
Abstract
Systemic outflow tract obstruction in single ventricle heart disease requires surgical reconstruction to progress through the different stages of palliation. Hypoplastic left heart syndrome and other anatomic variants commonly undergo the Norwood procedure. We describe a double-barrel Norwood operation that can be applied to complex forms of systemic outflow tract obstruction.
Introduction
Systemic outflow tract obstruction in single ventricle physiology usually requires surgical reconstruction in the neonatal peroid. 1 The Norwood operation is common practice for hypoplastic left heart syndrome, 1 or similar pathology with small left-sided structures. Traditional Norwood reconstruction leaves the ascending aorta and transverse arch in continuity with the aortic root, allowing for arch reconstruction and aortopulmonary amalgamation using a piece of patch material (type of patch being institution specific), which has been previously described.1–3 Patients who require a Norwood as the first stage of single ventricle palliation but have complex anatomy that precludes a traditional Norwood because of great vessel orientation or arch sidedness remain a surgical challenge. These include anatomic substrates such as a hypoplastic right aortic arch with normally related great vessels, double inlet left ventricle (DILV), or tricuspid atresia with dextro- or levo-transposition of the great arteries (d-TGA, L-TGA). Traditionally, an arch augmentation in addition to a Damus-Kaye-Stansel type operation, where the pulmonary artery (PA) is divided and sewn end to side into the aorta, has been proposed for these complex anatomic variants, but recurrent arch obstruction can be problematic. 2 Here, we describe the double-barrel Norwood operation, which allows for a symmetrical reconstruction that is reproducible despite challenging, complex anatomy and great vessel orientation.
Results
We have operated on four patients, all with different anatomy: (a) DILV, d-TGA, hypoplastic left aortic arch (HAA-L), and subaortic stenosis (subAS), (b) tricuspid atresia, d-TGA, subAS, and HAA-L (Figure 1), (c) interrupted right aortic arch (type B), ventricular septal defect (VSD), subAS, and normally related vessels; and (d) double outlet right ventricle (DORV), d-TGA, remote VSD, HAA-L, and subAS. Surgical indications for the double-barrel Norwood operation include patients in whom it would be difficult or prohibitive to perform a traditional Norwood-style operation. These include patients with great vessels in a D-TGA or L-TGA orientation, or patients with a hypoplastic right aortic arch with normal great vessel orientation. In our cohort, the most common reason for not being able to perform a traditional Norwood procedure and thus being a candidate for the double-barrel Norwood operation was great vessel orientation (d-TGA, n = 3), and having a hypoplastic right aortic arch with normally related great vessels (n = 1). Additional intraoperative variables, including cardiopulmonary bypass time, cross clamp time, antegrade cerebral perfusion (ACP) time, and postoperative hospital length of stay, are summarized in Table 1.
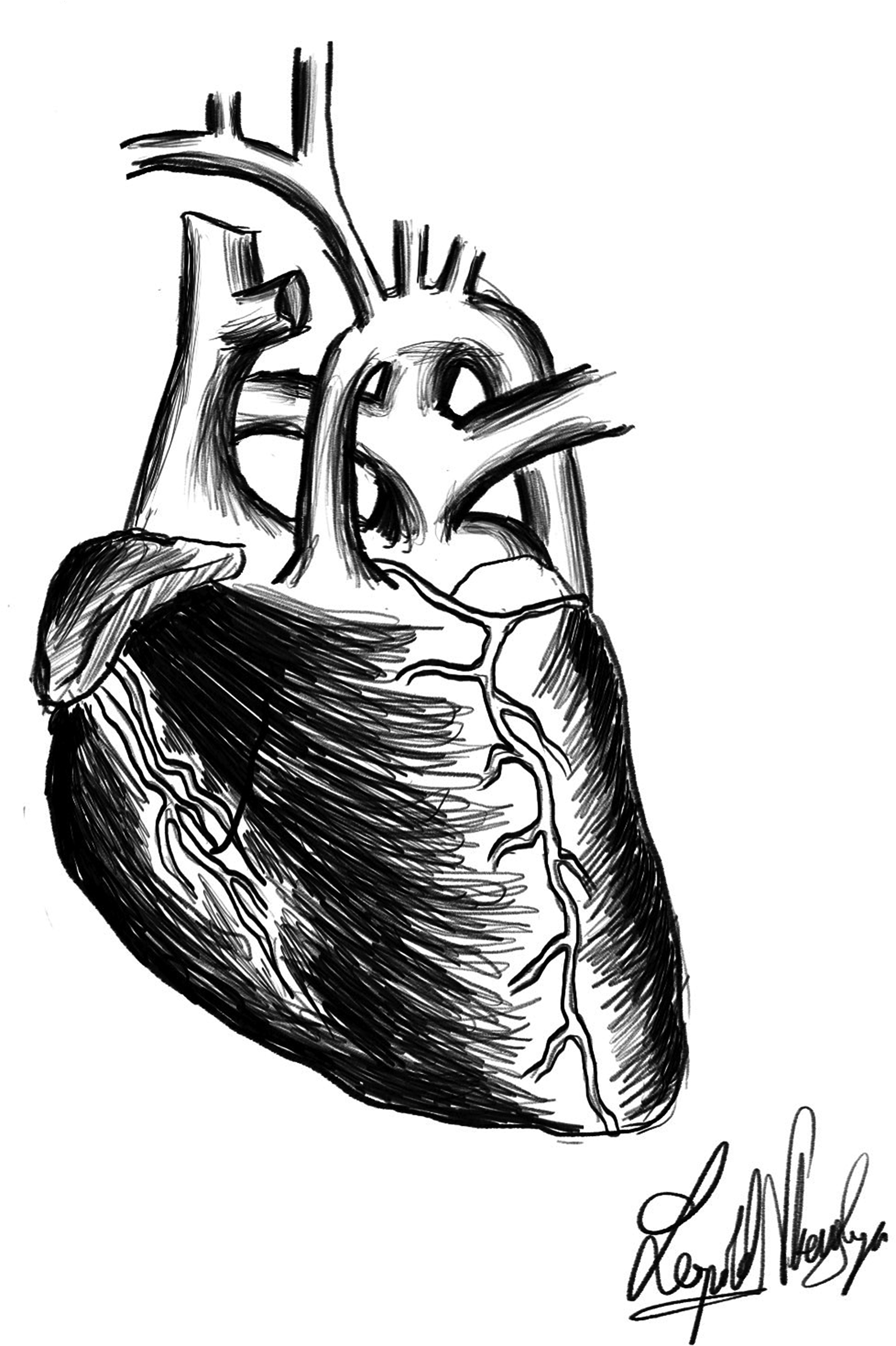
Tricuspid atresia, d-TGA, and hypoplastic aortic arch. Abbreviation: d-TGA, dextro-transposition of the great arteries.
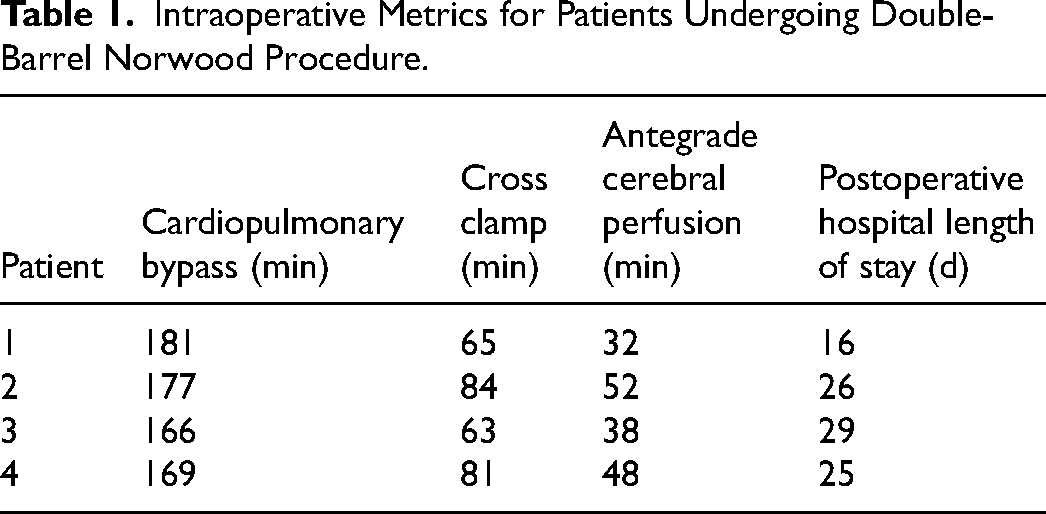
Intraoperative Metrics for Patients Undergoing Double-Barrel Norwood Procedure.
Operative Technique (Double-Barrel Norwood)
The procedure is performed in the neonatal period. Preoperative imaging includes transthoracic echocardiogram (TTE) and a computed tomography angiogram (CTA) scan of the chest to confirm great vessel anatomy. We routinely use selective ACP for cases involving arch reconstruction. The procedure is performed via median sternotomy, and a 3.5 mm Gore-tex graft is sutured to the innominate artery for arterial cannulation. We usually suture the graft on the lateral side of the artery to plan for a modified Blalock-Taussig-Thomas (mBTT) shunt in these nontraditional Norwood-style cases. Routine right atrial cannulation is performed, and the patient is cooled to 20 °C. During cooling, the PAs are mobilized and snared. The aortic arch and head vessels are dissected free from surrounding tissue. Once we are at target temperature, the ductus arteriosus is ligated and divided. The heart is arrested with antegrade cardioplegia. We will use a small antegrade needle in the ascending aorta if it is big enough; otherwise, we will give cardioplegia through the arterial cannula with a short period of deep hypothermic circulatory arrest (DHCA). Once the heart is safely arrested, the cross clamp remains on the ascending aorta, and we continue full cardiopulmonary bypass to the body. Figure 2A shows the aorta and PA are completely transected at the level of the sinotubular junction (STJ). The point at which these great vessels are transected must be at the same level or height, to ensure appropriate orientation during reconstruction. The distal PA confluence is patched with PhotoFix (Artivion) pericardium and if a Sano is to be performed (in RV dominant pathology), we will place the proximal Sano in the RV at this time using the dunk technique. 3 The side wall of the aortic and PA roots adjacent to each other are now sutured together using 7-0 prolene suture, which creates a double-barrel configuration (Figure 2B). A short period of DHCA is undertaken while we perform the atrial septectomy. Next, neuroclips are applied to the head vessels, a Norwood clamp to the descending aorta, and ACP begins (Figure 2B). The arch reconstruction is performed by dividing the isthmus and removing all ductal tissue from the descending aorta and distal transverse arch. An interdigitating technique for arch reconstruction which has been previously described, 3 is performed with PhotoFix (Artivion) pericardium (Figure 3A and B). This continues until the bovine pericardial patch is brought up and around to the transected ascending aorta, completing a reconstructed circle (Figure 4A). This serves as the newly created ascending aorta. The double-barrel neo-root is now brought up to the reconstructed arch and distal ascending aorta, and these two are sutured together in an end to end fashion (Figure 4B). The size of the reconstructed ascending aorta will be slightly smaller than the double-barrel root configuration. This will allow the newly created STJ to not “splay out” helping to keep the semilunar valves competent. The heart is deaired and clamps removed. Full flow bypass is reinstituted, and the patient is rewarmed to 36 °C while the distal Sano or mBTT shunt is completed. If a mBTT shunt is performed, prior to reinstituting full flow bypass, a short period of DHCA is used to move the arterial cannula to the ascending aorta. The patient is weaned from bypass, and the chest left open per our institution's protocol. Figure 5 shows the completed double-barrel Norwood.
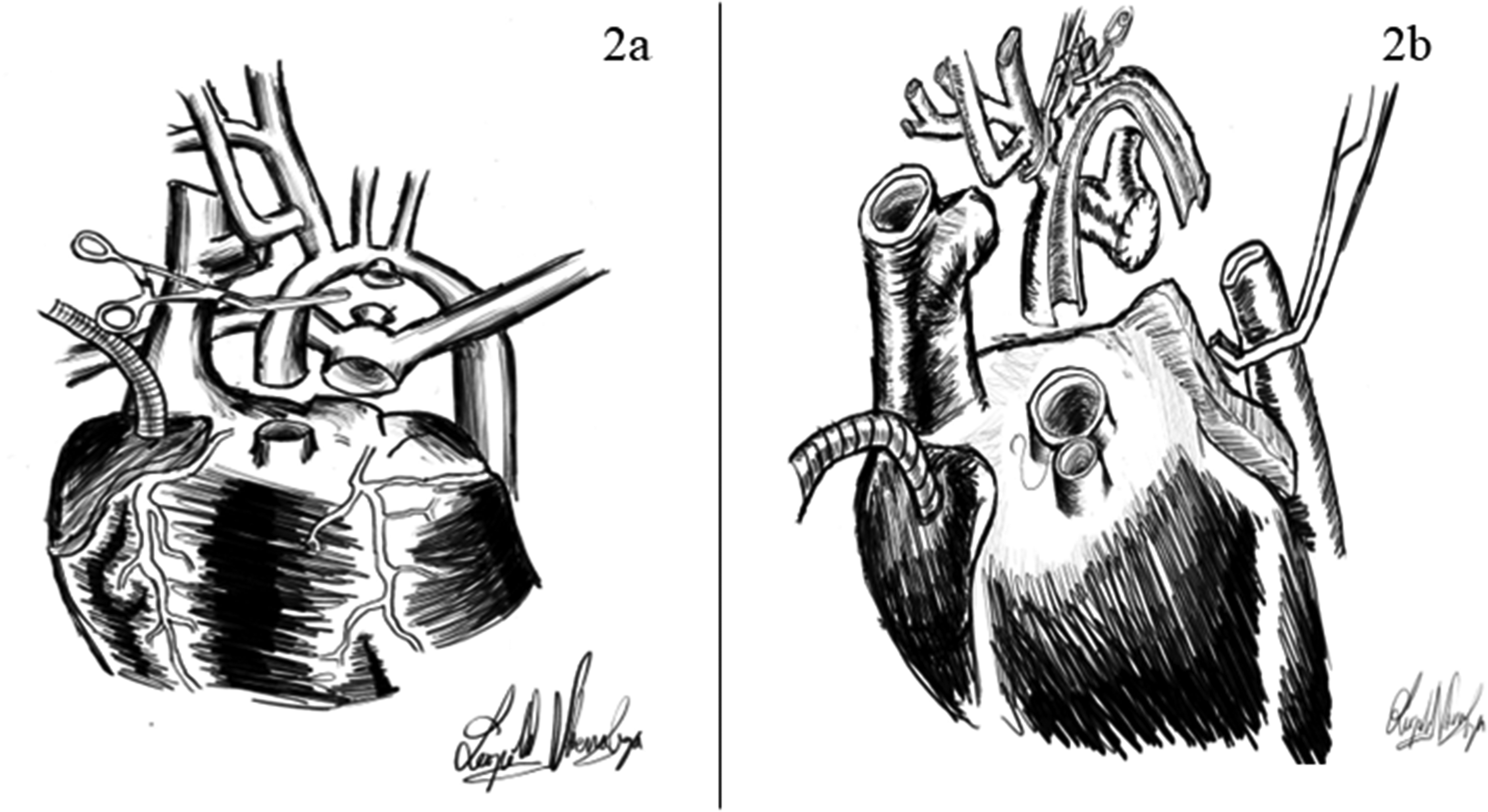
Surgical steps for a double-barrel Norwood repair. (A) The aorta and pulmonary artery (PA) are transected at the level of the sinotubular junction. (B) The sidewalls of the aortic and PA roots are anastomosed creating a double-barrel configuration. The distal PA is patched with pericardium. Next, neuroclips are applied to the head vessels, a Norwood clamp placed on the descending aorta, starting antegrade cerebral perfusion (ACP) and the arch reconstruction.
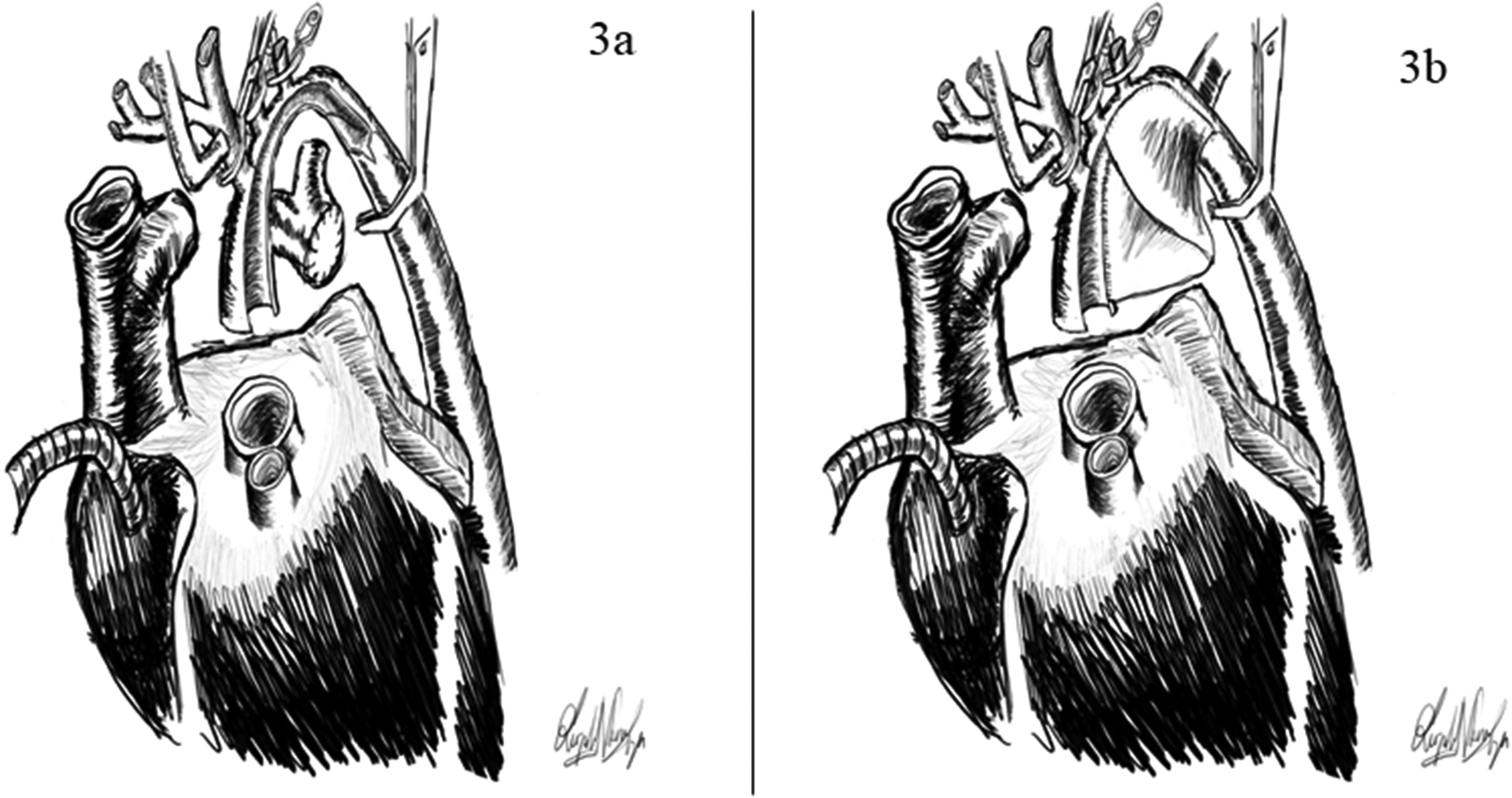
Surgical steps for a double-barrel Norwood repair. (A and B) Isthmus is divided and ductal tissue removed from the descending aorta and distal transverse arch; an interdigitating technique with Photofix pericardium is used to complete the arch reconstruction.
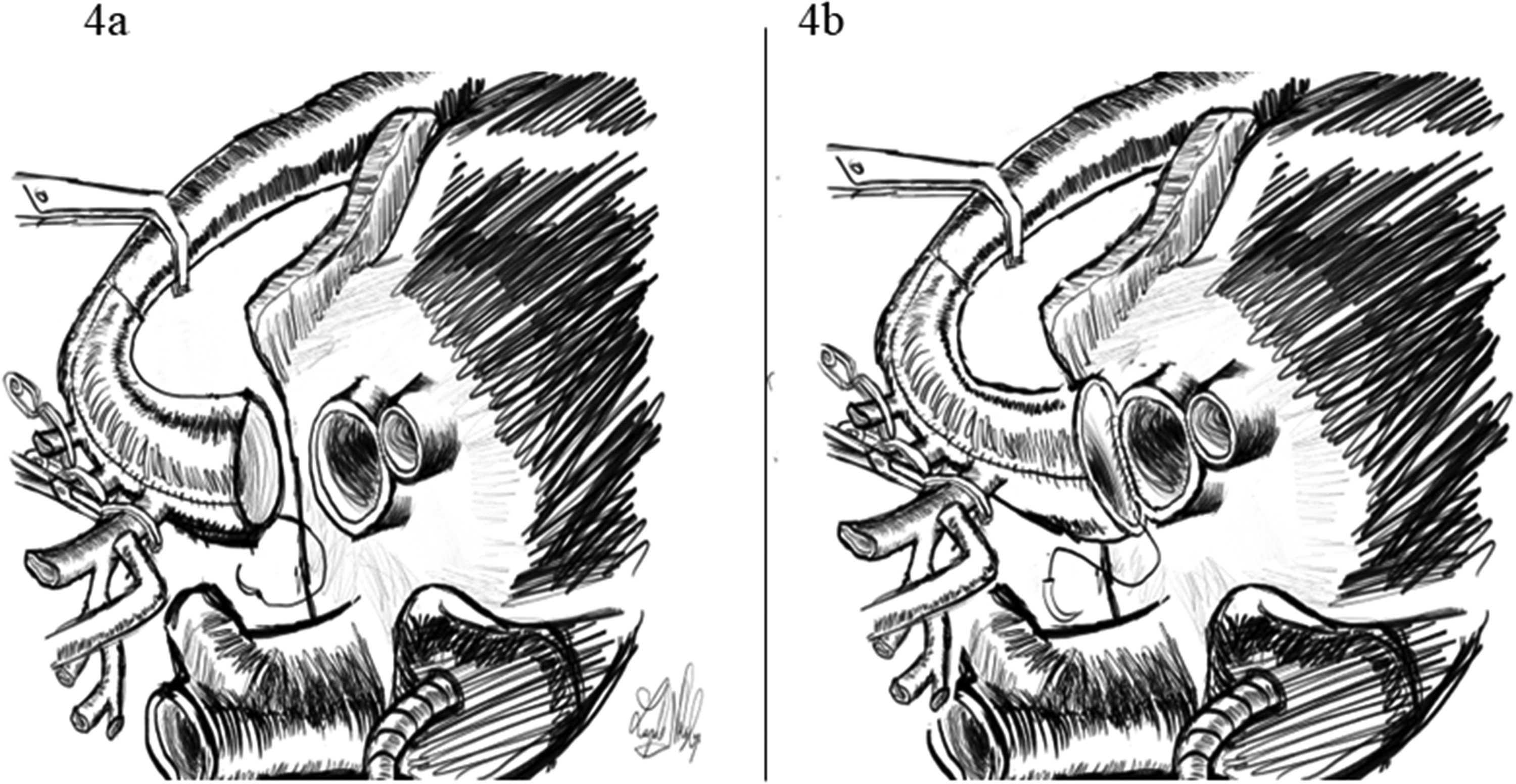
Surgical steps for a double-barrel Norwood repair. (A) The arch reconstruction is finalized by suturing the pericardial patch around until reaching the edges of the transected ascending aorta, completing a reconstructed circle. (B) The double-barrel neo-root is anastomosed with the distal ascending aorta.
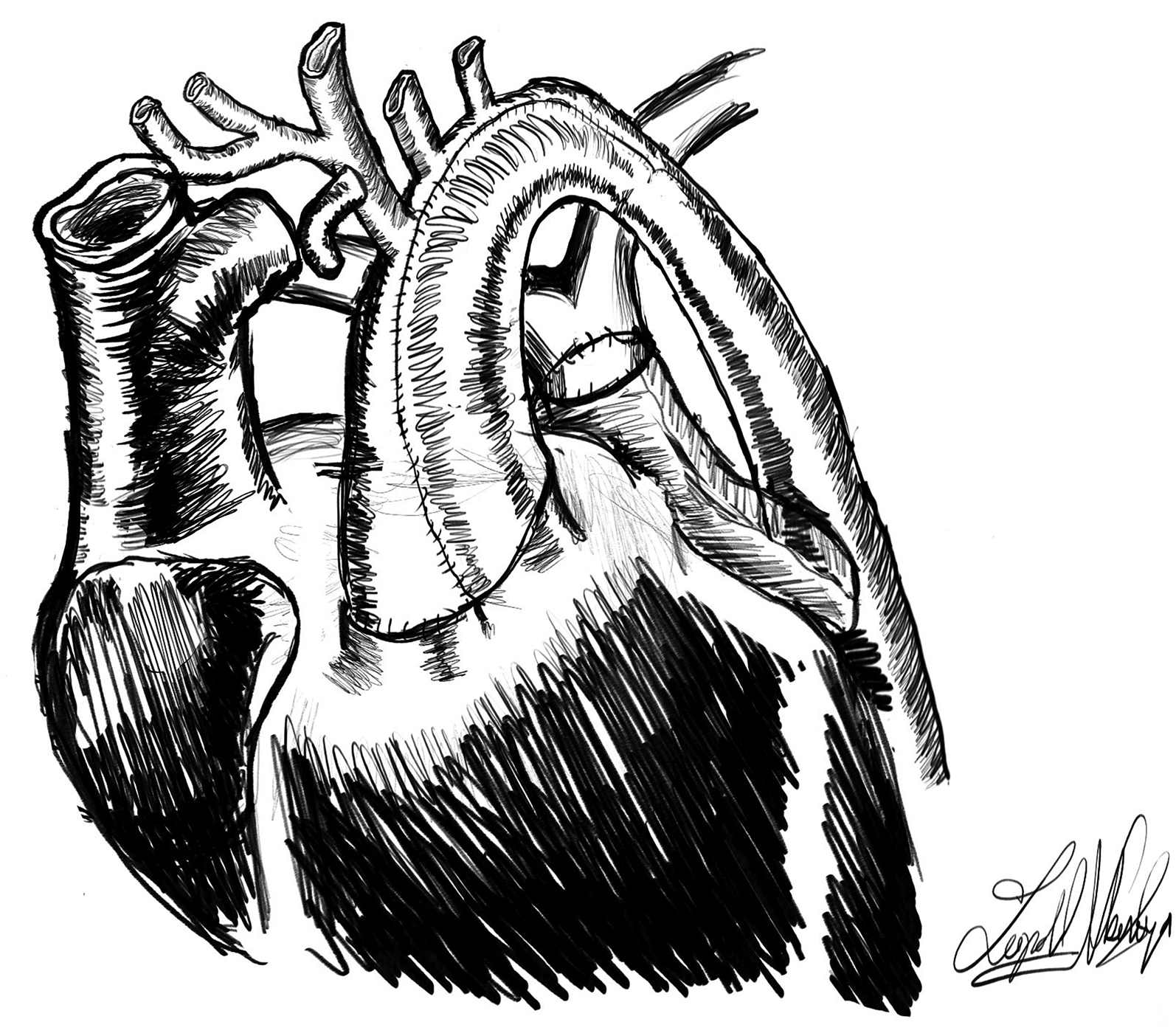
Completed double-barrel Norwood.
Follow-Up
All patients are alive and well at last follow up. Most recent postoperative echocardiograms demonstrate good ventricular function and no arch obstruction. Three patients have undergone second-stage palliation with a bidirectional Glenn procedure and discharged home in good condition. The other patient is alive awaiting bidirectional Glenn as second-stage palliation.
Conclusion
Surgical reconstruction for complex systemic outflow tract obstruction in single ventricle physiology can be challenging. The double-barrel Norwood can be applied in many cases where a traditional Norwood may be difficult or prohibitive. The technique is reproducible, and short-term results are satisfactory.
Footnotes
Authors’ Note
Central Message: Double-barrel Norwood offers a reproducible option for complex outflow tract obstruction in single ventricle cases, with satisfactory short-term outcomes when traditional methods fail. Central Picture Legend: Double Barrel Norwood Procedure for Complex Systemic Outflow Tract Obstruction.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This protocol was approved, and consent for this study was waived by our IRB under exempt category 4 (IRB-300014346).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.