
Abstract
Background
Carotid artery ligation has been a common practice after extracorporeal membrane oxygenation (ECMO) decannulation due to the risks of embolization, cerebral infarction, aneurysm, and stenosis over time. Carotid artery reconstruction (CAR) after ECMO decannulation is increasingly used, though studies report variable stenosis rates. Data on CAR in children with heart disease, who may require carotid artery patency for future surgery or repeat ECMO, are lacking.
Objective
To evaluate carotid artery patency and the incidence of cerebral infarction in pediatric cardiac patients after CAR and ECMO decannulation.
Methods
A retrospective review of children (0-21 years of age) who required venoarterial extracorporeal membrane oxygenation (VA-ECMO) via neck cannulation in the cardiovascular intensive care unit at a quaternary children's hospital (2015-2022) was conducted. Children who underwent CAR and survived to discharge were included.
Results
Fifty-three children (ages 2 days to 21 years, median, 2 years of age) met the study criteria. Carotid artery imaging was performed in 25 children (47%), with 84% (21/25) showing unobstructed arteries. Imaging follow-up ranged from two days to four years, with a median of three months. Of 33 children who had post-ECMO head imaging, 11 showed new cerebral infarcts, with 4 of those infarcts diagnosed following transition to ventricular assist device (VAD). Given the variability of timing and modality of head imaging and the significant proportion of patients on a VAD, we are unable to determine the true incidence of new infarcts following CAR.
Conclusion
Carotid artery reconstruction after VA-ECMO decannulation in children with congenital heart disease shows early favorable vessel patency, but the long-term neurological benefits compared with ligation remain unclear. Further prospective studies are needed to evaluate long-term patency and neurological outcomes.
Keywords
Introduction
Neonates placed on venoarterial extracorporeal membrane oxygenation (VA-ECMO) undergo either ligation or reconstruction of the carotid artery at the time of decannulation. When ECMO was first introduced for neonates, carotid artery ligation was a common practice due to the theoretical risk of embolization of a clot or air during or after reanastomosis potentially resulting in cerebral infarction.1,2 Other complications of carotid artery repair include aneurysm, infection, and stenosis as the infant grows. 2 However, ligation leaves the patient with a single carotid artery which raises concern about potential neurologic sequelae, especially in patients who do not have a complete circle of Willis and therefore do not develop adequate collateral circulation. 1 Some studies have reported infants who had computed tomography (CT) scans after decannulation having either right cerebral hemispheric ischemic abnormalities or contralateral hemorrhagic changes consistent with hyperperfusion of the left hemisphere.3,4 In addition, vessel ligation does not allow for repeat access for ECMO or cardiac catheterization at that site. 5 This is especially relevant for patients with congenital heart disease (CHD) where risk of repeat ECMO is the highest. 5
Successful carotid artery repair after ECMO was first reported in 1990 by Crombleholme et al and Adolph et al independently.6–8 Studies examining the patency of the artery over time have had mixed results, with some showing high rates of patency while others showing elevated rates of stenosis. A recent review of 80 studies showed carotid artery patency rates ranged from 44% to 100% with variable follow-up time of 0 to 11 years. 9 There is also significant variability in practice, with a recent survey showing 90% of general surgeons ligating the carotid artery and 83% of cardiothoracic surgeons performing carotid artery reconstruction (CAR). 10 Most studies on CAR in the pediatric population include patients who required ECMO due to respiratory failure from causes such as congenital diaphragmatic hernia or meconium aspiration.1,6,11,12 There is a paucity of data in the CHD population, in whom CAR may be beneficial given the risk for recurrent ECMO cannulations. Our aim is to describe the patency rate of CAR in patients with congenital or acquired heart disease. Given that the neurologic sequela of CAR remains largely unknown, our secondary aim is to describe the incidence of cerebral infarction following ECMO decannulation and CAR.
Methods
This is a retrospective review of children 0- to 21-years of age admitted to the cardiovascular intensive care unit at a quaternary children's hospital from 2015 to 2022. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and received approval from the Stanford Institutional Review Board. Confidentiality and anonymity of the participants were strictly maintained throughout the study.
Children who were cannulated to VA-ECMO via neck cannulation, had their carotid artery reconstructed, and survived to discharge were included. A chart review of the children's demographics, underlying diagnosis leading to ECMO cannulation, whether extracorporeal cardiopulmonary resuscitation (ECPR) was required, duration of ECMO, length of hospitalization, and intensive care unit (ICU) duration was performed. The operative note for each child was reviewed to evaluate whether CAR was performed at the time of decannulation.
The primary outcome measure was patency of the carotid artery. For patients who received follow-up imaging, ultrasound (US) and CT of the carotid artery were evaluated for patency. Given that not all CT reports commented on the carotid artery, a separate cardiac imaging expert reviewed the images and confirmed whether the carotid artery was patent or occluded. The secondary outcome was to describe the incidence of cerebral infarction following CAR. Ultrasound, CT, and magnetic resonance imaging (MRI) of the head prior to cannulation and after decannulation were reviewed for abnormalities such as ischemic or hemorrhage stroke. Only neurological imaging after the first ECMO course were included for children requiring more than one ECMO course. Descriptive statistics such as median, mean, and frequency were utilized to summarize baseline characteristics and outcome measures. Chi-square and Wilcoxon rank-sum tests were used in Statistical Package for the Social Sciences software to compare the differences between pateints who received imaging and those who did not. 13
Results
Fifty-three patients met the study inclusion criteria. There were 24 (45%) females and 29 males ranging from 2 days to 21 years of age and a median age of two-years (Table 1). The top three underlying diagnoses for ECMO cannulation were primary arrhythmias, myocarditis, and cardiomyopathy, respectively. The other indications for ECMO included obstruction to pulmonary blood flow, respiratory arrest/acute respiratory distress syndrome, rejection following heart transplantation, coronary artery obstruction, drug toxicity, right ventricular failure, and sepsis (Table 1). Thirteen of 53 patients (24%) required ECPR and 10 patients were transitioned to a ventricular assist device (VAD) following ECMO. The duration of ECMO ranged from 1 to 25 days with a median of seven days. The duration of ICU stay ranged vastly from 3 to 202 days with a median of 27 days, and the duration of total hospitalization ranged from 5 to 242 days with a median of 38 days. There were no significant differences in age or duration of ECMO in patients who received carotid artery and head imaging compared with those who did not (Table 2). Patients requiring ECPR were more likely to receive head imaging (10/13 or 77%), although this difference was not statistically significant. Patients with cardiomyopathy were more likely to receive both head imaging (100%) and carotid artery imaging (7/8, 87%) (see Supplemental Table 1).
Demographics and Clinical Characteristics of Patients Receiving Carotid Artery Reconstruction Following Decannulation From VA-ECMO (N = 53).
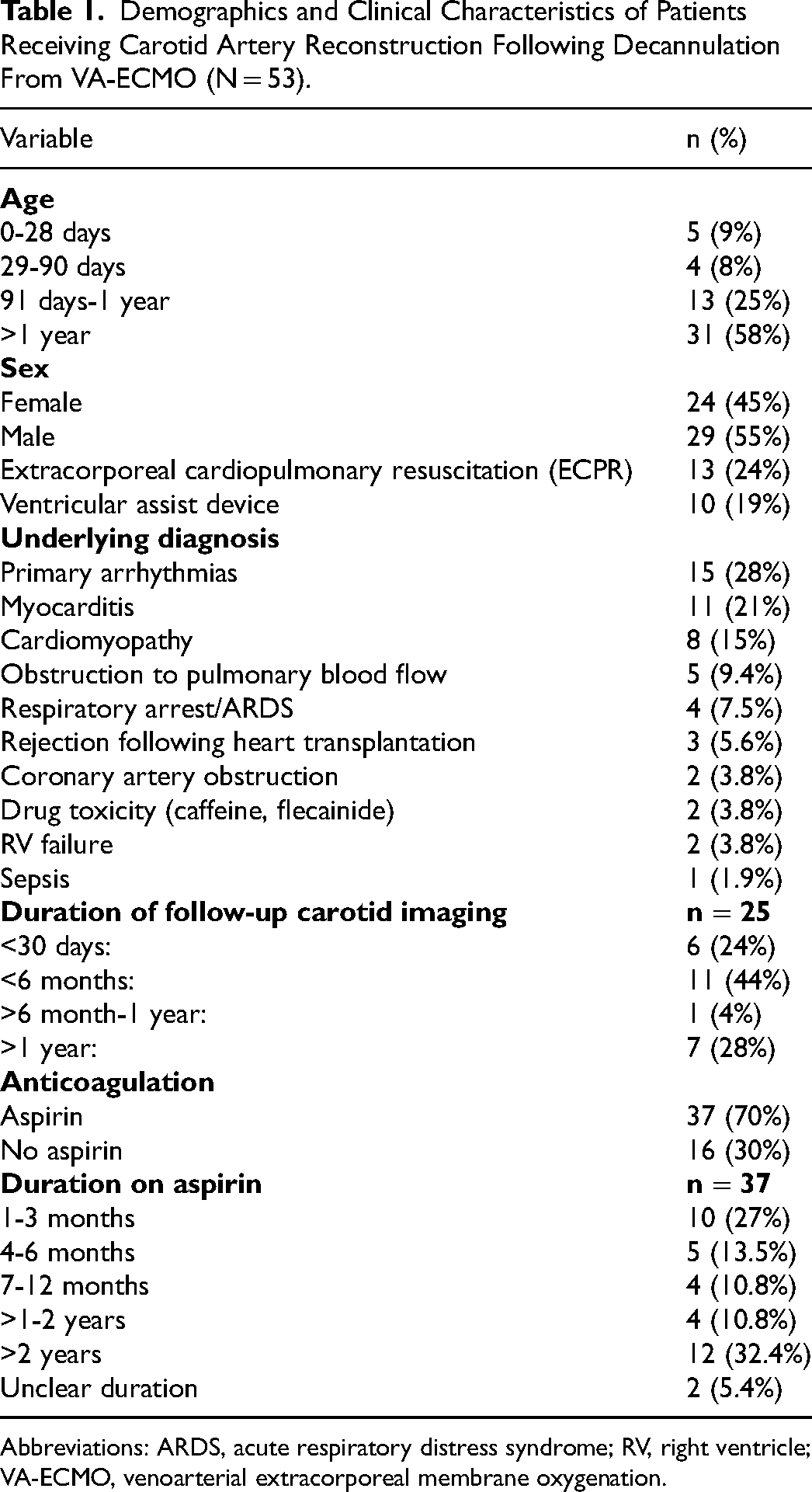
Abbreviations: ARDS, acute respiratory distress syndrome; RV, right ventricle; VA-ECMO, venoarterial extracorporeal membrane oxygenation.
Comparison of Patient Characteristics With and Without Carotid Artery and Head Imaging.

Abbreviation: ECMO, extracorporeal membrane oxygenation; ECPR, extracorporeal cardiopulmonary resuscitation.
Characteristics of New Cerebral Infarcts Diagnosed Post ECMO Decannulation and Carotid Artery Reconstruction (n = 11).
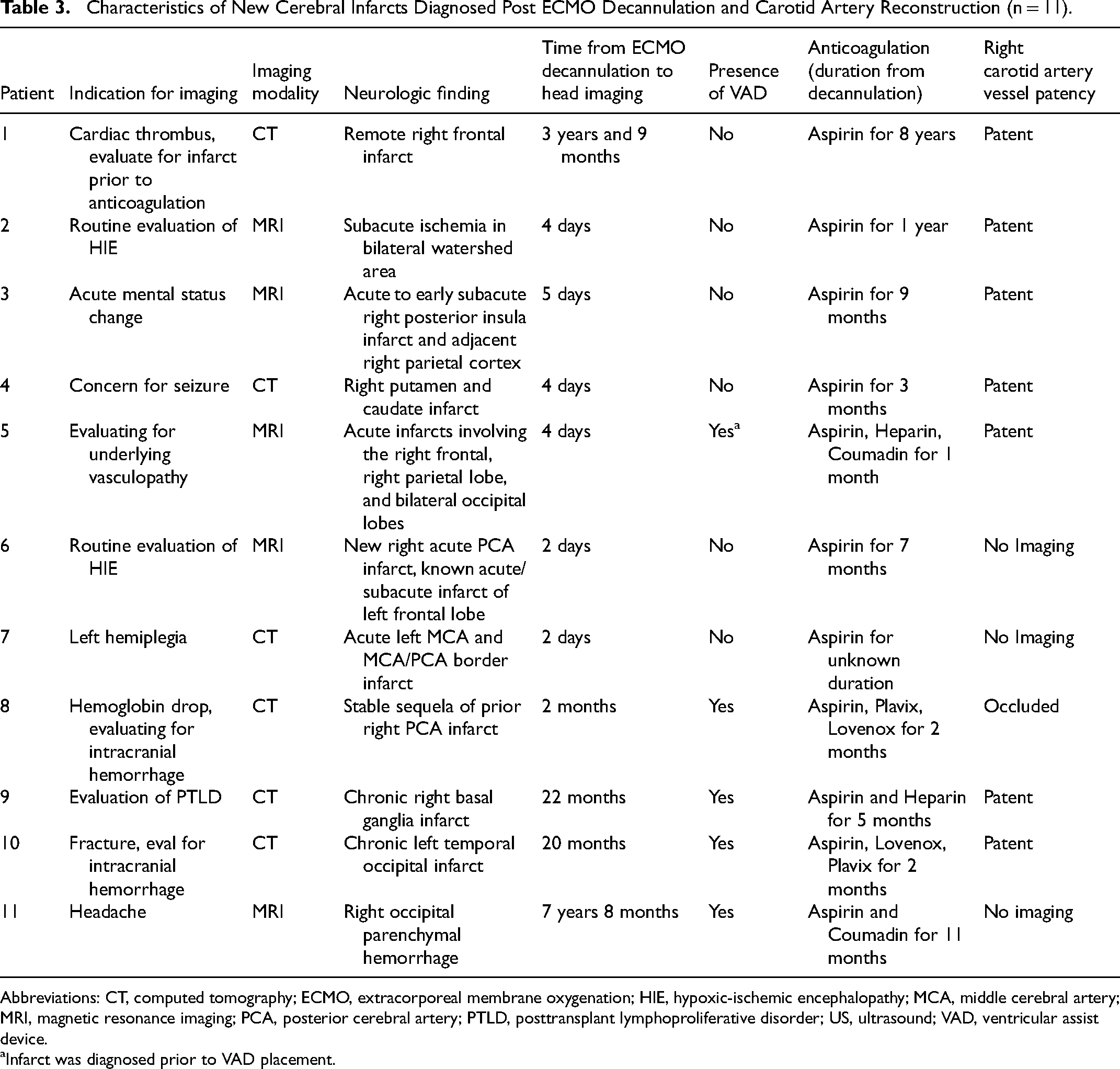
Abbreviations: CT, computed tomography; ECMO, extracorporeal membrane oxygenation; HIE, hypoxic-ischemic encephalopathy; MCA, middle cerebral artery; MRI, magnetic resonance imaging; PCA, posterior cerebral artery; PTLD, posttransplant lymphoproliferative disorder; US, ultrasound; VAD, ventricular assist device.
Infarct was diagnosed prior to VAD placement.
Thirty-seven of 53 (70%) of patients received aspirin for anticoagulation post CAR. For the 16 patients who were not on aspirin, one was on bivalirudin and Plavix for three weeks while on a VAD, two were on Apixaban for venous thrombus, and two were on Lovenox for venous thrombus, and nine were not on any anticoagulation. The duration of aspirin therapy ranged vastly from 1 month to 9.5 years with a median duration of nine months (Table 1). It is our institutional practice to prescribe aspirin for three to six months following CAR for thromboprophylaxis. However, this is dependent on the individual surgeon, and the practice is not consistently followed. The patients who were on aspirin for a shorter duration of time tended to be patients on VADs and once they received their heart transplant, all anticoagulation was discontinued. The patients who were on aspirin for several years did so for other indications such as indwelling stents, right ventricle to pulmonary artery (RV-PA) conduits, or atrial septal defect device closure.
Of 53 patients 25 (47%) had follow-up imaging of the carotid artery following CAR, 12 by ultrasound and 13 by CT, at two days to four years following decannulation with a median of three months (Table 1, Figure 1). Imaging was obtained in 15 of 25 patients (60%) for other clinical reasons other than evaluating the carotid artery. In 9 of 25 patients (36%), imaging was obtained for vascular mapping prior to planned procedure or due to risk of decompensating and requiring ECMO. Only one patient had a dedicated ultrasound specifically evaluating the carotid artery for thrombus due to stroke. Twenty-one out of 25 (84%) patients had unobstructed normal carotid arteries. One patient had 50% stenosis of the carotid artery, and the remaining three had complete occlusion of the carotid artery. The three patients with complete occlusion included a 13-year-old with a seven-day ECMO duration, a two-week-old with a seven-day ECMO duration, and a three-month-old with a 17-day ECMO duration, in whom the vessel was noted to be of poor tissue integrity at the time of reconstruction.
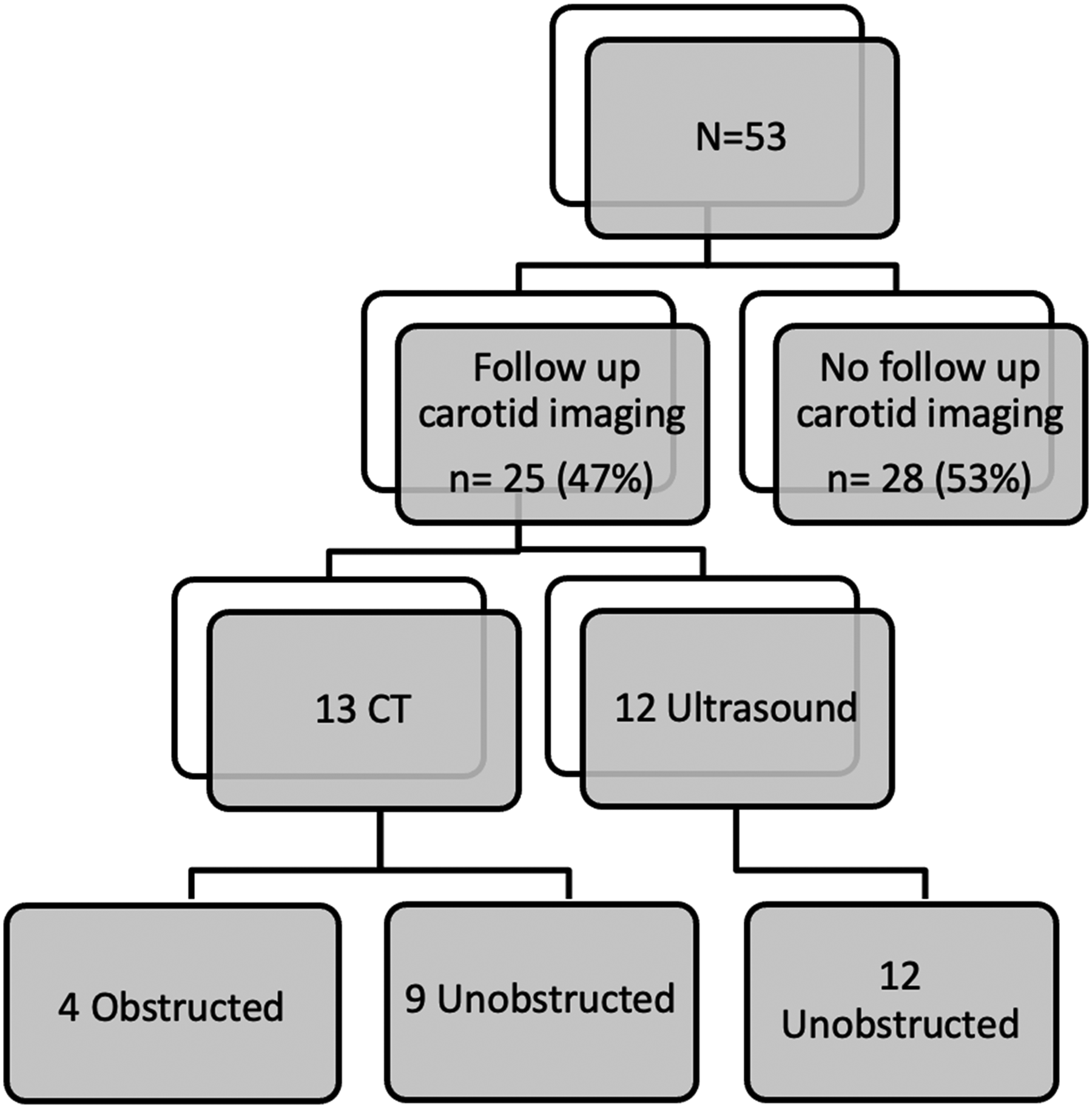
Children with follow-up carotid artery imaging following carotid artery reconstruction (CAR) and extracorporeal membrane oxygenation (ECMO) decannulation. CT, computed tomography.
A total of 33 children had at least one head imaging study after CAR and ECMO decannulation, and 14 of them had follow-up imaging at a later date. Of the 33 children with head imaging, 19 (58%) had head CT, 10 (30%) children had MRI, and 4 (12%) had head ultrasound. Timing between the first head imaging and ECMO decannulation varied from the same day as decannulation to three years and nine months depending on the clinical scenario for obtaining head imaging. The median time from decannulation to head imaging was four days, with 22 out of 34 (65%) patients receiving imaging within the first week. Nineteen children of 33 (58%) had acute clinical indications for head imaging such as focal neurological symptoms concerning for stroke or intracranial hemorrhage. Five of 33 children (15%) had head imaging to follow-up known ischemic strokes or intracranial hemorrhage noted previously on EMCO, and the remaining nine children (27%) were asymptomatic with routine follow-up imaging given their history of ECMO or cardiac arrest. Of the 14 children who had subsequent head imaging, we looked at their most recent imaging and noted 10 (71%) had acute neurological symptoms prompting imaging. The time from decannulation to the most recent neurological imaging ranged vastly from three days to eight years with a median duration of 7.7 months.
In total, 11 children in this cohort were noted to have new focal infarcts, seven identified from the initial post decannulation imaging and four who had normal head imaging initially but were later found to have infarcts (see Table 3 for further clinical characteristic). In terms of lateralization of the infarct, seven were right-sided, two were left-sided, and two were bilateral. Of the seven children who were diagnosed on the first head imaging post decannulation, one had no imaging during ECMO and the other six had CT or head ultrasound done during ECMO and MRI following decannulation. The difference in study modality could impact the sensitivity of stroke diagnosis. Of the four children who had a new diagnosis of focal infarcts on later imaging, all these patients were on a VAD (patients 8-11 in Figure 3).
Three patients did not receive CAR. Two out of the three had longer than average ECMO duration of 21 and 25 days, and the surgeon noted in one of those patients that the vessel was extensively damaged. The third patient was on ECMO for five days, but had concern for infection at the cannulation site, thus the right internal jugular and right common carotid artery were clipped distally. Regarding head imaging, one patient had no imaging, one had normal imaging, and one had a preexisting left posterior cerebral artery (PCA) infarct prior to ECMO, later developing a right PCA infarct due to severe stenosis three years following decannulation.
As mentioned above, four children had an obstructed carotid artery. Regarding their neurological findings, one had a right PCA infarct on CT, one had a normal head CT, and one had diffuse hypoxic-ischemic encephalopathy on MRI. All three of these patients had head imaging performed after the known carotid artery occlusion. The fourth patient had a normal head ultrasound that was done prior to discovery of the occluded carotid artery, and no head imaging after.
Discussion
In this retrospective analysis of children with congenital and acquired heart disease who underwent VA-ECMO cannulation, 84% (21/25) of the imaged reconstructed carotid arteries following decannulation remained unobstructed. Only three patients did not undergo CAR due to longer ECMO runs with poor vessel integrity or concern for infection at the cannulation site. To our knowledge, this is the largest cohort to date of specifically cardiac patients who have had CAR following ECMO decannulation.
Our findings are consistent with some of the current literature in the general pediatric population, which has reported a wide range of carotid artery patency rates after CAR. A recent systematic review of clinical outcomes after carotid artery ligation versus CAR, which included 80 studies, showed an overall carotid arterypatency rate of 44% to 100%. 9 However, when specifically looking at the subset of studies evaluating noncomparative clinical outcomes after CAR, the patency rate was higher at 71% to 100%. 9 The review did not specify whether patency rates differed based on the surgical specialty performing the CAR (eg, general vs cardiothoracic surgeons). Cardiothoracic surgeons, with their specialized skillset and greater experience performing vascular anastomoses, may achieve higher patency rates. Importantly, only two of these 12 noncomparative studies included patients with CHD, emphasizing the need for more research focused specifically on this patient population. 9 Like the current study, the review showed that the timing of carotid artery imaging following decannulation ranged vastly from immediately post-decannulation to 11 years after. 9 Another recent systematic review in 2023 revealed the carotid artery patency rate was also favorable at 78.6%. 14 Although 9 of 15 studies demonstrated patency rates greater than 90%, there was significant variability ranging from 28% to 100%. 14 The authors attributed the variability to surgeon experience or selection bias as patency was increased with shorter ECMO duration, so improved rates could be secondary to choosing candidates for reconstruction who were more likely to have positive outcomes. 14 Interestingly, the largest series in this review had 51 patients, which is comparable to the number of patients in our study.2,14 However, this study excluded patients with CHD. 2
Regarding neurologic outcomes following CAR, we found that 11 of 33 children who had head imaging following decannulation had new findings of focal ischemia. However, one child did not have imaging during ECMO, six had CT or head US during ECMO, and MRI following decannulation, so it is unclear whether these were new findings after decannulation, or findings identified by more sensitive imaging. Additionally, four patients had infarcts after transitioning to a VAD so it is unclear whether the infarct is related to the VAD and underlying illness or CAR. The decision to ligate or repair the right carotid artery during ECMO has been influenced by concerns about potential neurological complications due to ischemia to the ligated right side resulting in increased compensatory flow to the left side. Early studies from the 1980s with small patient cohorts initially showed concerns for lateralizing brain injury following right carotid artery ligation after ECMO.15,16 Infants were noted to have varying degrees of right hemispheric brain injury with left neuromotor abnormalities and EEG showing increased incidence of slowing and attenuation over the right hemisphere. 15 However, recent systematic reviews have not found any definitive laterality to brain lesions, with many finding bilateral lesions outnumber unilateral lesions.9,14 Across all studies evaluating cross-sectional imaging and functional neurologic testing, there were no differences in ischemic or hemorrhagic strokes, developmental delay, or intelligence quotient scores between children with carotid artery ligation or CAR.9,14 Overall, neurological outcomes are influenced by various factors, and distinguishing the specific contributions of carotid artery ligation, CAR, and ECMO-related complications can be challenging.
Although there is no rigorous evidence at this time to suggest that children with CHD may benefit from selective CAR following VA-ECMO, there are many reasons why this may be beneficial. This subgroup of patients may have anomalies such as hypoplastic or interrupted aortic arch where the contralateral carotid artery would have to be manipulated during surgical repair, or the right carotid artery might be used for procedures such as a Blalock-Taussig-Thomas shunt in patients who need a source of pulmonary blood flow. 9 This would call for an intact right carotid artery and make it crucial for it to be reconstructed following VA-ECMO decannulation. Additionally, cardiac patients tend to have shorter duration of ECMO making it more technically feasible for CAR with good patency rates. For example, Sarioglu et al found that only 50% of neonates were able to undergo CAR via end-to-end anastomosis based on the inflammatory changes of the vessel at the time of decannulation. 6 The time on ECMO for the repair group was approximately 6 days versus 12 days for the ligation group. 6 In addition, ligation of the artery does not allow for a second ECMO run using the same cannulation site. In one study using ELSO data, 3.2% of children requiring ECMO had more than one ECMO course. 17 The authors found that second ECMO courses in children can achieve survival comparable to the first course, but more often require central cannulation, and reusing cannulation sites for a second ECMO course is associated with fewer total complications than cannulating at new sites. 17 Children with heart disease are more likely to require a second course of ECMO. One large single center study found that 4.6% of children required a second course of ECMO and 76.9% of those patients had underlying cardiac pathologies. 18
There are some important limitations to our study. First, this is a retrospective review at a single center with a small sample size. There is variable follow-up time with nearly one-half of patients not having follow-up carotid artery imaging. If all patients underwent follow-up imaging, this could change the percentage of patients who had unobstructed carotid arteries. In addition, with the variable follow-up time from two days to four years and a median duration of three months, it is unclear whether the arteries will remain patent if the follow-up time was longer. Finally, because of the retrospective nature of the study, timing, and variability of head imaging modality, we are unable to determine if neurological findings were secondary to carotid artery strategy utilized or other ECMO complications. Additionally, the study includes a high proportion of patients on VADs which can confound the etiology for the infarcts. To answer these questions, prospective studies with prespecified time points of outcome measures and long-term follow-up are required.
Conclusion
In summary, CAR following VA-ECMO decannulation in children with congenital and acquired heart disease show early patency in those who received carotid artery imaging. Among patients with head imaging, there were 11 patients with new infarction diagnosed, although there are multiple confounding factors, and we are unable to determine whether these infarctions were related to CAR or the ECMO/VAD course. In children with heart disease requiring ECMO, CAR can be considered except in cases where the surgeons are concerned about the tissue integrity of the vessel or risk for infection at the cannulation site. However, these data should be viewed as hypothesis generating and not confirmatory regarding the superiority of this approach. Currently, there is significant variation in practice, and establishing uniform guidelines for the management of cervical vessels in children following ECMO decannulation will aid our understanding of the impact of carotid artery strategy on vascular and neurologic outcomes.
Supplemental Material
sj-docx-1-pch-10.1177_21501351251338830 - Supplemental material for Favorable Vessel Patency Following Carotid Artery Reconstruction During Extracorporeal Membrane Oxygenation Decannulation in Children With Congenital Heart Disease
Supplemental material, sj-docx-1-pch-10.1177_21501351251338830 for Favorable Vessel Patency Following Carotid Artery Reconstruction During Extracorporeal Membrane Oxygenation Decannulation in Children With Congenital Heart Disease by Ariya Chau, Shiraz A. Maskatia, Basma Albuliwi, Elisabeth Martin and Kathleen R. Ryan in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.