
Abstract
Introduction
The availability of prosthetic valves in young children with atrioventricular (AV) valve annuli of <15 mm is very limited. 1 In 2012, the first two cases of surgical implantation of a Melody™ valve (Medtronic) in the mitral position in infants were reported. The Melody valve is a stent-mounted bovine jugular vein graft designed for transcatheter pulmonary valve replacement. The competence of this valve has been demonstrated for a wide range of internal diameters (10-22 mm). Moreover, the valve, which is approximately 2.5 cm long can be manually shortened. The off-label use of surgical implantation of a folded or trimmed Melody valve seems to no longer be an experimental procedure but has become a good option for mitral valve dysfunction (regurgitation and/or stenosis) in this population when surgical valve repair failed.2,3 Recent reports have shown reasonable medium-term results in small children.4-6 The morbidity and mortality risks appear to be comparable to those of mechanical prostheses. Other potential benefits of the Melody valve in the AV position are the feasibility of balloon expansion during growth and valve-in-valve procedures when necessary. As the use of the Melody valve in a high pressure environment is a recent approach, the durability of this approach still needs to be analyzed in longer-term studies. We report the Leuven experience and long-term results of implanting the Melody valve in the AV valve position and the long-term follow-up data. Approval for this study was obtained from the Ethics Committee UZ Leuven.
Technique
Implantation of the Melody Valve
Preoperative evaluation consisted of detailed echocardiography with measurements of annular, ventricular, and atrial dimensions. Regarding the mitral valve annulus, measurements were performed at the hingepoints of the valve leaflets in the lateral plane from the apical four-chamber view. Z-scores versus body surface area (BSA) were based on the Boston Children's Hospital references. The midventricular to midleft atrial length was an indicator for valve preparation.
Based on the pioneering work of the Boston group,1,2,7,8 before initiating cardiopulmonary bypass, the Melody valve was manually adapted to the patient. In its original configuration, the Melody valve varies between 28.8 and 24.6 mm when expanded to 18 and 22 mm. The folding modification of the Melody valve leads to a theoretical maximum reduction in the stent length of 7.9 mm. 9
After washing the valve in saline and testing its competence, both the proximal and distal ends were carefully folded to reduce the total length of the stent. A pericardial strip was sutured to the exterior part of the frame, allowing surgical fixation within the annulus. This was done not in the middle of the stent, but lower to the leaflet part to prevent left ventricular outflow tract (LVOT) obstruction by the stent. The valve was then crimped manually. Manipulation of the valve should be performed carefully to avoid asymmetric compression of the stent graft. Intermittent infusion of saline was used to prevent injury to the valve.
After cardioplegia was accomplished, left atrial access was provided, and the native mitral valve was excised. The posterior leaflet and supporting subvalvular apparatus were completely resected, and the anterior leaflet was partially resected to maintain sufficient distance between the valve and the LVOT. The Melody valve was anchored within the annulus using the external circumferential pericardial skirt, with placement of multiple adjacent interrupted sutures (Figure 1).
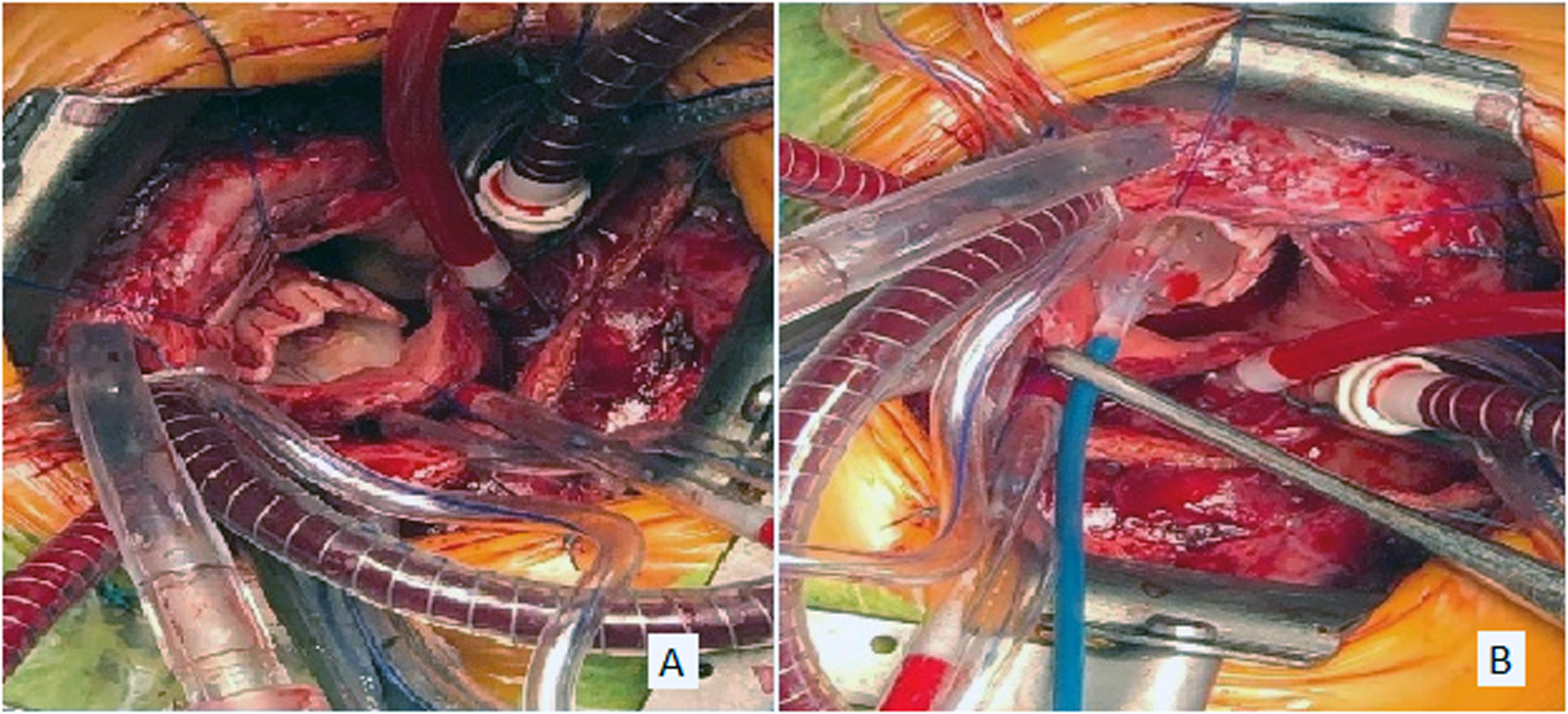
Surgical view, left atriotomy. (A) Folded and collapsed Melody stent-mounted valve, being attached into the mitral annulus by a pericardial band; (B) Balloon dilation of the valve.
Thereafter, the valve was dilated using catheterization balloons, such as Atlas Gold (Bard) or Tyshak (NuMED) balloons. The final balloon size for valve dilation was determined during surgery based on the surgeon's visual inspection and in situ measurement of the annulus with a Hegar probe.
Finally, the stent was fixed with a single stitch onto the interatrial septum to ensure that the angle of the stent frame pointed away from the LVOT. In two patients only, an extra stitch was used to fix the stent to the lateral wall of the left ventricle (LV). Leaflet function was tested using a filling test of the LV. The left atrium was inspected to ensure unrestricted inflow from the pulmonary veins. Perioperative transoesophageal echocardiography was used to assess both ventricular and valvular function, such as LVOT obstruction and paravalvular leaks. Patients were monitored in the pediatric intensive care unit (PICU). Therapeutic heparin was started as soon as the surgical bleeding was under control, replaced by prophylactic enoxaparine subcutaneaously after discharge from the PICU and then replaced by low dose acetylsalicylic acid (3 mg/kg/d) at discharge from hospital.
Balloon Dilation of the Valve to Accommodate for Growth
The timing of the follow-up cardiac catheterization was based on clinical and echocardiographic findings. Procedures were performed through an 8F introducer sheath in the femoral vein (n = 5) or transhepatic (n = 1) and 4F femoral arterial access. Transseptal needle puncture of the interatrial septum by Brockenbrough needle (Medtronic) and a 0.014″ Iron Man wire was placed into the left upper pulmonary vein. An 8F 45 cm Cook sheath was advanced into the left atrium. The interatrial septum was dilated with a 5 mm Powerflex balloon. A 4F internal mammaria catheter was placed into the LV using a 0.035″ Terumo RF wire. The Terumo wire is snared retrogradely using a 10 mm Gooseneck snare to stabilize the wire position in the LV apex. Coronary proximity was always checked using angiography before dilation (Figure 2). The Melody valve was balloon dilated with either a Tyshak (range 14 mm/3 cm-20 mm/4 cm) or Atlas Gold (range 16 mm/2 cm-20 mm/2 cm).
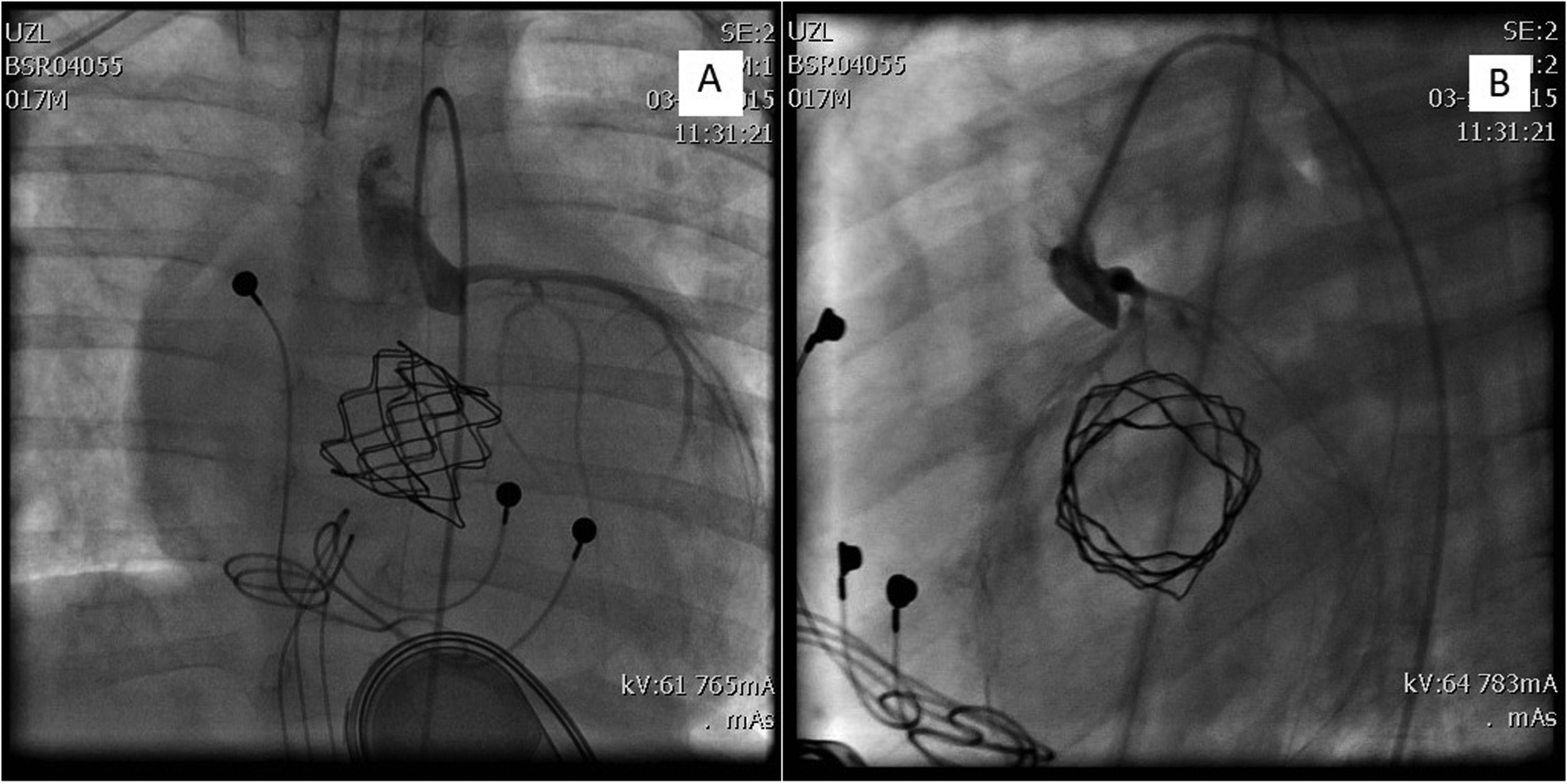
Coronary angiography (A: en face; B: lateral) before percutaneous balloon dilation of the Melody stent-mounted valve, showing relationship of coronary artery to the stent.
Valve-in-Valve Procedure
The procedure was performed in a hybrid setting with a surgical transapical left ventricular access. Femoral venous access was used for right ventricular (RV) pacing.
The Melody valve was prepared by trimming the extremities after resection of the distal zigs. The valve was manually and carefully crimped on a 12 mm Tyshak balloon. Under general anesthesia, the LV apex was punctured through a double purse-string suture via sternotomy. A 7F sheath was then advanced. A 0.035″ Terumo wire was placed through the Melody valve in the mitral position and anchored in the left pulmonary vein. Exchange for an Amplatz Superstiff 0.035″ wire. Progressive upsizing of apical access to 16, 18, 20, and then 24F (Gore Dryseal). Positioning of 22F frontloaded trimmed Melody on a 16 mm BIB balloon (Numed). Subsequent progressive dilation of the valve up to 20 mm was performed using a high-pressure Atlas Gold balloon and indeflator up to 16ATM. The procedure was performed under rapid RV pacing using a 5F NBIH pacing catheter placed in the RV septal position.
Results
Patient Characteristics
We describe four similar cases in which the implantation of a Melody valve was lifesaving, as these patients had developed severe mitral dysfunction (Table 1). Our first three patients were initially diagnosed with atrioventricular septal defect, and patient 4 had progressive subaortic stenosis due to mitral dysplasia with aberrant mitral tissue. None of the patients had comorbidities, such as prematurity or genetic anomalies. All patients had undergone mitral or left atrioventricular valve repair. The mean number of previous surgical interventions was 2.5 (range, 2.0-3.0). The mean age at implantation was seven months (range, 4-16 months). Mean weight was 6.8 kg (range, 4.1-9.5). Mean mitral annulus was 9.75 mm (range, 8.0-12.0), corresponding to a mean Z-score of −2.5 (range, −3.7 to −1.9). The indication for valve replacement was stenosis in one patient (patient 3) and severe regurgitation in three patients.
Patient Characteristics.
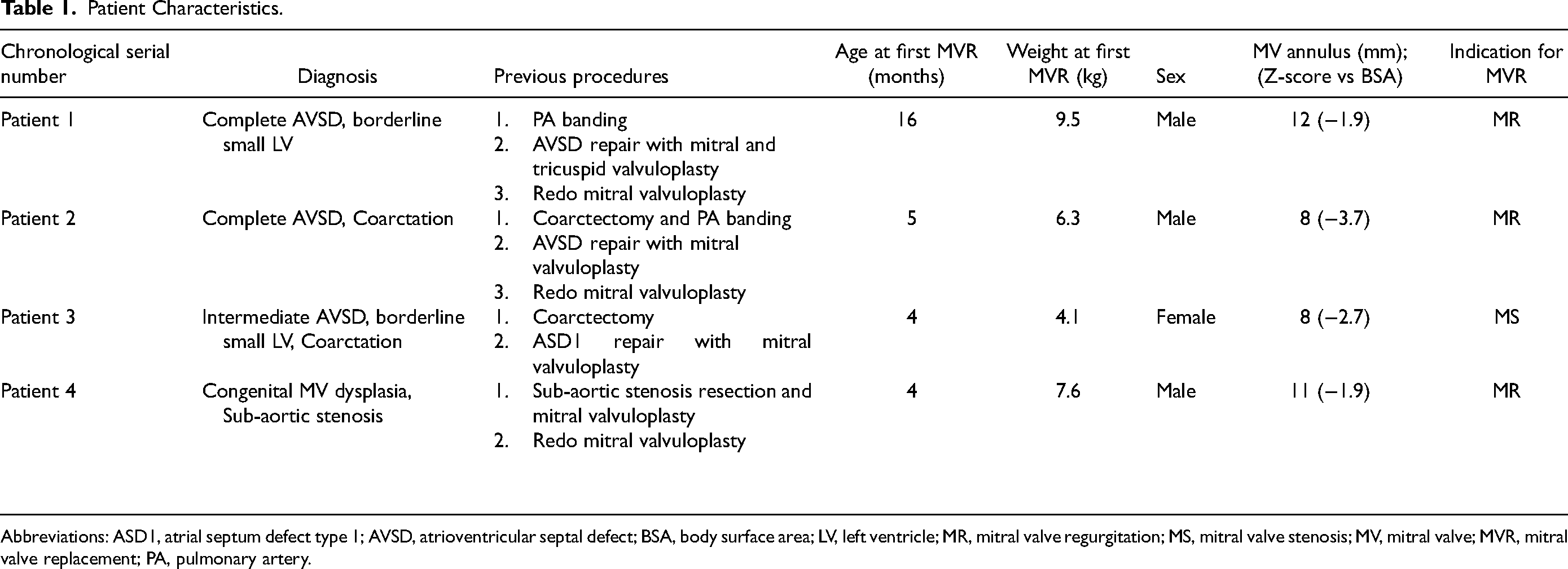
Abbreviations: ASD1, atrial septum defect type 1; AVSD, atrioventricular septal defect; BSA, body surface area; LV, left ventricle; MR, mitral valve regurgitation; MS, mitral valve stenosis; MV, mitral valve; MVR, mitral valve replacement; PA, pulmonary artery.
Surgical Implantation
The Melody valve modification consisted of a pericardial strip with a strip position slightly lower than the leaflet part (at the ventricular end) to prevent LVOT obstruction. The distal stent was fixed to the LV wall in two patients; all had a single stitch on the interatrial septum, in order to avoid LVOT obstruction. The Melody valve was expanded to an internal diameter of 13 mm (range 10-16).
Early Postoperative Results
Using transesophageal echocardiography, the immediate postoperative transvalvular mean gradient was 3.3 mm Hg (mean; range 2.5-4.0) with central mitral regurgitation (MR) 0 to maximum 1/4 in all patients. One patient had a mild paravalvular leak. The postoperative peak gradient on the LVOT was 10 mm Hg (range, 5-15).
One patient required postoperative support with extracorporeal membrane oxygenation (ECMO) for three days. Another patient was on ECMO for five days before Melody valve implantation and was weaned off of ECMO at the end of the surgical procedure.
The mean stay in the intensive care unit was 19 days (range, 16-22). The mean total length of hospital stay was 27 days (range, 21-32). All patients were on acetylsalicylic acid 3 mg/kg/d at discharge (Table 2).
Perioperative Data.

Abbreviations: AVB, atrioventricular block; BSA, body surface area; ECMO, extracorporeal membrane oxygenation; IAS, interatrial septum; LV, left ventricle; LVOT, left ventricle outflow tract; MR mitral valve regurgitation; PICU, pediatric intensive care unit
There was 100% procedural success without procedure-related mortality or early valve failure. We did not encounter well-known complications such as coronary injury or LVOT obstruction. There was no history of bleeding or thrombosis. Our main early complication was a total atrioventricular block in three of four patients without recuperation; thus, requiring pacemaker implantation.
Mid- and Long-Term Results
Follow-up after Melody valve implantation was up to 8.5 years in our first patient and over four years for the rest of the patients. The mean follow-up was 5.9 years (range, 4.2-8.5).
Catheter-Based Interventions
Every patient had a minimum of one and a maximum of two balloon expansions of the valve, with a total of six balloon expansions realized in our cohort (Table 3). The mean time between valve implantation and the first balloon expansion was 11 months (range, 1-26). Our smallest patient (patient 3), weighing 4.1 kg and 60 cm tall at Melody valve implantation, had the longest time between surgery and the first balloon dilation. Patients 2 and 4 underwent a second balloon expansion of the valve at 20 and 26 months after the first one, respectively.
Catheter-Based Interventions After First Mitral Valve Replacement.
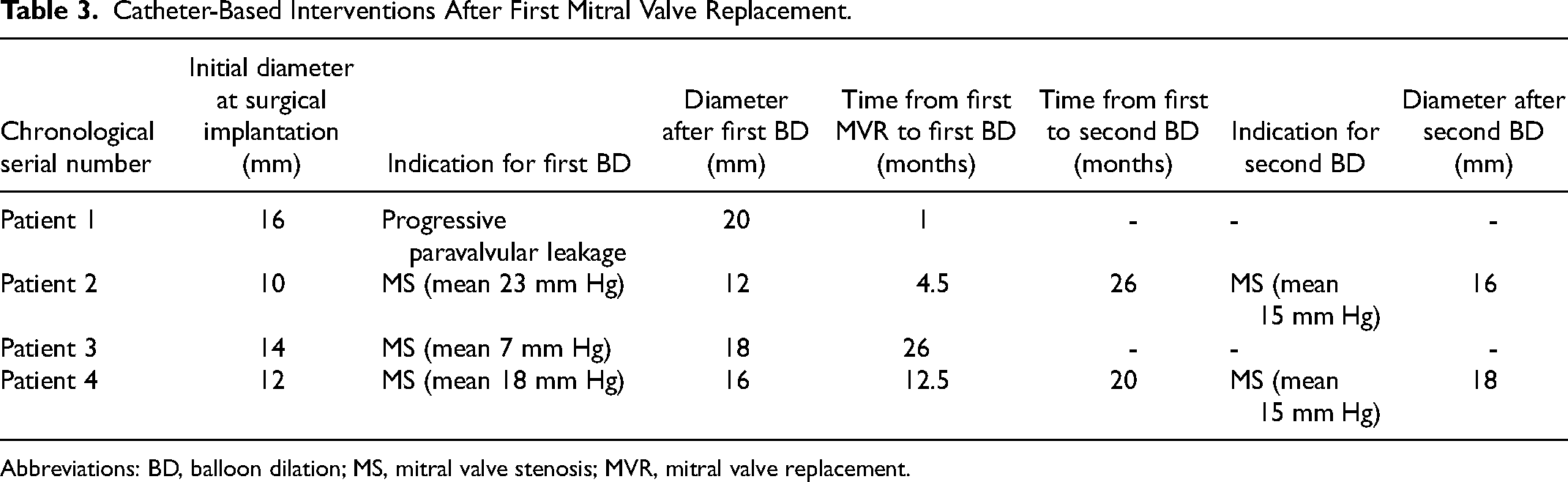
Abbreviations: BD, balloon dilation; MS, mitral valve stenosis; MVR, mitral valve replacement.
Of the six catheter-based interventions, only one was indicated for a progressive paravalvular leak (patient 1) one month after implantation. The five other balloon expansions were performed because of mitral stenosis with a mean gradient of 15.6 mm Hg (range 7.0-23.0). In all procedures except one, percutaneous access was through the femoral vein. One patient (patient 3) required transhepatic access because of femoral thrombosis. During all six balloon dilations, arterial femoral access was ensured during all six balloon dilations. The mean final valve diameter after balloon dilation was 16 mm (range, 12-20 mm). The valve was stretched for 4 mm in four of the six procedures and 2 mm in the two other procedures. After dilation, transthoracic cardiac ultrasound showed a mean transmitral gradient of 5.8 mm Hg (range 2.0-14.0) and MR grade between 0 and 2/4.
Subsequently, in one patient (patient 2), we applied the Melody valve-in-valve technique using a transapical hybrid procedure at 37 months of age. This second Melody valve was expanded up to 20 mm. The patient had persistent mitral stenosis despite two catheter expansions of the Melody valve. After the last dilation, MR grade 2/4 occurred, leading to postcapillary pulmonary hypertension. The longevity of his first Melody valve was 32 months. He is clinically well 47 months after the valve-in-valve procedure without any reintervention on his second Melody valve.
Valve Degeneration
Two patients (patients 1 and 3) required valve replacement with a prosthetic valve. The first one (patient 1) for severe MR 62 months after Melody implantation. He was 6.5 years of age at the time. Perioperative inspection revealed degenerated Melody valve leaflets. In toto excision of the valve was performed. In contrast, upscaling the annular scale was challenging. A sizer was used and a mechanical valve, type St. Jude Medical (Abbott) was chosen but needed several radial incisions. Off-label use of a 23 mm St. Jude Medical aortic valve was positioned in a reversed position. The patient required pacemaker system replacement during the same surgery. The second patient (patient 3) required Melody valve excision because of bacterial endocarditis 40 months after implantation. She was 3.6 years of age at the time. Transthoracic echocardiography showed severe mitral stenosis, with a peak gradient of 54 mm Hg, severe tricuspid regurgitation grade 3 to 4, and right ventricle pressures estimated at 85 mm Hg. Perioperative inspection revealed large vegetation on the atrial site of the Melody valve. Hemocultures were positive for Staphylococcus aureus. A bioprosthetic Epic valve (Abbott) of 19 mm was used in the mitral position.
Longevity and Latest Follow-up
Longevity (duration before final valve failure) of the first three implanted Melody valves was 62, 32, and 40 months (mean: 44.6). The mean age of the patients was 4.3 years (range: 3-6.5). The fourth patient still had his Melody valve in place 51 months after implantation (Figure 3).
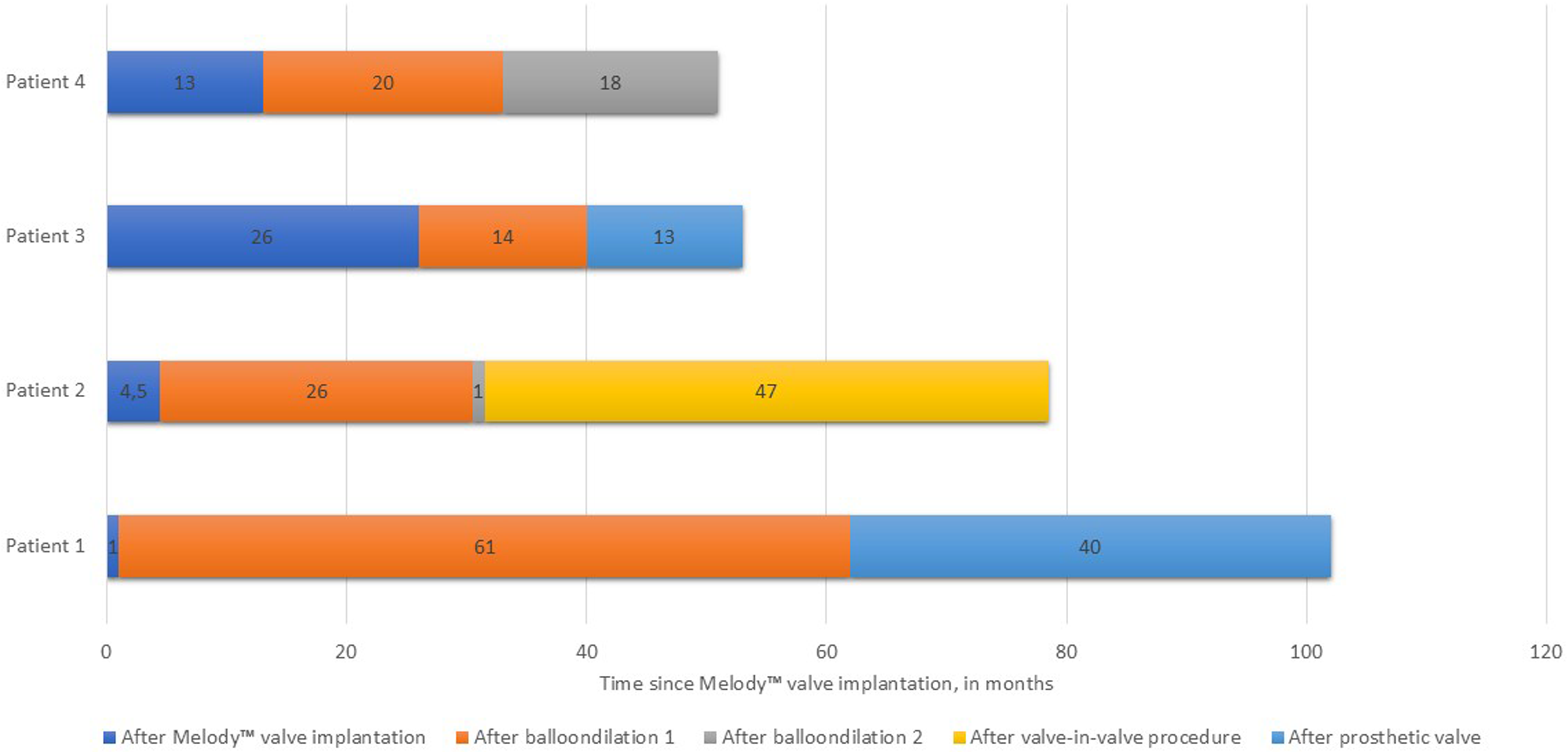
Timeline of patients’ evolution since first surgical implantation of the Melody valve.
At the end of our data collection in April 2024, echocardiography findings showed a mild paravalvular leak in one patient (patient 2) and central MR in one patient (patient 4), grade 1/4. All four patients had mean transmitral gradients below 5 mm Hg. The maximum LVOT gradient was 10 mm Hg (patient 3). No thromboembolic events were documented. Total duration of patients follow-up since first mitral valve replacement was mean 71 months (range: 51-102) (Table 4).
Discussion
As in small children, atrioventricular (AV)-valve incompetence may be challenging to correct surgically, and cardiac valve replacement is sometimes unavoidable. Prosthetic valves are limited by their fixed diameter, as they are often too large for small infants at the time of implantation. Moreover, they cannot be expanded to accommodate somatic growth. The concept of surgically implanted Melody valves is therefore attractive. This technique has been described for over a decade and no longer appears to be experimental.2–6 The durability of the Melody valve under systemic blood pressure seems acceptable.
Long-Term Follow-up Data.
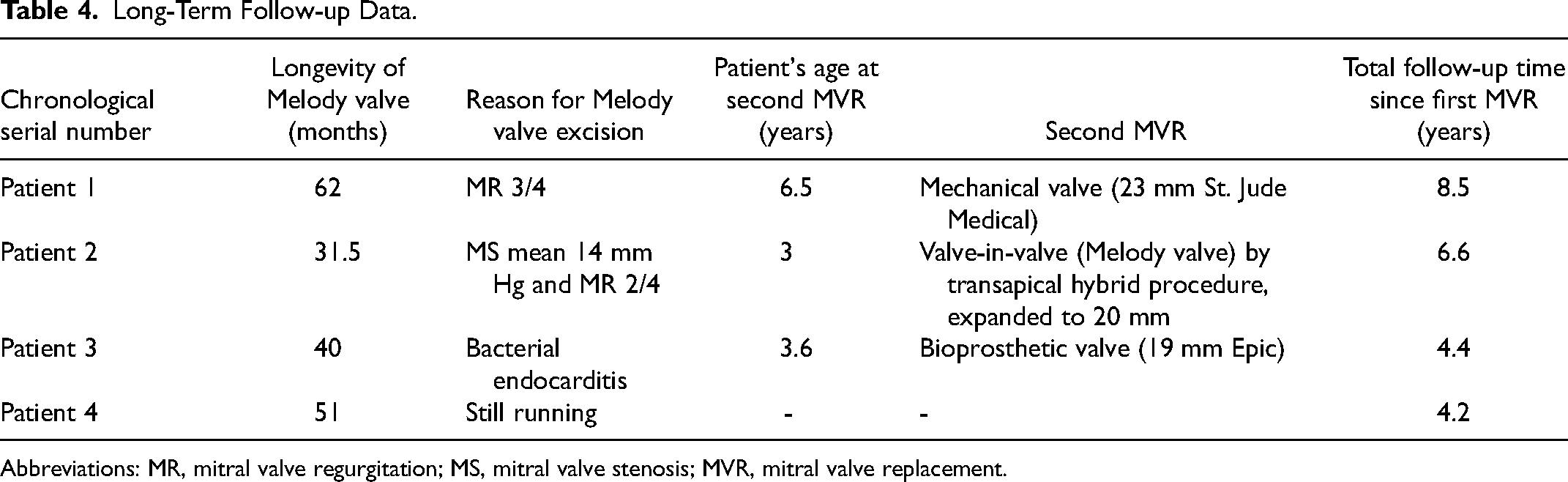
Abbreviations: MR, mitral valve regurgitation; MS, mitral valve stenosis; MVR, mitral valve replacement.
One key advantage is that the valve can be tailored to fit a small annulus, avoiding the need for supra-annular placement, which is sometimes required with other prostheses. Due to the relatively thin stent wall, the effective orifice area for a given external diameter is larger than that of a prosthetic valve with a sewing cuff. Additionally, the stent can be expanded to a range of sizes and allows for stepwise percutaneous dilation later on. This feature reduces the need for early reintervention and allows for growth until an adult-sized prosthetic valve replacement becomes feasible. The feasibility of balloon expansion has been demonstrated in previous publications.2–4,10
We analyzed clinical and technical data from four young patients, from the time of valve replacement through subsequent procedures during follow-up, providing insight into the potential of Melody valve implantation in the mitral position in this population.
For the surgical technique, access was gained via left atriotomy. For percutaneous interventions, we used transseptal puncture. In some previous reports, 8 the Melody valve was implanted via right atriotomy, and an interatrial fenestration was left in place to facilitate future catheterization.
In our series, all four patients underwent at least one balloon dilation of the Melody valve, which proved to be a safe and feasible technique. The transmitral gradient was significantly reduced after the first balloon dilation (all <5 mm Hg), without significant MR. Two patients required a second balloon expansion. In patient 2, balloon dilation was repeated 26 months after the first procedure due to persistent Melody stenosis and the appearance of grade 2 MR afterward. This led to a second mitral valve replacement. First Melody valve-in-valve technique was published in 2018. 11 We were able to successfully repeat this technique in patient 2 at 37 months of age and a body weight of 12.6 kg. The Melody valve-in-valve was expanded up to 20 mm with excellent results. Further expansion up to 22 mm remains an option. In the event of valve dysfunction, a new bioprosthetic valve—24 mm or 26 mm in diameter, depending on the patient's biometric data—could be implanted. Transapical or transatrial access may be chosen based on future anatomical considerations.
In patient 4, the second balloon dilation, up to 18 mm, was highly effective, and the Melody valve remained functional at the end of the follow-up period.
Freedom from surgical reintervention in our cohort was 46 months (mean; range: 32-62 months), which is comparable to other reported series. 4 Our cohort was particularly at risk for early valve failure, as age <12 months and weight <10 kg are significant risk factors. 5
Compared with mechanical prostheses, another advantage of the Melody valve is that long-term anticoagulation is not required. The thrombotic risk appears to be low, even under systemic pressure. All patients were maintained on low-dose acetylsalicylic acid. No thromboembolic events occurred during long-term follow-up.
Nonetheless, the technique of surgical Melody valve implantation in the mitral position remains challenging. There is a risk of creating LVOT obstruction if the valve protrudes into the LV, or pulmonary vein obstruction if it protrudes into the left atrium. Various technical modifications—such as trimming, folding, or excising the stent—can help address these issues. “High-riding” or supra-annular implantation, potentially combined with left atrial patch augmentation, has also been described to avoid LVOT or pulmonary vein obstruction.12,13 In our series, we used the folding technique. With a pericardial suture ring placed at the ventricular end of the Melody valve and fixation to the interatrial septum, we did not observe any LVOT obstruction.
Expanding beyond the measured native annular diameter may increase the risk of injury to the conduction system, potentially leading to AV block, a major complication. In our series, the incidence of complete AV block was consistently higher than the reported 9% to 15%.2,4 However, the prevalence of postoperative AV block is nontrivial after surgical mitral valve replacement in children, even in the supra-annular position, ranging up to 33%. 14 Atrioventricular block was not related to weight or age, as both our smallest and largest patients were affected. We hypothesized that after native mitral valve resection, the resting diameter was oversized to fix the Melody valve. When we indexed the final inner diameter of the Melody valve immediately postoperatively, the Z-scores versus BSA of the patients with AV block were −1.2, +0.63, and +2.0. In contrast, in the patient without AV block, the Z-score was −2.0. As described above, the initial “native” Z-scores ranged from −3.7 to −1.9.
Possibly, expanding the mitral size up to Z-scores near 0 or higher than the mitral valve annulus in small infants is not advisable. We therefore recommend respecting the preoperative echographically measured annulus diameter during balloon inflation at the time of Melody valve implantation, and adding 1 or 2 mm, with later upsizing via percutaneous dilation, as recommended by Quinonez et al. 8 For the patient without AV block, we expanded 2 mm from the native annulus. However, the risk of AV block may persist during subsequent dilations. All AV blocks in our patients were immediate complications after Melody valve implantation. We did not observe any need for pacemaker implantation after catheter dilation. In addition, interestingly, Freud et al 15 retrospectively attempted to use preoperative echocardiograms to determine potential measurements for Melody expansion in the mitral position without impinging on nearby structures, such as the presumptive location of the atrioventricular node. In their cohort, comparable with ours in terms of patient characteristics, the mitral z-scores were also frequently hypoplastic preoperatively. The “potential” z-scores determined by echocardiogram, however, were often closer to 0, which would permit a normal-sized annulus for BSA. In contrast, other authors have suggested that valve longevity improves when the balloon is inflated to 1.20 to 1.35 times the expected (Z-score 0) annular diameter. 5 Larger studies are needed to validate these findings. In any case, patient selection for Melody implantation in the mitral position should include consideration of the possible need for permanent pacemaker placement.
Coronary compression during Melody valve expansion is a known risk but was not observed in our cohort. A prompt coronary angiogram prior to balloon dilation of the Melody valve in the mitral position is recommended.
Stent fracture is a potentially serious complication that can lead to acute mitral stenosis; fortunately, we did not encounter this issue.
Additionally, we recommend lifelong endocarditis prophylaxis for this patient population. One patient in our series developed bacterial endocarditis, necessitating urgent mitral valve excision.
In our experience, Melody valve implantation was performed after multiple failed mitral valve repairs in children with heart failure. Successful balloon dilations and valve-in-valve procedures during long-term follow-up offer promising perspectives for this pediatric population. As more reports with favorable medium-term outcomes of Melody valve implantation in the mitral position in young children become available, future indications may evolve, and this technique may be prioritized in managing MR and/or stenosis in the pediatric population.
Larger, multicenter studies are needed to optimize patient selection, device design, and implantation techniques. Complication rates—such as complete AV block—should be more thoroughly investigated. Long-term outcomes and experience with surgical excision of the Melody valve in later childhood or adulthood are currently lacking.
Atrioventricular valve replacement with a Melody valve in patients with single ventricle physiology also warrants close attention in the coming years, as they appear to be at increased risk of early valve failure. 5
Looking forward, innovative methods to improve outcomes should be explored. One promising approach is the use of preoperative, patient-specific heart models created from three-dimensional echocardiography. These models may help optimize device sizing and surgical planning for implantation 16
Conclusion
The use of the Melody valve in the mitral position is an effective approach, even in cases with a mitral annulus as small as 10 mm. LVOT obstruction can be avoided by positioning the stent in a supra-annular location and securing it solely to the interatrial septum. However, expansion of the valve up to 14 to 16 mm in small infants has been associated with a higher incidence of AV block.
Close clinical and echocardiographic follow-up is essential in this population to detect any early signs of valve dysfunction. Balloon dilation of the Melody valve, in the event of paravalvular leakage or an increased transmitral gradient, is a feasible and seemingly safe procedure, particularly with respect to the potential risk of coronary injury.
In cases of valve dysfunction, valve-in-valve treatment via a hybrid procedure should be considered in pediatric patients. These medium-term results offer promising perspectives for the use of the Melody valve in the pediatric population.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.