
Abstract
Purpose
We reviewed all 181 patients with pediatric and/or congenital heart disease (CHD) who underwent cardiac transplantation at the University of Florida from January 1, 2011, to March 1, 2022, and compared those with CHD with those who had acquired heart disease (AHD).
Methods
Patient characteristics were assessed, stratified by CHD versus AHD. Continuous variables are presented as mean (SD); median[interquartile range](range). Categorical variables are presented as N (%). Univariable associations with long-term mortality were assessed with a Cox proportional-hazards model. The impact of CHD versus AHD on mortality was estimated with multivariable models. The Kaplan-Meier method was applied to estimate survival stratified by CHD versus AHD status.
Results
Congenital heart disease was present in 112/181 patients = 61.9% of the total cohort. Acquired heart disease was present in 69/181 = 38.1%. More patients with CHD had prior cardiac surgery (95/112 = 84.8% vs 35/69 = 50.7%, P < .0001) and pretransplant liver dysfunction (19/112 = 17.0% vs 4/69 = 5.8%, P = .037). Congenital heart disease patients had longer bypass times (minutes): 148 (55.2); 137 [113-174] (72-526) versus 108 (40.3);101 [81-125] (59-300), P < .0001; longer cross clamp time (minutes): 85.9 (21.2); 85 [73-100] (49-152) versus 66.3 (14.7); 65 [55-75] (44-106), P < .0001; and lower minimum temperature on bypass (°C): 27.4 (4.3); 28 [24-31] (19-34) versus 31.6 (3.1); 32 [31-34] (20-36), P < .0001. Posttransplant length of stay (days) was longer in CHD patients: 34.5 (26.8); 27 [19-40] (3-158) versus 29.7 (48.2); 18 [15-26] (0-343), P = .0001. In multivariable analysis, CHD remained a risk factor for mortality after controlling for all variables significant in univariable modeling. Overall Kaplan-Meier 5-year survival in all 181 patients (95% confidence interval) = 85.8% (80.0%-92.1%). Kaplan-Meier 5-year survival = 77.4% (68.4%-87.5%) in CHD and 98.5% (95.6%-99.9%) in AHD, P < .0001.
Conclusion
Congenital heart disease is a risk factor for mortality after cardiac transplantation. Efforts must be made to understand and mitigate this risk.
Keywords
Introduction
The characteristics and outcomes of patients undergoing cardiac transplantation continue to evolve.1–3 This evolution is especially important for patients with pediatric and congenital heart disease (CHD) secondary to a notable shortage of donor hearts from smaller patients1,4,5 as well as the lack of available implantable ventricular assist devices (VAD) for these smaller patients.4,6–8 Strategies have been developed to transplant hearts into patients with even the most complex forms of CHD 9 ; however, many questions remain unanswered. Patients with CHD have unique characteristics that are associated with increased risk and complexity before, during, and after cardiac transplantation. It is only by understanding these characteristics and developing strategies to mitigate these risks that outcomes will continue to improve.
In 2023, we published our single-institution analysis of 186 heart transplants for pediatric or CHD and examined the impact of a pretransplant VAD. 10 This prior publication concluded that the “presence of a pretransplant VAD is not a risk factor for mortality after transplantation for pediatric or congenital heart disease.” 10 This previous analysis included all pediatric patients (neonates, infants, and children) with CHD or acquired heart disease (AHD) and all adults with congenital (but not acquired) heart disease who underwent heart transplantation at the University of Florida from January 1, 2011, to March 1, 2022, inclusive. This previous analysis reported that “survival 5 years posttransplant in patients with a pretransplant VAD is roughly equivalent to patients without a pretransplant VAD.” 10 A variety of prior multi-institutional analyses have demonstrated that patients with CHD have increased posttransplantation mortality compared with those without CHD.11–14 Therefore, during the peer review of our prior publication, 10 we were asked by the reviewers to generate two new subanalysis from this prior publication: (1) a specific analysis of the subset of patients with CHD in our previously published cohort 10 (ie, excluding those patients with AHD), and (2) a direct comparison of the patients with CHD with those with AHD in our previously published cohort. 10 In 2025, we published a manuscript to address the first of these two requests; this 2025 publication contained a retrospective review of our management strategy and outcome data for all 112 patients with CHD who underwent cardiac transplantation from January 1, 2011, to January 3, 2022 at the University of Florida, in order to evaluate the impact of pretransplant support with a VAD in this specific cohort. 15 Our current manuscript addresses the second request described above from the reviewers and is based on the 181/186 patients in the previously published cohort of 186 patients with either CHD or AHD (ie, the five patients who were retransplants in this original cohort were excluded from the current analysis). Therefore, the purpose of this manuscript is to review our management strategy and outcome data for all 181 patients with pediatric and/or CHD who underwent cardiac transplantation at the University of Florida from January 1, 2011, to March 1, 2022, and to compare the outcomes of those with CHD with the outcomes of those with AHD.
Patients and Methods
Institutional Review Board and Database
This study was approved by the University of Florida Institutional Review Board with waiver of the need for consent (IRB202101584, approved June 29, 2021). Data were sourced from a registry and database (CardioAccess Incorporated, Saint Petersburg, Florida, and Fort Lauderdale, Florida: http://www.cardioaccess.com) that uses software certified by the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database and has been prospectively maintained on all patients undergoing pediatric and/or congenital cardiac surgery at the University of Florida. In this manuscript, we use the definition of Operative Mortality utilized by STS.
Patients
This analysis includes all 181 patients who underwent cardiac transplantation at the University of Florida from January 1, 2011, to March 1, 2022, inclusive, with the diagnosis of pediatric and/or CHD. In other words, this analysis includes pediatric patients (with AHD or CHD) and all adults with CHD (but not AHD) heart disease. Patents with AHD had diagnoses of cardiomyopathy or myocarditis, while patients with CHD had either biventricular CHD or univentricular CHD. These 181 patients received 186 heart transplants because five of these patients underwent retransplantation at the University of Florida, with the second transplant performed secondary to chronic rejection. For this analysis, we defined pediatric as patients <18 years of age; therefore, this analysis includes all heart transplants performed in patients <18 years of age at the time of transplant (n = 161), as well as all heart transplants performed in patients ≥18 years of age at the time of transplant with the diagnosis of CHD (n = 25). For the analyses reported in this manuscript, patients who had multiple heart transplants were limited to only their first heart transplant in order to remove dependencies in the data. Consequently, the five cases of retransplantation were excluded from these analyses; therefore, this analysis only includes 181 cases of first-time cardiac transplantation.
Our detailed protocols for immunosuppression, desensitization of immunosensitized patients with elevated panel reactive antibody (PRA), and immunosurveillance have previously been published. 16 Similarly, our surgical techniques for VAD insertion and our detailed protocols for VAD management and anticoagulation while supported with VAD have previously been published.10,17,18
Statistical Methodology
Initial descriptive comparisons between the characteristics of the two cohorts of patients (CHD vs AHD; Table 1) were performed for all 181 transplants. Patient characteristics (Table 1) were assessed, stratified by CHD versus AHD. Continuous variables are presented as mean (SD); median [interquartile range, ie, 25th-75th percentile] (range). Categorical variables are presented as a number (percentage). Univariable P-values are the results of Fisher exact tests (categorical variables) or Wilcoxon rank-sum tests (continuous variables).
Patient Characteristics (n = 181 Patients) Stratified by Disease Status.
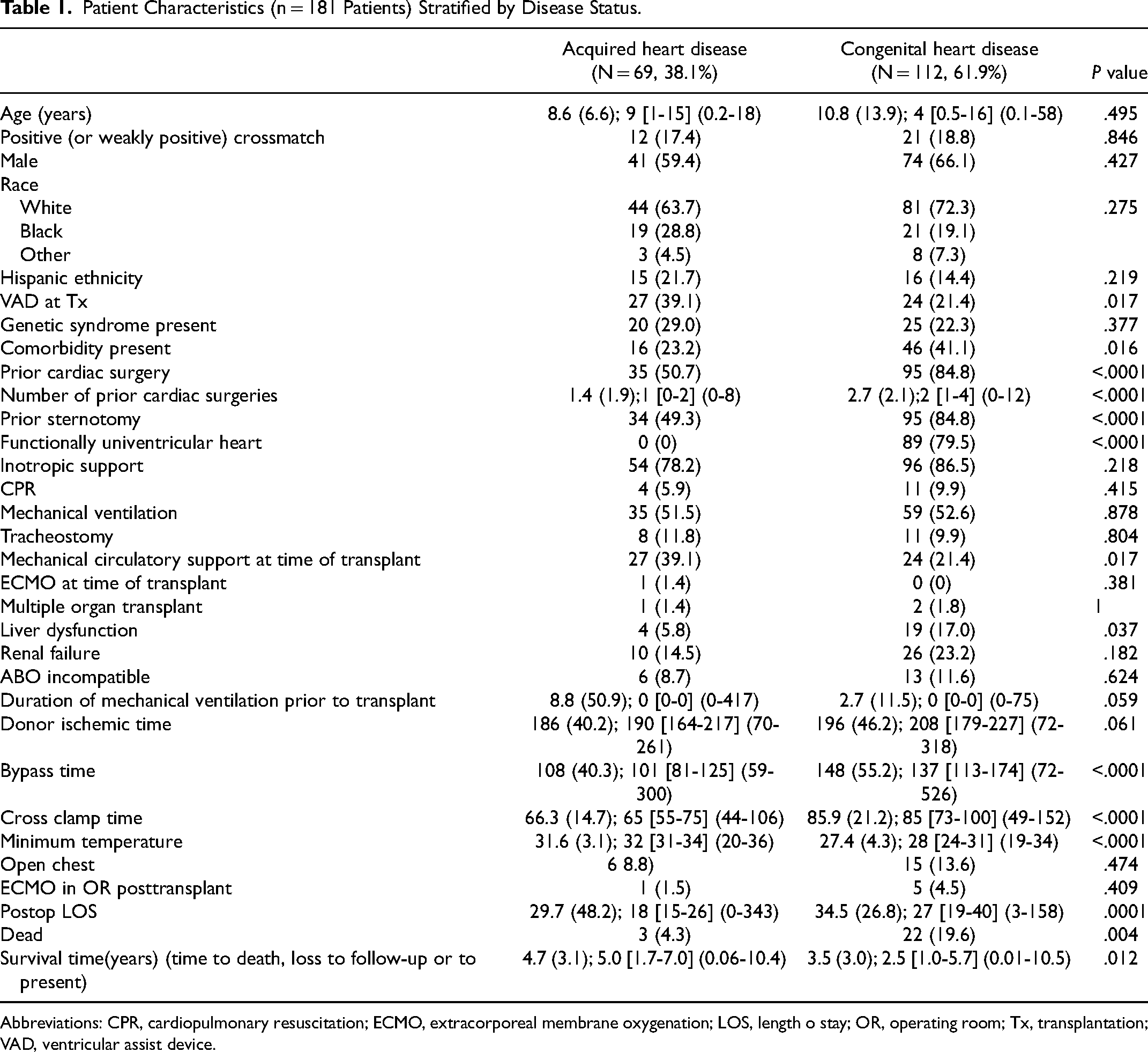
Abbreviations: CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation; LOS, length o stay; OR, operating room; Tx, transplantation; VAD, ventricular assist device.
Univariable associations with long-term mortality (Table 2) were assessed with Cox proportional-hazards models with the factor as the only predictor of mortality; hazard ratios (HRs) and P-values are reported. Because of the sample size (n = 25 deaths), the impact of CHD versus AHD on mortality was estimated with a series of multivariable models (Table 3), each controlling for only one of the factors shown in univariable analysis to be associated with long-term mortality. The Kaplan-Meier method (Table 4; Figures 1 and 2) was used to estimate 1-, 3-, 5-, and 10-year survival for patients stratified by CHD versus AHD status, and the log-rank test was applied to compare groups. All analyses were performed using the R statistical software package (V.4.1.0; R Foundation for Statistical Computing).
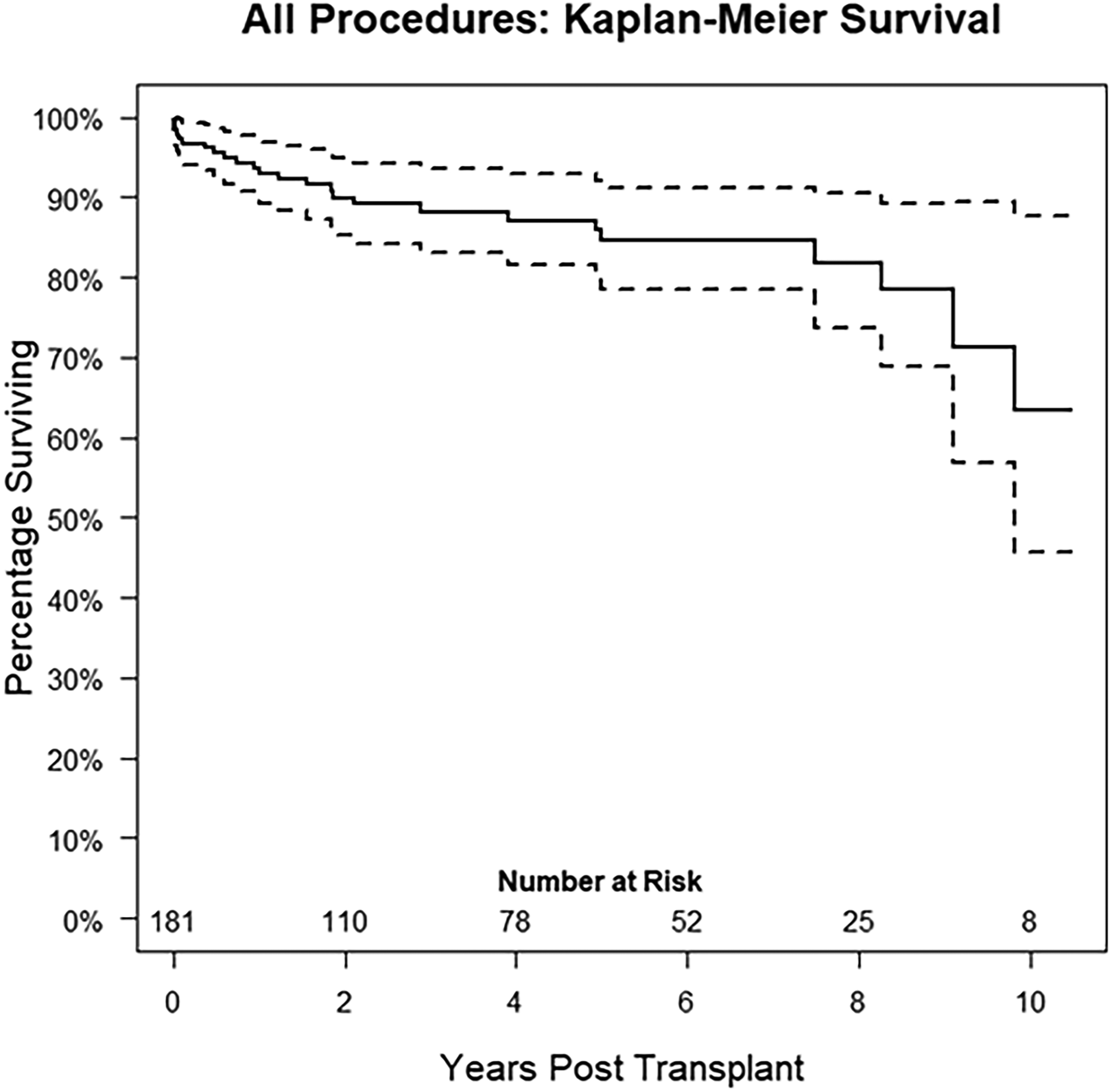
Kaplan-Meier survival curve that documents longitudinal survival with 95% confidence intervals for all 181 patients. Overall Kaplan-Meier 5-year survival (95% confidence interval) for all 181 patients is 85.8% (80.0%-92.1%).
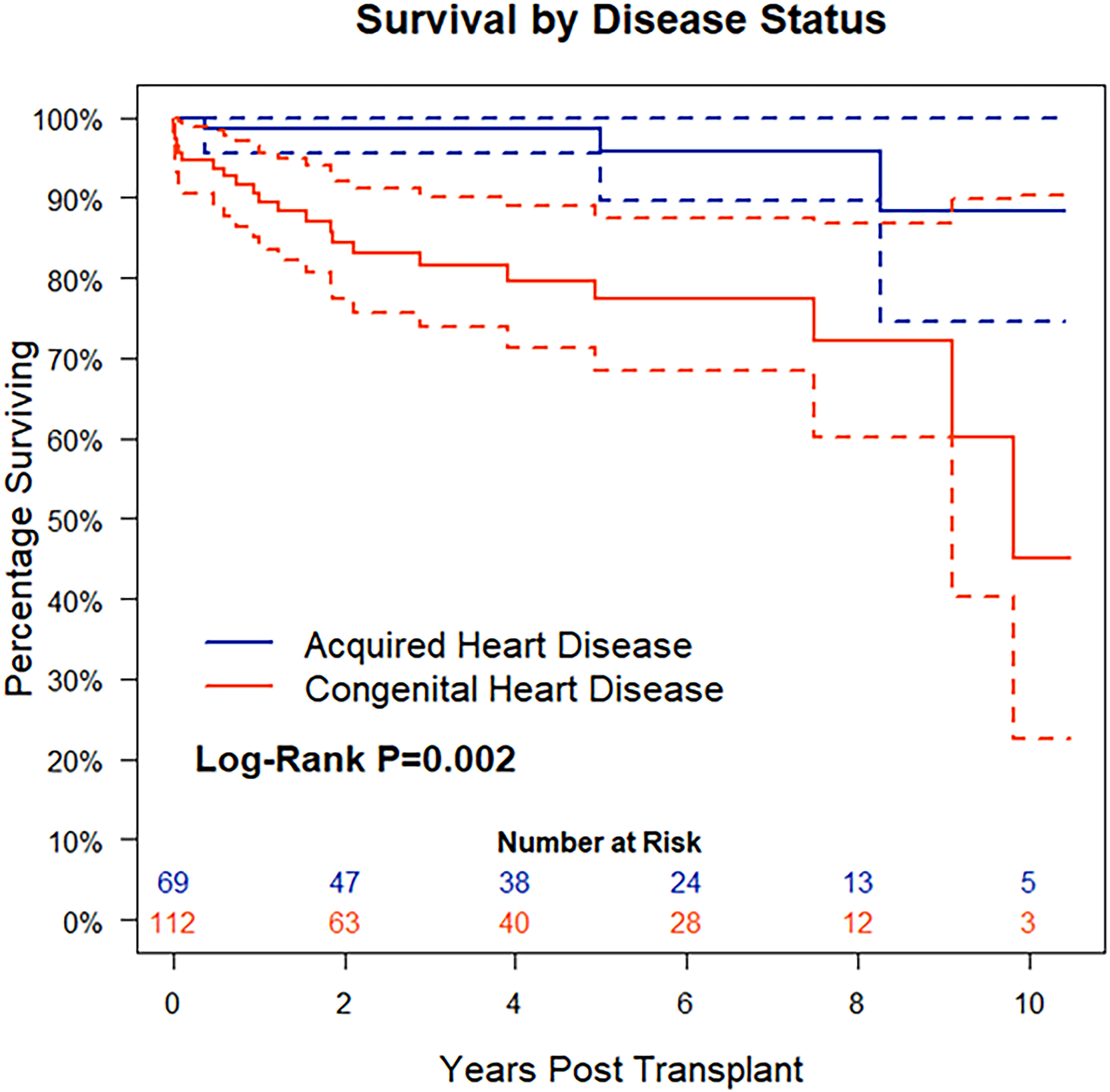
Kaplan-Meier survival curve that documents longitudinal survival with 95% confidence intervals for all 181 patients, comparing patients with acquired heart disease (69/181 = 38.1%) with those with congenital heart disease (112/181 = 61.9%). Survival is significantly worse in congenital heart disease (CHD) (log-rank P = .002).
Univariable Associations with Long-Term Survival.a
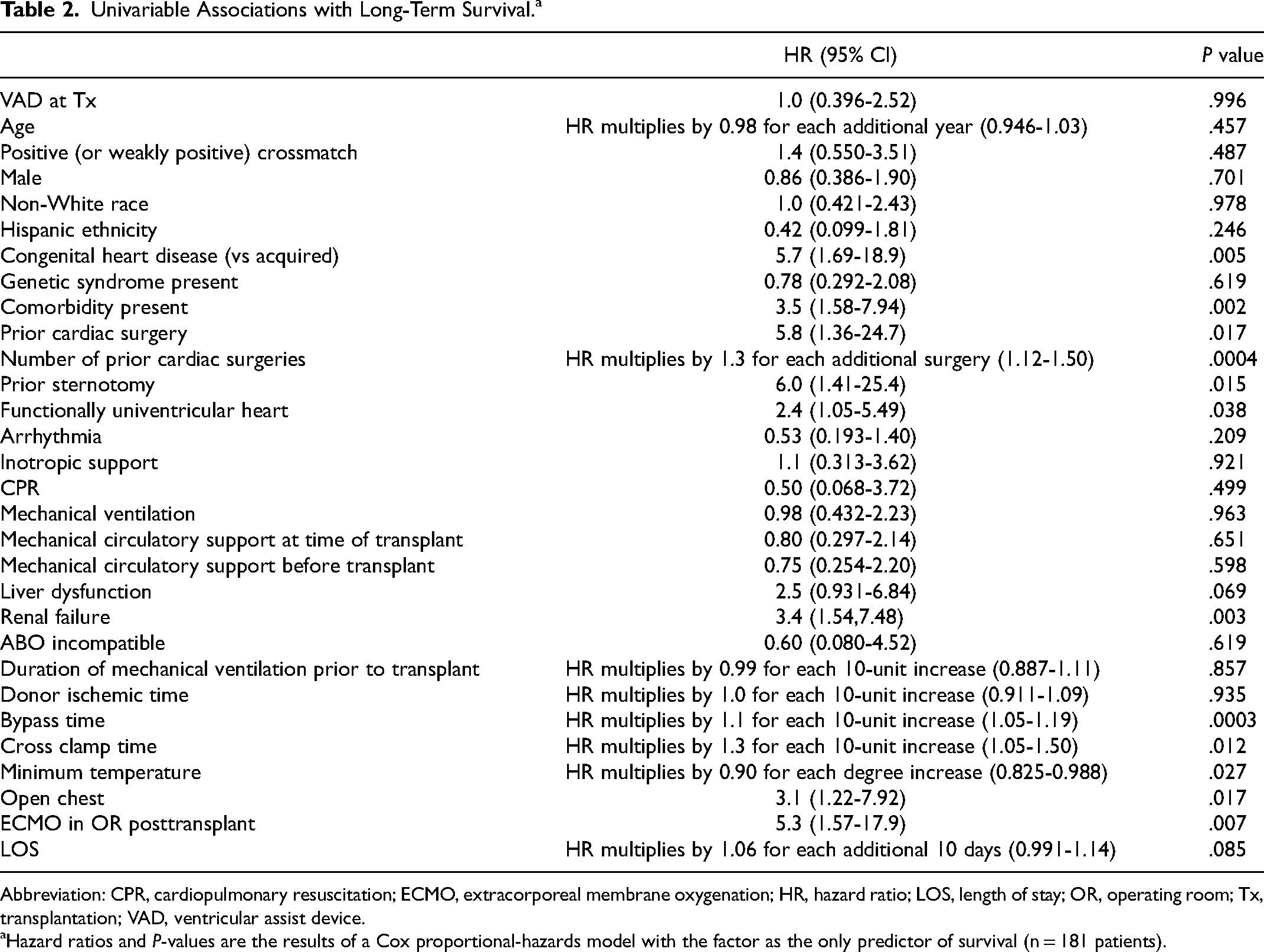
Abbreviation: CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation; HR, hazard ratio; LOS, length of stay; OR, operating room; Tx, transplantation; VAD, ventricular assist device.
Hazard ratios and P-values are the results of a Cox proportional-hazards model with the factor as the only predictor of survival (n = 181 patients).
Multivariable Analyses: Estimated Effect of Congenital Heart Disease Versus Acquired Heart Disease When Controlling for Factors Associated With Survival (n = 181 Patients).
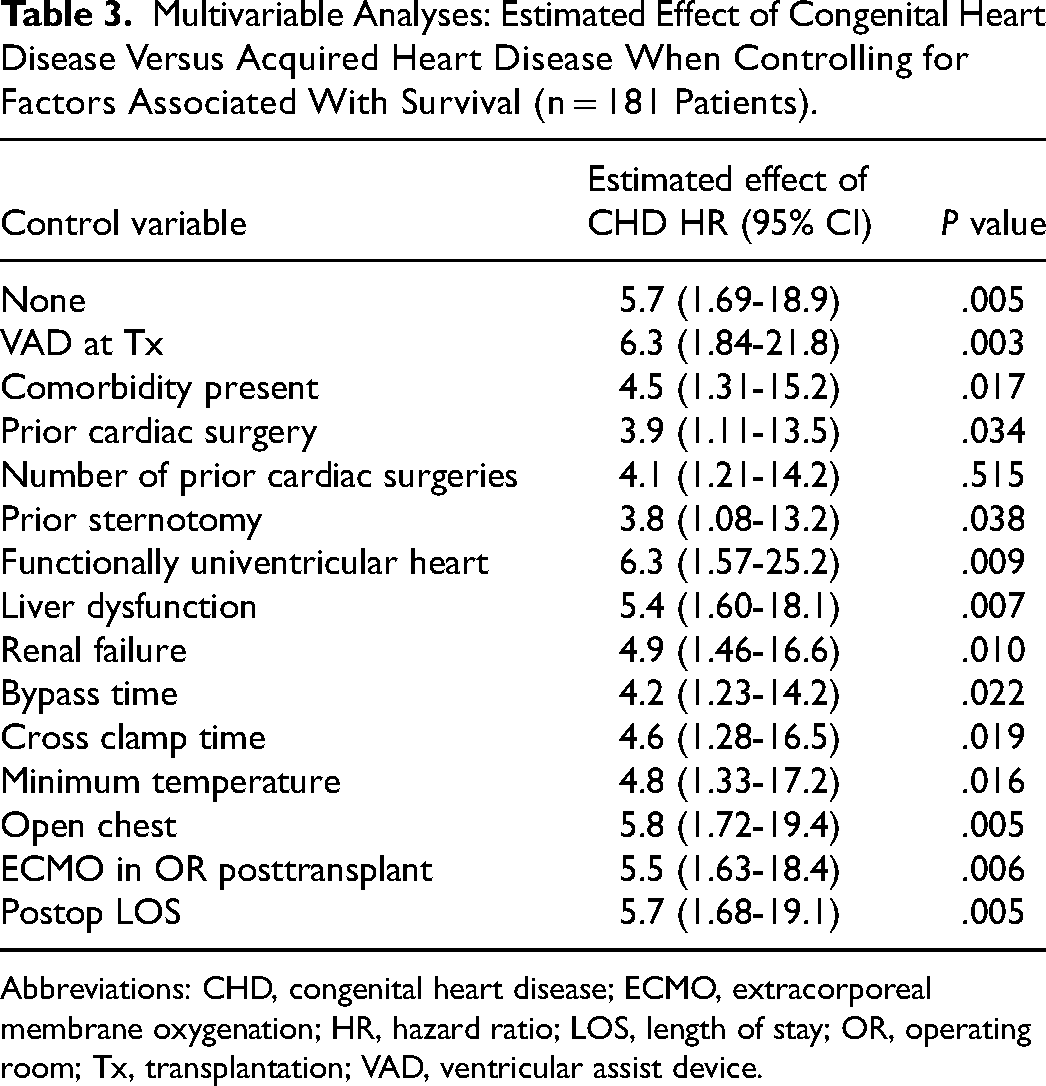
Abbreviations: CHD, congenital heart disease; ECMO, extracorporeal membrane oxygenation; HR, hazard ratio; LOS, length of stay; OR, operating room; Tx, transplantation; VAD, ventricular assist device.
Kaplan-Meier Survival Estimates for All 181 Patients and for those Patients with Acquired Heart Disease (AHD = 69/181 = 38.1%) Versus Congenital Heart Disease (CHD = 112/181 = 61.9%).

Results
This study retrospectively reviews all 181 patients with pediatric and/or CHD who underwent cardiac transplantation at the University of Florida from January 1, 2011, to March 1, 2022, inclusive and compares the outcomes of those with CHD with the outcomes of those with AHD. Congenital heart disease was present in 112/181 = 61.9%. Acquired heart disease was present in 69/181 = 38.1%.
Table 1 documents patient characteristics (n = 181 patients) stratified by disease status (CHD vs AHD). Pretransplant differences included:
Fewer CHD patients were supported with pretransplant VAD: 24/112 = 21.4% versus 27/69 = 39.1%, P = .017 More patients with CHD had prior cardiac surgery: 95/112 = 84.8% versus 35/69 = 50.7%, P < .0001 Congenital heart disease patients had a higher number of prior cardiac surgeries: 2.7 (2.1); 2 [1-4] (0-12) versus 1.4 (1.9); 1 [0-2] (0-8), P < .0001 More CHD patients had univentricular circulation (which is by definition congenital): 89/112 = 79.5% versus 0/69 = 0%, P < .0001 More CHD patients had pretransplant liver dysfunction: 19/112 = 17.0% versus 4/69 = 5.8%, P = .037
Intraoperative differences included:
Congenital heart disease patients had longer bypass time (minutes): 148 (55.2); 137 [113-174] (72-526) versus 108 (40.3); 101 [81-125] (59-300) versus, P < .0001 Congenital heart disease patients had longer cross clamp time (minutes): 85.9 (21.2); 85 [73-100] (49-152) versus 66.3 (14.7); 65 [55-75] (44-106), P < .0001 Congenital heart disease transplants had lower minimum temperature on bypass (°C): 27.4 (4.3); 28 [24-31] (19-34) versus 31.6 (3.1); 32 [31-34] (20-36), P < .0001
Posttransplant differences included:
Posttransplant length of stay (days) was longer in CHD patients: 34.5 (26.8); 27 [19-40] (3-158) versus 29.7 (48.2); 18 [15-26] (0-343), P = .0001
Table 2 provides univariable associations with long-term survival. Hazard ratios and P-values are the results of a Cox proportional-hazards model with the factor as the only predictor of survival (n = 181 patients).
Table 3 provides multivariable analyses and documents the estimated effect of disease status (CHD vs AHD) when controlling for factors associated with survival (n = 181 patients). In multivariable analysis (Table 3), CHD remained a risk factor for mortality after controlling for all variables found to be significant in univariable modeling.
Table 4 provides Kaplan-Meier survival estimates for all 181 patients and for those patients with AHD (69/181 = 38.1%) versus CHD (112/181 = 61.9%). Overall Kaplan-Meier 5-year survival (95% confidence interval [CI]) was 85.8% (80.0%-92.1%). Kaplan-Meier 5-year survival was 98.5% (95.6%-99.9%) in AHD and 77.4% (68.4%-87.5%) in CHD, P < .0001.
Figure 1 is a Kaplan-Meier survival curve that documents longitudinal survival with 95% CIs for all 181 patients. Overall Kaplan-Meier 5-year survival (95% CI) for all 181 patients was 85.8% (80.0%-92.1%).
Figure 2 is a Kaplan-Meier survival curve that documents longitudinal survival with 95% CIs for all 181 patients, comparing patients with CHD (112/181 = 61.9%) versus AHD (69/181 = 38.1%). Survival was significantly worse in CHD (log-rank P = .002).
Discussion
Our single-institution analysis of all 181 patients who underwent cardiac transplantation for pediatric and/or CHD over 11.25 years reveals an overall Kaplan-Meier 5-year survival (95% CI) of 85.8% (80.0%-92.1%). Kaplan-Meier 5-year survival was 98.5% (95.6%-99.9%) in AHD and 77.4% (68.4%-87.5%) in CHD, P < .0001. Longitudinal survival is worse in those with CHD, even after controlling for multiple risk factors. The presence of CHD is a risk factor for mortality after cardiac transplantation. Efforts must be made to understand and mitigate this risk.
While the outcomes of patients with CHD have improved tremendously over the past few decades, these patients continue to be at elevated risk for mortality compared with their counterparts with AHD. In contemporary studies, CHD continues to be identified as a risk factor for mortality in several settings, although survival is improving. Our group previously evaluated the impact of CHD versus AHD on survival after paracorporeal VAD insertion. 17 Among 82 pediatric patients with either CHD (n = 44) or AHD (n = 37), most patients in both groups survived to transplantation (28/44 = 63.6% CHD, 28/37 = 75.7% AHD). Nonetheless, postimplant survival through five years was lower in VAD-supported patients with CHD compared with those with AHD (5-year survival estimate: 55.4% [95% CI = 40.8%-75.2%] in CHD vs 85.3% [95% CI = 74.0%-98.2%] in AHD, P = .002). In that analysis, we concluded that although survival was lower in patients with CHD, “high-risk patients with CHD, including those with functionally univentricular hearts who are suboptimal candidates for conventional palliation or who have failed conventional palliation, can be successfully stabilized with pulsatile VAD insertion while awaiting cardiac transplantation.” While many of these patients were once not salvageable, advances in management have allowed for both VAD support and transplantation of younger, smaller patients with CHD.2,3,13,19 Ultimately, the outcomes of patients with CHD are continuing to improve, although the outcomes have not yet reached those of patients with AHD.
Clearly, the management of patients with CHD entails unique challenges that put them at risk for mortality following several types of interventions, including VAD insertion and cardiac transplantation. Several of these challenges have been described and include prior cardiac surgery, 20 and “abnormalities of the systemic or pulmonary venous return, atrial ‘situs,’ relationship of the great arteries, main or branch pulmonary arteries, ascending aorta and aortic arch, and/or orientation of the ventricular mass.” 17
The finding that CHD remains a risk factor for mortality following cardiac transplantation is not novel; however, contemporary posttransplantt survival in CHD patients compared with that reported in historical literature highlights how higher risk patients are being transplanted without worsened survival. In a global International Society for Heart and Lung Transplantation (ISHLT) analysis of pediatric heart transplants performed between 2000 and 2012, Kaplan-Meier estimated 5-year survival was roughly 80% for patients with CHD ages 6 to 10 years and was roughly 70% for patients with CHD ages 0 to 5 years and 11 to 17 years. 21 In our current analysis, CHD patients had a median age of 4 (IQR 0.5-16) years. As such, their 5-year survival would be expected to be closer to 70% based on this historical international dataset. While the 5-year Kaplan-Meier survival estimate of 77.4% (68.4%-87.5%) in CHD patients in our study represents only a slight improvement from the historical ISHLT analysis when considering mortality alone, contemporary CHD patients are higher risk patients than were previously transplanted over a decade ago. Specifically, at our institution, patients transplanted in the most recent era (2011 through 2022) compared with those transplanted in the previous era (1986 through 2010) were younger and had higher rates of CHD, high PRA, ABO incompatible transplantation, prior sternotomy, prior Norwood operation, prior Fontan operation, and VAD use at the time of transplantation. 3 These findings contextualize the reported survival rate in CHD patients. Although higher risk CHD patients are being transplanted in the current era, longitudinal survival has not worsened.
While our current analysis discusses the transplant outcomes of the global population of patients with CHD, others have evaluated the impact of functionally univentricular CHD versus biventricular CHD on posttransplant survival with differing findings.22–25 Dib and Eberly22,23 and O’Connor and colleagues 24 each performed institutional analyses and found that patients with functionally univentricular CHD had worse posttransplant survival than biventricular patients. In the analysis by Dib and colleagues, 22 149 adult CHD patients who underwent heart transplantation across three institutions between 1988 and 2021 were evaluated. Among 55 patients with univentricular physiology and 94 patients with biventricular physiology, univentricular physiology was associated with increased risk of operative mortality in multivariable analysis (odds ratio, 2.99; 95% CI, 1.33-6.74). Notably, for patients surviving the early posttransplant period, there was no difference in longitudinal mortality between univentricular and biventricular patients (P = .764). O’Connor and colleagues 24 included patients with AHD in their single institutional analysis of 74 pediatric patients who underwent heart transplantation between 2010 and 2016. Congenital heart disease was present in 48.6% of patients. In that analysis, 24 functionally univentricular CHD was a risk factor for longitudinal mortality (HR, 3.2; 95% CI, 1.03-9.5 P = .042), while the categorization of all CHD did not reach significance (HR, 3.2; 95% CI, 0.98-10.4, P = .055). That analysis 24 suggests that functionally univentricular CHD may be the driving factor behind increased posttransplant mortality found in patients with CHD in other studies.
Other studies have also shown that cardiac transplantation followed failed staged palliation.26,27 Particularly in the setting of a previous Fontan operation, higher posttransplant mortality is hypothesized to be due to “longer warm ischemic time required for cardiac reconstruction at the time of transplant, a higher incidence of HLA sensitization (particularly with the use of allograft patch material and/or multiple prior operations), and frequent baseline renal insufficiency.” 27
In contrast to the studies by Dib and Eberly22,23 and O’Connor and colleagues, 24 a registry analysis of the United Network for Organ Sharing and Pediatric Health Information System (PHIS) databases by Riggs and colleagues 25 found that functionally univentricular patients had similar longitudinal survival to biventricular patients with CHD. They included 1517 patients with CHD who underwent heart transplantation between 2006 and 2017, as identified by the PHIS database. Most of these patients had functionally univentricular physiology (67%, n = 1016). Functionally univentricular, biventricular, and indeterminate patients had similar longitudinal survival (log-rank P > .1), and in multivariable analysis, functionally univentricular physiology was not a risk factor for mortality (HR, 0.89; 95% CI, 0.78-1.32, P = .894). Furthermore, a subgroup analysis of Fontan (n = 130) and bidirectional Glenn (n = 185) patients found that survival for both of these groups of patients was equivalent to that of patients with biventricular circulation (log-rank P > .500). Together, these studies suggest that the posttransplant outcomes of CHD patients with functionally univentricular or biventricular circulation differ across institutions. While our current analysis highlights that higher risk patients with CHD are being transplanted while maintaining excellent survival, inferior longitudinal posttransplant survival compared with patients with AHD highlights the need for future subgroup analyses to direct quality improvement. As these studies suggest, analyses of functionally univentricular versus biventricular CHD are necessary, as well as other analyses of specific subsets of patients.
Value of This Analysis
This study highlights that despite transplanting higher risk CHD patients than were previously transplanted years ago, the longitudinal survival of these patients has not worsened, suggesting that the field has progressed to allow transplantation of patients who were previously considered at prohibitive risk. Advances in immunosuppression, desensitization of immunosensitized patients with elevated PRA, immunosurveillance, surgical techniques, and strategies of VAD insertion and VAD management, including anticoagulation while supported with VAD, may help explain these improved outcomes. Nonetheless, despite these improvements, posttransplant survival in CHD patients remains lower than that of AHD patients. While these results are encouraging, they highlight that there is still room for improvement to achieve posttransplant survival in patients with CHD that is equivalent to the posttransplant survival achieved in patients with AHD.
Limitations
Several limitations must be addressed. First, although this series is a relatively large single-institutional experience, this analysis is limited by its small sample size. Second, this is a single-center study and therefore results are not necessarily generalizable.
Conclusion
Our single-institution analysis of all 181 patients who underwent cardiac transplantation for pediatric and/or CHD over 11.25 years reveals an overall Kaplan-Meier 5-year survival (95% CI) of 85.8% (80.0%-92.1%). Kaplan-Meier 5-year survival was 98.5% (95.6%-99.9%) in AHD and 77.4% (68.4%-87.5%) in CHD, P < .0001. Longitudinal survival is worse in those with CHD, even after controlling for multiple risk factors. The presence of CHD is a risk factor for mortality after cardiac transplantation. Efforts must be made to understand and mitigate this risk.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.