
Abstract
Introduction
Organ transplantation has long been limited by a shortage of donor organs, resulting in high waitlist mortality and driving the transplant community to explore innovative ways to expand the donor pool. 1 One strategy is the use of ABO-incompatible (ABO-I) allografts in pediatric recipients. Historically, ABO incompatibility was considered a contraindication for transplantation due to the high risk of graft rejection and other complications. However, in the early 1990s, Dr West and the team at SickKids revolutionized this notion by successfully performing 10 ABO-I heart transplants (HTs) in newborns with congenital heart defects.2,3 By leveraging the immunologic immaturity of infants, who lack isohemagglutinins to A/B blood group antigens, they achieved an 80% survival rate, providing the first evidence that ABO-I transplantation could be a viable option for reducing mortality among pediatric patients waiting for a HT. 3
Subsequent studies, including those from the Pediatric Heart Transplant Society registry, have further demonstrated that survival rates and freedom from rejection for ABO-I heart recipients are comparable with those of ABO-compatible (ABO-C) heart recipients.4–6 Despite these promising outcomes, Henderson and colleagues found that ABO-I transplants still represented less than a fifth of total HTs performed. 5 As such, on July 7, 2016, the United Network for Organ Sharing (UNOS) implemented updates to the heart allocation policy for pediatric HT candidates, including an expansion of the criteria for ABO-I transplants, by extending ABO-I HT eligibility to include candidates listed before two years of age and providing equal allocation priority to those under one year of age. 7
While prior studies have analyzed the impact of the 2016 policy change on waitlist survival for pediatric HT candidates overall,8,9 there remains a paucity of studies examining the landscape of ABO-I HT specifically. Moreover, UNOS introduced a new policy update in 2023, further expanding eligibility for ABO-I HT in pediatric patients by extending the eligible age of listing to 18 years old and expanding to a lower urgency for all children (Status 2). 10 However, despite these policy changes, ABO-I allograft offers remain classified as secondary blood type offers for all candidates ≥1 year of age, resulting in decreased likelihood of an ABO-I offer for those candidates, despite having been listed as willing to accept an ABO-I allograft. It is therefore crucial to assess the present state of ABO-I HT, as this analysis provides a detailed assessment of current utilization trends, includes two years of data following the 2023 policy change, and will provide a baseline with which to evaluate the future impact of the 2023 policy change on both transplant accessibility and clinical outcomes.
This study therefore aims to examine the trends and outcomes in pediatric HT over the past 16 years, with a particular emphasis on ABO-I transplants in the pre- and post-2016 policy eras.
Methods
Data Source
Data were obtained and analyzed from the Organ Procurement and Transplantation Network (OPTN) database, which contains comprehensive information on all donors, candidates on the waitlist, and transplant recipients across the United States. The OPTN is managed under the guidance of the Health Resources and Services Administration and the U.S. Department of Health and Human Services. Because the OPTN registry contains deidentified data, this study was exempt from full review by the Institutional Review Board at the University of Colorado Anschutz Medical Center.
Study Population
All patients who were listed for HT at ≤2 years of age between July 2008 and July 2024, and who had follow-up through March 2025, were identified in the OPTN database. Patients undergoing repeat or multiorgan transplantation were excluded from the analysis, as were those with missing data. Based on the ABO compatibility of the recipient and the donor as reported within the OPTN, the study population was divided into ABO-I and ABO-C groups.
Study Eras and Endpoints
The primary outcome of interest was posttransplant survival. Survival was defined as the interval from transplant to death. Patients who were alive on March 31, 2025, were censored at the date of last known follow-up. To account for changes in the UNOS organ allocation policy, the study period was divided into two eras: July 7, 2008, to July 7, 2016, and July 8, 2016, to July 8, 2024. 7
To evaluate the impact of transplant center volume on outcomes, we conducted a volume-based analysis limited to the modern era (post-2016) to ensure alignment with contemporary practice patterns. Centers were stratified into quartiles based on their total pediatric (age ≤ 2) HT volume, with centers in the top quartile being classified as high-volume centers (HVCs); these centers performed ≥35 transplants between July 2016 and July 2024. The remaining centers were classified as non-HVCs.
Statistical Analysis
Continuous variables are reported as means with standard deviation if normally distributed and otherwise as medians with interquartile range. Categorical data are presented as group proportions. The Mann-Whitney U, 2-sided Student t, and Pearson χ2 tests were used to compare the significance of intergroup differences between groups, as appropriate.
For survival analyses, Kaplan-Meier estimates were generated and graphically represented for each cohort. Cox proportional hazards models were used to calculate the risk-adjusted hazard of posttransplant mortality (hazard ratio [HR]), with associated 95% confidence intervals (CIs). All analyses included adjustment for donor and recipient characteristics; covariates included recipient age, donor and recipient race, intensive care unit (ICU) admission status, ventilator dependence, extracorporeal membrane oxygenation (ECMO) prior to transplant, history of prior cardiac surgery, functional status, and UNOS status.
All statistical analyses were performed using Stata version 18.5 software (StataCorp. College Station, TX). For all analyses, a two-sided P-value less than .05 was considered statistically significant.
Results
Over the study period, a total of 2,770 children listed at age ≤ 2 years underwent HT, of whom 2,277 (82%) comprised the ABO-C group and 493 (18%) comprised the ABO-I group. The percentage of ABO-I pediatric HT increased from 10% in 2008 to 21% in 2016, to a peak of 28% in 2019 (Figure 1).
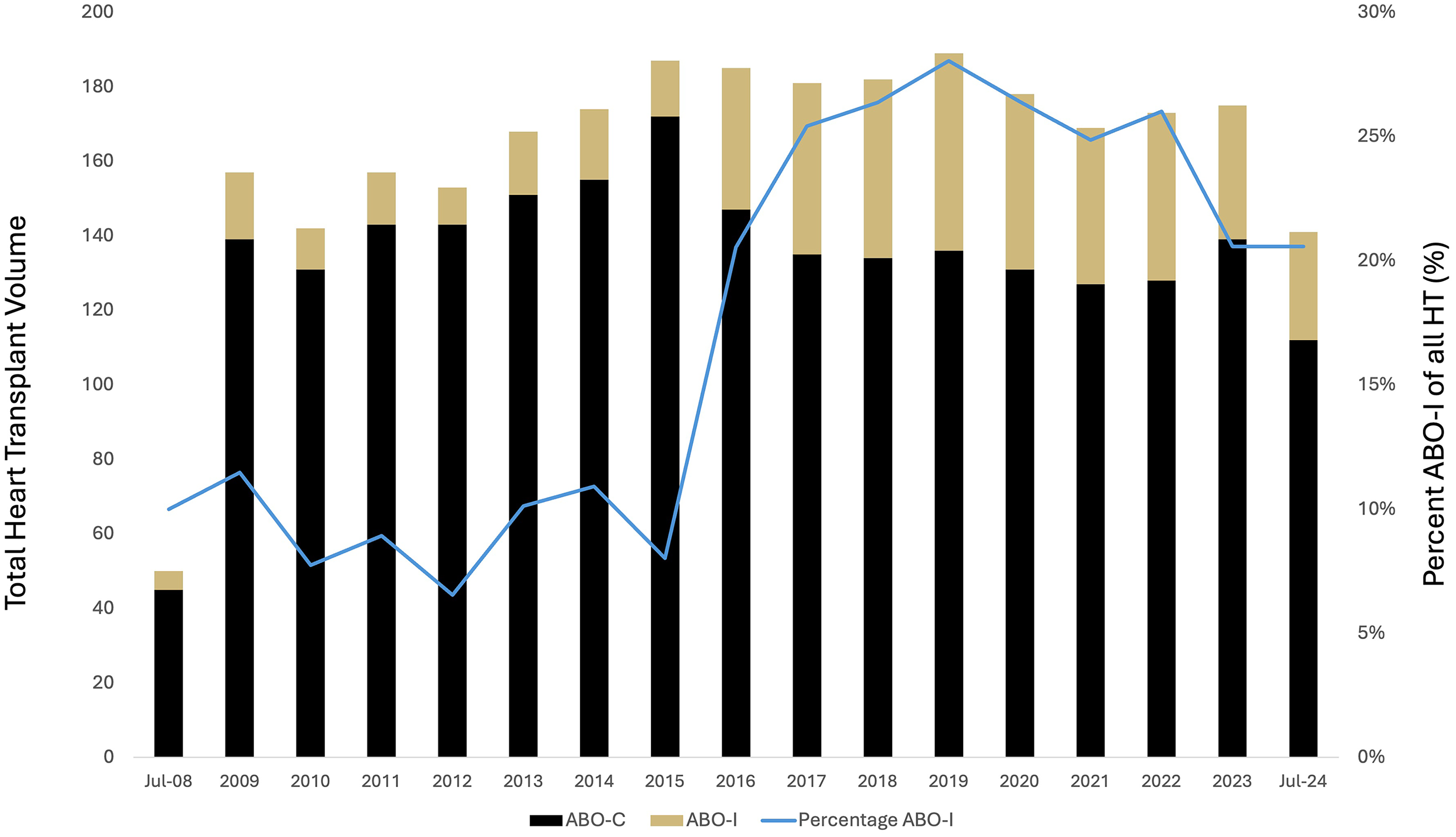
Trends in ABO-compatible (ABO-C) and ABO-incompatible (ABO-I) pediatric heart transplant (HT).
Between 2008 and 2016, ABO-C recipients compared with ABO-I recipients had a similar distribution of sex (47.7% [557/1167] vs 45.1% [55/122]) female, P = .35) and race (all categories P > .05), but they more often presented with ventilator dependence (39.9% [466/1167] vs 58.2% [71/122], P < .001) and were more frequently admitted to the ICU prior to transplantation (83% vs 63%, P < .001).
Between 2016 and 2024, the ABO-I cohort demonstrated a similar distribution of sex compared with the ABO-C group (44.5% [165/371] vs 48.1% [534/1110], P = .26) and race (all categories P > .05). However, ventilator dependence remained more common in the ABO-I group during this period (37.7% [140/371] vs 31.2% [346/1110], P = .02), as did pretransplant ICU admission (73.1 [271/371] vs 64.3 [714/1110], P = .002). A detailed summary of recipient demographics and clinical characteristics for each cohort can be found in Table 1.
Recipient Characteristics, Stratified by ABO Donor-Recipient Compatibility Status (ABO-C vs ABO-I) and Transplant Era (2008-2016 and 2016-2024).
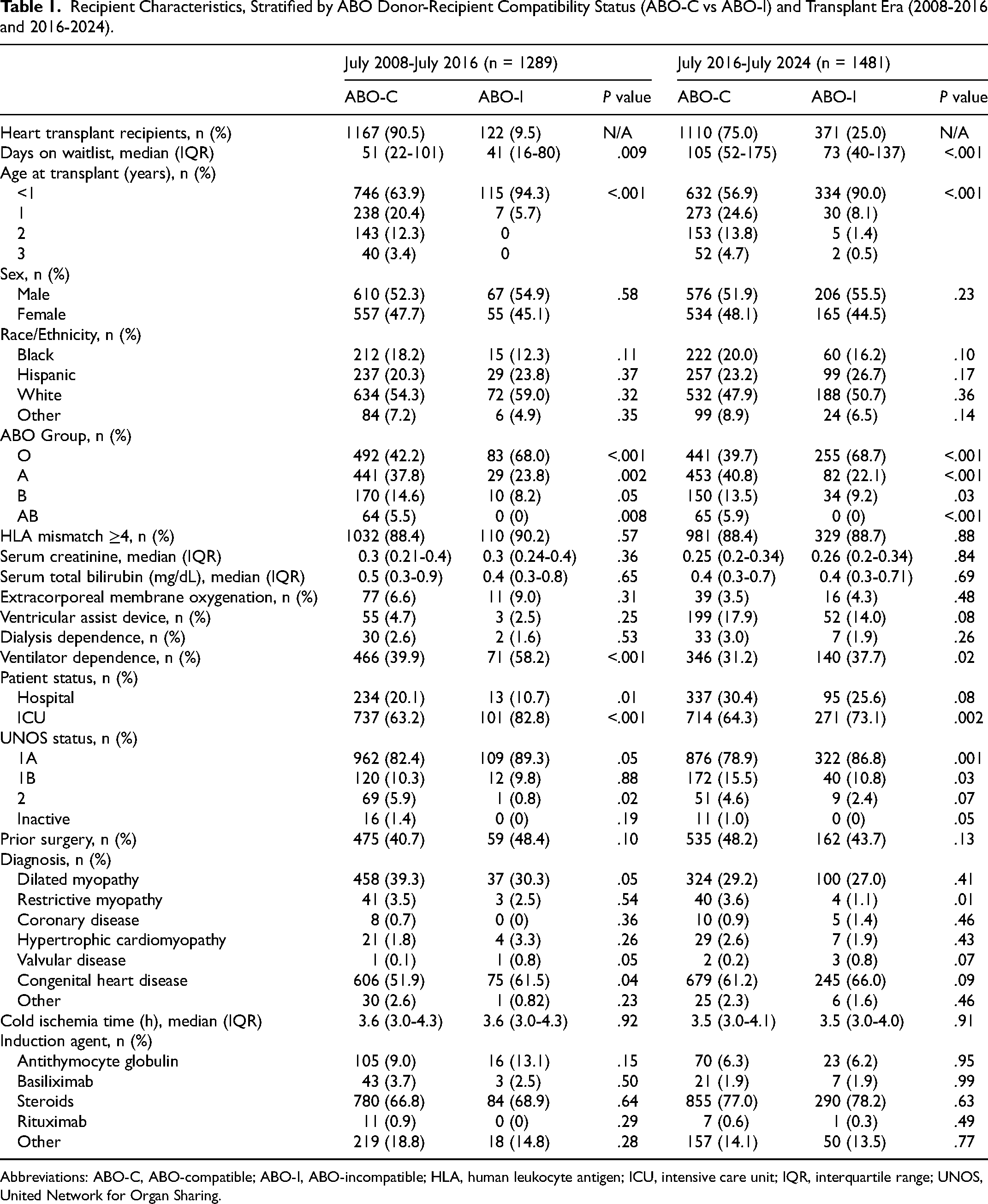
Abbreviations: ABO-C, ABO-compatible; ABO-I, ABO-incompatible; HLA, human leukocyte antigen; ICU, intensive care unit; IQR, interquartile range; UNOS, United Network for Organ Sharing.
A total of 2,115 (55%) patients listed for HT across the study period were listed as willing to receive an ABO-I allograft. After adjusting for recipient characteristics, one-year waitlist mortality for these candidates remained similar before and after the 2016 UNOS policy change (HR 0.70, CI 0.48-1.02, P = .07). In those transplanted, ABO-I recipients in the pre-2016 era spent an average of 41 days on the waitlist, versus those transplanted in the post-2016 era, who spent an average of 73 days on the waitlist (P < .001) (Table 1). Additional sensitivity analysis for waitlist mortality for only those candidates <1 year old was conducted; waitlist mortality was comparable across eras (HR 0.77, CI 0.55-1.07, P = .12).
On unadjusted survival analysis, patients in the ABO-I cohort had inferior one- (85% vs 89%) and five-year survival (73% vs 82%) compared with ABO-C recipients undergoing transplantation between 2008 and 2016 (log-rank P = .02). However, after risk-adjustment, there was no difference in one- (HR 1.13, CI 0.67-1.91, P = .65) or five-year survival (HR 1.45, CI 0.97-2.17, P = .07) between the groups (Figure 2A). For ABO-I patients undergoing HT between 2016 and 2024, unadjusted survival analysis demonstrated no difference in one- (90% vs 90%) and five-year survival (82% vs 80%) compared with ABO-C patients (log-rank P = .55). Following risk-adjustment, ABO-I maintained comparable one- (HR 0.88, CI 0.59-1.32, P = .54) and five-year survival (HR 0.84, CI 0.61-1.15, P = .27) with the ABO-C cohort (Figure 2B). Additionally, across the study period, ABO-I patients experienced comparable rates of postoperative stroke, graft nonfunction, and acute rejection. Full postoperative outcomes for both cohorts can be found in Table 2.
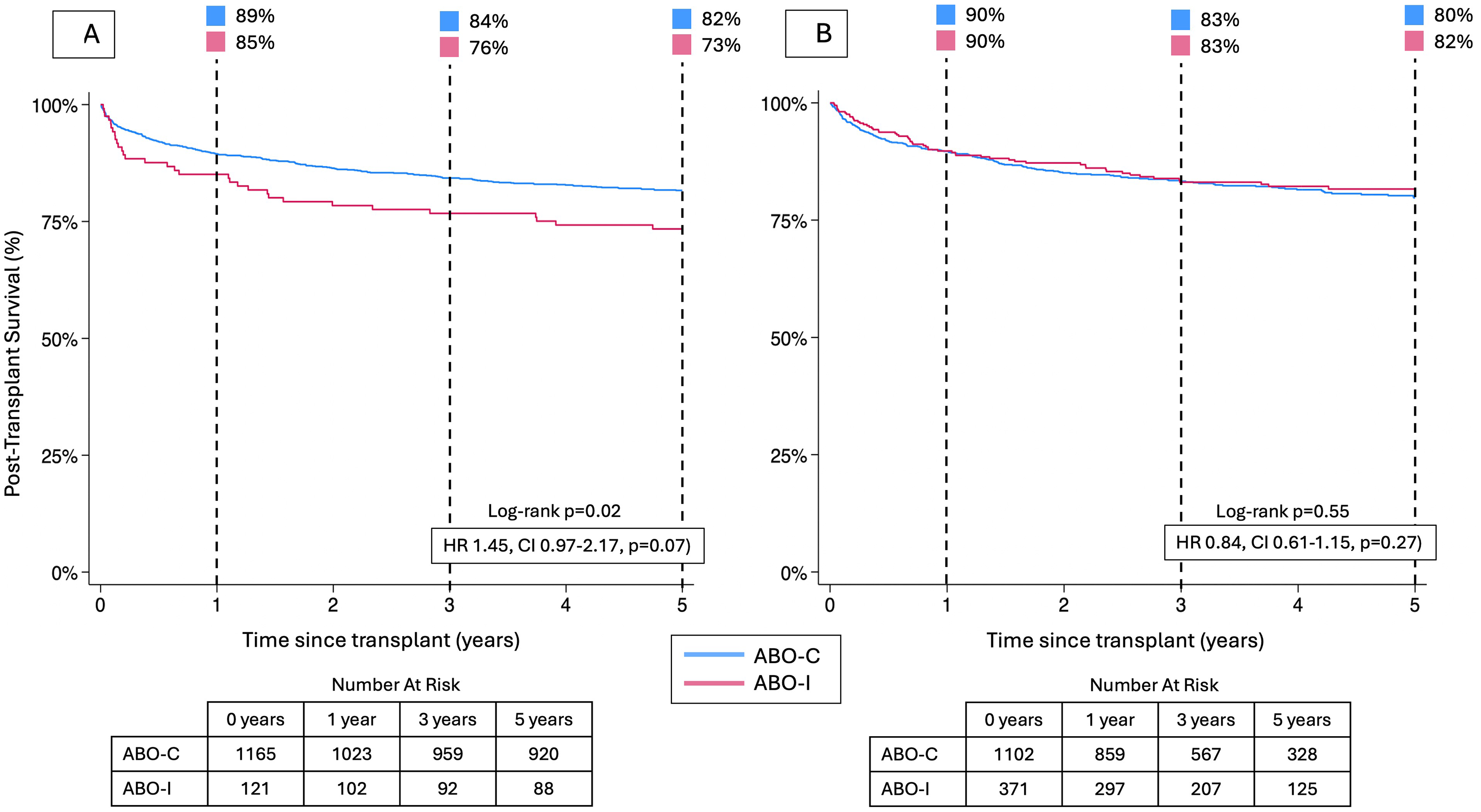
Five-year posttransplant survival between ABO-compatible and ABO-incompatible pediatric heart transplant recipient cohorts between 2008 and 2016 (A), and 2016 to 2024 (B). ABO-C, ABO-Compatible; ABO-I, ABO-Incompatible; HR, hazard ratio; 95% CI, 95% confidence interval.
Secondary Outcomes for All Recipients, Stratified by ABO Compatibility Status (ABO-C vs ABO-I) and Transplant Era (2008-2016 and 2016-2024).
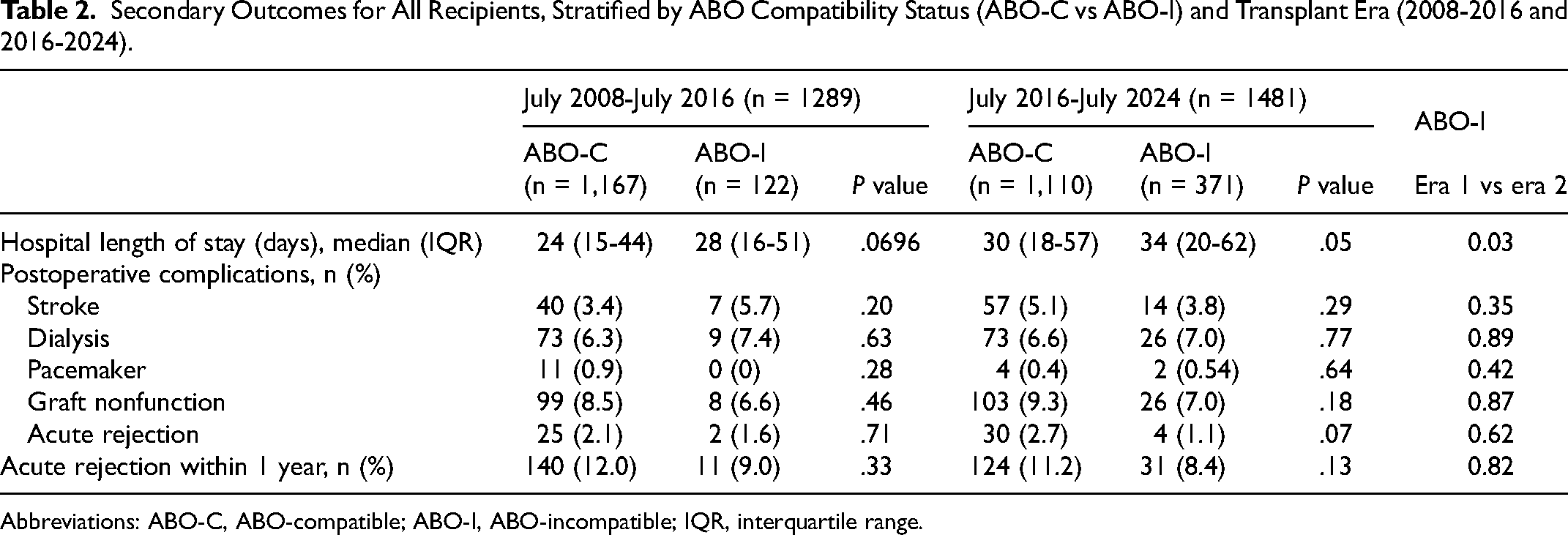
Abbreviations: ABO-C, ABO-compatible; ABO-I, ABO-incompatible; IQR, interquartile range.
Regression analysis identified pretransplant serum creatinine >1 mg/dL (HR 2.86, CI 1.29-6.31, P = .009), pretransplant ECMO (HR 2.26, CI 1.51-3.38, P < .001), and history of prior cardiac surgery (HR 1.72, CI 1.32-2.24, P < .001) as predictors of one-year posttransplant mortality for patients undergoing HT between 2008 and 2016. For ABO-I recipients between 2016 and 2024, a higher pretransplant serum total bilirubin (HR 1.05, CI 1.02-1.07, P < .001), pretransplant ECMO (HR 1.95, CI 1.02-3.71, P = .04), and a history of prior cardiac surgery (HR 2.39, CI 1.65-3.45, P < .001) were associated with increased risk of death in the first posttransplant year.
In the post-policy change period, 63 transplant centers performed ABO-I transplantation. Of those, 24% (n = 15) were defined as HVCs. HVCs performed 83% (n = 307/371) of the ABO-I HTs between 2016 and 2024 (Figure 3). Of all transplants done at HVCs, ABO-I comprised 26% of HT compared with 20% of HT at non-HVCs (Figure 4).
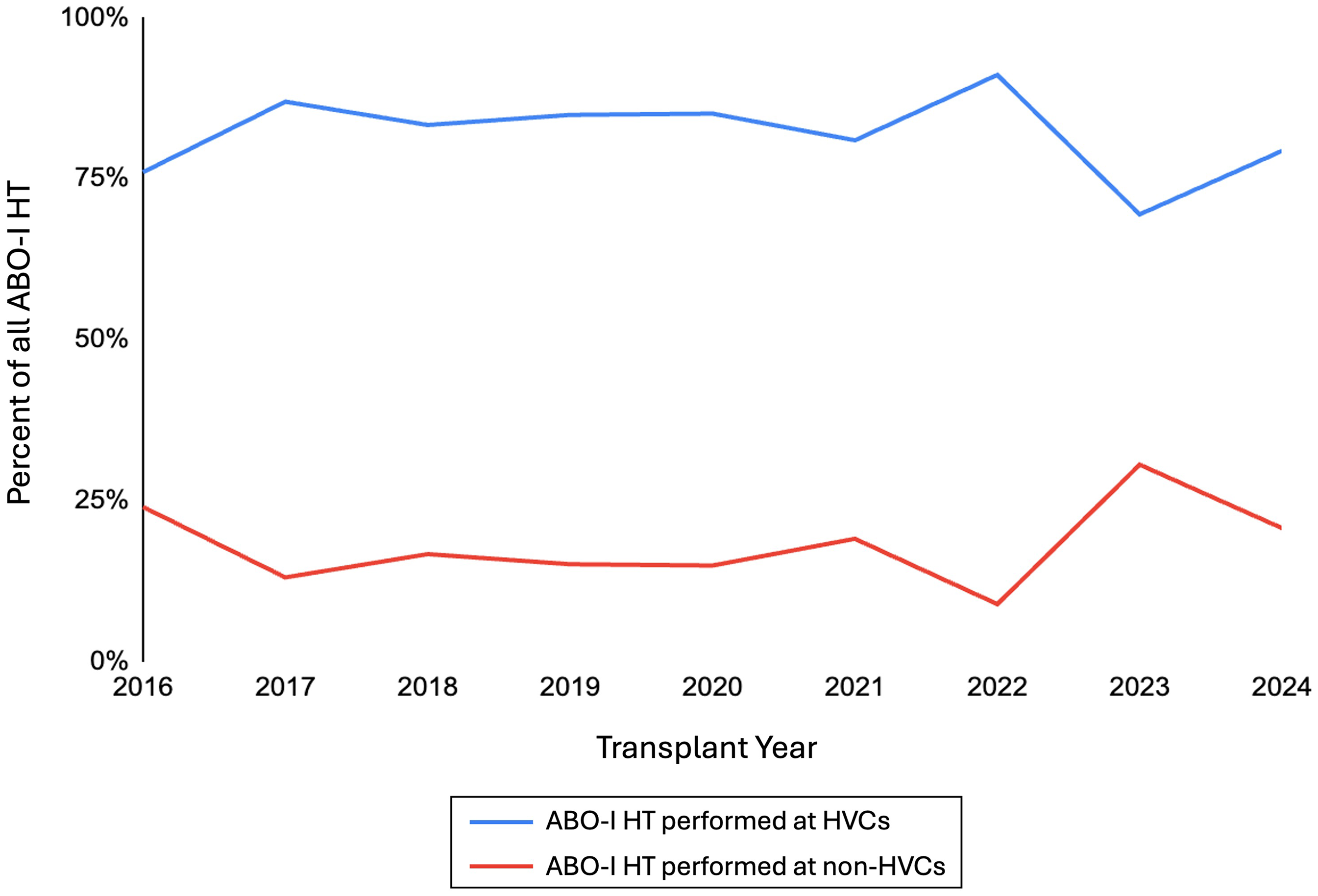
Percent of ABO-incompatible (ABO-I) heart transplants performed at high-volume centers (HVCs) versus non-high-volume centers (non-HVCs), by year, in the post-2016 policy change era.
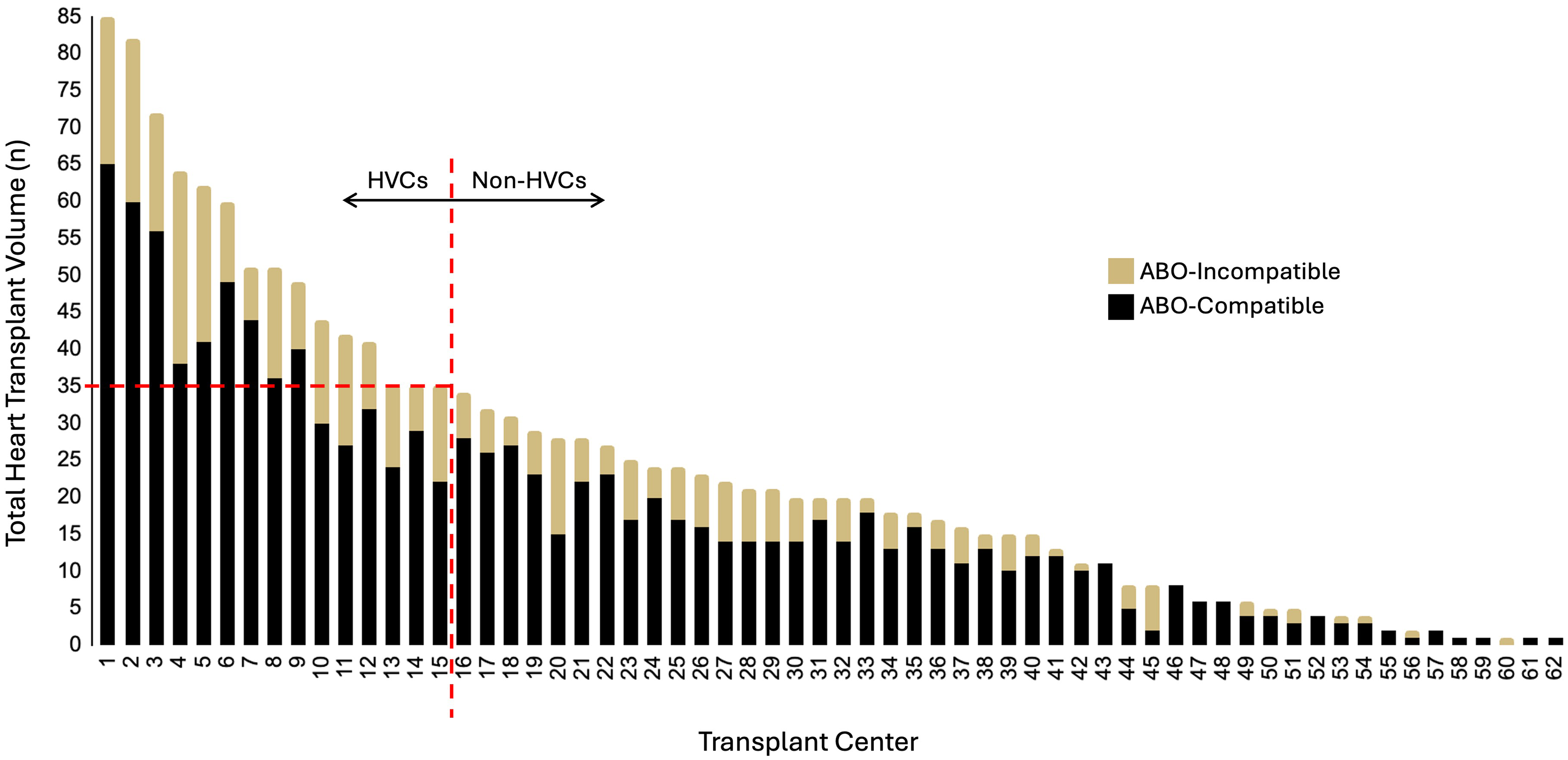
ABO-Incompatible and ABO-compatible (ABO-C) heart transplant volume in the post-2016 policy change era, by transplant center. High-volume centers (HVCs) and non-HVCs are delineated by total pediatric heart transplant volume ≥35 transplants over the study period. Transplant centers are shown with unique, deidentified codes.
Unadjusted survival for ABO-I recipients at HVCs was 90% at one-year compared with 89% at non-HVCs (log-rank P = .60). On adjusted analysis, one-year survival between HVCs and non-HVCs was also comparable (HR 0.87, CI 0.43-1.76, P = .69) (Figure 5A).
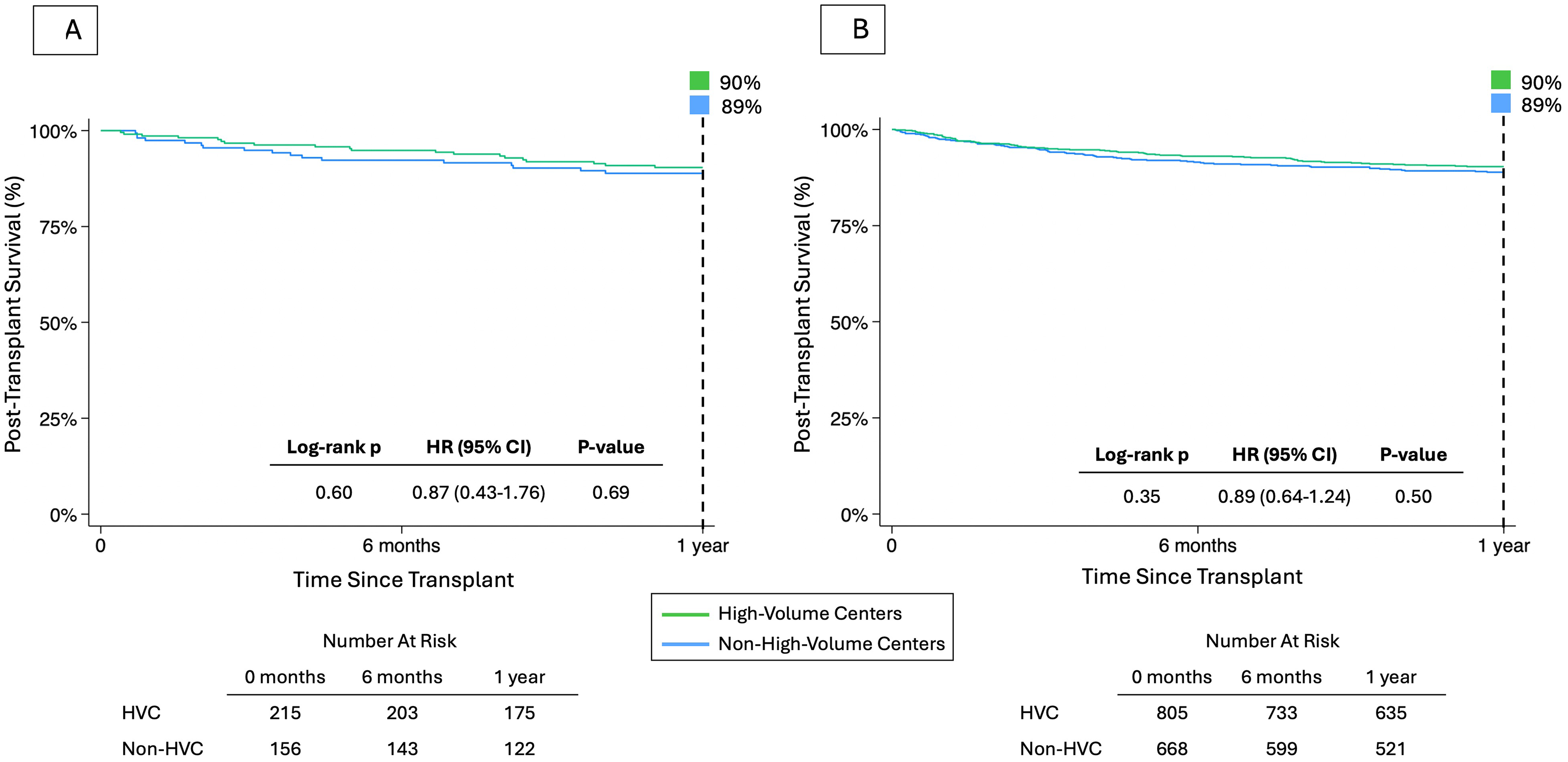
One-year posttransplant survival. (A) Survival for ABO-I recipients at high-volume centers (HVCs) and non-HVCs in the post-2016 policy change era. (B) Survival for all pediatric HT recipients in the post-2016 era. ABO-I, ABO-incompatible; ABO-C, ABO-compatible; HT, heart transplant; HR, hazard ratio; 95% CI, 95% confidence interval; HVCs, high-volume centers.
When examining one-year posttransplant survival across the entire pediatric HT cohort, outcomes were comparable at both high- and non-HVCs in unadjusted (log-rank P = .35) and adjusted analyses (HR 0.89, CI 0.64-1.24, P = .50) (Figure 5B). Additionally, we conducted a sensitivity analysis of the top volume decile of transplant centers; one-year survival for both ABO-I recipients (log-rank P = .84, HR 1.10, CI 0.51-2.35, P = .81) and overall HT recipients (log-rank P = .30, HR 0.90, CI 0.64-1.26, P = .53) remained comparable between volume groups.
Discussion
In 2016, updated guidelines were introduced to prioritize critically ill pediatric patients and improve the allocation of donor hearts through refined stratification strategies. Key changes included expanding eligibility for ABO-I HT to candidates who were listed before two years of age without titer restrictions for those under one year of age, and with titer criteria for those who were one to under two years of age—and granting candidates <1 year of age equal allocation priority as ABO-C recipients. These changes aimed to increase access to suitable allografts and improve waitlist mortality in this vulnerable population. 7 Building on this change, the 2023 policy changes aimed to further reduce waitlist mortality by allowing ABO-I transplants for pediatric Status 2 heart candidates. 10 In light of these changes, our study provides a comprehensive national analysis of the current ABO-I HT landscape.
We demonstrate an increasing proportion of ABO-I HT over the study period, from 9% of patients in 2008% to 2016% to 25% of patients in the 2016 to 2024 era. This increase corresponds to changes in the UNOS allocation policy, which removed preferential allocation of HT to ABO-C recipients for infants transplanted before their first birthday. However, since 2016, the annual percentage of ABO-I HT has remained relatively stable. This could be a result of ongoing hesitancy towards utilizing ABO-I organs; despite reassuring outcomes, nearly a third of candidates who were younger than one-year-of age declined to accept an ABO-I heart in the past few years. 7 This is supported by our finding that just over half of those listed for HT during the study period had been listed as willing to receive an ABO-I allograft. The recent 2023 OPTN policy now expands ABO-I HT to all pediatric candidates and includes Status 2 candidates. It also added additional data collection points for those candidates, which may help to better identify candidates as well as elucidate reasons behind ongoing reluctance to ABO-I HT in the future. Increasing waitlist times were observed not only among ABO-I recipients but also among ABO-C candidates, indicating a broader trend across the field. Median wait times for ABO-C transplants more than doubled post-2016 (51-105 days), while the number of ABO-C procedures declined slightly. In parallel, the number of ABO-I transplants nearly tripled, with waitlist times also increasing from 41 to 73 days. Taken together, these data suggest that system-level factors, including evolving allocation policies, donor availability, and candidate selection, may have contributed to prolonged waiting times irrespective of ABO compatibility status. Importantly, despite these pressures, the expansion of ABO-I transplantation continues to provide a critical pathway to transplant for infants who might otherwise face prohibitive barriers to access. Subsequent studies can further assess the results of the policy in years to come; however, preliminary results from our study already show promise with an increasing number of transplantations in 2024.
The findings from this study highlight evolving clinical characteristics among ABO-I HT recipients over time. Across both eras, ABO-I transplants were more frequently performed in critically ill patients, as evidenced by a higher incidence of ventilator dependence and ICU admission prior to transplant. This pattern may reflect a historical reluctance to utilize ABO-I grafts, reserving them for patients with limited alternatives on the waitlist, as well as the inability to list Status 2 candidates as ABO-I eligible before the 2023 policy change.5,6,11 Although ABO-I candidates have historically presented with greater illness severity, the difference compared with ABO-C recipients has narrowed in the post-2016 era, with lower rates of ventilator dependence and ICU admission. Post-2016, ventilator dependence in the ABO-I group was only modestly higher than in ABO-C recipients (37% vs 31%). Additionally, we observed a significant increase in the use of ventricular assist devices (VADs) and a concurrent decrease in preoperative ECMO use between eras. This trend may reflect evolving clinical perspectives, including those outlined in the International Society for Heart and Lung Transplantation's 2021 consensus statement, which emphasized that over one-third of patients transplanted are bridged with a VAD and that ECMO support prior to VAD implantation does not confer a survival benefit. 12 Similarly, a 2023 analysis by Das et al found that durable VAD use increased following the 2016 UNOS policy change among pediatric HT recipients with congenital heart disease. 13 These shifts likely mirror broader advancements in transplant care, including improved preoperative optimization, refined patient selection, enhanced postoperative management, and ongoing progress in surgical techniques.
Consistent with previous studies, we found no significant difference in survival at 1 and 5 years, nor in rejection rates, between ABO-I and ABO-C HT recipients.14–17 Our analysis also revealed no significant difference in postoperative complications, including stroke, dialysis, pacemaker placement, and graft nonfunction. These findings align with past research showing comparable outcomes between ABO-I and ABO-C transplants regarding survival and complications such as rejection, dialysis dependence, and reoperation.15,17 Notably, Patel and colleagues previously reported a 3-fold higher stroke rate and 10-fold higher pacemaker dependence in ABO-I recipients based on operations from 1999 to 2007. 16 However, our study, which focused on transplants performed in the last decade, found no such disparities. These improved outcomes may be indicative of cumulative progress in operative approaches and perioperative care, which have collectively enhanced the safety and efficacy of ABO-I HT. 18
Additionally, we found no significant difference in one-year waitlist mortality for ABO-I eligible patients between the pre-2016 era and the post-2016 era. In a comprehensive analysis of pediatric HT waitlist outcomes following the 2016 UNOS policy change, Power et al found that the policy change itself was not an independent predictor of outcomes and, while it benefited certain subgroups, it insufficiently addressed overall pediatric HT waitlist mortality. 19 Similarly, we found that although ABO-I eligible listings increased across the study period, waitlist mortality for those patients remained comparable between eras. This limited benefit may be related to the lack of equitable allocation irrespective of blood type for children >1 year of age. This underutilization raises important questions about current transplant practices and highlights an opportunity to expand access to pediatric candidates through broader adoption and allocation of ABO-I allografts.
Our analysis revealed no significant difference in posttransplant survival based on transplant center volume, either among overall HT recipients or ABO-I allograft recipients. While prior studies have reported mixed findings regarding the association between center volume and outcomes,20,21 our results indicate that centers performing a lower volume of transplants can achieve outcomes comparable to HVCs, even when performing ABO-I transplants. This suggests that ABO-I transplantation is not limited to high-resource or high-volume institutions. Taken together with our finding of equivalent posttransplant outcomes between ABO-I and ABO-C recipients, these results support broader adoption of ABO-I HT as a safe and scalable strategy to increase access to HT across a wider range of centers.
Our findings provide timely confirmation that five-year outcomes following ABO-I transplantation remain equivalent to ABO-C transplantation in the contemporary era. Importantly, these data extend beyond earlier single-center and registry reports by capturing outcomes after the 2016 allocation changes, reflecting current candidate selection and perioperative practices. This updated evidence is particularly relevant in light of the March 2023 OPTN policy change expanding access to intended ABO-I donor offers for pediatric status 1A and 1B candidates, underscoring the importance of ongoing national-level evaluation as clinical practice continues to evolve.
The findings of this study should be interpreted with some important limitations in mind. As our analysis is based on a national database, we are constrained by the available data, which lack detailed clinical and physiologic information, including adherence to and dosing of immunosuppressive agents, specific prior surgical interventions, and the severity of cardiac diagnoses. Additionally, our study does not account for posttransplantation pathways that may influence outcomes, as we did not have access to comprehensive hospital-specific protocols. Future research should aim to explore intraoperative factors, such as surgical techniques and anesthesia protocols, that could affect outcomes. Moreover, a more granular examination of posttransplant complications and their management may provide valuable insights into differences between ABO-I and ABO-C transplant recipients.
Conclusion
Our study underscores that ABO-I HT should no longer be considered merely a backup option. In the appropriate patient population, it offers survival outcomes that are equivalent to ABO-C transplants. With consistently excellent outcomes observed across both high-volume and non-HVCs and the growing national experience, it is likely time to expand the primary offer of ABO-I hearts to all pediatric age groups. This shift would align with the OPTN Final Rule by reducing waitlist mortality without increasing organ futility. Our findings also demonstrate improved listing access for ABO-I transplants across the US, regardless of center volume—supporting a model of equitable allocation independent of geography or institutional volume. Given these promising results, transplant centers should consider adopting ABO-I transplantation as standard practice. As the 2023 policy update continues to shape the field, it will be important to continue to monitor its impact on ABO-I access and utilization. Ultimately, broader adoption of ABO-I HT may enhance access to this lifesaving treatment modality and further reinforce their essential role in pediatric HT.
Footnotes
Abbreviations
Authors’ Note
Ethical Considerations: This study was exempt from IRB approval due to the retrospective and deidentified nature of the data source.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.