
Abstract
Introduction
Rheumatic heart disease (RHD) continues to be the leading cause of cardiovascular death globally, with a prevalence of over 40 million across all ages. 1 Indications for cardiac surgery for valvular heart disease in adults are well characterized and published in guideline format.2,3 In contrast, evidence based indications for cardiac surgical intervention for children with isolated aortic regurgitation (AR) remain sparse, particularly limited for those with rheumatic AR. This is likely due to the limited knowledge of the natural history and impact of cardiac surgery in this group.
In contrast to pediatric rheumatic mitral valve surgery, to our knowledge there are no published data describing risk factors for mortality and late left ventricular (LV) dysfunction or rates of late complications for children undergoing surgery for isolated rheumatic aortic valve disease. Studies either include patients with concomitant mitral valve surgery; patients with congenital aortic valve disease; or adults.4–10 Hence, there is little information on which to base recommendations for the timing of cardiac surgery for isolated rheumatic AR in children.
We sought to examine a contemporary cohort of young people in Aotearoa New Zealand (NZ) who had undergone isolated aortic valve surgery for RHD, aiming to determine risk factors for long-term LV dysfunction and survival.
Methods
A single institution retrospective cohort study was undertaken at the Green Lane Paediatric and Congenital Cardiac Services (PCCS), Starship Children's Hospital, Health NZ – Te Whatu Ora, Te Toka Tumai Auckland, NZ. The PCCS is the only provider of cardiology and cardiac surgery to children in the country. Surgery is undertaken at Starship Children's Hospital and cardiology clinics provide follow-up assessment throughout the country. The inclusion criteria were patients with severe rheumatic AR, 18 years of age and under, with surgical intervention between 2000 and 2019. Patients who had concomitant moderate or severe mitral valve regurgitation (MR) or any surgical intervention to the mitral valve were excluded. Patients with a concomitant congenital aortic valve lesion or nonrheumatic valvular heart disease were excluded. Those who were not residents of NZ were excluded. The study received ethical approval from the Auckland Health Research Ethics Committee (AH23874).
Echocardiographic Assessment
Grading of AR was based on echocardiogram. Left ventricular dimensions and volumes were expressed as body surface area (BSA)-adjusted z-score. 11 The PCCS model of care involves echocardiography in the core surgical center, with follow up frequently occurring in local visiting cardiology clinics in the patient's home region (noncore lab sites). We used information from the original echocardiogram reports when available and when the echocardiogram was unavailable for reanalysis from regional follow-up clinics. To justify this methodology, one investigator (SK), a cardiac sonographer with expertise in RHD, reanalyzed a subset of 24 echocardiograms blinded to the original reports.
Left ventricular dysfunction was defined as a LV ejection fraction (LVEF) of <55% or if there was no ejection fraction available then a LV shortening fraction (LVSF) of <27%. Mild LV dysfunction was defined as LVEF 45% to 54% or LVSF 22% to 26%; moderate dysfunction as LVEF 30% to 44% or LVSF 17% to 21%; and severe dysfunction as LVEF <30% or LVSF <16%. 12
Acute Versus Chronic
Acute rheumatic fever (ARF) was diagnosed according to local guidelines. 13 Patients with cardiogenic shock on the basis of severe acute valve disease were determined to have fulminant carditis. Patients who had no features of ARF and presented with features of RHD on echocardiogram were determined to have chronic RHD.
Follow Up
Epidemiological, echocardiographic, surgical, and clinical data were collected from existing PCCS records. Data were collected at three time points—baseline, intermediate, and late. Baseline was defined as immediately prior to the index operation. Intermediate follow up was defined as 6 to 24 months after the index cardiac surgery. Late follow up was defined as greater than two years after surgery. For those with multiple follow-up time points, the most recent clinical review and echocardiogram was used. For those who underwent reoperation, late follow up was defined as the echocardiogram immediately prior to the second surgical event.
Late postoperative complications included death, reoperation, late LV dysfunction, infective endocarditis, thromboembolic events, and arrhythmia. The primary outcomes were death and late LV dysfunction.
Statistical Analysis
Generalized Linear Model was used to investigate continuous outcome of interest between groups. Kruskal-Wallis test was performed for nonparametric variables. Chi-square test for categorical measures was used for differences in counts and percentages. Continuous variables are summarized as mean ± standard deviation for parametric variables, otherwise median and interquartile range.
Survival was measured from the date of the first operation. Cox proportional-hazards regression model was carried out to examine the relationship of the survival distribution of follow-up time to covariates. Kaplan-Meier survival curve was also presented to analyze time to late complications and survival to compare among subset groups.
Statistical analyses were carried out using SAS 9.4 (SAS Institute Inc) and R (R Core Team (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing (URL https://www.R-project.org/).
Results
From 2000 to 2019, 50 individuals under 18 years of age underwent their first surgery for isolated aortic rheumatic valve disease—representing 16% of all young people in NZ undergoing rheumatic valve surgery in that time. Of these 50, 11 were excluded and 39 cases were included for the final analysis (Figure 1). Of the 11 patients excluded, nine were lost to follow up and two were excluded due to non-RHD requiring cardiac surgery prior to their RHD diagnosis. One patient had a congenital bicuspid aortic valve and developed ARF and severe AR with normal aortic valve function on a previous surveillance echocardiogram. Surgical findings (including histology when available) were consistent with RHD. The term “isolated” aortic valve reflects the hemodynamic importance of the aortic valve disease at the time of surgical intervention, notwithstanding that a significant proportion of the cohort had concomitant mild MR.
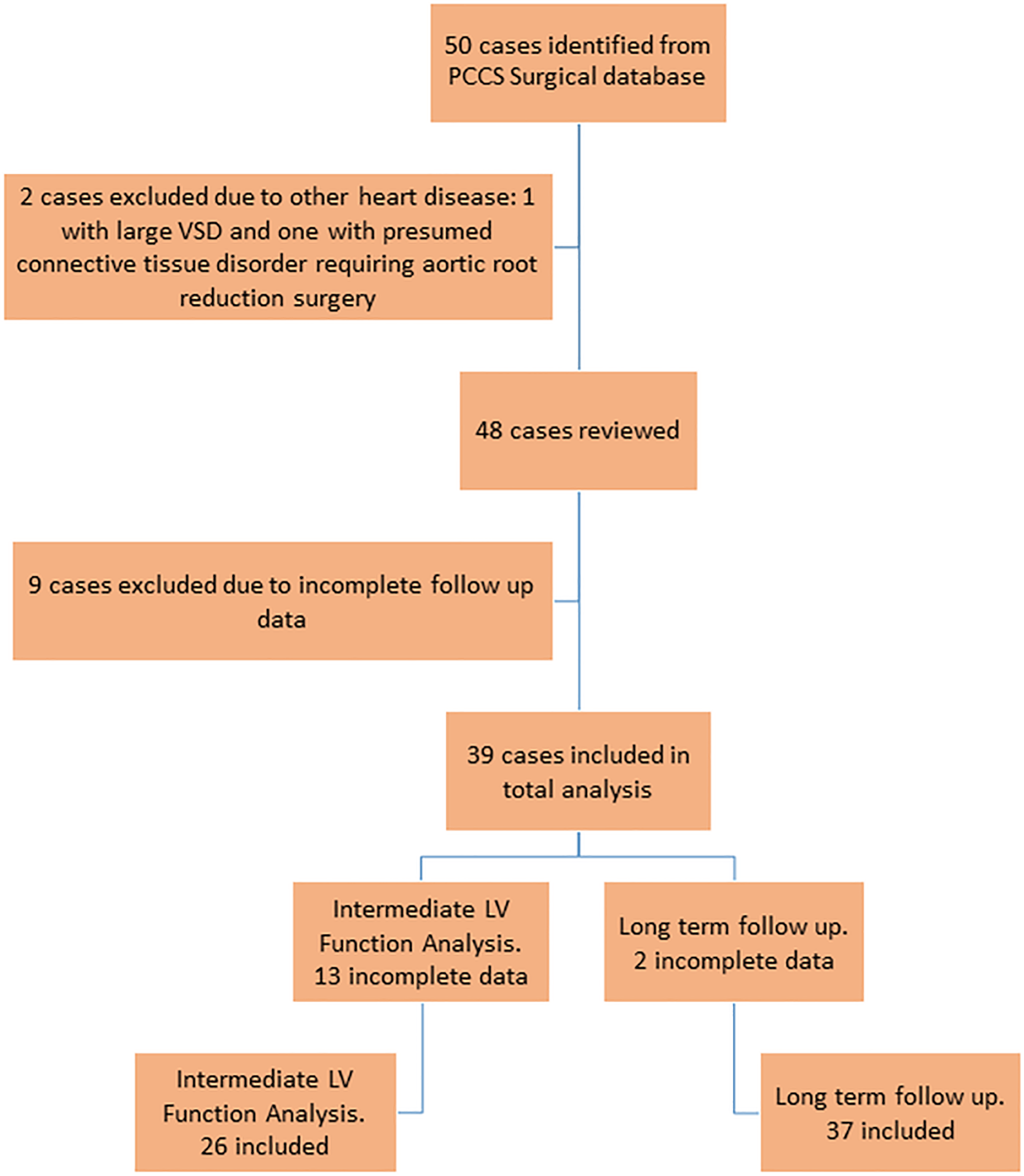
Flowchart demonstrating case selection and follow up.
Indication for surgery was severe AR in all cases. The index surgeries included six valve repairs and 33 valve replacements. Of those, 20 were homograft replacements and 13 were mechanical valves. All cases were discussed at a multidisciplinary surgical conference prior to the operation. Three senior surgeons performed 38/39 index operations. Indication for valve repair was the presence of a single leaflet prolapse. When replacement of the valve was required, homograft valve replacement was the preferred option to avoid the need for anticoagulation. Mechanical valve replacements tended to be chosen in young people with very high body mass index (BMI)—there was concern these children had a higher risk of early reoperation on the aortic root, and the increased afterload may shorten the durability of the homograft. Mechanical valves were also chosen for those with an annulus >28 mm due to a lack of larger homograft valves in our valve bank.
Surgical Techniques—Valve Repair
Valve repairs were performed by two senior surgeons. In five of six cases, the noncoronary cusp prolapsed. Each repair involved an annuloplasty as well as either wedge resection and reapproximation of the free edge of the prolapsing leaflet (n = 5) or plication (n = 1). No leaflet material was added; however, leaflets were debrided at the free edge and hinge points where the leaflet was restricted or thickened.
Echocardiographic Assessment
Twenty-four echocardiograms were reanalyzed with the previously reported measurements compared with the review data. There was strong agreement between the original and repeat measurement (interclass correlation coefficient ranges 0.89-0.99) (Table 1).
Interobserver Reliability on Baseline Echocardiographic Data.
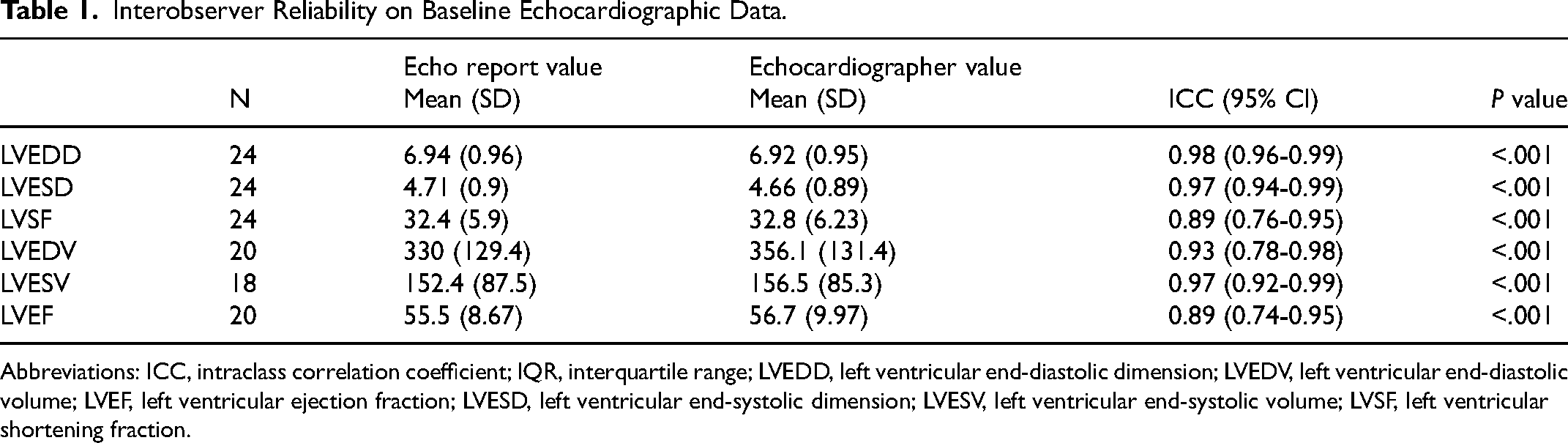
Abbreviations: ICC, intraclass correlation coefficient; IQR, interquartile range; LVEDD, left ventricular end-diastolic dimension; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic dimension; LVESV, left ventricular end-systolic volume; LVSF, left ventricular shortening fraction.
Echocardiographic volumetrics and an ejection fraction were available for 34 of 39 patients for the baseline echocardiogram, and two-dimensional data for 37 of 39 patients. At intermediate follow up, 24 of 26 patients had two-dimensional data, 15 of 26 had volumetric data and 19 of 26 had an ejection fraction available. At late follow up, 30 of 37 patients had two-dimensional data, 22 of 37 had volumetrics, and 34 of 37 had an ejection fraction available.
Baseline patient demographics and echocardiography data are listed in Table 2. The median age was 14 years (range 8-18 years), 28/39 (72%) were male and 37/39 (95%) were Māori or Pacific Peoples. When grouped by type of operation (repair, homograft valve replacement and mechanical valve replacement), there was no significant difference in age or ethnicity, but there were significant differences in patient size parameters with increasing weight, BSA and BMI seen in the homograft group and further increasing in the mechanical valve group (P = .02). There were differences in gender between the three surgical groups (P = .03) with only one female of the 13 patients who underwent mechanical valve replacement.
Baseline Patient Characteristics by Type of Operation.
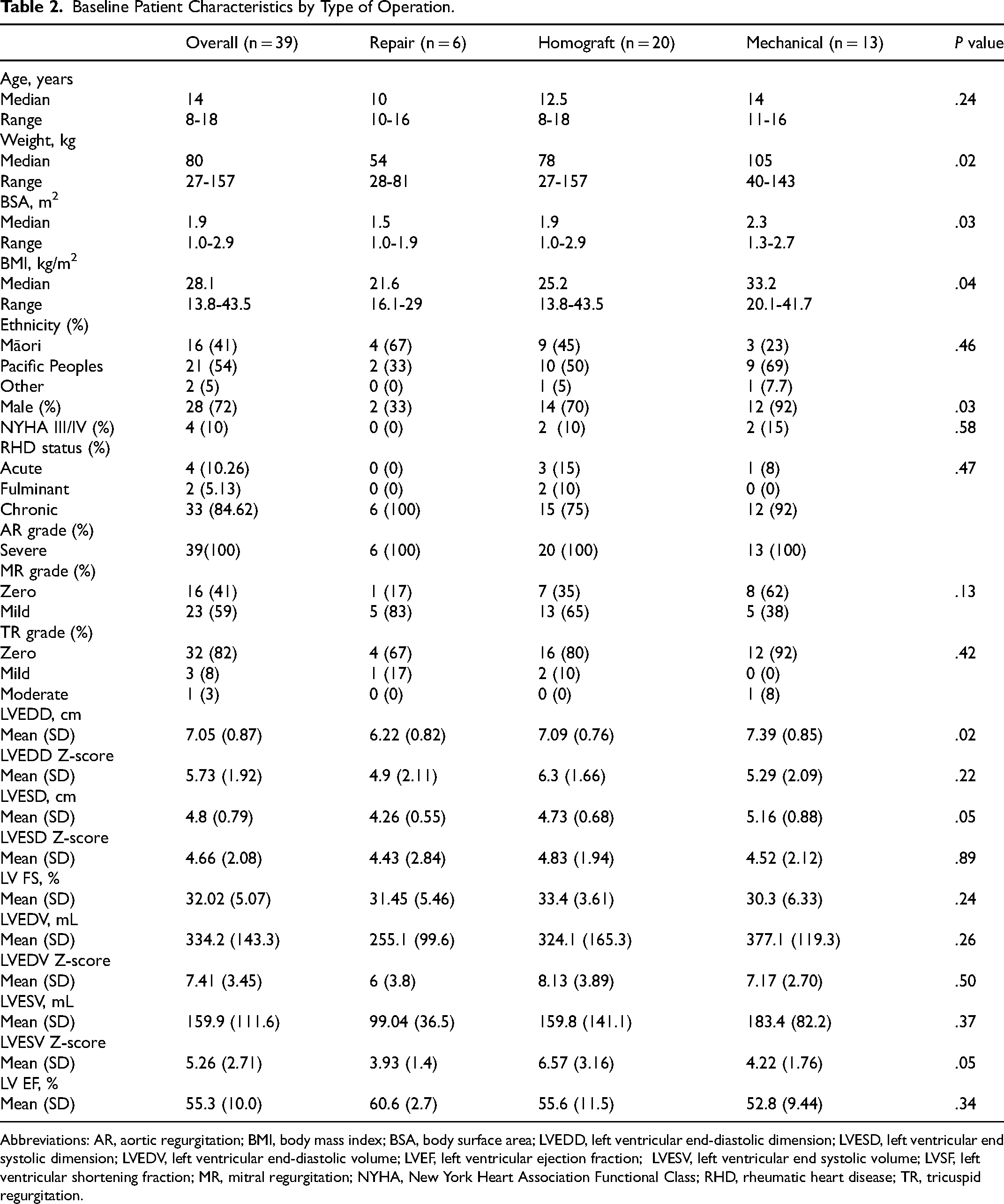
Abbreviations: AR, aortic regurgitation; BMI, body mass index; BSA, body surface area; LVEDD, left ventricular end-diastolic dimension; LVESD, left ventricular end systolic dimension; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end systolic volume; LVSF, left ventricular shortening fraction; MR, mitral regurgitation; NYHA, New York Heart Association Functional Class; RHD, rheumatic heart disease; TR, tricuspid regurgitation.
All patients had severe AR, and 23/39 (59%) had mild MR. Prior to the index operation, the mean LVEF was 55 ± 10% with 10 of 39 (26%) patients having LV dysfunction. There was no statistical difference in LV function for the surgical groups; the mechanical replacement group had the lowest mean LVEF at 52.8%. Those with mechanical valve replacement had higher absolute end-diastolic and end-systolic dimensions (P = .02), while those undergoing homograft replacement had greater end-systolic volume z-score (P = .05).
Early Outcome
Thirty-day mortality and morbidity
There were no deaths or valve reoperations within 30 days of the index operation. A pacemaker for postoperative complete heart block was required for one patient.
Late outcome
Median time from surgery to late follow up was seven years (range 2-15 years). All 39 patients were included in the survival analysis. Late follow-up echocardiographic and clinical data were available for 37 of the 39 patients. Two patients who were included in the intermediate follow-up analysis had no echocardiographic data available during the late follow-up period so were excluded from the echocardiographic analysis.
Late follow up and survival
There were eight deaths during follow-up (8/39, 20%) (Table 3), none in the repair group, 5 of 20 (25%) in the homograft group, and 3 of 13 deaths (23%) in the mechanical group.
Characteristics of Patients who Died During Follow Up.
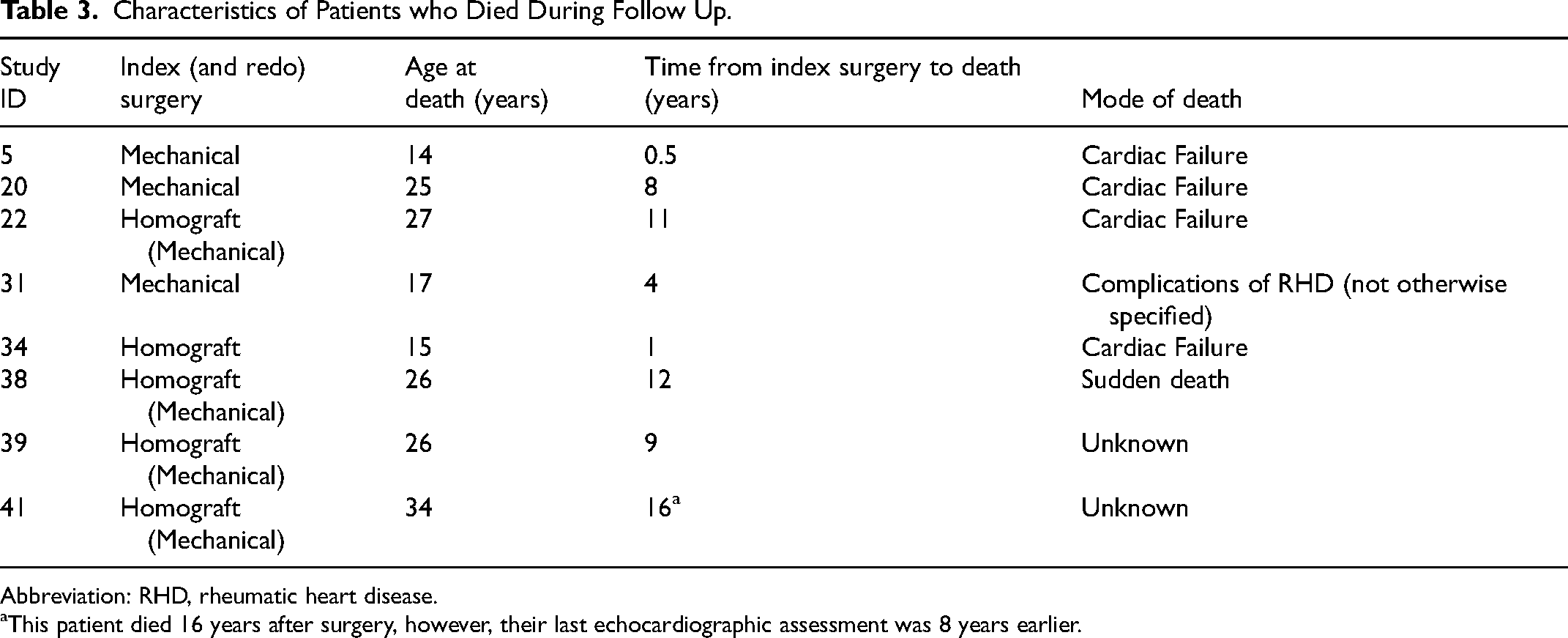
Abbreviation: RHD, rheumatic heart disease.
This patient died 16 years after surgery, however, their last echocardiographic assessment was 8 years earlier.
Cardiac failure was the cause of death for 4 of 8 patients. There was one sudden death and one death was reported as a complication of RHD without further details available. There were two deaths of unknown cause. Actuarial survival for the cohort at 5, 10, and 15 years was 92%, 87%, and 82%, respectively (Figure 2). Median age of death was 25 years (IQR 16-26 years), and the median time from surgery to death was 8.5 years (range 6 months-16 years).
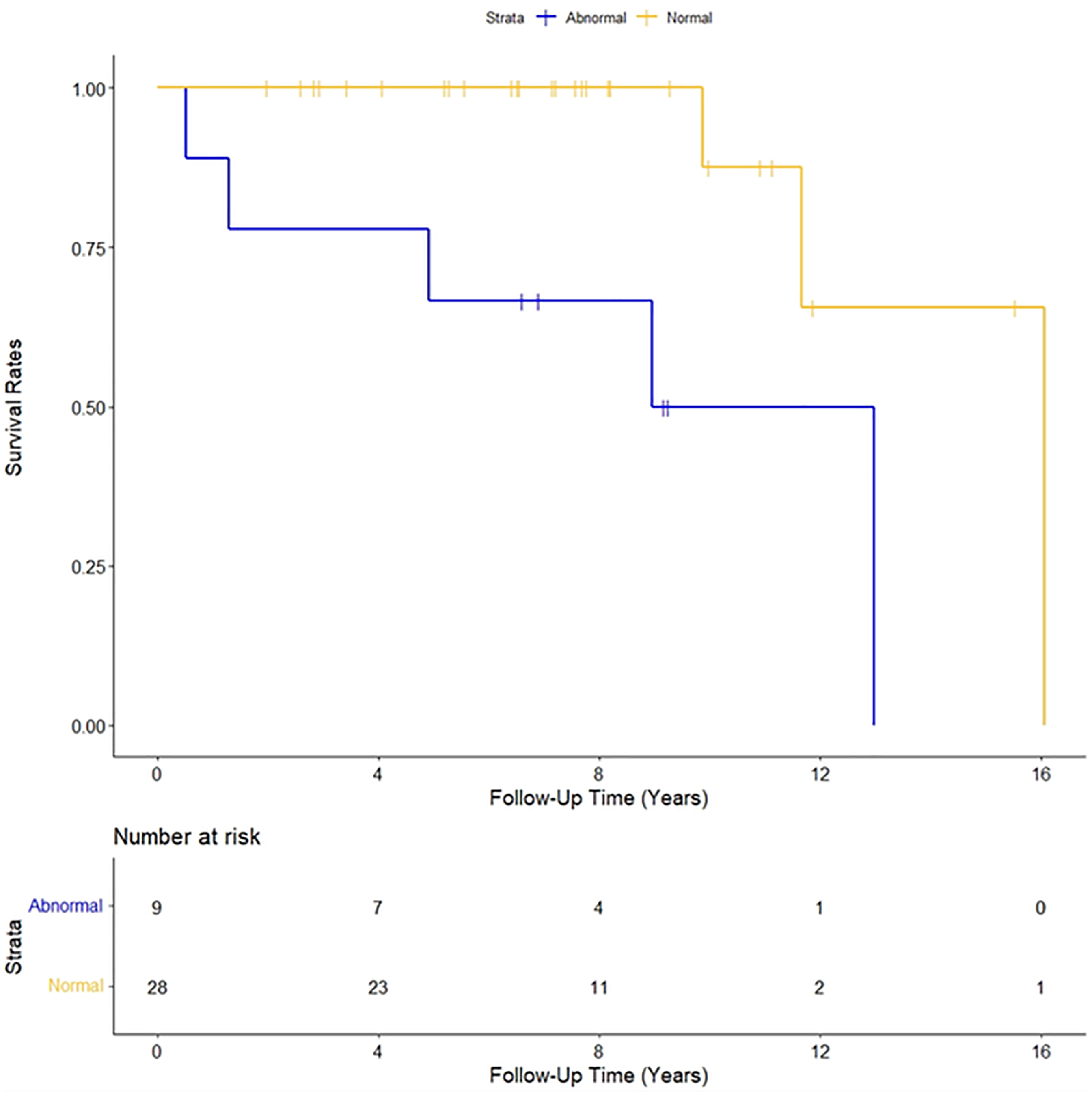
Actuarial survival curve for normal (left ventricular ejection fraction [LVEF] ≥55% or left ventricular shortening fraction [LVSF] ≥27%) versus abnormal baseline LV function.
Univariate analysis showed that only LV dysfunction and higher baseline BSA were associated with increased risk of death (Table 4)—abnormal LV function at baseline had a hazard ratio (HR) 13.3 (95% CI 1.52-115.5) (P = .003).
Univariate Analyses.
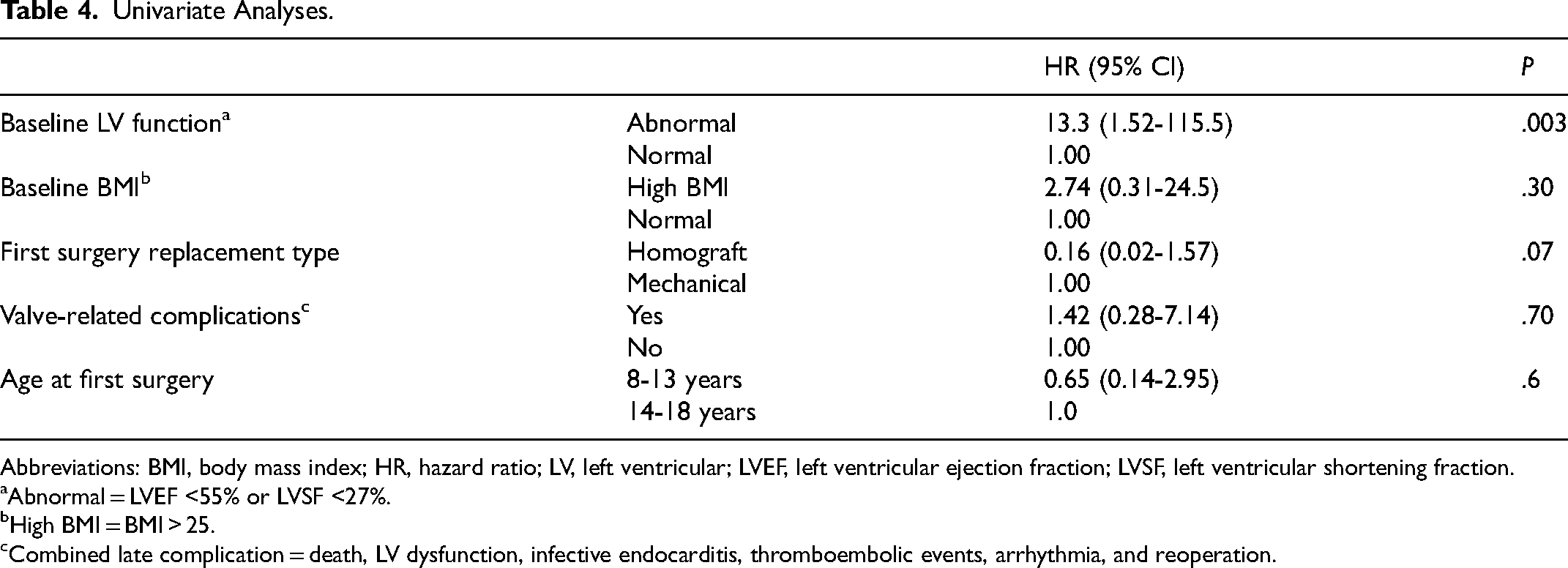
Abbreviations: BMI, body mass index; HR, hazard ratio; LV, left ventricular; LVEF, left ventricular ejection fraction; LVSF, left ventricular shortening fraction.
Abnormal = LVEF <55% or LVSF <27%.
High BMI = BMI > 25.
Combined late complication = death, LV dysfunction, infective endocarditis, thromboembolic events, arrhythmia, and reoperation.
In multivariate analysis, patients with baseline LV dysfunction were more likely to die during the follow-up period when adjusting for BSA (HR 27.5, 95% CI: 1.5-491, P = .02).
There was no difference in mortality or rates of reoperation between those with ARF, fulminant carditis or chronic RHD (HR 0.92, 95% CI: 0.30-2.80, P = .9). Similarly, when combining ARF and fulminant carditis, there was also no significant difference compared with chronic RHD.
Impact of type of surgery on outcome
In the cohort, there were six aortic valve repairs, with long-term outcomes available for five patients. At late follow-up, one patient had required reoperation for severe mixed AR and aortic stenosis (AS), three had mild AR and one had moderate AR. Two patients had mild LV dysfunction, and the remainder had normal LV function.
Of the 20 patients who underwent homograft valve replacement, late follow-up data were available for 19. Reoperation was required for 16 of the 19 (84%) patients after a median of 6.5 years, IQR 2.75 years (range 2-15 years). Of those who did not undergo reoperation, two had mild AR at late follow up and one had asymptomatic severe homograft regurgitation with normal LV size and function.
Of the 13 patients who underwent mechanical valve replacement as their first operation, none had required reoperation. Median size of mechanical valve was 25 mm, range 21 to 29 mm. The mechanical prosthesis to BSA ratio was calculated—median 11.2 mm/m2, range 9.2-18.4 mm/m2. The actuarial survival for those with homograft replacements compared to those with mechanical valves showed a hazard ratio of 0.16 (95% CI: 0.02-1.57, P = .07) (Figure 3). There were two cases of endocarditis in the mechanical valve group, and none in the homograft group. All cases of thromboembolic events occurred in patients after mechanical valve replacement.
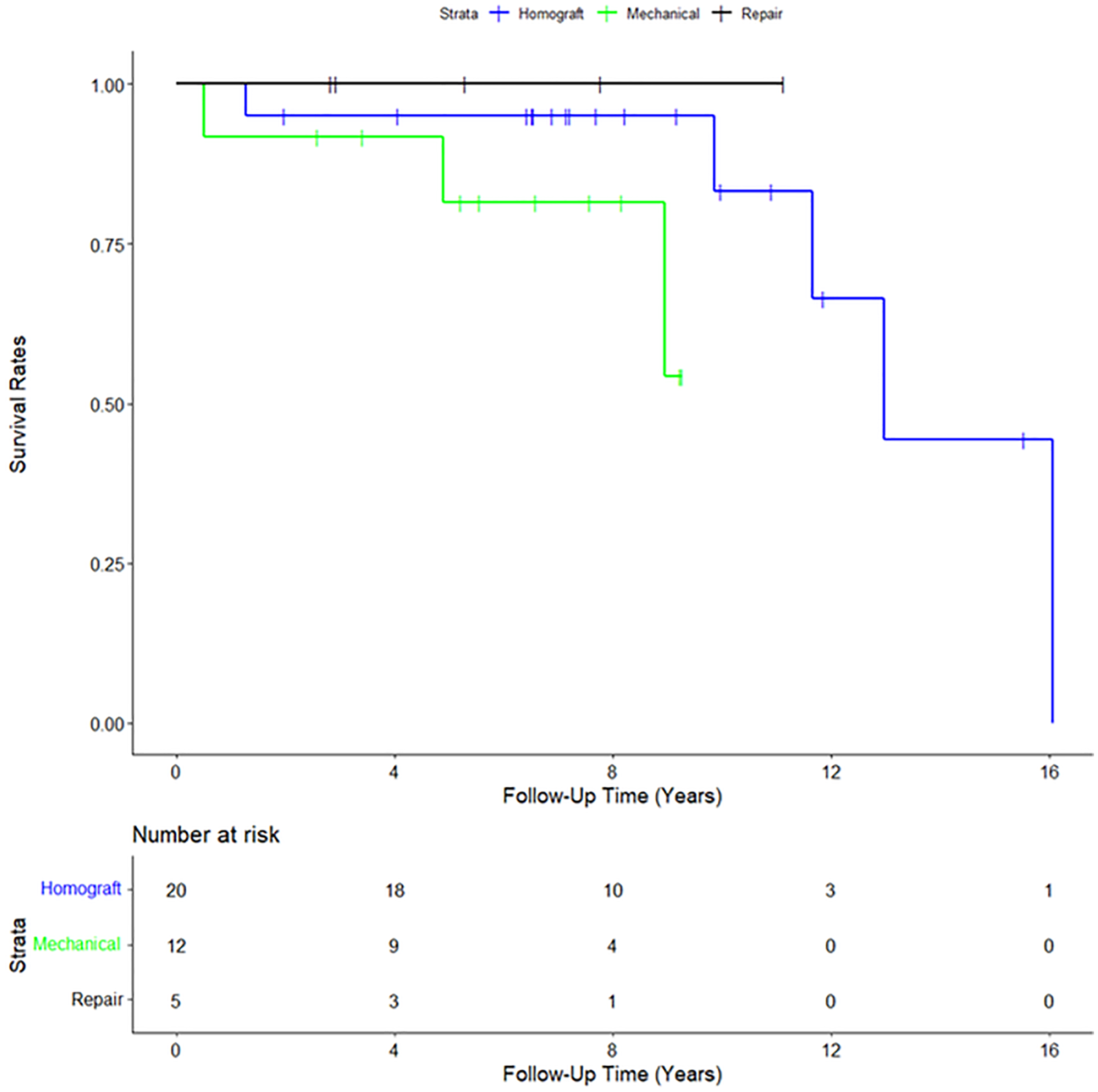
Survival curve based on index surgery type.
Serial Late Ventricular Dimensions and Late Ventricular Dysfunction
Preoperatively 26% (10/39) of patients had LV dysfunction, compared with 27% (7/26) at intermediate follow up and 53% (18/34) at late follow up. Not all echocardiographic data were available for each patient at each time point, limiting the analysis potential.
Intermediate and Late Left Ventricular Function Outcomes
Median time from surgery to intermediate follow up was nine months (range 6-24 months). Thirteen patients were excluded as there was no echocardiogram within the time frame, leaving 26 of 39 patients (67%) in this analysis.
Ventricular dimensions and volumes tended to normalize by the intermediate follow-up period, although LV dysfunction persisted at intermediate follow up for 50% of those with LV dysfunction at baseline. Three patients developed new LV dysfunction at intermediate follow up. Baseline LVESV had the strongest correlation with LV dysfunction at intermediate follow up (r = 0.92, P < .01) (Table 5). Correlations were not improved by indexing for BSA.
Correlation Between Baseline LV Dimensions and Volumes, and Their Associated Z-Scores, with LV Dysfunction at Intermediate and Late Follow Up.a
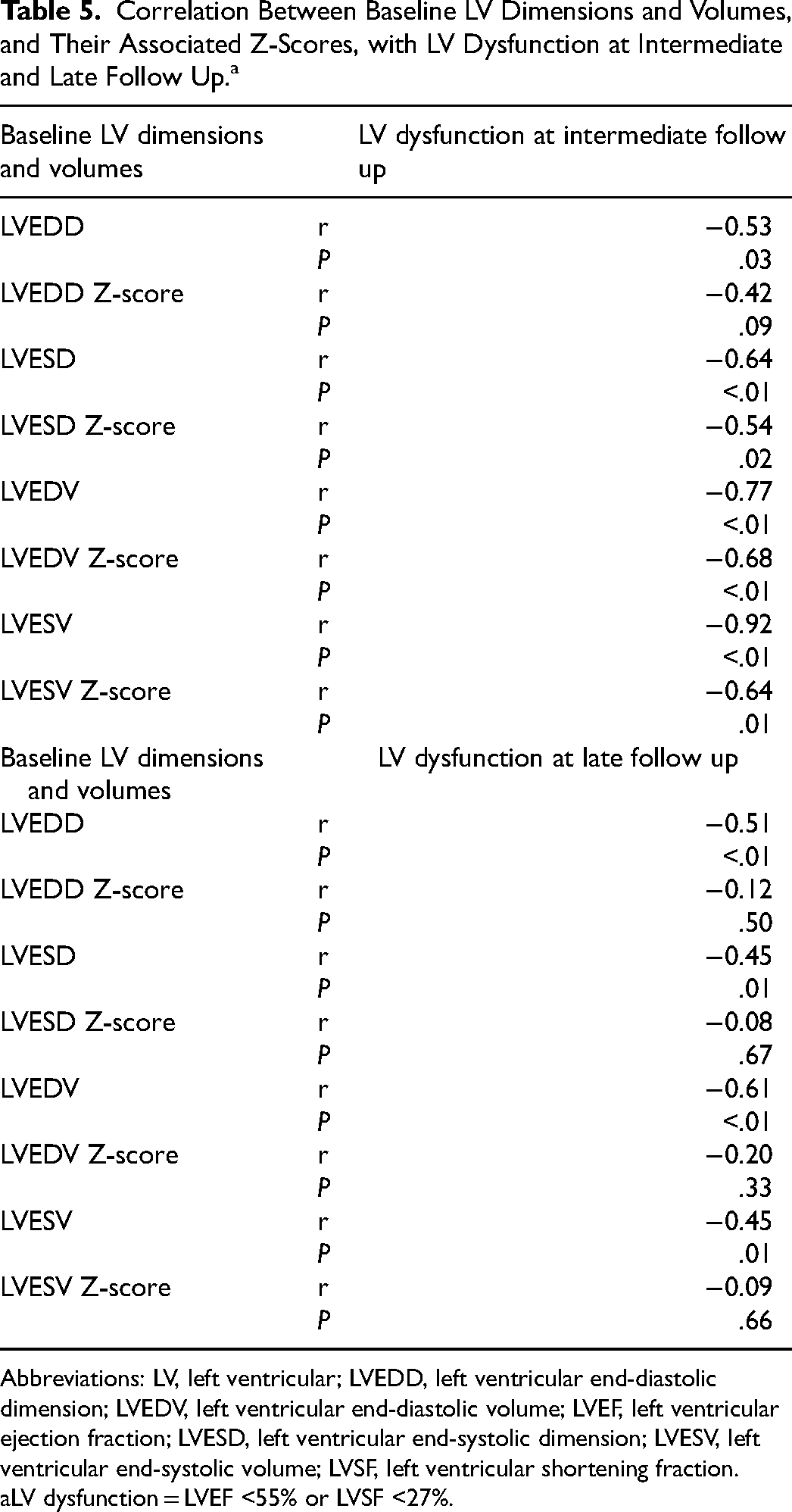
Abbreviations: LV, left ventricular; LVEDD, left ventricular end-diastolic dimension; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic dimension; LVESV, left ventricular end-systolic volume; LVSF, left ventricular shortening fraction.
LV dysfunction = LVEF <55% or LVSF <27%.
Left Ventricular Function at Late Follow Up
Left ventricular dysfunction was detected at late follow up in 18 of 34 patients (53%). Higher baseline LV volumes and dimensions correlated with late LV dysfunction with LVEDV above 330 mL associated with late LV dysfunction (P = .04). Baseline LV dimensions and volumes indexed to BSA did not correlate significantly with late ventricular dysfunction (Table 5).
Body habitus
Median BMI for the cohort (n = 39) at baseline was 28 kg/m2 (range 13-43). At intermediate follow up (n = 26), the median BMI was 30 kg/m2 (range 16-45). By late follow up (n = 34), the median BMI was 37 kg/m2 (range 17-58). Of the patients who died during the follow-up period, six of the eight patients (75%) had a BMI above 30 kg/m2 at the time of their index surgery, compared with 9 of the 31 remaining patients (29%). All patients with weight of more than 105 kg prior to their first surgery died or had LV dysfunction at late follow up (P = .001). High BMI (BMI >25) was not significantly associated with an increased risk of dying during the follow-up period (HR 2.74, 95% CI: 0.31-24.5, P = .3). Age was not associated with death during the follow-up period (Table 4).
Median BSA at the time of the index surgery was 1.93 m2 (range 0.99-2.88 m2). In multivariate analysis, a higher BSA (by 1 m2) was associated with an increased risk of dying during the follow-up period when adjusting for LV dysfunction (HR 27.5, 95% CI: 1.5-491, P = .02) (Figure 4).
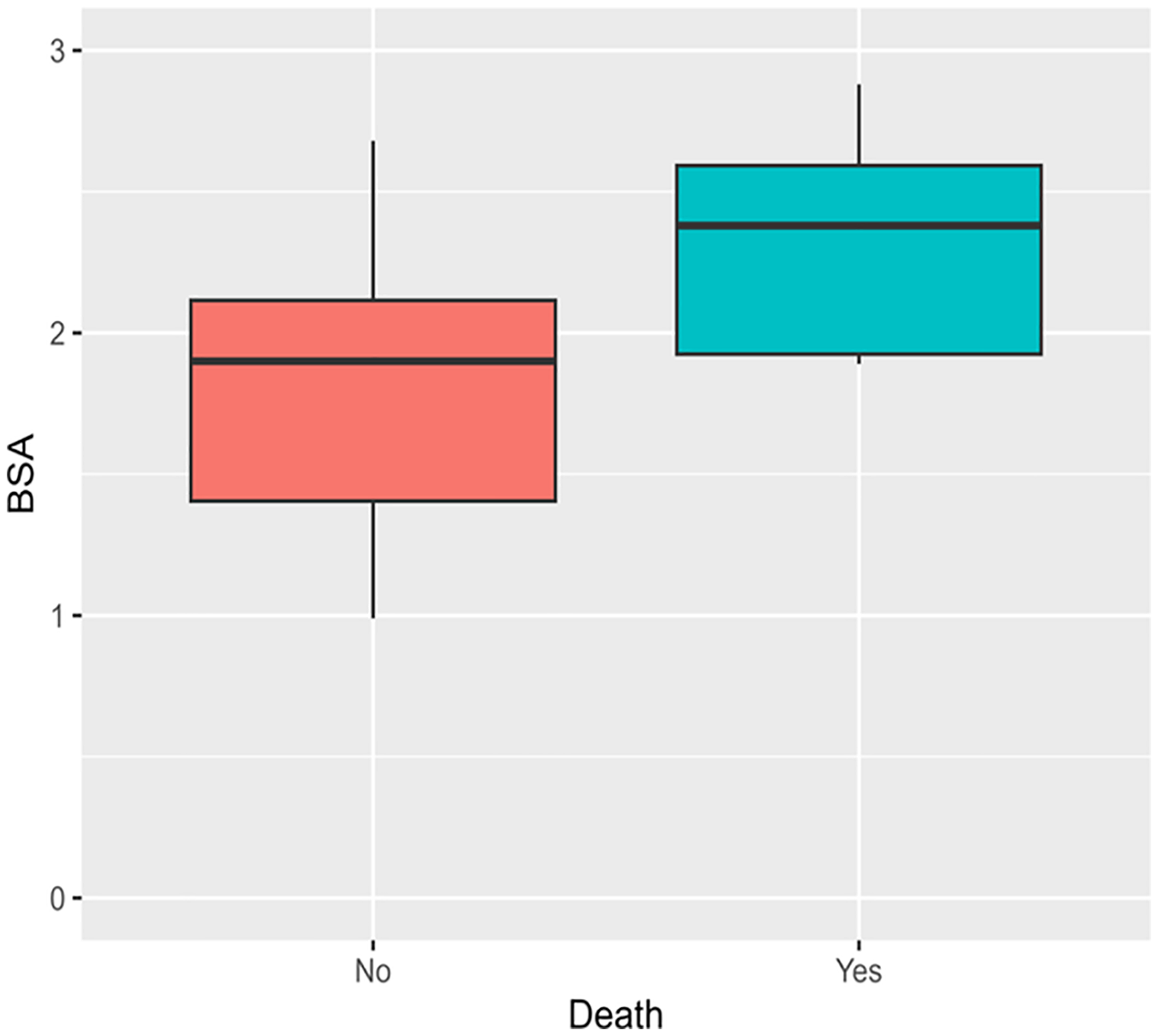
Baseline body surface area compared with death during the follow-up period.
Reoperation
Reoperation was undertaken in 17 of 37 (46%) patients. Of those, 14 underwent only aortic valve replacement (AVR), two had AVR and mitral valve repair, and one had AVR and mitral and tricuspid valve repairs. Most (16/17) of the reoperations were in patients who underwent homograft valve replacement as their index operation.
Fifteen of the 17 reoperations (88%) were mechanical valve rereplacements. There was one homograft valve rereplacement and one bioprosthetic valve rereplacement. The indication for reoperation was mixed AR and AS in six patients, severe AR in six cases, and severe AS in five cases. The patient who underwent bioprosthetic valve replacement was the only one in the cohort to undergo a third operation—a mechanical valve two years later in the setting of endocarditis.
Event-free survival
Freedom from all valve-related complications (death, LV dysfunction, infective endocarditis, thromboembolic events, arrhythmia, and reoperation) at the end of the follow-up period was 20% (Figure 5). Actuarial freedom from late complications after aortic valve surgery at 5, 10, and 15 years was 72%, 31%, and 23%, respectively.
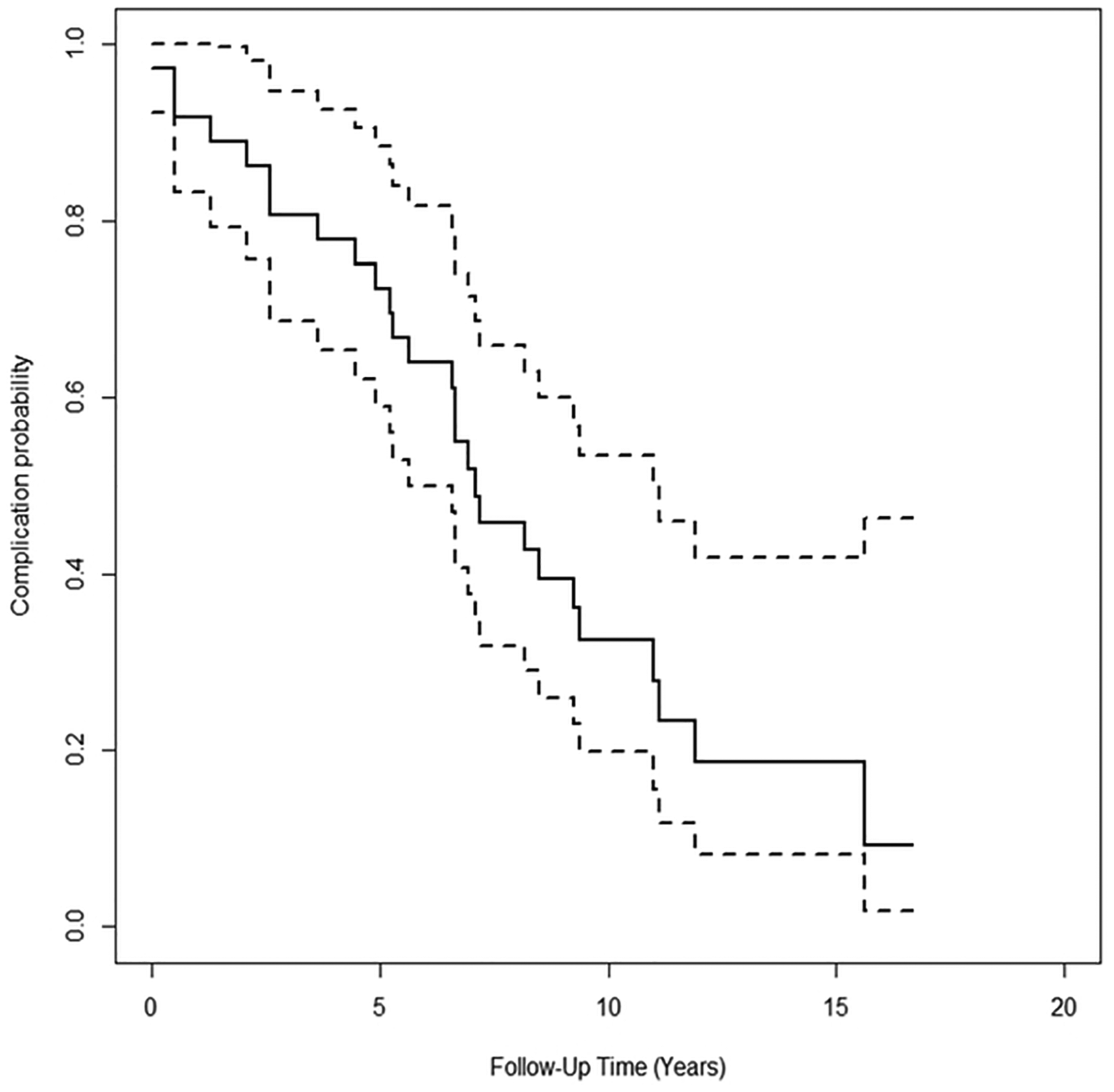
Kaplan-Meier curve showing freedom from late complications.
Endocarditis
Rates of infective endocarditis were 2.4% per patient year of follow up—three cases in the 35 patients with late follow-up data available. Of these, two had index homograft valve replacements and one had a mechanical valve—one case was managed conservatively, one surgically, and one resulted in death.
Thromboembolic events
Of the 10 cases of thromboembolic events, five were after mechanical valve replacements and five were after homograft valve replacements. Seven patients had cerebral infarcts, one had an embolic renal infarct, and two had thrombotic coronary events. All 10 patients had mechanical valves at the time of event; five had previous hospital admissions for subtherapeutic International Normalized Ratio.
Arrhythmia
There were two patients who experienced arrhythmias requiring hospitalization. One patient had atrial fibrillation requiring over 20 hospital admissions, and one patient had ventricular tachycardia.
Mitral valve disease
Mild MR was present in 23 of 39 (59%) patients at baseline. During the follow-up period, six patients went on to develop moderate or severe MR (five moderate, one severe) and only three patients underwent mitral valve surgery at their second operation—all mitral valve repairs were in conjunction with aortic valve surgery.
Discussion
While short-term outcomes for young people undergoing surgery for rheumatic isolated aortic valve disease are favorable, this cohort had high mortality and morbidity in the midterm, median follow up of seven years.
This study demonstrates that preoperative LV dysfunction is a risk factor for midterm survival. The 2020 revision of the AHA/ACA guidelines for the management of valvular heart disease lowered the threshold for intervention due to ventricular dysfunction for patients with AR to an EF of 55% 3 compared with the previous (50% in the 2014 iteration), and our study supports that change also being applied for children. We now recommend consideration for surgery for those with a trend to low normal LVEF, or LVEF < 55%.
Baseline LV dimensions and volumes, and their associated Z-scores, correlated with LV dysfunction at intermediate follow up but not with late follow up. A previous study of those undergoing aortic valve surgery from our institution reported preoperative LV systolic volume indexed to BSA was predictive for LV dysfunction at early (seven month) follow up. 9 We cannot ascertain from this study whether the complexities of the wide range of body habitus, or other time-related factors reduce the usefulness of indexing LV dimensions for predicting late LV dysfunction.
Very large body habitus was significantly associated with poor mortality and morbidity outcomes in our cohort. Though the baseline body habitus status in our cohort is in contrast to many settings globally where RHD remains endemic, it likely represents the indigenous Māori and Pacific Peoples rheumatic population. All patients who were more than 105 kg at baseline died or had LV dysfunction at late follow up. At baseline, only 7 of 39 patients (18%) in our cohort were in the healthy weight category according to The American Academy of Paediatrics categories of BMI for children. 14 Twenty-two of 39 (56%) were either obese or severely obese, and a further 10 were in the overweight category. We considered whether mechanical prosthesis mismatch may have contributed to poor survival and the associated LV dysfunction in those who have high BMI and mechanical valves. However, we could only identify two patients with an increasing velocity across the valve between intermediate and late follow-up time points with new-onset LV dysfunction. Clearly, mechanical prosthesis mismatch should be considered at follow up in all pediatric patients cognizant of growth. We recognize the impacts of childhood obesity on metabolic and cardiovascular health overall. 15 Ambulatory 24 h blood pressure measurements determining the presence or absence of systemic hypertension were not available for this cohort. We cannot exclude hypertension as a confounder for the development of LV dysfunction in individual patients. To our knowledge this is the first study in young people reporting outcomes of patients with high BMI having AVR and highlights the need for more data and closer follow up of this group. Management of obesity should also be considered in the overall care for the patient.
Rheumatic mitral valve repair has been demonstrated to have superior long-term outcomes compared with replacement. 16 In our cohort, there were six aortic valve repairs, all of whom had confirmed ARF episodes. All six had chronic RHD, consistent with local surgical experience that acutely inflamed aortic valves are not reparable due to early tissue stretch and recurrence of prolapse. There were no deaths, episodes of endocarditis, thromboembolic events, arrhythmias, or ARF recurrences in the group who underwent repair. However, there was significant selection bias. These patients were smaller and all had chronic RHD, and LV dimensions and volumes were smaller in this group than the replacement group.
For rheumatic aortic valve disease, replacement has long been the mainstay of treatment and repair a treatment strategy debated over time, due to challenging techniques and the ongoing concern regarding the durability and need for reoperation.17–19 Previous studies assessing outcomes after aortic valve repair for RHD have included significant cohorts of patients having concomitant mitral valve surgery.10,19–23 It is hypothesized that repair of the aortic valve as the nondominant lesion has a more favorable long-term outcome. Myers et al demonstrated promising long-term outcomes of aortic valve repair by cusp extension, with a freedom from reoperation at 15 years of 75%, although 73% of the patients had concomitant mitral valve surgery. 10 Similarly, Grinda et al described a seven-year freedom from reoperation rate of 90% after aortic valve repair with cusp extension. 24 There remains a paucity of evidence on the outcomes of children undergoing isolated aortic valve repair for RHD without significant mitral valve disease.
Our cohort of homograft replacements had superior outcomes compared with mechanical valve replacement in terms of endocarditis and thromboembolic complications as expected. However, reoperation rates were high with 75% undergoing a second operation, after a median time of only 6.5 years. There were five deaths, although four were after the redo mechanical valve replacement. Median weight of the homograft group was significantly lower than the mechanical replacement group. In our practice, the choice of homograft from the Homograft Valve Bank limits our ability to insert valves into larger patients who often had an aortic annulus over 28 mm. Concerns that the longevity of the homograft might be shortened due to increased afterload and high-risk reoperations once the homograft degrades for severely obese patients has led to an institutional bias to replace the homograft with mechanical valves in very large patients.
Autograft AVR is superior to homograft for nonrheumatic aortic valve disease in adults. 25 In the setting of RHD however, concerns have primarily focused on secondary rheumatic involvement on the native pulmonary valve once in the aortic position leading to early autograft failure with therefore high reoperation rates.26–29 This has led to many centers avoiding the Ross technique. Concomitant mitral valve disease has also been demonstrated to be a risk factor for autograft failure and reoperation.30,31 A recent study from Brazil compared outcomes following autograft AVR in patients with rheumatic aortic valve disease with those who had surgery for bicuspid aortic valve, including 86 matched pairs. 26 Only 33 of 147 (22%) of the rheumatic group were receiving regular secondary prophylaxis. There was no difference in survival or reoperation rates between the groups. 26 There were only three reoperations where the autograft failure was attributed to rheumatic valvular disease. 26 There were no Ross operations in our cohort. The promising outcomes from Brazil, when compared to the high rates of reoperation in our homograft cohort, make the Ross operation a potentially appealing option particularly in our population where adherence to secondary prophylaxis is excellent in the young and where there are very low rates of ARF recurrences in children.32,33 However, more data are required to determine the long-term trajectory after the Ross operation in those with rheumatic aortic valve disease.
All patients in this cohort had surgical and echocardiographic findings consistent with RHD. Just under 60% (23/39) had concomitant mild MR and 46% (18/39) had rheumatic morphological changes on the mitral valve on their baseline echocardiogram. One quarter of patients (6/23) with mild MR had progressive mitral valve disease; three patients later underwent mitral valve repair at the time of their reoperation. There were no documented ARF recurrences in the patients with progressive MR.
Limitations
Small study size is a limitation of this study; a common feature of studies on rheumatic aortic valve disease in the young globally. The differences seen with LV volumes and late ventricular function may be related to this small sample size. Those who underwent repair likely had the most favorable anatomy, and those who underwent homograft were also chosen based on patient characteristics, which may influence late outcomes.
This is also a retrospective analysis, with missing data and not all dimension and volumetric echocardiographic data were available for each patient. For many patients in this cohort, reasons for loss to follow up is likely multifactorial and contributed to by the social determinants of health. The authors recognize the impact of colonization and the systemic barriers to accessing health care faced by families in Aotearoa NZ. 34
While all patients were prescribed secondary antibiotic prophylaxis, individual adherence rates were not sought. The study detected three cases of ARF recurrences, similar to the documented rate of ARF recurrences for those receiving secondary antibiotic prophylaxis in NZ. 32 This suggests recurrences were unlikely to be a significant factor in disease progression of the cohort.
Conclusion
Isolated aortic valve surgery for children with RHD is associated with high rates of mortality and reoperation, and low freedom from complications. Left ventricular dysfunction at baseline is associated with increased risk of dying in the follow-up period. There were high rates of reoperation after homograft replacement, and mechanical valve replacements had the highest complication rate. Although our aortic valve repair group was small, outcomes were promising; however, they need to be interpreted in this limited context. Body habitus data demonstrated elevated BMI at baseline which continued to rise through the follow-up time, and elevated BSA is a risk factor for death and LV dysfunction. The surgical threshold for rheumatic aortic valve surgery in children should be influenced by the onset of any degree of LV dysfunction or significantly increasing body habitus.
Footnotes
Abbreviations
Authors’ Note
Data Availability Statement: All data generated or analyzed during this study are included in this published article and its supplementary information files. Ethics Approval: The study received ethical approval from the Auckland Health Research Ethics Committee (AH23874). Informed Consent: This is an IRB-approved retrospective study, all patient information was de-identified and individual patient consent was not required. Patient data will not be shared with third parties.
Acknowledgments
The authors thank Charlene Nell for providing expert assistance with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.