
Abstract
Objectives
Review our clinical experience with eight patients at the University of Florida undergoing En-bloc combined heart+liver transplantation (ECH + LTX).
Methods
Continuous variables are reported as median (interquartile range = IQR) and categorical variables are reported as N (%).
Results
Eight patients underwent ECH + LTX between August 2020 and May 2023 at the University of Florida, with triple heart+liver+kidney transplantation performed in 2/8 = 25%. Median age at ECH + LTX was 47.34 years (IQR = 33.66-53.37), and all eight patients were >18 years of age. Six out of eight patients (75%) had congenital heart disease (CHD): one had biventricular CHD and five had functionally univentricular circulation and Fontan failure. Two out of eight patients (25%) had structurally normal hearts and acquired heart disease: one patient with hemochromatosis and combined cardiac and hepatic failure with nonischemic restrictive cardiomyopathy and one patient with nonischemic cardiomyopathy and alcoholic cirrhosis. Median wait list time was 93 days (IQR = 27.50-176.25). Three patients (3/8 = 37.5%) were supported with an intra-aortic balloon pump prior to ECH + LTX, and two of these three patients were subsequently also supported with extracorporeal membrane oxygenation secondary to progressive decompensation prior to ECH + LTX. Median hospital length of stay was 147 days. Median posttransplant length of stay was of 29 days. Seven of eight patients survived ECH + LTX and are alive today. One patient died two days after ECH + LTX. Mean length of follow-up after ECH + LTX of seven surviving patients (years) is 3.60 ± 0.38 (median = 3.79, IQR = 3.05-4.38, range = 1.91-4.64).
Conclusion
En-bloc heart-liver transplantation is an effective treatment option for patients with combined heart and liver failure.
Keywords
Introduction
For patients with end-stage combined cardiac and hepatic failure, combined heart+liver transplantation remains the only suitable option for long-term survival. There are a limited number of such procedures performed annually in the United States. From January 1988 to June 2023, a total of only 531 combined heart+liver transplants were performed in the United States. 1 However, the indications and strategies of management for combined heart+liver transplantation are evolving. Patients with end-stage hepatic dysfunction and either end-stage acquired heart disease or end-stage congenital heart disease (CHD) are candidates for combined heart+liver transplantation. A variety of disease processes (eg, alcohol use disorder, CHD, hemochromatosis, hepatitis C, metabolic syndrome) can devolve to combined cardiac and pulmonary failure, including those associated with both biventricular circulation and those associated with univentricular circulation.
Among patients with functionally univentricular CHD, it is currently estimated that over 70 000 patients worldwide have undergone the Fontan operation, with over one-third of these patients living in the United States.2,3 Importantly, it is estimated that most of these patients living with Fontan circulation are under the age of 25. 2 As this vulnerable population ages, these patients are at risk to develop cardiac-related congestive hepatopathy, which can eventually cause Fontan-associated liver disease (FALD).
One of the challenges of caring for patients with FALD is predicting which patients with Fontan failure and FALD will experience stabilization or regression of their hepatic fibrosis after cardiac transplantation versus which patients with Fontan failure and FALD will experience further hepatic decompensation after cardiac transplantation. It is known that combined heart+liver transplantation is associated with satisfactory outcomes and mitigation of the need for subsequent liver transplantation in patients with Fontan failure and FALD.4,5
Two technical approaches to combined heart+liver transplantation are sequential combined heart+liver transplantation and en-bloc combined heart+liver transplantation (ECH + LTX). In 2020, the heart and liver transplant teams at University of Florida established a program of ECH + LTX. The purpose of this study is to review our clinical experience in all eight patients at the University of Florida who underwent ECH + LTX.
Methods
Patient Selection
At the University of Florida, patients with combined end-stage cardiac and hepatic failure are reviewed at a multidisciplinary conference that includes cardiac surgeons, liver transplant surgeons, cardiologists, hepatologists, nurses, social workers, and administrators. The decision to proceed with ECH + LTX is made on a case-by-case basis.
Surgical Technique
Our surgical technique for combined en-bloc heart and liver procurement, with preservation of the inferior caval venous connection between the donor heart and the donor liver, has been previously described. 6 Similarly, our surgical technique for combined en-bloc heart and liver transplantation has been previously described. 7
Statistics, Database, and Institutional Review Board
This analysis includes all patients undergoing ECH + LTX at the University of Florida. These eight patients underwent ECH + LTX between August 2020 and May 2023. Patients who underwent multiorgan transplantation that did not involve an ECH + LTX were excluded. Statistical analysis included univariable descriptive statistics. Data reported include the following descriptive statistics: count (n), median, interquartile range [Q1-Q3], and range (minimum-maximum). All statistical examinations were conducted utilizing Microsoft Excel 2021.
Data were sourced from a registry and database (CardioAccess Incorporated, http://www.cardioaccess.com) that uses software certified by The Society of Thoracic Surgeons Congenital Heart Surgery Database and has been prospectively maintained on all patients undergoing pediatric and/or congenital cardiac surgery at the University of Florida. This study was approved by the University of Florida Institutional Review Board with a waiver of the need for consent: IRB202101584.
Results
Study Population and Demographics
In this series of eight patients who underwent ECH + LTX at the University of Florida, the median age at transplant was 47.34 years (IQR = 33.66-53.37), and all patients were over the age of 18 at time of transplant. A total of 5 of 8 (62.5%) patients were male and median weight at transplant was 73.75 kg (IQR = 65.70-81.15). Congenital heart disease was the most common cardiac diagnosis: 6 of 8 patients (75%) had CHD, and five of these six patients (83.3%) had functionally univentricular circulation with Fontan failure. In the two patients with acquired heart disease, one patient had hemochromatosis with combined cardiac and hepatic failure as well as nonischemic restrictive cardiomyopathy, and the other patient had nonischemic cardiomyopathy as well as alcoholic cirrhosis. The fundamental diagnosis, cardiac diagnosis, hepatic diagnosis, and results of the pretransplant liver biopsy for all eight patients are documented in Table 1.
After the completion of this current analysis of the eight patients who underwent ECH + LTX at the University of Florida, a ninth patient underwent successful ECH + LTX at the University of Florida in August 2024 and is not included in this series. This patient had combined cardiac and hepatic failure with complex biventricular CHD (status post repair of complete atrioventricular septal defect, status post right atrioventricular valvar replacement, status post epicardial pacemaker placement, status post right transcatheter tricuspid valve replacement, cirrhosis with end-stage liver failure, autism, and hypothyroidism); this patient is currently alive and well today, as of March 30, 2025, seven months after ECH + LTX.
The Fundamental Diagnosis, Cardiac Diagnosis, Hepatic Diagnosis, and Results of the Pretransplant Liver Biopsy for All Eight Patients.
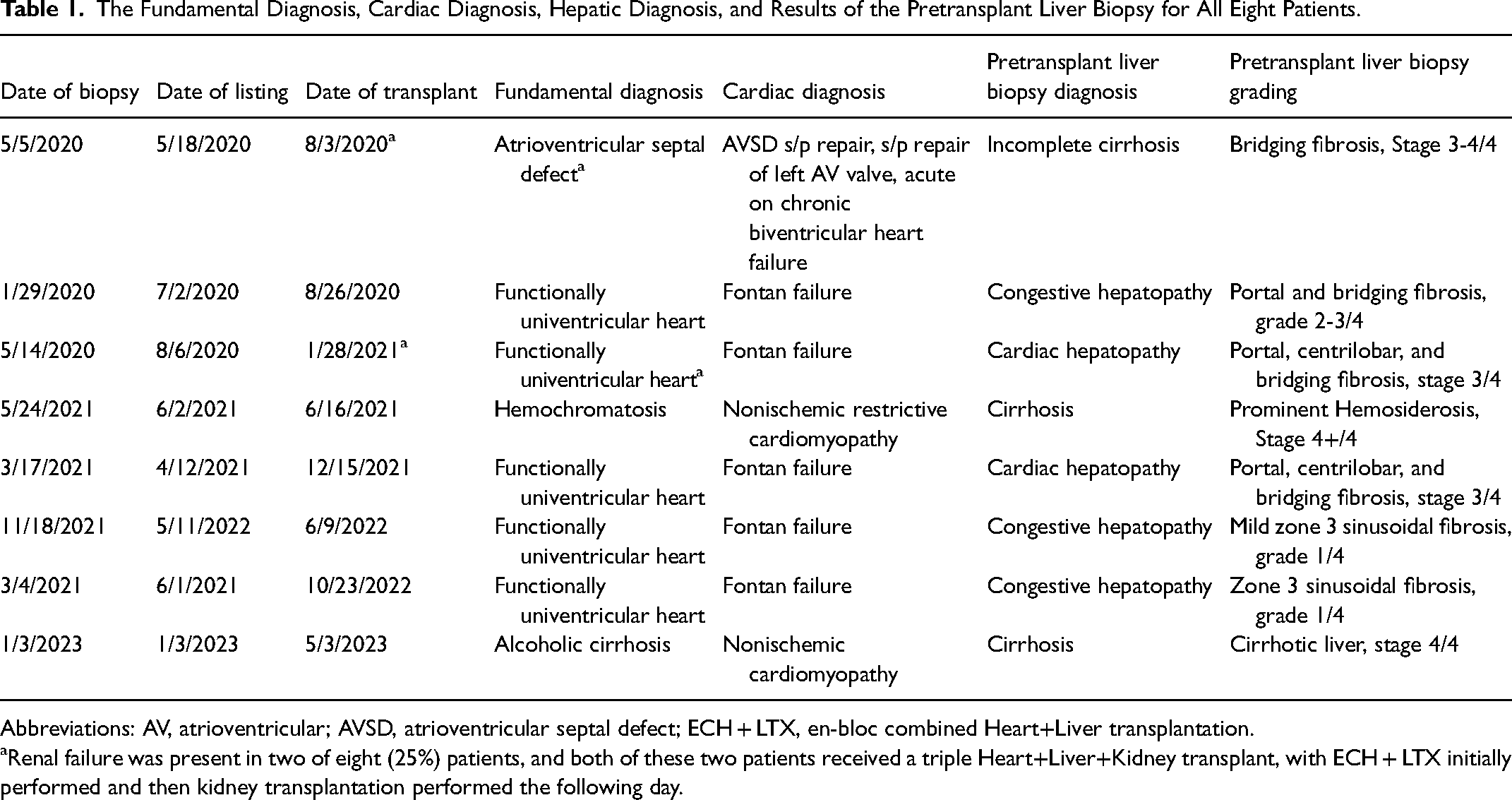
Abbreviations: AV, atrioventricular; AVSD, atrioventricular septal defect; ECH + LTX, en-bloc combined Heart+Liver transplantation.
Renal failure was present in two of eight (25%) patients, and both of these two patients received a triple Heart+Liver+Kidney transplant, with ECH + LTX initially performed and then kidney transplantation performed the following day.
Pretransplant Characteristics
Pretransplant characteristics are reported in Table 2. A total of 6 of 8 (75%) patients had undergone prior cardiac surgery, with a median of three prior cardiac surgeries. Median waitlist time was 93 days (IQR = 27.5-176.25). Cirrhosis was diagnosed in 3 of 8 (37.5%) patients. The hepatic diagnoses of the five remaining patients are listed in Table 1; all five of these patients had biopsy proven advanced hepatopathy, with additional details provided in Table 1.
Pretransplant Variables of Patients Undergoing Combined En-Bloc Heart+Liver Transplantation.
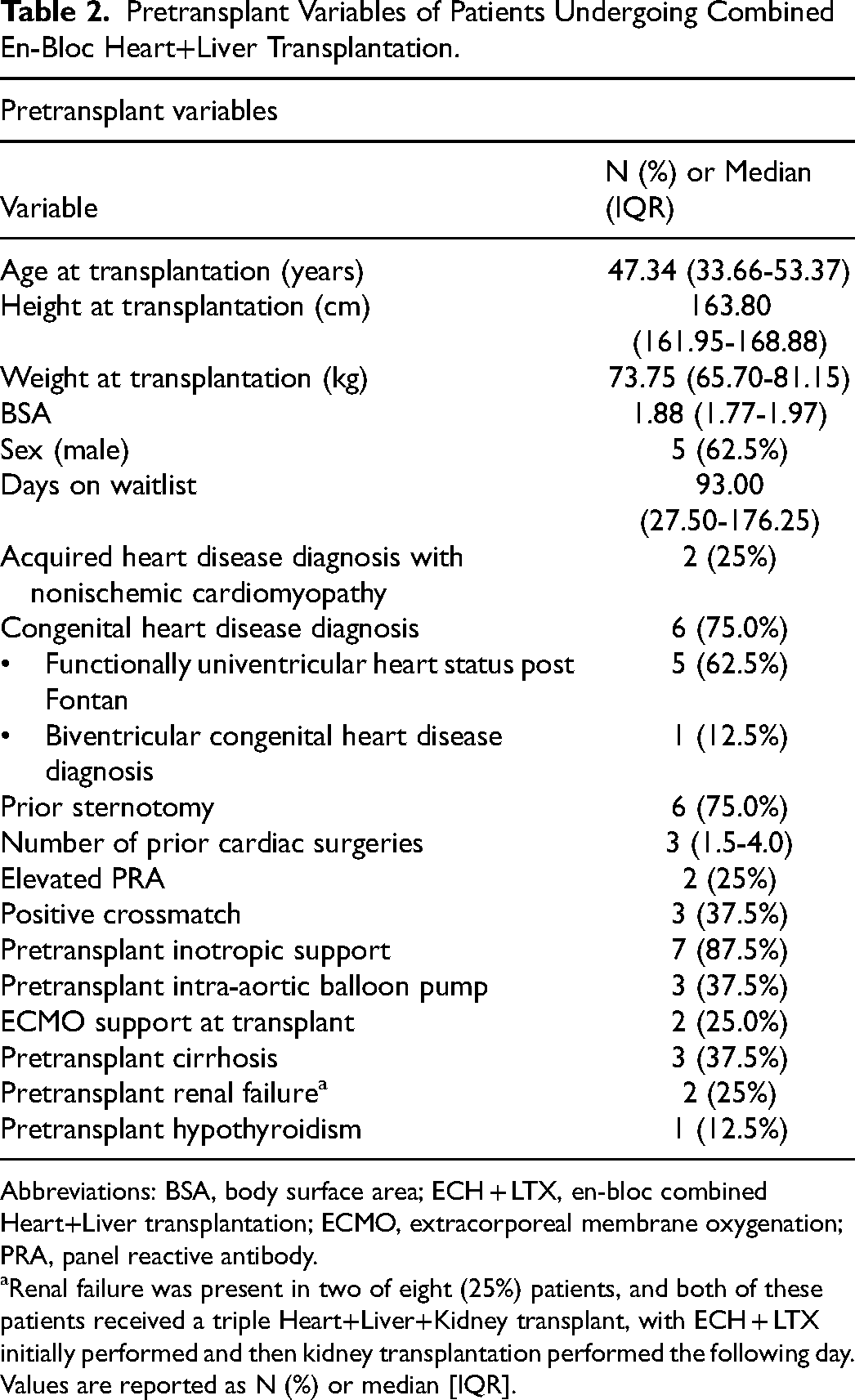
Abbreviations: BSA, body surface area; ECH + LTX, en-bloc combined Heart+Liver transplantation; ECMO, extracorporeal membrane oxygenation; PRA, panel reactive antibody.
Renal failure was present in two of eight (25%) patients, and both of these patients received a triple Heart+Liver+Kidney transplant, with ECH + LTX initially performed and then kidney transplantation performed the following day. Values are reported as N (%) or median [IQR].
Renal failure was present in 2 of 8 (25%) patients, and both of these patients received a triple Heart+Liver+Kidney transplant, with ECH + LTX initially performed and then kidney transplantation performed the following day. Almost all patients (7/8 = 87.5%) were supported with intravenous inotropes prior to and at the time of ECH + LTX. Three patients (3/8 = 37.5%) were supported with an intra-aortic balloon pump (IABP) prior to ECH + LTX, and two of these three patients were subsequently also supported with extracorporeal membrane oxygenation (ECMO) secondary to progressive decompensation prior to ECH + LTX. Immunological burden was reasonable considering prior sensitization events, with 2 of 8 (25%) patients with a panel reactive antibody (PRA) value of greater than 10% and 3 of 8 (37.5%) patients having a positive crossmatch.
Intraoperative Characteristics
Intraoperative characteristics are reported in Table 3. Median cardiac donor ischemic time was 174.5 min (IQR = 144.5-186), median bypass time was 154.5 min (IQR = 119.25-242.25), and median cross clamp time was 66 min (IQR = 54.25-85.5). Median minimum temperature was 23.8 °C (IQR = 21.15-29.65).
Intraoperative Variables of Patients Undergoing Combined En-Bloc Heart+Liver Transplantation.a
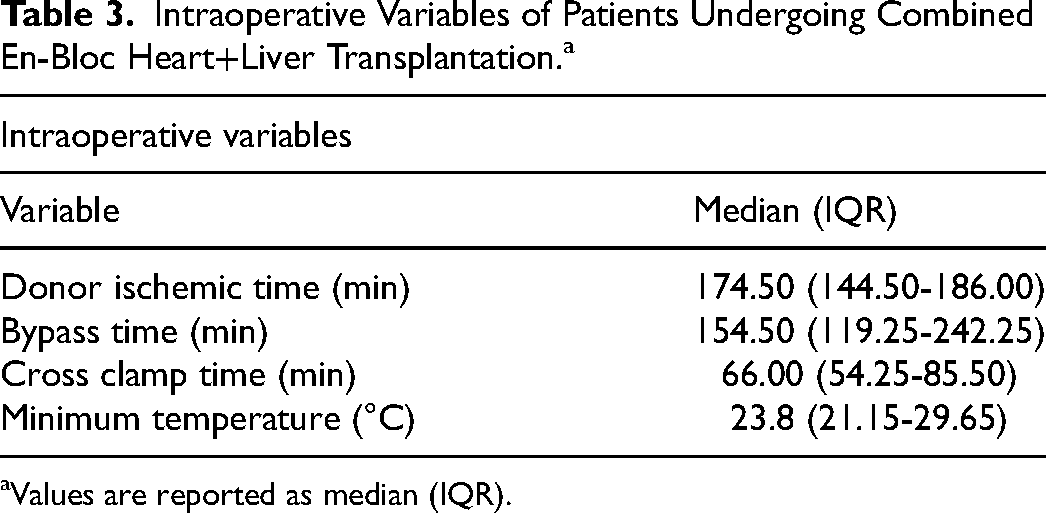
Values are reported as median (IQR).
Posttransplant Outcomes
Posttransplant outcomes are reported in Table 4. Patients had a median posttransplant stay of 29 days (IQR = 21.75-42). One patient died two days after ECH + LTX secondary to severe coagulopathy, multisystem organ dysfunction, and disseminated intravascular coagulation. Of the eight patients who underwent ECH + LTX, 7 of 8 (87.5%) were discharged alive, with all seven of these patients alive at last follow up, with mean length of follow-up after ECH + LTX of seven surviving patients (years) of 3.60 ± 0.38 (median = 3.79, IQR = 3.05-4.38, range = 1.91-4.64) as of March 30, 2025.
Posttransplant Outcomes of Patients Undergoing Combined En-Bloc Heart+Liver Transplantation.a
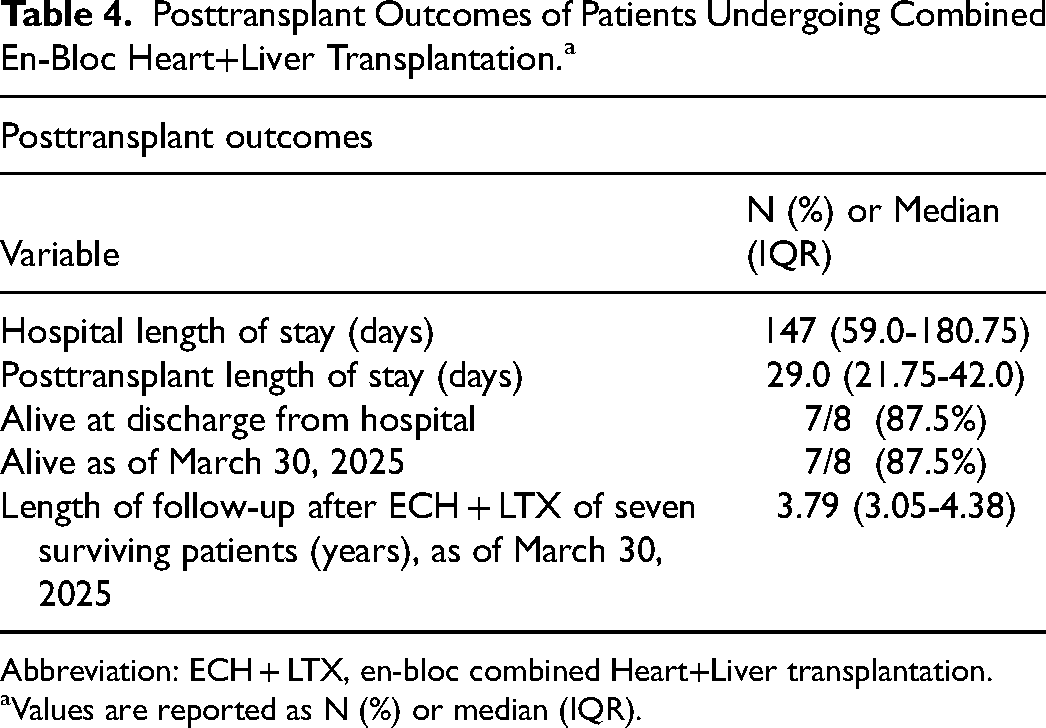
Abbreviation: ECH + LTX, en-bloc combined Heart+Liver transplantation.
Values are reported as N (%) or median (IQR).
Discussion
Combined heart+liver transplantation can be done with sequential transplantation (with either transplantation of the heart first and then the liver or transplantation of the liver first and then the heart) or the simultaneous transplantation of both organs with ECH + LTX. Our experience with our initial eight patients undergoing ECH + LTX tells us that this technique is safe and can be lifesaving for the most challenging of patients. Cardiac and hepatic ischemic time can be minimized with the simultaneous transplantation of both organs with ECH + LTX.
Previously Published Series of Combined Heart+Liver Transplantation
Although ECH + LTX is an uncommon operation performed at few centers, previous single center analysis have been published.8–13 An early study published in 2012 from Stanford University described their experience with three pediatric patients undergoing ECH + LTX; this analysis reported 100% patient and graft survival at one year and no operative complications in any of the three patients. 8 A more recent 2019 study looked at adolescents and young adults (median age 20.7, range 14.2-41.3 years) specifically with failing Fontan physiology (n = 9) and reported a one-year survival of 100%. 9 Meanwhile, a larger study (n = 20) reported in 2021 (7-56 years of age; biventricular diagnoses were idiopathic cardiomyopathy, previously repaired Ebstein malformation of tricuspid valve, previously repaired double outlet right ventricle, previously repaired Tetralogy of Fallot, and hypoplastic left heart syndrome palliated to Fontan circulation and later converted to biventricular circulation with mechanical aortic valve placement; all remaining patients had single ventricle physiology palliated to Fontan circulation) showed similar outcomes with only one early death and two late deaths. 10 Also in 2021, Brozzi and colleagues reported a series of five patients who underwent ECH + LTX (mean recipient age = 43 years, range = 26-63); hospital survival was 80% (one patient died on postoperative day 55 due to fungal sepsis) and among patients discharged from hospital, one-year survival was 100%, with no evidence of rejection or infectious complications. 12 Finally, a study of pediatric patients (n = 18) reported in 2024 documented a one year survival of 89%. 13
Isolated Heart Transplantation or Combined Heart+Liver Transplantation
The decision of whether to list patients for isolated heart transplantation or combined heart+liver transplantation is largely an institutional decision, with no universally accepted guidelines available for centers to follow. A standard requirement for consideration for combined heart+liver transplantation is the diagnosis of both cardiac failure and hepatic failure. 8 Other centers use specified markers of liver failure such as severe hepatic fibrosis or portal hypertension. 13 However, indications can vary slightly from center to center, and a need exists for standardization and harmony of these guidelines. Larger multi-institutional studies need to be conducted to identify patients who are at high risk for hepatic failure after an isolated heart transplant and who would have otherwise benefitted from combined heart+liver transplantation. These studies will serve as a clinical basis for teams to make the best decision for each patient. In the interim, at the University of Florida, patients are evaluated for potential ECH + LTX on an individual basis, with collaborative input from multiple care teams.
Combined Heart+Liver Transplantation in the Setting of Fontan Failure
As our series shows, ECH + LTX can be an effective therapy for a variety of conditions that result in combined cardiac and hepatic failure. However, by far the most common indication in our cohort was combined cardiac and hepatic failure secondary to Fontan failure, an indication that will likely only increase in prevalence given the growing population of functionally univentricular adults with CHD.14,15 The mechanism that Fontan failure leads to hepatic failure is related to chronic hepatic congestion secondary to the elevated venous pressures that are associated with Fontan circulation. 16 These patients with failing Fontan physiology can also present with additional comorbidities from their physiological state, such as protein losing enteropathy, plastic bronchitis, and kidney disease, which in some cases may be severe enough to necessitate kidney transplantation as well. 17 These patients with failing Fontan often present to centers with a challenging decision: whether to proceed with a ECH + LTX, or instead list patients for isolated heart transplants and hope improved cardiac function and circulation resolves hepatic congestion. In patients with less significant liver disease, isolated cardiac transplantation is often the preferred option, although the long-term fate of the liver in these patients is debatable.18,19 In 2023, Lewis and colleagues reported a retrospective cohort study of adult Fontan patients who underwent HT or CHLT across 15 centers. 20 These investigators concluded that “Higher FALD scores were associated with posttransplant mortality. Although prospective confirmation of our findings is necessary, compared with heart transplant alone, combined heart+liver transplant recipients were older with higher FALD scores, but had similar survival overall and superior survival in patients with a FALD score ≥2.” 20 Clearly, the role of heart transplant alone versus combined heart+liver transplant is evolving, with important variation in practice across centers, especially in the setting of failing Fontan physiology. Thus, the experience of programs with ECH + LTX at large, as well as specifically with patients with failing Fontan physiology, represents valuable information to be added to the literature.
Sequential Combined Heart+Liver Transplantation Versus Simultaneous ECH + LTX
Uniform agreement does not exist regarding the decision of whether to perform combined heart+liver transplantation with (1) sequential transplantation (with either transplantation of the heart first and then the liver or transplantation of the liver first and then the heart) or (2) the simultaneous transplantation of both organs with ECH + LTX. Sequential transplantation may involve transplanting the heart first or the liver first. Heart first sequential combined heart+liver transplantation may be preferred by some in order to minimize cardiac ischemic time, given that the heart has less tolerance of ischemia than the liver. Liver first sequential combined heart+liver transplantation involves implanting the liver before the heart to allow liver perfusion and removal of donor-specific antibodies for sensitized patients. (Some believe that ECH + LTX may not allow enough liver circulation to accomplish antibody removal.) The Mayo Clinic reported a total of seven patients (age 43 ± 7 years, 86% women) with high allosensitization (median calculated panel reactive antibody = 77%) who underwent heart-after-liver transplantation. 11 These authors concluded that “A heart-after-liver transplantation protocol enables successful transplantation via near-elimination of donor specific antibodies (DSA) and is effective in preventing adverse immunological outcomes in highly sensitized patients listed for combined heart-liver transplantation.” 11
At the University of Florida, we utilize ECH + LTX because ECH + LTX facilitates shorter ischemic times of both grafts in comparison with sequential heart+liver transplantation. 10 Furthermore, en-bloc implantation also simplifies the transplant in patients with complex venous anatomy such as heterotaxy, and ECH + LTX can be performed in patients with dextrocardia or levocardia, irrespective of the side of inferior caval vein or superior caval vein. 10
Triple Heart+Liver+Kidney Transplantation
Our current series is eight consecutive patients undergoing ECH + LTX from 2020 to 2023. As mentioned previously, two of these patients underwent triple organ heart+liver+kidney transplantation. Both of these patients who underwent triple organ heart+liver+kidney transplantation had a diagnosis of CHD; however, only one of these patients had functionally univentricular physiology after the Fontan operation, while the other had biventricular CHD. Triple organ heart+liver+kidney transplantation is a rarely performed operation; thus, the experience of programs with this rare operation also represents valuable information to be added to the literature.
Immunology
One of the more surprising findings in our study was the relatively low immunological burden in these patients, with only 2/8 (25% presenting to transplant with elevated PRA >10%). This finding is despite a plethora of sensitization events in the cohort, with the average heart+liver recipient in our series undergoing three prior cardiac surgeries. Our protocol for desensitization of sensitized patients has been previously published. 21 Whether elevated PRA is a risk factor for heart+liver transplant remains a question of significance, given the role of elevated PRA in rejection in the setting of isolated cardiac transplantation; however, recent findings suggest an immunoprotective role of the liver allograft.5,11
Mechanical Circulatory Support
Mechanical circulatory support (MCS) was utilized as a bridge to transplant in 3 of 8 (37.5%) of our patients. All three of these patients had an IABP placed, with two of the three patients transitioned to ECMO prior to ECH + LTX. Our utilization of IABP and ECMO as bridge-to-transplantation for combined heart+liver transplantation contrasts with the recently published experience of another center that reported postoperative ECMO use but made no mention of pretransplant bridge to transplantation. 10 The use of MCS in this challenging population can buy valuable time for critically ill patients while mitigating waitlist concerns for multiple organs. Overall, early results from our cohort are extremely promising. While one patient died in hospital after their ECH + LTX, the other seven have remained well, with a median survival of 3.79 years as of March 30, 2025.
Limitations
Our study possesses several limitations that are important to address. Given the relative rarity of ECH + LTX, our series contains only eight patients in a three-year span, making it difficult to draw generalizable conclusions from our data due to center variability. While we are able to highlight trends and interesting findings in this cohort, given such a small sample size, we cannot say whether our experience with excellent early survival and relative lack of immunosensitization is shared by other centers or is to be expected. Additionally, given our small sample size and only one death in the cohort, our study lacks the statistical power to perform detailed modeling for risk factors. Nevertheless, the reporting of these outcomes serves to provide another contemporary datapoint on the utility and promising outcomes of ECH + LTX.
Value of this Analysis
Our analysis provides additional data about the characteristics and outcomes of patients with combined cardiac and hepatic failure who are treated with the rare operation of ECH + LTX. Our experience also demonstrates the possibility of achieving excellent outcomes with the utilization MCS as bridge-to-transplantation for ECH + LTX. Our institutional experience supports the utilization of ECH + LTX for selected patients with combined hepatic and cardiac failure. More data are needed to determine the ultimate advantages of ECH + LTX versus sequential combined heart+liver transplantation. Unfortunately, the UNOS OPTN database does not allow differentiation of en-bloc versus sequential combined heart+liver transplantation. In the future, we hope that the OPTN database adds the collection of these details regarding operative technique so that one can perform a multi-institutional comparison of the characteristics and outcomes of patients undergoing ECH+LTX versus sequential combined heart+liver transplantation. 22
Conclusions
Our experience with ECH + LTX reveals excellent early survival for a variety of indications. ECH + LTX shows promise specifically in the population of patients with failing Fontan circulation and combined cardiac and hepatic failure; therefore, ECH + LTX is a valuable tool to combat end-stage FALD. Due to the rareness of ECH + LTX within the United States and globally, future studies utilizing multi-institutional databases are needed to generate generalizable results with greater statistical power. These future studies can serve to provide information about optimal indications and strategies for ECH + LTX, in order to optimize patient selection and address additional risk factors in this challenging patient population.
Footnotes
Authors’ Note
IRB approval: This study was approved by the Institutional Review Board at the University of Florida and qualified as Exempt: IRB202101584.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.