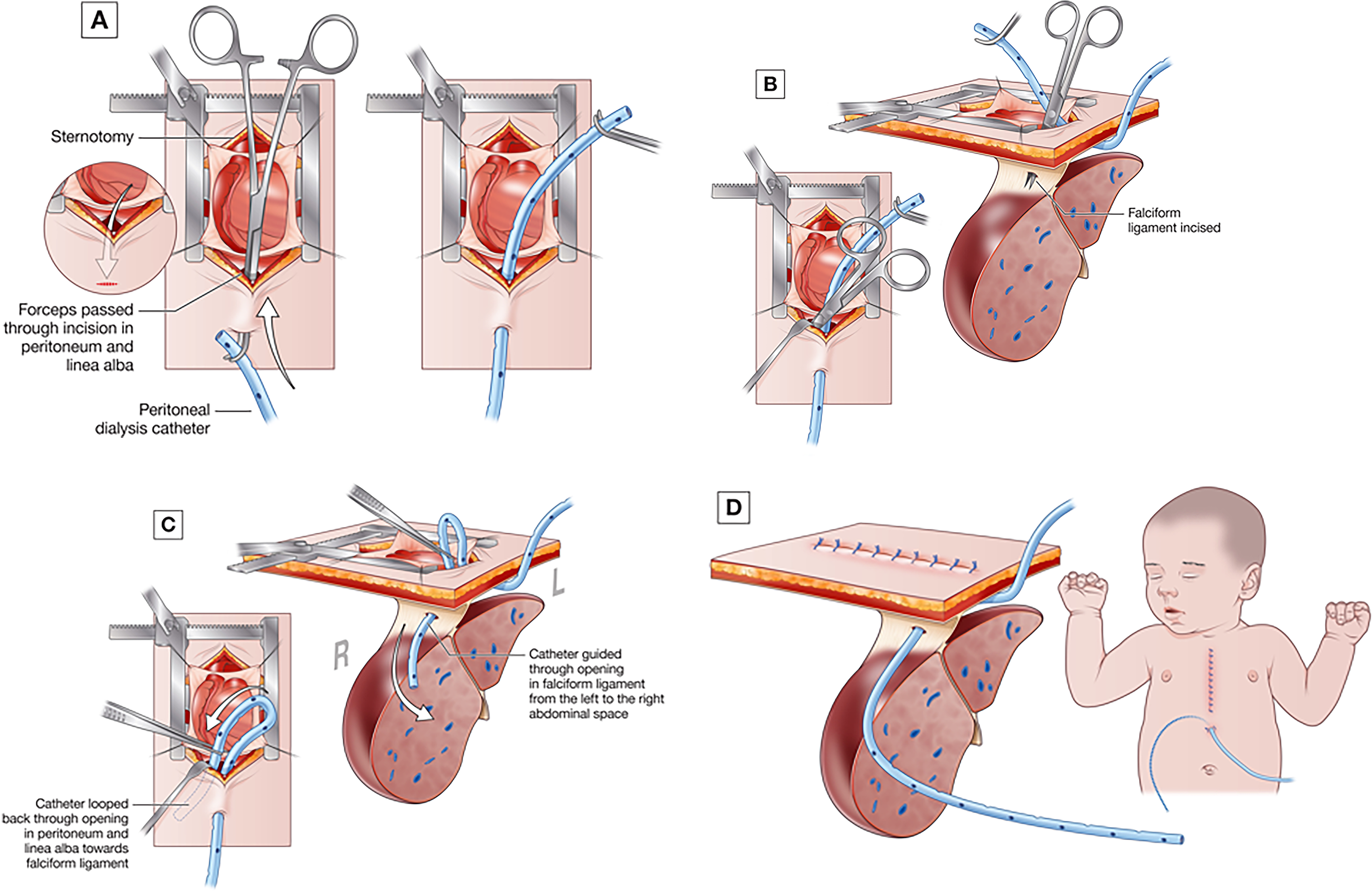
Technique of peritoneal dialysis catheter insertion on the right side of the falciform ligament. (A) The catheter is tunneled via a midline incision, (B) an incision is made in the falciform ligament, (C) the catheter tip is guided through the incision, (D) the incision in the peritoneum is closed and the sternum closed in the standard fashion.
Via the incision in the peritoneum, the falciform ligament is grasped with a forcep, and electrocautery or blunt dissection is used to create a small incision in the ligament (Figure 1B). The catheter is passed through this incision and over the right lobe of the liver (Figure 1C) where it is allowed to rest immediately below the diaphragm (Figure 1D). The incision in the peritoneum is closed with a double layer of continuous 6/0 polypropylene suture, taking careful bites to avoid tension or tearing, and the catheter is secured to the skin using a 4/0 silk suture.
Outcome and Discussion
We routinely place PD catheters in all neonates and small infants at risk of renal failure such as children under 5 kg undergoing ventricular septal defect closure or tetralogy of Fallot repair unless there is a contraindication (previous abdominal surgery, necrotizing entercolitis). Patients coming back from the operating room will have the PD catheter left on free drainage in the initial postoperative period with the catheter being removed 24 to 48 h after its last use. In patients for whom there is a large volume of drainage from the catheter and who do not require dialysis, the PD catheter is capped for 24 h and then removed if no abdominal distention occurs. Indications for PD in our practice include anuria persisting >2 h, hyperkalemia, metabolic acidosis, and accumulating positive fluid balance. Peritoneal dialysis is performed using 10 mL/kg of 1.5% dialysate with hourly cycles, letting the dialysate dwell in the peritoneal space for 45 to 50 min and then allowing it to drain freely from the catheter.
Multiple techniques have been described for insertion of PD catheters after cardiac surgery, 3 but omental obstruction often necessitates the use of an additional catheter for cross flow. Our technique places the catheter in a peritoneal compartment away from the omentum, thereby reducing the chance of obstruction (Figure 2). Occasionally, there will be communication between the peritoneum and the pericardial and/or pleural space resulting in drainage from the chest drains, however, both of these issues are rare. In a review of a series of 618 PD catheter placements using this technique at the Royal Children's Hospital, Melbourne, we found an incidence of malfunction requiring catheter replacement of 0.6% (Table 1). Within this series, 70% of the patients undergoing the arterial switch operation required PD, with a median duration of use of 14 (24-35) hours and the longest use of the PD catheter being 13 days.
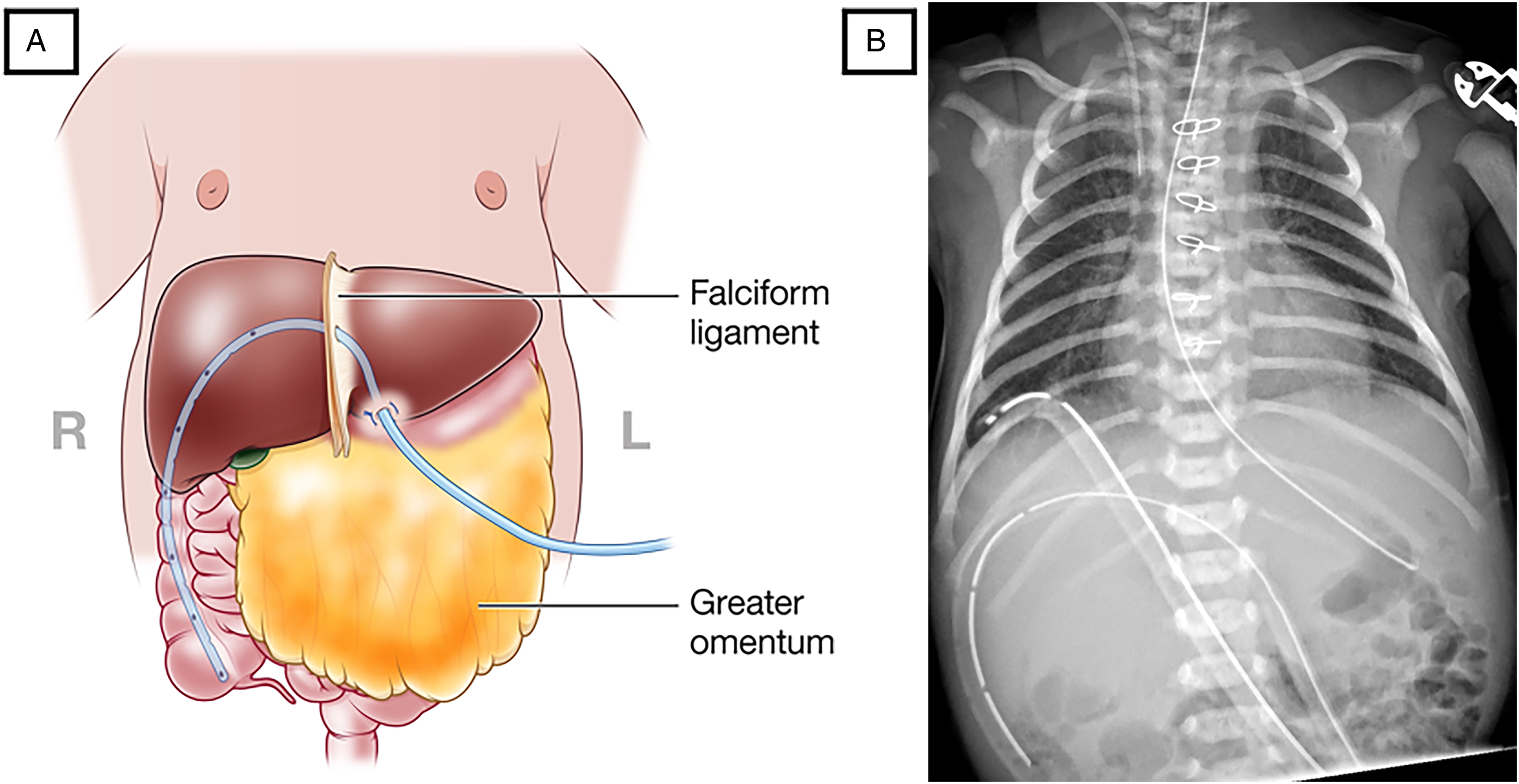
Peritoneal dialysis catheter in the peritoneal cavity away from the omentum (A) schematic (B) postoperative chest X-ray.
Peritoneal Dialysis Catheter Complications.
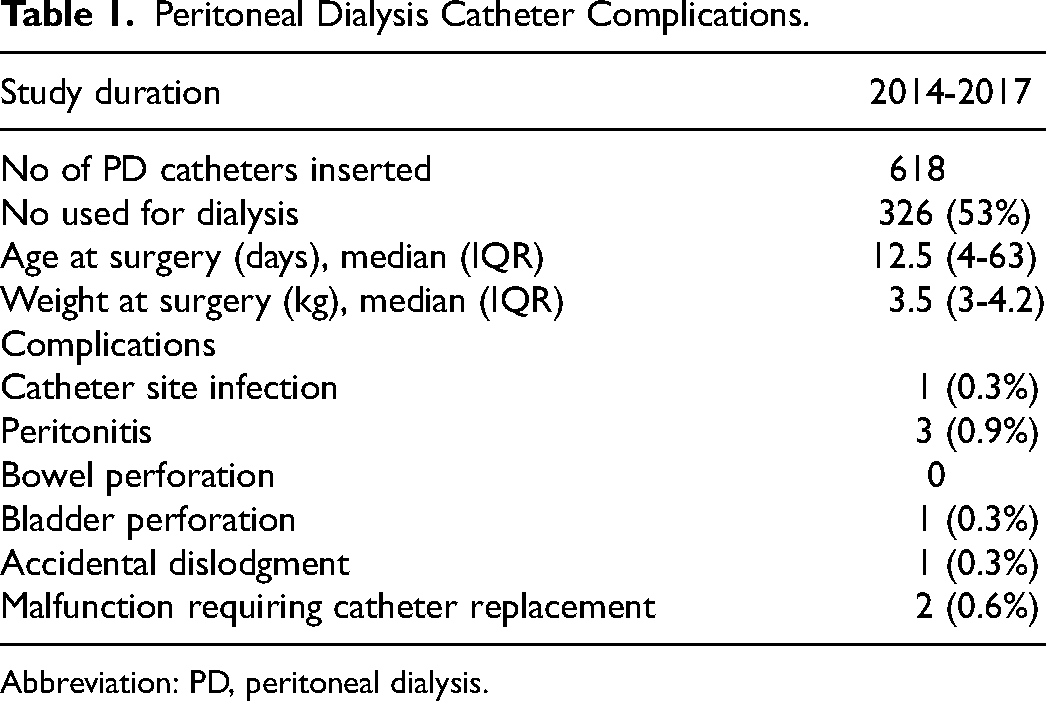
Abbreviation: PD, peritoneal dialysis.
Insertion of a reliable PD catheter encourages the use of prophylactic dialysis which has been associated with a reduction in major adverse events and is currently under investigation in a randomized control trial. 4
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.