
Abstract
Background
Chylothorax, the accumulation of triglyceride-rich fluid in the pleural cavity, is a well-recognized complication after surgery for congenital heart disease in children. Treatment protocols and role of surgery are not standardized.
Objective
This study aims to evaluate the outcomes of a standardized technique of thoracoscopic ligation of the thoracic duct (TLTD), for the management of persistent chylothorax following pediatric cardiac surgery.
Methods
A longitudinal study was conducted on children diagnosed with postoperative chylothorax at a single center from 2018 to 2024. Children who required surgery were included in the study. Data on demographics, treatment timelines, and outcomes were collected and analyzed.
Results
Out of 11,429 children who underwent cardiac surgery, 24 children (median age of 33.5 months) required surgery for persistent chylothorax. Thoracoscopic ligation of the thoracic duct was typically performed on day 7 after diagnosis. Chylothorax resolved in 23 out of 24 cases by a median of 10 days following TLTD. The procedure caused minimal morbidity, and no significant procedure-related complications. There were two deaths due to poor cardiac function despite resolution of chylothorax.
Conclusion
Thoracoscopic ligation of the thoracic duct is a safe and effective technique for persistent chylothorax in children following cardiac surgery. This standardized technique is reproducible and its timely application enhances recovery and reduces hospital stay. Further research will define the role of this technique in overall management of chylothorax postcardiac surgery.
Keywords
Introduction
Chylothorax is accumulation of milky, triglyceride rich fluid in the pleural spaces. 1 In infants and young children, a common cause is surgery for congenital heart disease. 2 The incidence of chylothorax after cardiac surgery for congenital heart disease varies from 2.8% to 3.8%, but can increase up to 6.9% in neonates and in those with single ventricle physiology. 3 Onset of chylothorax is associated with prolonged hospital stay, increased morbidity from hypoproteinemia and immune suppression, and increased mortality. 4
Management of chylothorax is not standardized, and there are no robust evidence based guidelines. 2 Therapy generally consists of a combination of treatments, with stepwise escalation. In the first instance, most children will have a trial of medical therapy. This includes intercostal drainage, use of fat-free diets, pharmacological agents such as octreotide (a somatostatin analogue), steroids, propranolol, and sildenafil. 2
When medical therapy fails, surgery is often necessary. However, there is no consensus on what “failed medical therapy’ is. The threshold, timing and nature of surgical interventions vary widely and are not standardized. The trigger value varies from >10 mL/kg/d to 100 mL/kg/d, or when the drainage persists for more than 2 to 4 weeks.2,3,5
Various surgical techniques have been described in those with failed medical therapy. These include pleurodesis, fenestration procedures, and pleurectomy. Ligation of the thoracic duct has been shown to provide excellent control of the chylothorax with low morbidity. 6
This article describes the application and outcomes of a standardized thoracoscopic technique for the management and surgical intervention for chylothorax after pediatric cardiac surgery.
Methods
This is a retrospective cohort study conducted at Narayana Institute of Cardiac Sciences—a large volume, quaternary care cardiac hospital based in Bangalore, India. Children who developed postoperative chylothorax after pediatric cardiac surgery for congenital heart disease, performed between 2018 and 2024, were evaluated. Among these patients, those who underwent TLTD were included in the study. Two children, whose parents did not consent for TLTD were excluded. Data were accrued from medical records. The Institution Ethics Committee granted a waiver for the consent procedure and for publication. The management algorithm is summarized in Figure 1.
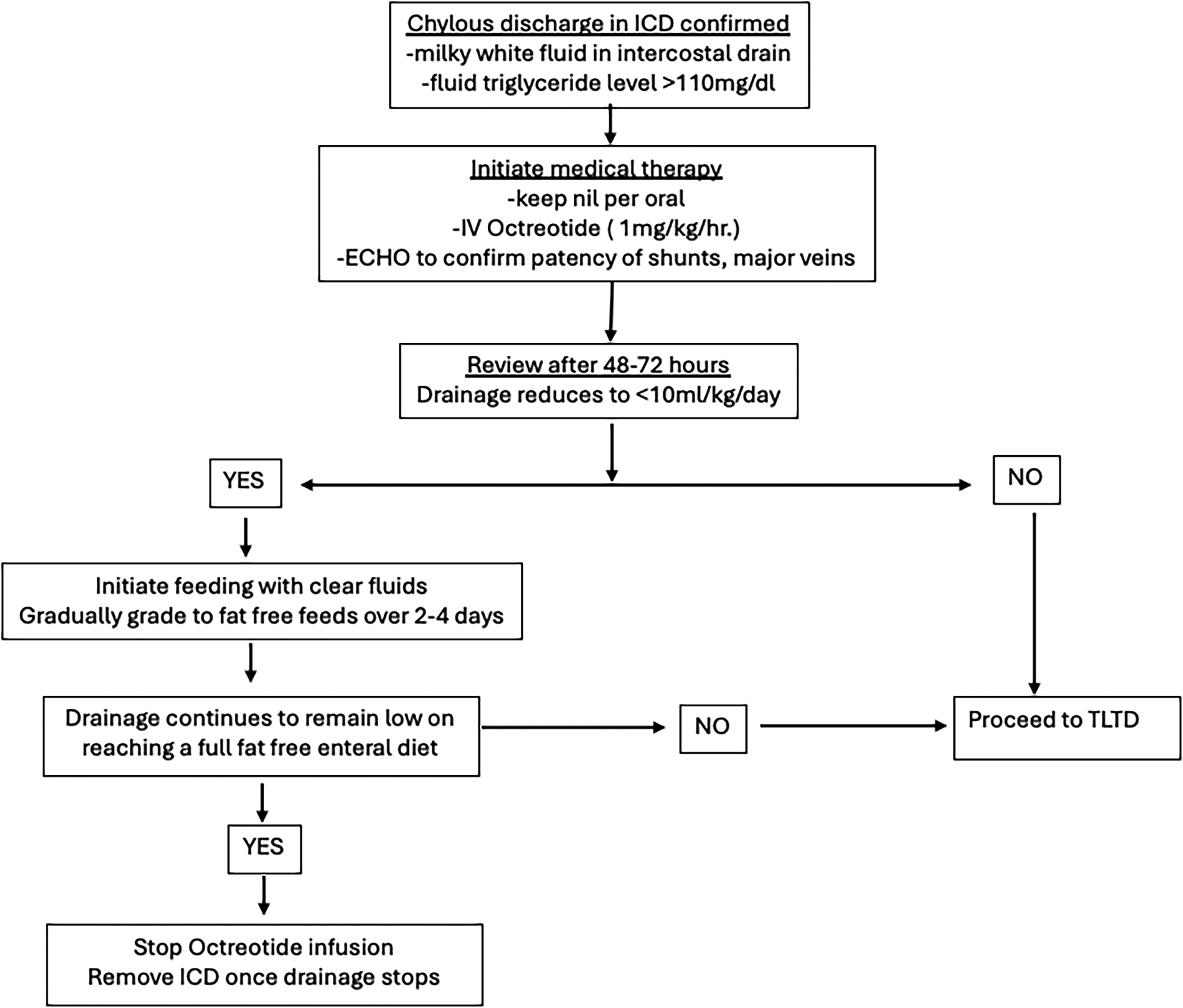
Algorithm for management of chylothorax after cardiac surgery in children. ECHO, echocardiography; ICD, implantable cardioverter defibrillato.
Chylothorax was diagnosed when the intercostal drain output or pleural fluid aspiration (in those who had no intercostal drain) was milky in appearance. A fluid triglyceride level of >110 mg/dL was considered diagnostic 7
All children, when diagnosed with chylothorax, were kept nil per oral and started on an Octreotide infusion (at a dose of 1mcg/kg/hour) for a period of 48 to 72 h. 2 If the drain output fell to <10 mL/kg/day, the child was started on clear fluids orally; and graded up over the next 2 to 4 days to a full fat-free diet. The octreotide infusion was continued until the child was on a full fat-free diet and the intercostal drain was removed. If the drain continued to remain at >10 mL/kg/day, surgery was considered. The surgery—TLTD—was usually done by the seventh to eighth day following congenital heart surgery.
Principles of the Thorascopic Ligation of the Thoracic Duct Procedure
The thoracic duct has an extremely variable and unpredictable course within the thoracic cavity, as it moves across the mediastinum to its insertion at the left subclavian internal jugular vein junction. Often, a number of smaller ducts run in place of a single large thoracic duct. However, as it enters the thorax, through the aortic hiatus of the diaphragm, and in close relationship to the anterior surface of the aorta, the thoracic duct is in a relatively constant position. By carrying the dissection low into the area between the diaphragm, vertebral body and costovertebral junction, it is possible to control the thoracic duct successfully and reliably at this location. The advent of 3 mm and 5 mm laparoscopic instruments allows this procedure to be performed with minimal morbidity.
All children requiring surgery underwent a standardized surgical procedure aimed at thoracoscopically ligating the thoracic duct as it enters the thorax through the aortic hiatus. This standardized technique of a right-sided TLTD is described in detail in the following section.
The procedure was performed under general anesthesia. Tracheal intubation was used. Single lung ventilation was not required. If the operative space was inadequate, a CO2 pneumothorax at a pressure of 4 to 6 mm Hg was used and was well tolerated, even by those with a Glenn or a Fontan procedure. The patient is placed in a left lateral decubitus position. The area of surgery is the costovertebral-diaphragmatic area, deep down in the posterior mediastinum—at the aortic hiatus. The child is well strapped and can be further tilted forward to allow the lung to fall ventrally and expose the area of interest.
The procedure starts with an initial survey conducted with a telescope introduced via the existing intercostal drain site. Filmy adhesions can be broken down with the telescope itself. Unlike in an established empyema, there is very little adhesion and inflammation in the pleural space in chylothorax. Repeated intercostal drain insertions are the usual cause of these adhesions in this instance. Two 3 mm working ports are placed to allow ergonomic triangulation aimed at the costovertebral-diaphragmatic recess posteriorly. In case there are numerous adhesions around the intercostal drain site and the free pleural space cannot be entered, the optical post is placed higher, near the angle of the scapula. Once the ports are introduced, the patient is tilted further ventrally to allow the lung to fall forward. Further ventral mobilization of the lung can be obtained, if required, by dividing the inferior pulmonary ligament.
The following structures are identified: (i) the lowest two vertebral bodies visible in the chest, (ii) the sympathetic chain, placed just lateral to the vertebral bodies, (iii) the aorta, (iv) the inferior vena cava, and (v) the esophagus. All these structures are truly retropleural and situated in a virtual space behind where the parietal pleura reflect off the vertebra ventrally to form the mediastinal pleura. The intercostal vessels in the area are also noted (Figure 2).
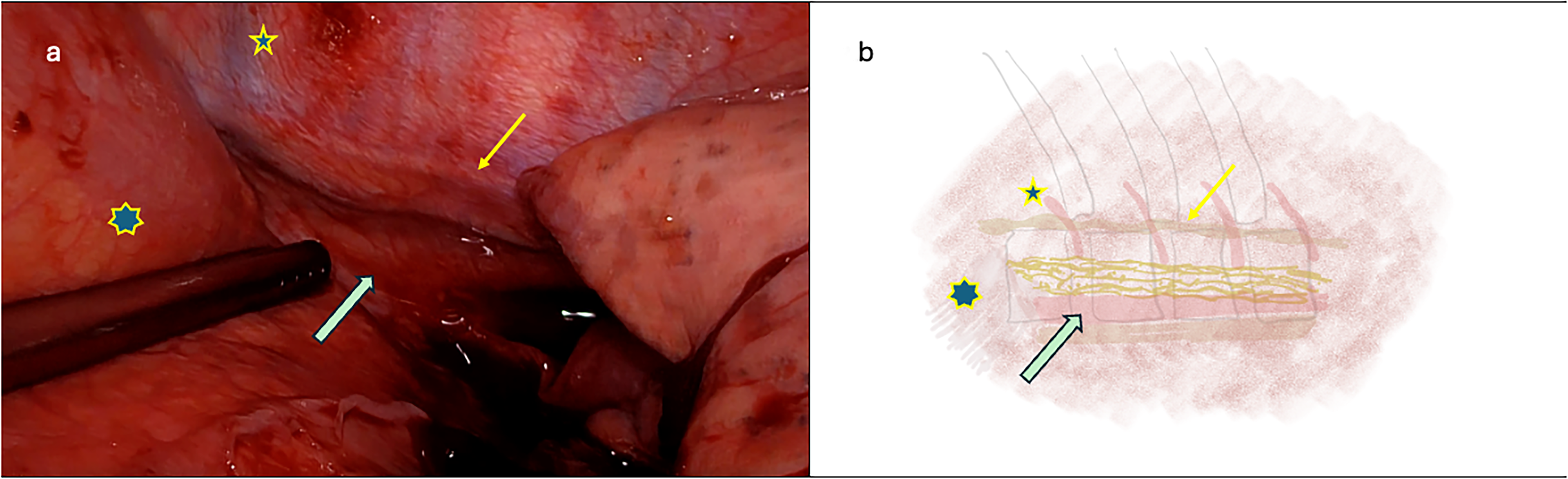
(A and B) Initial thoracoscopic view. The intercostal vessels (star), paraspinal ganglia chain (thin arrow) and the area of the aorta (thick arrow) are clearly visible. Also note the congestion on the pleura due to high venous pressure. The 7-point star indicates the diaphragm, which is being pushed down with the instrument.
A hook electrode is used to make a craniocaudal incision, sited on the anterolateral border of the vertebral body, well medial to the sympathetic chain. The incision is centered on the lowest two vertebral bodies that are visible when the diaphragm is pushed caudally. The pleural incision is then extended for the length of about 2 to 3 vertebral bodies (Figure 3).
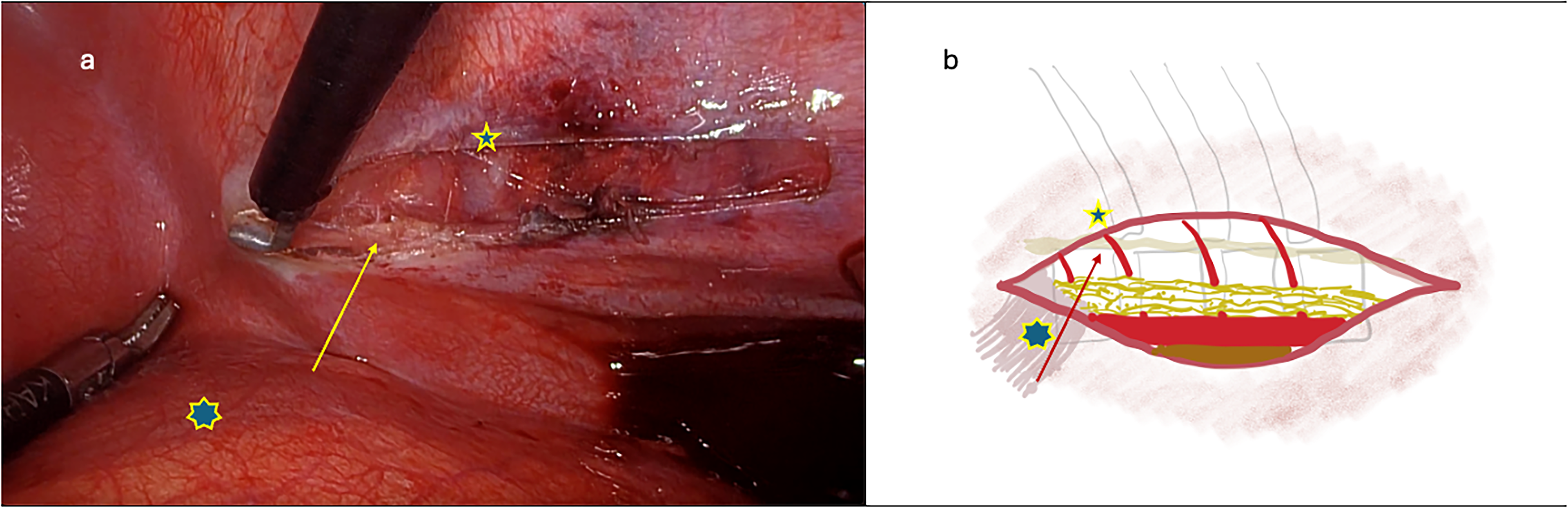
(A and B) Parietal pleura over the anterolateral aspect of vertebral bodies opened longitudinally (small star). Arrow points to the paraspinal sympathetic chain, 7-pointed star marks the diaphragm.
The pleural edges are then retracted to open the retropleural space. Blunt dissection is used to create a plane on the periosteum of the vertebral body by sweeping off all fibro lymphatic tissue ventrally. Dissection is carried forward into the periadventitial tissue on the aorta. Following the intercostal vessels medially greatly facilitates this dissection. Next, another plane of dissection is created along with the anterior pleural flap by stripping away all fibro lymphatic tissue from the back of the pleura. This dissection is carried dorsally toward the aorta to join the plane that was created from dorsal to ventral from the vertebral side. These dissection planes are usually avascular, and dissection is clean, even in those with significant venous congestion (Figure 4).
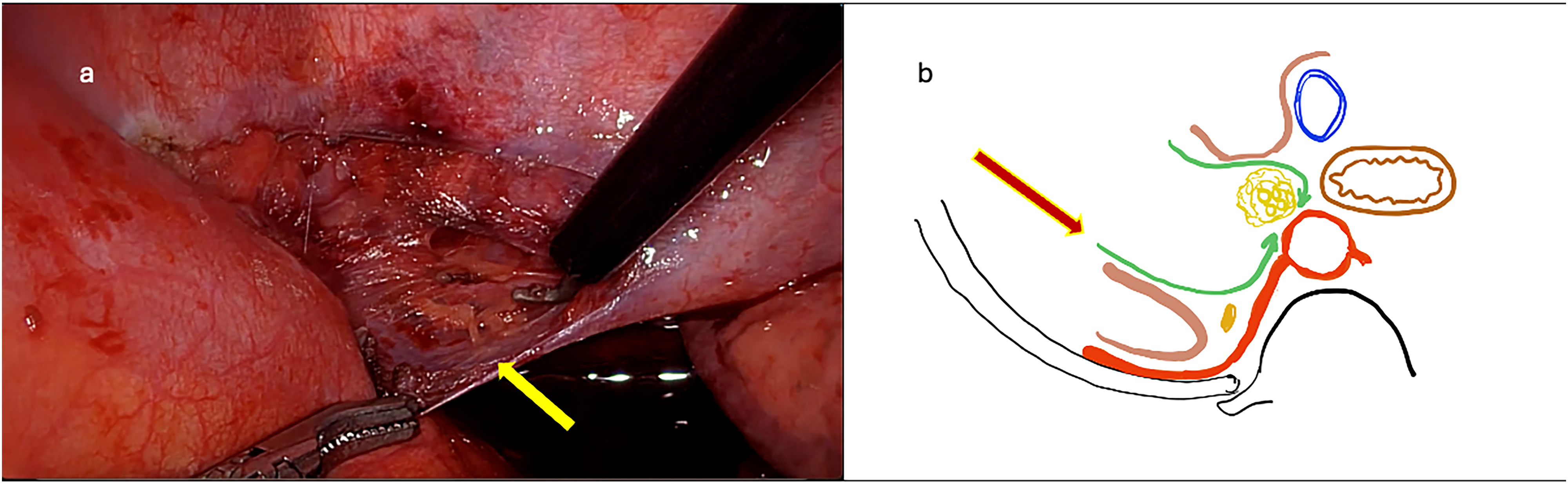
(A and B) Dissection is continued on the pleural surface from anterior to posterior; all fibro lymphatic tissue is swept off the pleura. The arrows indicate the plane of dissection. No attempt is made to isolate the thoracic duct. Similar dissection is also performed on the body of the vertebra, posterior to anterior. The intercostal vessels provide a reliable plane of dissection.
Blunt dissection with a right-angled instrument along with the anterior surface of a conveniently located intercostal vessel allows these two dissection planes to be joined. A vascular loop is slung around the cylinder of fibro lymphatic tissue. At no point in this entire dissection is an attempt made to identify, isolate, or otherwise dissect the thoracic duct itself, even if clearly visible (Figure 5)
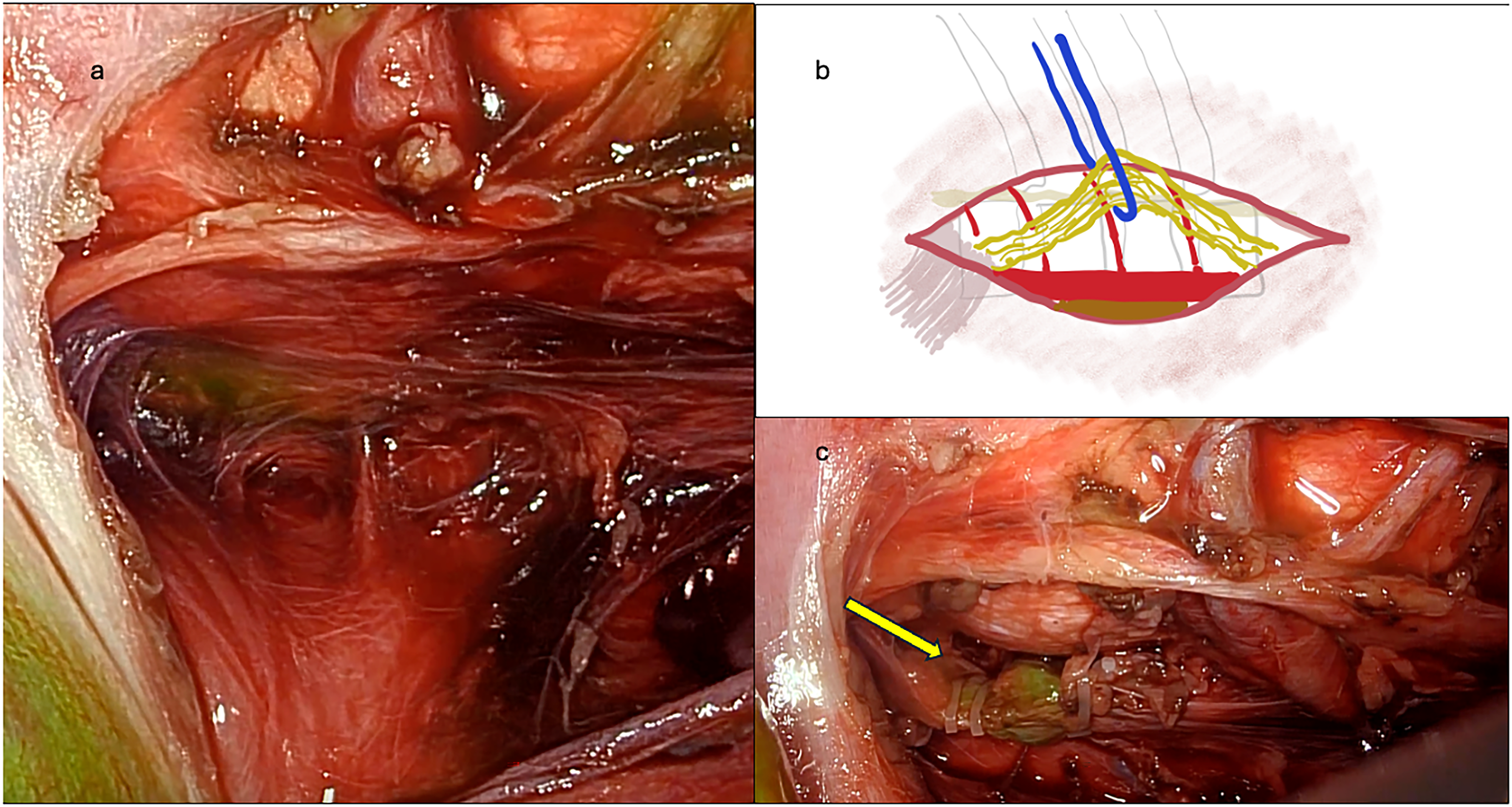
(A-C) Using the intercostal vessels as the dissection plane, the entire cylinder of fibrolymphatic tissue anterior to the aorta is isolated and mobilized. A vessel loop facilitates dissection. Sequential Hem-o-lok clips (Weck Polymer Ligation System) are applied to occlude the thoracic duct. Use of Indocyanine green fluorescence helps confirm secure ligation of the thoracic duct and the cessation of leak (arrow).
Now, gentle traction can be applied on the vessel loop, and this cylinder is further developed—for a length of approximately three vertebral bodies. An attempt must be made to enter the aortic recess in the diaphragm—this is achieved by gently pushing the diaphragm inferiorly while carrying the dissection caudally. The planes as mentioned are generally avascular and gentle blunt dissection is all that is required.
Once an adequate length of fibro lymphatic cylinder is isolated, 3 to 4 Hem-o-lok clips are serially applied, caudocranially, starting as posteriorly as possible, toward the diaphragm. The tissue can then be divided between these clips, and some retrieved for pathology examination if deemed necessary (Figure 5). Hemostasis is confirmed, fibrin glue is instilled into the diaphragmatic recess, an intercostal drainage tube is placed, and the ports are withdrawn.
We usually do NOT perform a pleurodesis as this can lead to significant morbidity and restriction of lung function going forward. It also can potentially make subsequent stages of cardiac surgery more difficult. Pleurodesis is reserved for when the chylothorax is on the left side, and thoracic duct ligation is not possible. In this instance, the pleural cavity is cleared of all chyle, the parietal pleura is abraded gently, and talc is instilled to ensure adhesion between the lung and thoracic wall. This procedure obliterates the pleural space and ensures that the lung does not collapse even if some chyle does collect around it.
Those patients with a left sided chylothorax were treated with video-assisted thoracic surgery and pleurodesis. The optical port was placed at the site of the previous intercostal drain. One additional port was placed at the level of the tip of the scapula. A thorough suction of chyle was performed; loculations if any, were opened into the main pleural space. A mechanical pleurodesis was performed on the parietal pleura using a sterile abrasive material (used to clean tips of cautery). Subsequently surgical talc was instilled all around the pleural space. The lung was inflated and an intercostal drain was placed. A low-pressure suction was maintained on the intercostal drain in the intensive care unit (ICU) for 48 h. In cases of bilateral chylothorax, a right-sided TLTD, as described above, was performed first. In the majority of patients, the left-sided chylothorax also resolved. If large outputs persisted on the left, a pleurodesis was performed. In those with situs inversus, the sides were simply reversed, the left side was treated with TLTD and the right with pleurodesis.
A standardized regimen of postoperative care was followed—the principle being to “hit it with all we have got,” until the area seals off completely.
Child is extubated from the ventilation at the earliest possible opportunity Octreotide infusion is continued until full feeding is reached The child is kept NPO for 48 h For the subsequent 48 h, clear fluids and juices are provided. Thereafter gradual introduction of a fat-free, high-protein diet is initiated.
Chylothorax was considered as resolved when drainage through the intercostal tube ceased and a chest x-ray confirmed a fully expanded ipsilateral lung. The intercostal tube was removed at this time.
Results
During the study period, 11,429 children underwent 12,551 procedures for congenital heart disease. Of these, 171 (1.5%) developed chylothorax. Twenty-four (14%) of these 171 patients underwent TLTD and were included in this study. Fifteen children were males and nine were females. Their median age was 33.5 months (range 2-192 months). Their median weight was 9.5 kg (range 1.4-26 kg). Seventeen of the 24 patients (70%) weighed less than the third centile for age. The details of cardiac procedures and laterality of chylothorax are summarized in Table 1.
Descriptive Data of the Cohort.
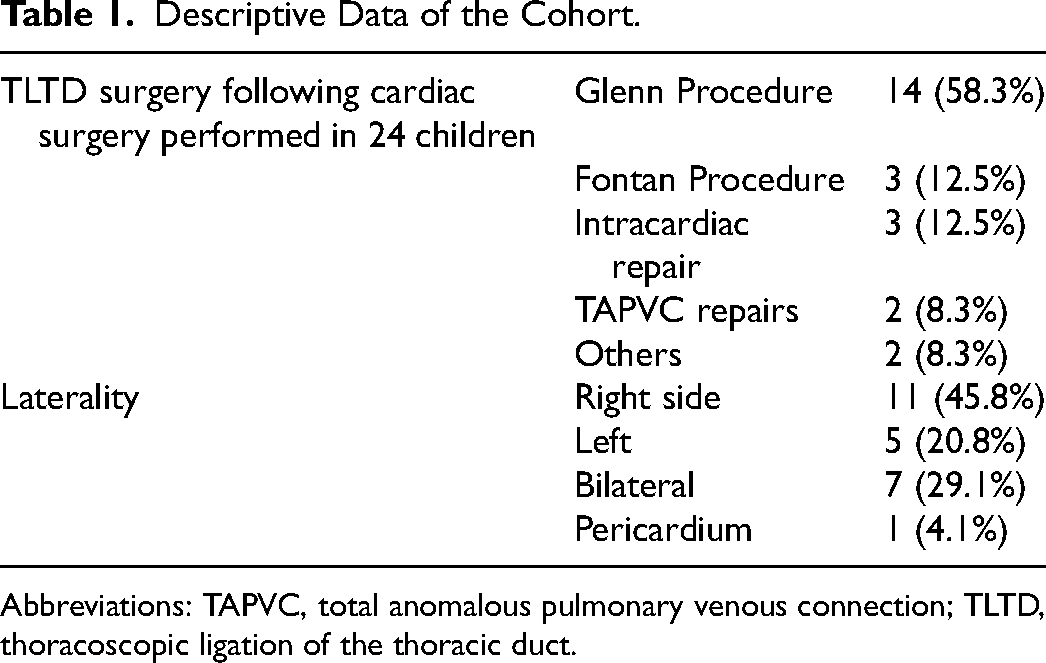
Abbreviations: TAPVC, total anomalous pulmonary venous connection; TLTD, thoracoscopic ligation of the thoracic duct.
Chylothorax was noted at a median period of seven days (range 1-32 days) following cardiac surgery. After these patients had failed an initial period of conservative therapy, TLTD was performed at a median of 15 days (range 2-60) days after the appearance of chylothorax.
Chylothorax resolved, and the intercostal drain was removed in 23 of the 24 patients with chylothorax by a median of 10 days (range 4-31 days) after TLTD. One child continued to have large-volume serous output through the intercostal drain; the triglyceride levels in the fluid were persistently low. The child eventually underwent reversal of his Glenn procedure, and the drainage stopped. The median duration of total hospital stay was 37 days (range 11-98 days).
There were two deaths. One was a two-year-old girl who had a Glenn procedure and the other a ten-year-old child who had a completion extracardiac Fontan. Both these children died from sequelae of persistent poor cardiac output and pulmonary complications; however, the chylothorax itself had resolved in both. There were no other procedure-related complications.
Discussion
Chylothorax is a known sequelae of surgery for congenital heart disease, with a reported incidence ranging from 2% to 6.5%.The incidence appears to be rising-likely due to increasing complexity of procedures being performed. 1 Chylothorax may result from direct trauma to the thoracic duct, high venous pressures or from preexisting lymphatic malformations. 8 The incidence is higher with certain procedures that result in eleation of right heart pressure or involve extensive dissection in the retro- or supracardiac areas for example.
Postoperative chylothorax can lead to several negative consequences. These include respiratory complications due to lung collapse, nutritional deficiencies, electrolyte imbalances, and infection risk. These in turn prolong ICU and hospital stay and increase the risk of mortality. 5 Risk factors for development of postoperative chylothorax include weight <10 kg, age <24 months, open chest, arrhythmias, genetic syndromes, central vein thrombosis, and high hospital volumes.5,9
The management of chylothorax is not standardized. 8 Generally, the initial treatment is conservative, involving use of fat-free diets, diuretics, infusions of somatostatin analogues such as octreotide and intercostal drainage. Pharmacological agents used include: steroids, propranolol, sildenafil, octreotide, sirolimus, and MEK inhibitors. 8 However, if these interventions fail, surgical intervention becomes necessary; about 4% to 9% children require surgery.5,9 Our cohort received octreotide as a part of the algorithm of care. Although octreotide has been known to cause serious side effects such as hyperglycemia, reduced intestinal motility, altered liver enzymes, and in rare cases necrotizing enterocolitis, the incidence of complications is low. In the postoperative cardiac surgery chylothorax setting, Jenkinson et al, in a systematic review of 621 children, reported a complication rate of 2%—mostly minor that did not require a cessation of treatment. 10
There is no standardized approach to surgical management of chylothorax. Procedures reported include pleurodesis, pleuroperitoneal shunts, pleurectomy, diaphragmatic fenestration and direct suture-ligation of leak points, and/or thoracic duct and microvascular lymph-venous anastomosis.11,12 Thoracoscopic pleurodiaphragmatic surface clipping has also been reported. 13 However, these procedures have not provided consistent results and are performed with great variability in different centers. Low ligation of the thoracic duct in the right chest via open thoracotomy has been described and had a success rate of 90%.14,15
The advent of thoracoscopic procedures has allowed principles of minimally invasive surgery to be applied even in small infants. Smaller 3 mm instrumentation is optimal for this purpose. The youngest child operated in this series was two months old and weighed 1.4 kg.
The procedure that we describe here is a standardized approach that can be used in nearly every scenario of children with chylothorax following cardiac surgery. It relies on the consistency of the thoracic duct's position as it enters the thorax through the aortic hiatus in the diaphragm. This anatomical position is constant and is easily accessible through thoracoscopy. It can be mirrored even in patients with situs inversus.
By using fixed and easily identifiable landmarks, the procedure ensures successful control of the thoracic duct, regardless of its configuration. By remaining in the subpleural plane, it is possible to dissect around the fibro lymphatic tissue, thereby avoiding iatrogenic injury to the fragile thoracic duct. As can be seen from the data presented, the procedure is highly reproducible and offers a high degree of control of chylothorax. Its minimally invasive nature and high success has prompted its early application in the course of illness. If medical therapy has not been successful by the end of one week, we proceed with TLTD. This approach is akin to the early application of VATS in the management of empyema in children, significantly shortening the course of the illness, reducing morbidity, ICU, and hospital stay. The procedure is well tolerated even in infants who have had complex cardiac surgery, including those with univentricular physiology. The procedure is also reproducible and easy to teach and learn.
Another concern is that ligation of the thoracic duct will increase the risk of chylous ascites; however, this phenomenon was not observed in our cohort, nor reported in other case series. 6
Indocyanine green (ICG) can serve as an adjunct to help identify lymphatic channels. 16 However, as our technique does not primarily focus on identifying the thoracic duct itself, the application of ICG in this scenario remains to be defined. Imaging with radioisotope as well as dynamic contract magnetic resonance lymphangiographic techniques provide excellent anatomical delineation of the lymphatic system. Cases of endovascular, microvascular, and lymphangiographic techniques to treat chylous leaks in children with cardiac anomalies have been reported. These are not without complications and long-term outcomes are unknown. 17
The small sample size, recruited from a single center, and its retrospective design are major limitations of this study. However, chylothorax following pediatric cardiac surgery is an infrequent problem even in large-volume pediatric cardiac surgery centers. Putting together a prospective, multicenter study, of adequate power is challenging given the low incidence of the problem and heterogeneity of its management protocols across centers. The strength of this report is the standardized approach to management and surgery. A standardized and reproducible surgical approach, one that provides excellent outcomes, has been presented.
In light of this experience, we recommend TLTD for children with chylothorax following cardiac surgery who do not respond by five to seven days of conservative therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.