
Abstract
Background
Late sequelae associated with chronic severe pulmonary regurgitation (PR) following transannular patch (TAP) repair of tetralogy of Fallot (TOF) have driven the use of alternative approaches. This study investigates mid-term pulmonic valve (PV) durability in TOF patients who underwent valve-sparing repair with intraoperative balloon dilation (VS-IBD).
Methods
Between 2010 and 2022, 139 TOF patients underwent VS-IBD (n = 66) or TAP (n = 73) repair at a single institution. Patients who underwent VS repair without IBD were excluded. Baseline differences were balanced by inverse probability of treatment weighting (IPTW). Primary outcome was freedom from reintervention, with median follow-up of 4.6 years.
Results
Valve-sparing repair with intraoperative balloon dilation patients were older (117 vs 64 days, P = .001) with higher PV annulus z-scores (−2.26 vs −2.62, P = .001) compared with TAP patients. After IPTW, VS-IBD patients had a higher reintervention rate (12.6% vs 2.2%, P = .028). At five years, 37/66 (56%) of VS-IBD patients remained free from ≥ moderate PR and 56/66 (85%) free from ≥ moderate pulmonic stenosis (PS). At the latest follow-up, VS-IBD patients demonstrated less right ventricular (RV) dilation (severe: 1.0% vs 15.5%, P = .002) and similar RV function (normal: 88.0% vs 91.8%, P = .273) as their TAP counterparts. In multivariable Cox analysis of VS-IBD patients, female sex (hazard ratio, HR [95% confidence interval, CI]: 4.4 [1.5, 13.2], P = .008) and preoperative PV z-score −2.67 to −2.18 (HR [95% CI]: 5.7 [1.6, 19.6], P = .006) were risk factors for developing ≥ moderate PR.
Conclusions
Despite a higher early reintervention rate, the trade-off for VS-IBD patients appears to be better-preserved valve competency overall, as well as less adverse RV remodeling.
Keywords
Introduction
Occurring in four out of 10,000 live births, tetralogy of Fallot (TOF) is the most common form of cyanotic congenital heart disease. 1 Elective primary repair of TOF in early infancy has traditionally involved ventriculotomy with transannular patch (TAP), which still remains the most prevalent technique. 2 Although this approach is highly effective in relieving right ventricular outflow tract (RVOT) obstruction, iatrogenic severe pulmonary regurgitation (PR) following TAP repair may lead to deleterious right ventricular (RV) remodeling over time, and progressive RV dilation and dysfunction have been shown to be risk factors for biventricular dysfunction, decreased exercise capacity, ventricular arrhythmias, and sudden cardiac death in this patient population.3–5 As a result, these patients often require late pulmonic valve (PV) replacement. 6
Valve-sparing approaches for TOF repair have been developed in recent decades in an attempt to avoid the late sequelae of chronic severe PR and the need for reoperation. Through the preservation of the native PV architecture and function, PV-sparing techniques aim to strike a balance between leaving residual pulmonic stenosis (PS) and avoiding chronic severe PR.7–13 In particular, valve-sparing repair utilizing intraoperative balloon dilation (VS-IBD) draws from prior observations that valve annuli can grow and remodel over time after percutaneous transcatheter balloon valvuloplasty of isolated PS.14–16 Although experience with the VS-IBD approach has increased over time, there is still a paucity of data on how these patients fare years after surgery. This retrospective study aimed to evaluate mid-term outcomes of TOF patients who underwent VS-IBD or TAP repair at our institution over a period of 12 years.
Patients and Methods
Study Cohort
This study was approved by the Columbia University Institutional Review Board (Protocol AAAU9729 approved on January 5, 2024) with a waiver of consent due to existing hospital records. A retrospective review of the electronic medical record was performed for 281 consecutive TOF patients with PS who underwent primary repair between February 2010 and December 2022 at New York-Presbyterian/Morgan Stanley Children's Hospital at Columbia University Irving Medical Center. Patients with anomalous coronary artery crossing the RVOT, no intervention on the PV, valve-sparing repair without IBD, prior RVOT stent, significant concomitant cardiac surgery, complex genetic syndromes, and age over two years were excluded from the study.
The 139 patients included in this study were stratified into VS-IBD (n = 66) and TAP (n = 73) cohorts based on the technique utilized during surgery. Distribution of PV annulus z-scores and frequency of VS-IBD versus TAP within each z-score range are shown in Supplemental Figure S1. Clinical characteristics, operative details, postoperative complications, reinterventions, and echocardiographic data were extracted from retrospective review of the electronic medical record and compared between cohorts. Missing data are shown in Supplemental Table S1 and were excluded from the analysis. Median follow-up time was 3.3 and 5.4 years in VS-IBD and TAP cohorts, respectively.
Study Endpoints
The primary outcome of this study was PV or RVOT reintervention. Secondary outcomes were echocardiographic parameters at last follow-up, including the degree of PR, PS, RV dilation, and RV function.
Operative Technique
Four out of seven total surgeons performed VS-IBD repairs in TOF/PS patients during the study period. At our institution, we utilize standard cardiopulmonary bypass (CPB) techniques with bicaval cannulation and moderate hypothermia for VS-IBD repair. After cardioplegic arrest, the right atrium is opened, intracardiac anatomy inspected, and a left ventricular vent is placed through the atrial septum. The ventricular septal defect (VSD) is inspected, and the decision is made to close the defect through a transatrial or transventricular approach. We have a relatively low threshold for performing a limited right ventriculotomy at the time of VS-IBD repair to help provide adequate exposure for VSD repair, RVOT muscle bundle resection, and/or assessment of the PV and subvalvar apparatus while keeping the incision to a minimum. In cases where the VSD can be closed adequately through a transatrial approach, the inferior extent of the right ventriculotomy can be lessened to avoid the potential impact on RV function. The main pulmonary artery (MPA) is opened longitudinally in almost every case to inspect and size the PV.
The PV is spared according to the surgeon's discretion based on the diameter of the PV annulus and anatomy of its cusps. Simple PV commissurotomy is generally done for patients with mild or moderate PS with only mildly dysplastic PV (not included in this study). For patients with moderate PS or PV dysplasia, the surgeon may elect to perform VS-IBD repair. With this technique, commissurotomy is followed by sizing of the effective PV orifice with Hegar dilators. A balloon 1 mm wider than the largest Hegar size that passes through the valve easily is then inserted through the infundibular incision or unopened RVOT transatrially. The balloon is inflated by hand with careful visual monitoring, and subsequent balloons are gradually increased in size by 1-mm increments until the beginning of a tear occurs at the annulus or cusps, at which time inflation is stopped. If the leaflet tear is large enough to require repair, the tear is patched using CorMatrix (CorMatrix Cardiovascular), native pericardium, or bovine pericardium. More recently, we have just accepted these tears and not repaired them with no impact on valve regurgitation, at least in the short term. In patients with supra-annular stenosis who are undergoing a VS repair, a posterior wall incision in the MPA is also considered if the most posterior sinus is tight.
After PV repair, both the MPA and RVOT incisions are patched. After separating from CPB following VS-IBD repair, we measure RVOT gradients by transesophageal echocardiography and RV pressures by direct measurement. In general, we accept a peak RVOT gradient < 20 mm Hg and an RV pressure < 50% systemic. Additional details of our VS-IBD technique have been described previously. 11
Statistical Analysis
Continuous variables were assessed for normality by the Shapiro-Wilk test and reported as median [interquartile range] as all were non-normally distributed. Categorical variables are presented as proportions with absolute numbers. Categorical variables were compared using the χ2 or Fisher exact test, as appropriate, and continuous variables were compared using the Mann-Whitney U test. PV annulus z-score categories were determined based on tertiles in the study cohort's z-score distribution to create three equal groups.
Inverse probability of treatment weighting (IPTW) with a covariate-balancing propensity score method was utilized to balance baseline differences between VS-IBD and TAP cohorts. Seven covariates were included in the binary logistic regression model due to potential associations with the outcomes of this study: sex, age, birth weight, gestational age, genetic syndrome, PV annulus z-score (Boston), and PV annulus diameter. A standardized mean difference (SMD) < 0.2 was considered an indicator of adequate balance, 17 with Supplemental Figure S2 displaying the distribution of SMD values before and after IPTW.
Kaplan-Meier analysis was performed for freedom from reintervention and freedom from at least moderate PR or PS, with P values generated by log-rank test. Multivariable Cox regression analysis of the VS-IBD cohort was utilized to identify risk factors for developing at least moderate PR after surgery. The proportional hazard assumption was evaluated by the Schoenfeld residuals plot and found not to be violated. No collinearity was found among variables in the multivariable models given all variance inflation factors < 2. Results are presented as hazard ratio (HR) with a corresponding 95% confidence interval (CI). All statistical analyses for the current study were performed with R statistical software (version 3.6.1; R Foundation).
Results
Patient Demographics and Preoperative Characteristics
Of the 139 patients included in the study, 66 patients underwent VS-IBD repair and 73 underwent TAP repair. Valve-sparing repair with intraoperative balloon dilation patients were older (median 117.0 vs 64.0 days, P = .001) and had larger preoperative PV annulus z-score (median −2.3 vs −2.6, P = .001) and diameter (median 6.8 vs 5.5 mm, P < .001) compared to TAP patients (Supplemental Table S2). After baseline differences were balanced with IPTW, 46.1% of VS-IBD patients were female with median age of 99.5 days (interquartile range [IQR]: 56.9, 140.8 days) at time of surgery. Median preoperative PV annulus diameter and z-score for the adjusted VS-IBD cohort were 6.1 mm (IQR: 4.6, 7.0 mm) and −2.4 (IQR: −2.8, −2.0), respectively (Table 1).
Inverse Probability of Treatment Weighted Baseline Characteristics of TOF Patients who Underwent VS-IBD or TAP Repair, Adjusted for Sex, Age, Birth Weight, Gestational Age, Genetic Syndrome, PV Annulus Z-Score (Boston), and PV Annulus Diameter (Shaded in Gray).
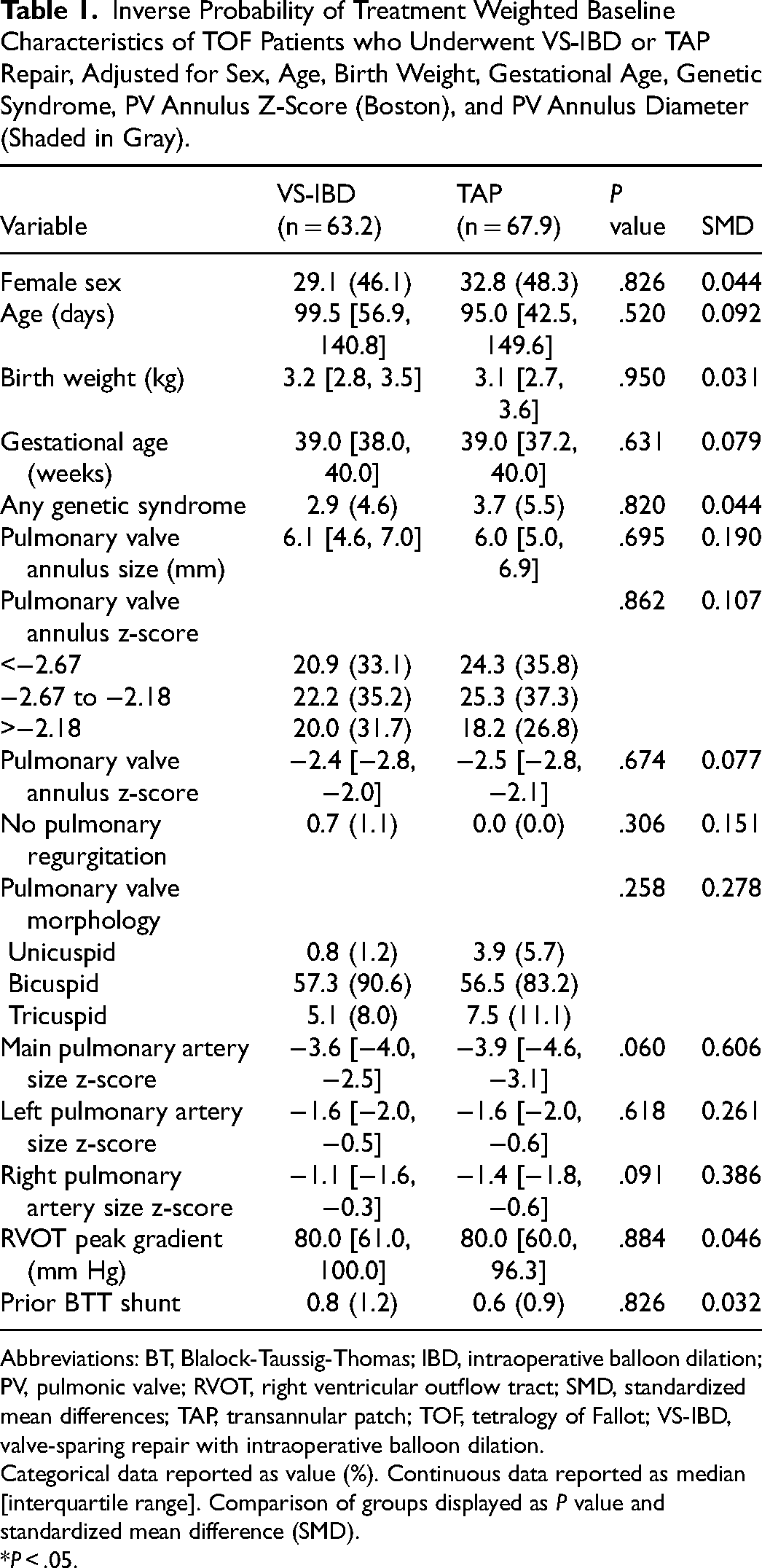
Abbreviations: BT, Blalock-Taussig-Thomas; IBD, intraoperative balloon dilation; PV, pulmonic valve; RVOT, right ventricular outflow tract; SMD, standardized mean differences; TAP, transannular patch; TOF, tetralogy of Fallot; VS-IBD, valve-sparing repair with intraoperative balloon dilation.
Categorical data reported as value (%). Continuous data reported as median [interquartile range]. Comparison of groups displayed as P value and standardized mean difference (SMD).
*P < .05.
Intraoperative Data
All intraoperative details are displayed in Table 2. In adjusted cohorts, 6.1/67.9 (8.9%) of TAP patients had initially undergone attempted VS repair which was converted to TAP intraoperatively. Each VS-IBD patient had a median of two balloon dilations performed (IQR: 1, 2) with median maximum balloon size to preoperative PV annulus diameter ratio of 1.3 (IQR: 1.1, 1.6). In addition to balloon dilation, all VS-IBD patients underwent commissurotomy of the PV, and 2.8/63.2 (4.4%) underwent leaflet patch augmentation. A limited right ventriculotomy was performed in 58.6/63.2 (92.8%) of VS-IBD patients. Concomitant left pulmonary arterioplasty (4.7% vs 14.9%, P = .038) and closure of patent foramen ovale or atrial septal defect (1.4% vs 9.6%, P = .036) were significantly less common in the VS-IBD group compared with TAP counterparts. While CPB time remained comparable (118.0 vs 108.3 min, P = .409), aortic cross-clamp time was longer (82.0 vs 70.6 min, P = .019) in the VS-IBD cohort. Post-CPB intraoperative transesophageal echocardiogram demonstrated significantly lower rates of severe PR (2.7% vs 71.2%, P < .001) and similar RV function (normal: 74.1% vs 83.3%, P = .273) in the VS-IBD group, although more of these patients had residual mild PS (52.2% vs 15.1%, P < .001).
Intraoperative Details for Inverse Probability of Treatment Weighted TOF Patients Who Underwent VS-IBD or TAP Repair.
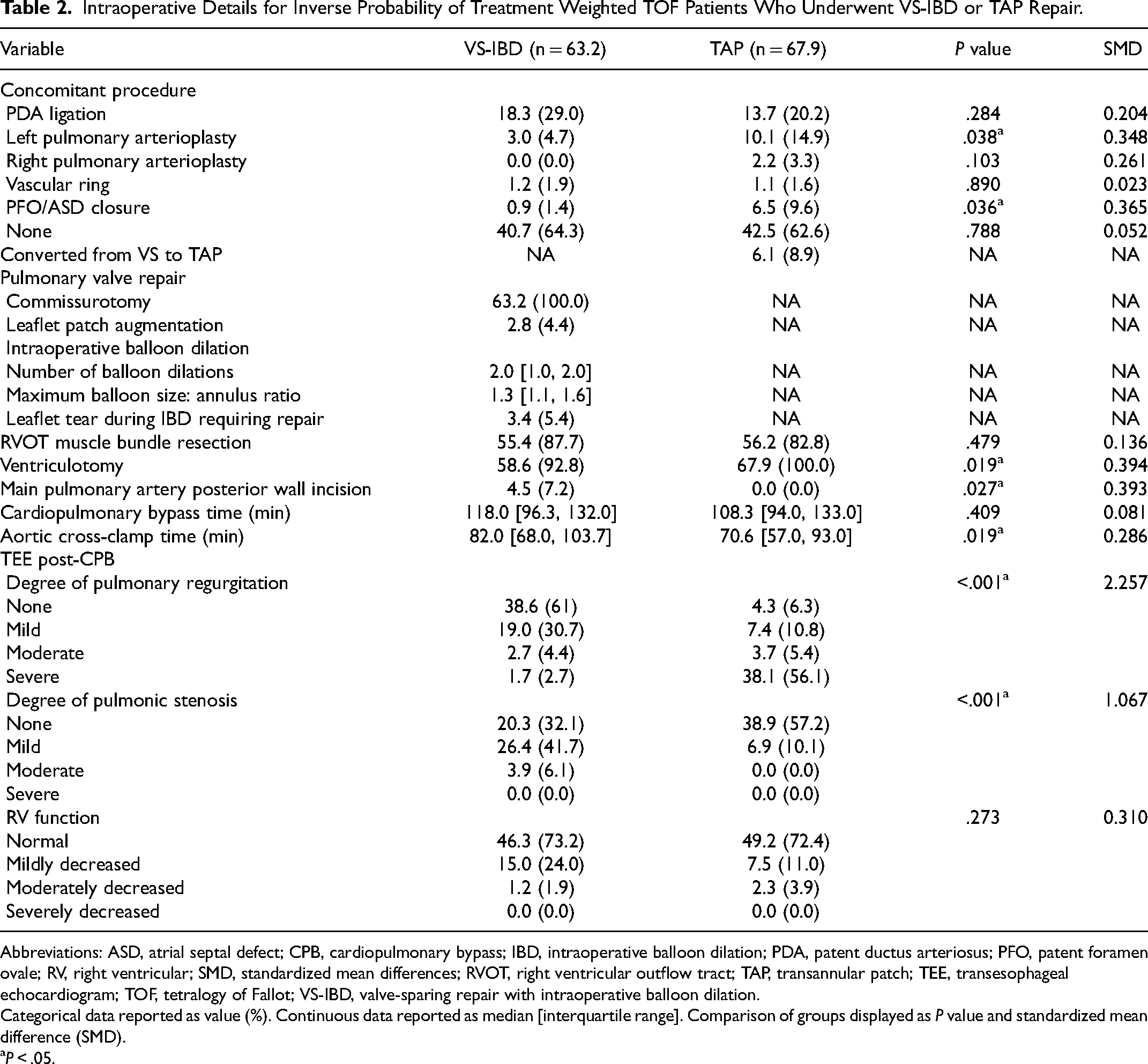
Abbreviations: ASD, atrial septal defect; CPB, cardiopulmonary bypass; IBD, intraoperative balloon dilation; PDA, patent ductus arteriosus; PFO, patent foramen ovale; RV, right ventricular; SMD, standardized mean differences; RVOT, right ventricular outflow tract; TAP, transannular patch; TEE, transesophageal echocardiogram; TOF, tetralogy of Fallot; VS-IBD, valve-sparing repair with intraoperative balloon dilation.
Categorical data reported as value (%). Continuous data reported as median [interquartile range]. Comparison of groups displayed as P value and standardized mean difference (SMD).
P < .05.
Early and Mid-Term Postoperative Data
Postoperative RVOT peak gradient measured by transthoracic echocardiography at the time of hospital discharge was higher in the VS-IBD group (24.8 vs 20.0 mm Hg, P = .003). Hospital length of stay was shorter in VS-IBD patients (6.0 vs 8.0 days, P = .014) compared with the TAP group, but in-hospital mortality (3.6% vs 4.3%, P = .892) and various postoperative complications during index hospitalization remained similar. Reinterventions on the PV or RVOT were more common after VS-IBD (12.6% vs 2.2%, P = .028) (Table 3), and all four reinterventions in the VS-IBD cohort occurred within the first year after surgery (Figure 1). One VS-IBD patient required RVOT patch revision with repeat balloon dilation of the PV 21 days after the initial surgery, one underwent transcatheter balloon valvuloplasty for decreased RV function in the setting of residual PS at three months postoperatively, one required conversion to TAP for worsening PS at six months postoperatively, and one underwent valve-sparing transannular repair for recurrent PS at nine months after surgery. Of the two TAP patients who required reintervention during the study period, one patient had further RVOT muscle bundle resection two years after surgery for recurrent infundibular stenosis and the other underwent late surgical PV replacement nearly eight years after surgery due to rapid RV dilation in the setting of chronic free PR (Supplemental Table S3).
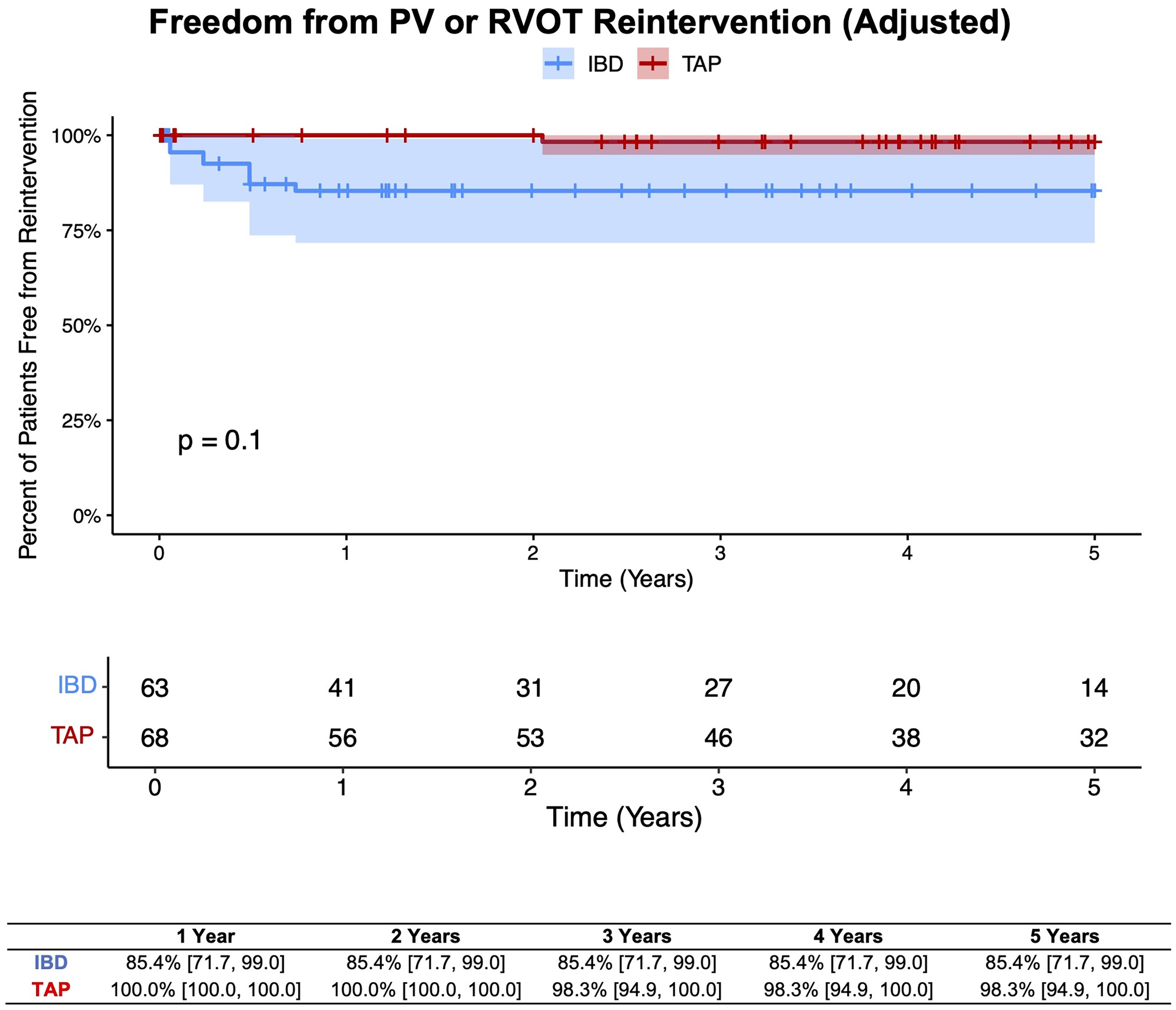
Five-year freedom from pulmonic valve (PV) or right ventricular outflow tract (RVOT) reintervention in inverse probability of treatment weighted tetralogy of Fallot (TOF) patients who underwent valve-sparing repair with intraoperative balloon dilation (VS-IBD) or transannular patch (TAP) repair. Log-rank P value and percentage [95% confidence interval] of patients free from the outcome at each time point are displayed.
Postoperative Outcomes for Inverse Probability of Treatment Weighted TOF Patients Who Underwent VS-IBD or TAP Repair.
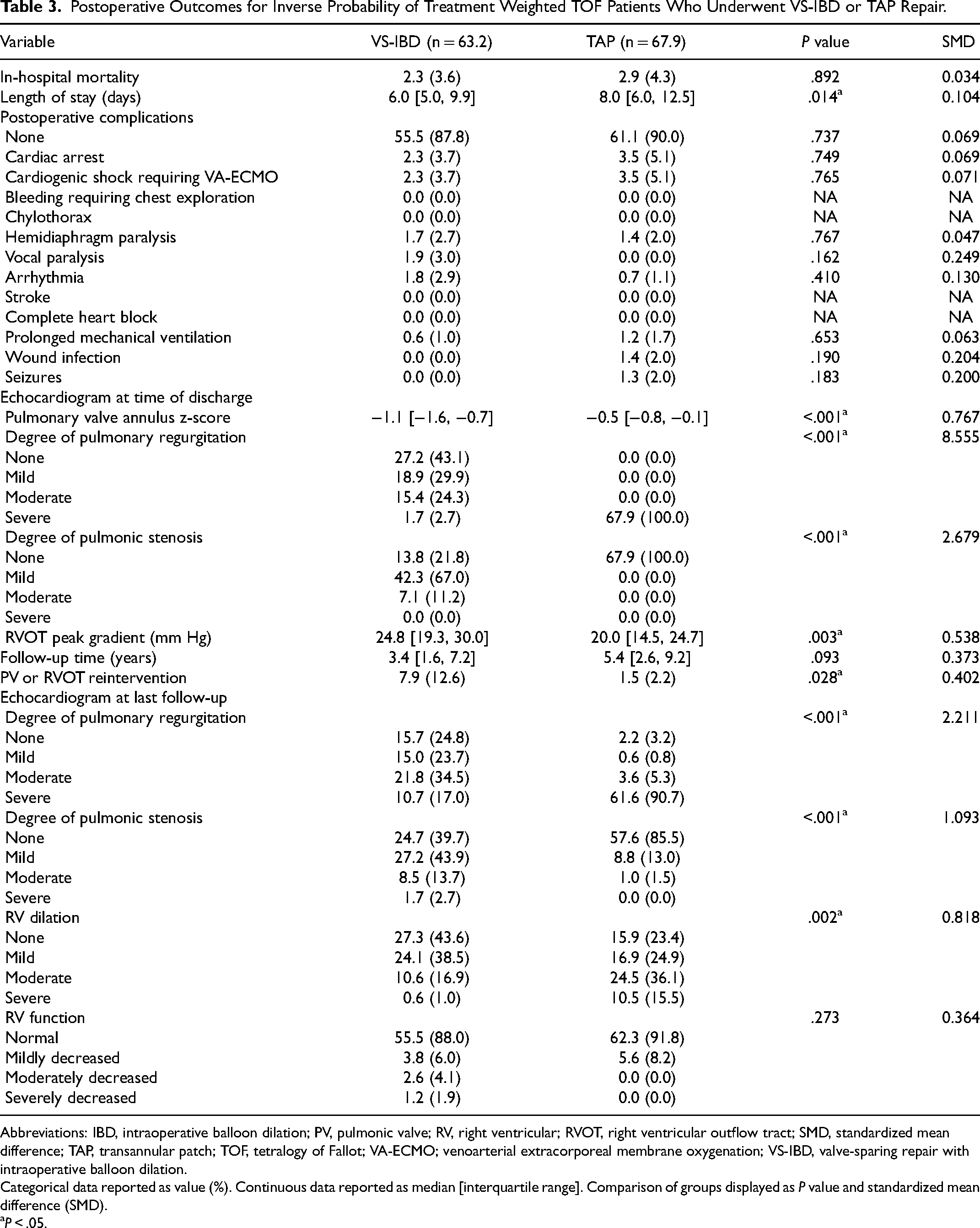
Abbreviations: IBD, intraoperative balloon dilation; PV, pulmonic valve; RV, right ventricular; RVOT, right ventricular outflow tract; SMD, standardized mean difference; TAP, transannular patch; TOF, tetralogy of Fallot; VA-ECMO; venoarterial extracorporeal membrane oxygenation; VS-IBD, valve-sparing repair with intraoperative balloon dilation.
Categorical data reported as value (%). Continuous data reported as median [interquartile range]. Comparison of groups displayed as P value and standardized mean difference (SMD).
P < .05.
As for mid-term PV competency, 36.9/66 (55.9%) of patients in the adjusted VS-IBD cohort remained free from at least moderate PR (Figure 2) and 56/66 (85.0%) free from at least moderate PS (Figure 3) at five years. When examining at least moderate PR or PS as a composite outcome, 50.3% of VS-IBD patients remained free from both outcomes at five years, in contrast to 3.9% of TAP patients (P < .001) (Figure 4). Furthermore, transthoracic echocardiogram at the latest follow-up showed that VS-IBD patients had less severe RV dilation (1.0% vs 15.5%, P < .002) although similar overall RV function (normal: 88.0% vs 91.8%, P = .273) as their TAP counterparts (Table 3). Unadjusted analyses are shown in Supplemental Figures S3 to S7 and Supplemental Tables S4 to S5. Multivariable Cox regression analysis of VS-IBD patients identified female sex (HR [95% CI]: 4.430 [1.483, 13.228], P = .008) and preoperative PV annulus z-score between −2.67 and −2.18 (HR [95% CI]: 5.680 [1.646, 19.602], P = .006) as independent risk factors for developing at least moderate PR (Table 4).
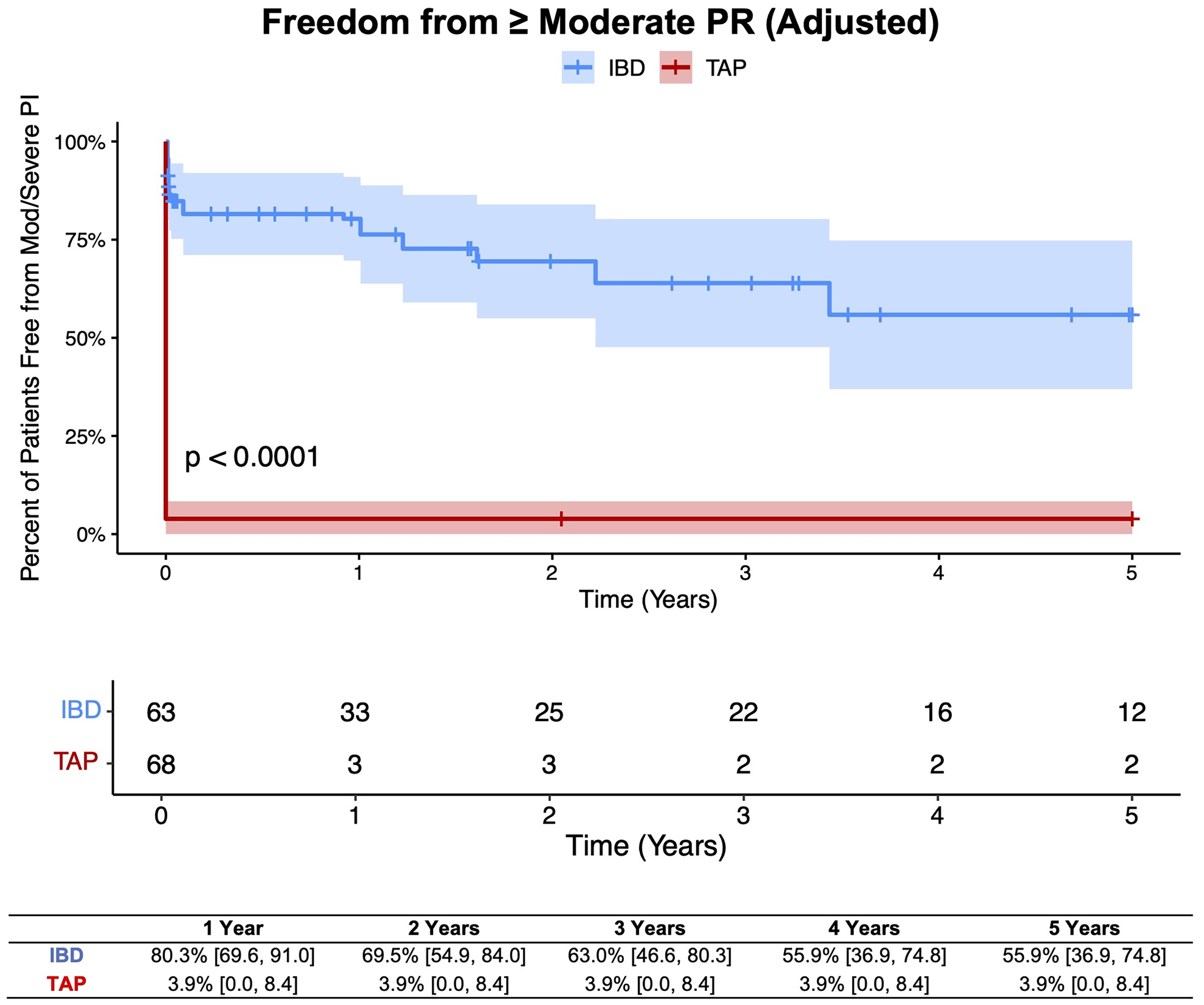
Five-year freedom from at least moderate pulmonary regurgitation (PR) in inverse probability of treatment weighted tetralogy of Fallot (TOF) patients who underwent valve-sparing repair with intraoperative balloon dilation (VS-IBD) or transannular patch (TAP) repair. Log-rank P value and percentage [95% confidence interval] of patients free from the outcome at each time point are displayed.
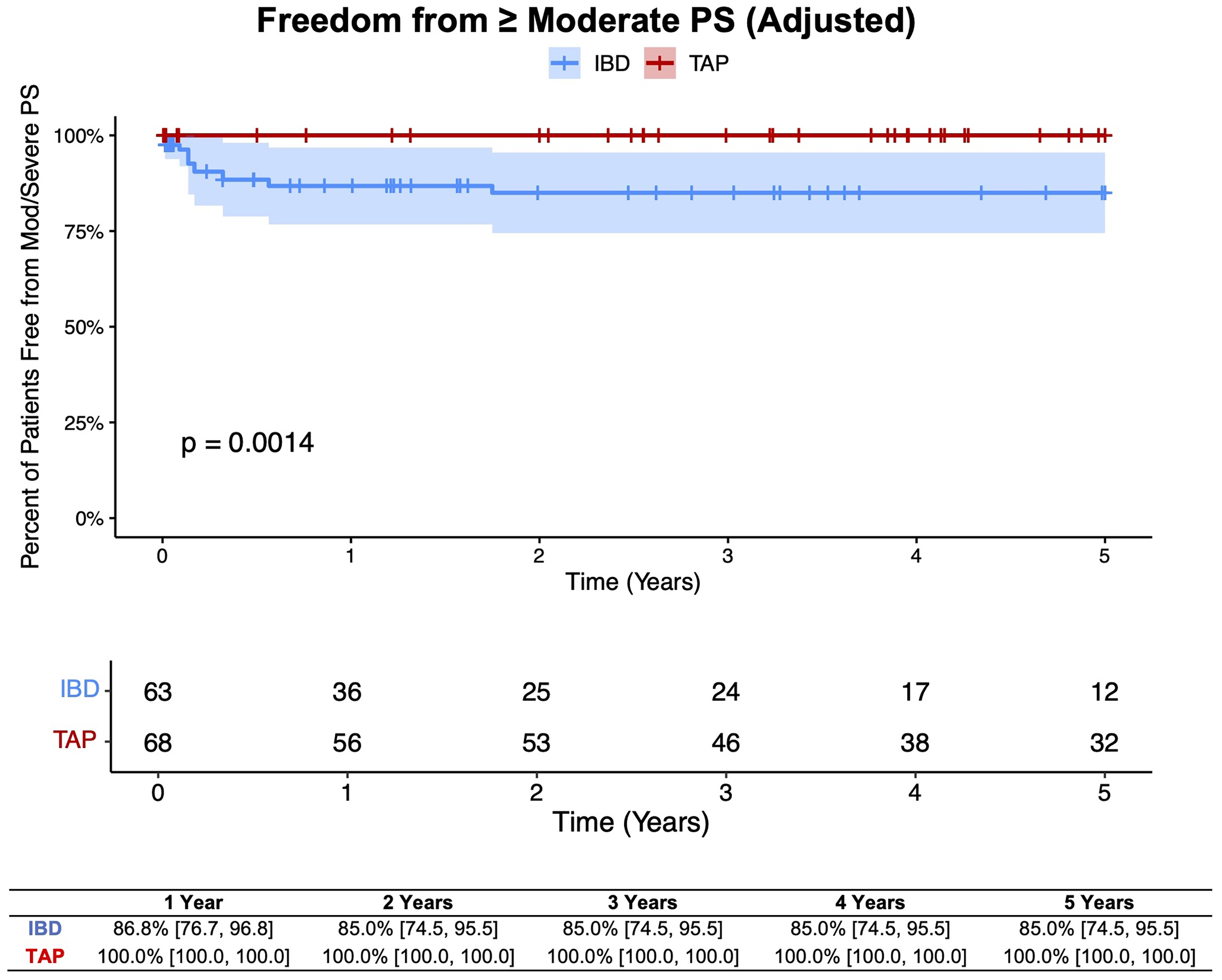
Five-year freedom from at least moderate PS in inverse probability of treatment weighted tetralogy of Fallot (TOF) patients who underwent valve-sparing repair with intraoperative balloon dilation (VS-IBD) or transannular patch (TAP) repair. Log-rank P value and percentage [95% confidence interval] of patients free from the outcome at each time point are displayed.
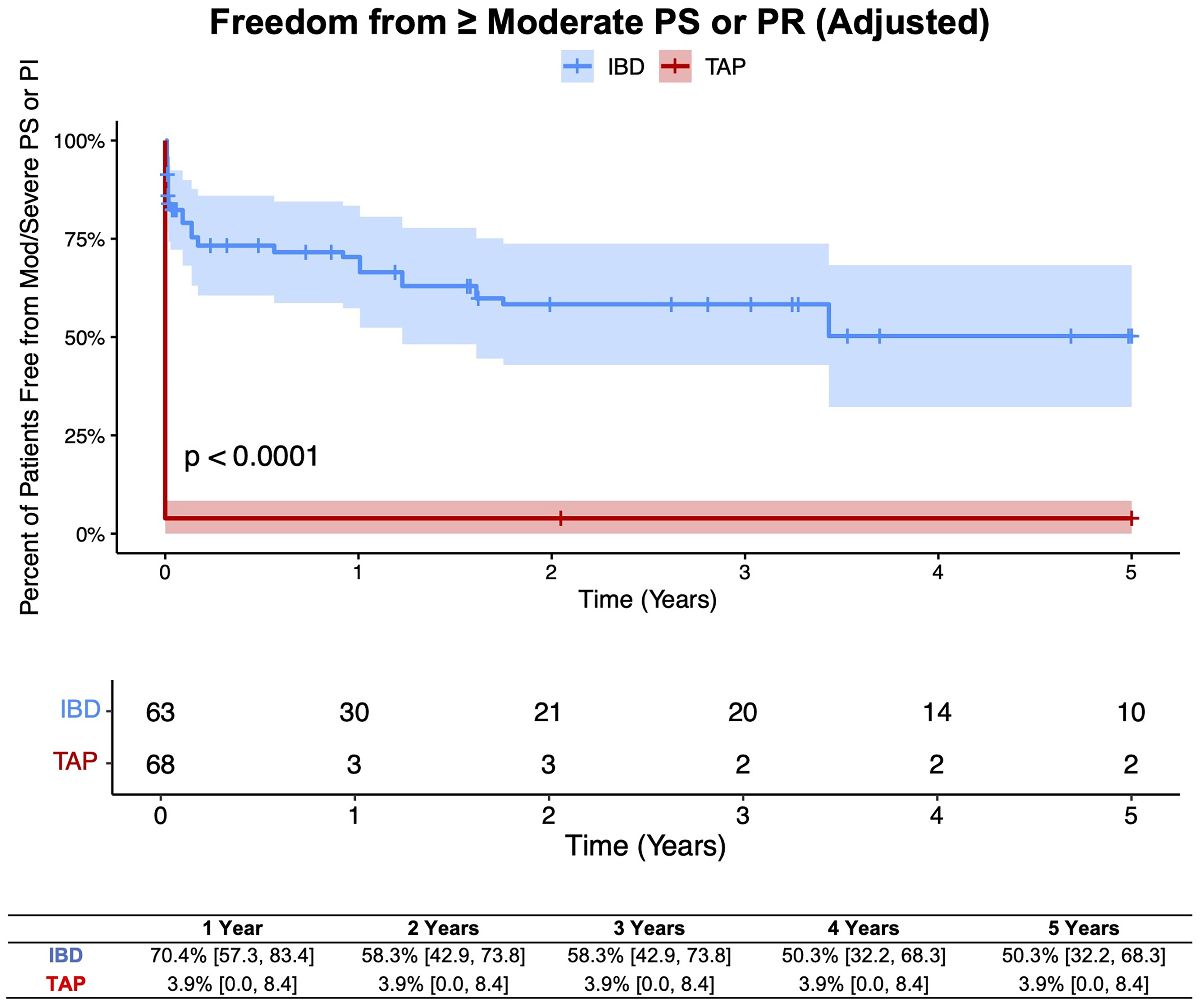
Five-year freedom from at least moderate PS or pulmonary regurgitation (PR) in inverse probability of treatment weighted tetralogy of Fallot (TOF) patients who underwent valve-sparing repair with intraoperative balloon dilation (VS-IBD) or transannular patch (TAP) repair. Log-rank P value and percentage [95% confidence interval] of patients free from the outcome at each time point are displayed.
Multivariable Cox Regression Analysis of Risk Factors for Developing at Least Moderate Pulmonary Regurgitation in TOF Patients Who Underwent VS-IBD Repair.
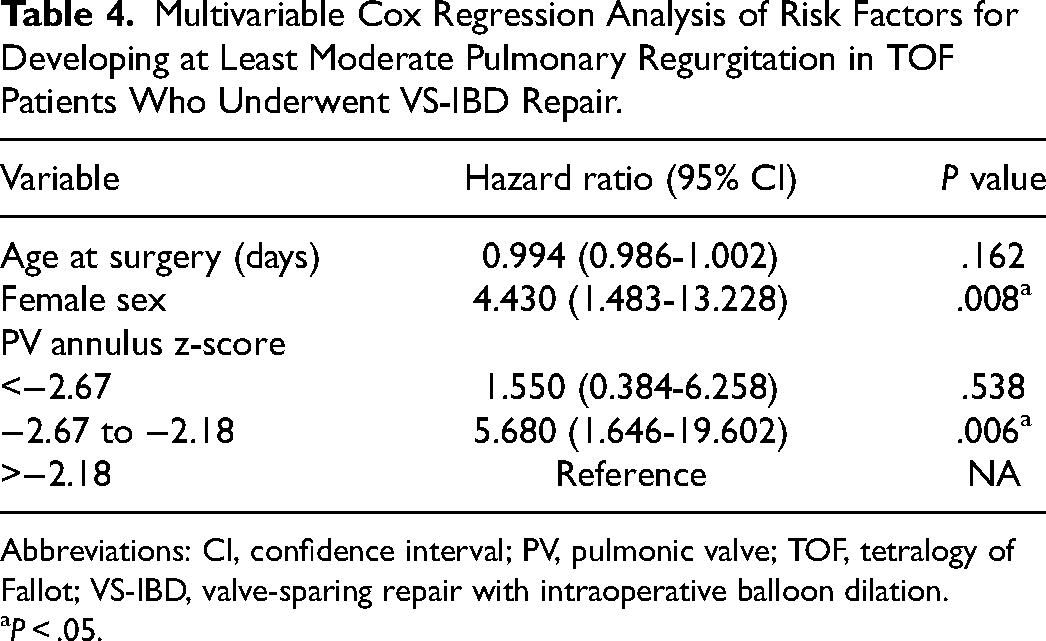
Abbreviations: CI, confidence interval; PV, pulmonic valve; TOF, tetralogy of Fallot; VS-IBD, valve-sparing repair with intraoperative balloon dilation.
P < .05.
Discussion
In this study, we present our 12-year institutional experience with the valve-sparing intraoperative balloon dilation technique for primary TOF repair. While the VS-IBD approach was associated with a higher rate of early reintervention, the absolute reintervention rate remained low. However, VS-IBD patients had better-preserved mid-term PV competency and less adverse RV remodeling compared with their TAP counterparts.
The strategy of using sharp commissurotomy followed by IBD to relieve PV stenosis was originally developed based on experience with transcatheter pulmonary valvuloplasty. 16 Balloon inflation across the PV orifice leads to radial transmission of stress, causing the valve annulus to dilate and stretch. This mechanism also allows for splitting of fused or incomplete leaflet commissures, which can subsequently introduce small tears in the annulus if the balloon diameter is sufficiently oversized. These radial tears not only enlarge the annulus but may also allow for remodeling and improved growth.14,15 In contrast to older valve-sparing techniques relying on rigid Hegar dilation, an inflatable balloon has the advantage of annular dilation in a static position and introduction into the valve orifice at a much smaller diameter.18,19
Mid-term outcomes with the VS-IBD technique have previously been reported by Hofferberth and colleagues. 12 In their study, 15.4% of patients required reintervention for residual valvar stenosis after VS-IBD repair, in contrast to 6.1% in our unadjusted analyses. After propensity matching these patients to a historical TAP cohort, they reported an early reintervention rate of 24.5% after VS-IBD. In a similar fashion, we utilized propensity score–based techniques and found this number to be only 12.6% at our institution, although we matched to TAP patients from the same era. Additionally, Hofferberth and coauthors reported 43% freedom from at least moderate PR at five years post-repair in their unadjusted VS-IBD cohort. In our analysis, 67% of the unadjusted VS-IBD cohort remained free from at least moderate PR at five years. More recently, Guariento and colleagues published their experience with 73 patients who underwent a variety of IBD techniques for TOF. 20 Although they did not utilize propensity score–based techniques to compare outcomes between VS-IBD and TAP repair, zero patients in their VS-IBD cohort required reintervention during the 14-year study period. Their findings contrast with those from our study and from Hofferberth and coauthors, suggesting that the VS-IBD approach can be associated with very low reintervention rates at early and mid-term follow-up. Altogether, the outcomes of VS-IBD repair appear variable. We acknowledge that there may be differences in techniques related to VS-IBD repair (ie, delamination, resuspension of the PV) that could contribute to the observed difference in reintervention rates between our study and the aforementioned studies. We also strongly believe that surgeon and center experience play a significant role in outcomes for this cohort of patients. Lastly, although median PV annulus z-score and several other baseline variables appeared comparable between these studies, there may be unmeasurable patient factors that could explain the outcome differences.
Regardless, the significantly higher rate of early reintervention after VS-IBD compared with TAP found in our study indicates that limiting PV annular enlargement with balloon dilation may leave a small fraction of patients with enough residual stenosis to require reoperation. The ultimate goal of this approach is to preserve the PV and consequently long-term RV function by avoiding chronic severe PR that requires eventual reoperation after TAP. Hofferberth and colleagues found that preoperative PV annulus z-score less than −2.45 was an independent risk factor for requiring PV reintervention in their VS-IBD cohort, while Guariento and colleagues found that z-score less than −2.85 was associated with increased risk of developing at least moderate PR at five years post-repair.12,20 While multivariable analysis for reintervention was not possible in our study due to the low number of events, we identified that PV z-score between −2.67 and −2.18 was associated with developing at least moderate PR in our VS-IBD cohort. Altogether these findings suggest that patients with significant annular hypoplasia may be less ideal candidates for this approach. As valve-sparing techniques continue to be developed and refined, it will be challenging but important to navigate the delicate balance between minimizing residual PS while preserving native PV architecture and function.
Although TAP was associated with lower early reintervention rates in our study, progressive adverse RV remodeling caused by chronic severe PR can occasionally lead to devastating long-term consequences.3–5 Some VS-IBD patients from our institution eventually developed progressive PR; however, approximately 50% of the cohort was able to avoid both significant PR and significant PS at five years postoperatively. Interestingly, our data suggest that female patients and those with lower preoperative PV annulus z-score may be more likely to develop significant PR after VS-IBD repair. Patient sex has previously been linked to differential outcomes after pediatric cardiac surgery and potentially attributed to biological differences in tissue remodeling, inflammatory response, metabolic reserves, and more. 21 When adjusted for procedural risk level, other studies have indeed reported a higher risk of postoperative mortality in female pediatric patients undergoing surgery for congenital heart disease.22,23
This retrospective, single-center study has several limitations to highlight. Due to inherent bias in patient selection for each type of repair, outcomes comparison can be challenging given differences in baseline PS severity and other anatomical factors. We attempted to mitigate this by adjusting for several important baseline differences with IPTW and subsequent multivariable regression modeling. However, quantitative variables, such as PV annulus z-score and diameter, only provide a partial picture of the effective PV orifice, and residual confounding may exist. Unmeasurable morphological differences also influence intraoperative decision-making, such as extent of balloon inflation and length of ventriculotomy, therefore impacting later outcomes. Moreover, variable surgeon experience and preference may contribute to bias. In addition, this study features patients who receive follow-up with outpatient cardiologists at other institutions; consequently, surveillance and thresholds for reinterventions may vary. Finally, although our study is one of the longest and largest to evaluate outcomes after VS-IBD, we focused on mid-term follow-up that is unlikely to capture the majority of late PV reinterventions after TAP repair. The results presented in this study should be interpreted in the context of follow-up data available.
In summary, our 12-year institutional experience with primary TOF repair utilizing the valve-sparing intraoperative balloon dilation technique demonstrates that despite a higher early reintervention rate, the trade-off for VS-IBD patients appears to be better-preserved overall PV competency and less adverse RV remodeling. More studies are warranted in the future to identify precise morphologic criteria to guide surgical decision-making as experience with valve-sparing approaches grows over time.
Supplemental Material
sj-docx-1-pch-10.1177_21501351251321528 - Supplemental material for Mid-Term Outcomes of Valve-Sparing Repair With Intraoperative Balloon Dilation in Tetralogy of Fallot
Supplemental material, sj-docx-1-pch-10.1177_21501351251321528 for Mid-Term Outcomes of Valve-Sparing Repair With Intraoperative Balloon Dilation in Tetralogy of Fallot by Morgan K. Moroi, Iris Feng, Alice V. Vinogradsky, Christine G. Yang, Stephanie N. Nguyen, David M. Kalfa, Andrew B. Goldstone and Emile A. Bacha in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Authors’ Note
Consent Information: Informed consent was waived by the Columbia University Institutional Review Board due to retrospective analysis of existing hospital records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This study received ethical approval from the Columbia University Institutional Review Board (approval #AAAU9729) on January 5, 2024.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.