
Abstract
Congenital tricuspid valve regurgitation (TR) is rare, and chordae tendinae rupture is an even more uncommon finding in neonates. We describe a case with intrauterine tricuspid valve chordae tendinae rupture leading to severe TR and hydrops fetalis. Successful tricuspid valve repair using artificial chordae, leaflet approximation, and annular reduction were used as rescue therapy for the neonate.
Meeting presentation: Western Thoracic Surgical Association Annual Meeting Dana Point, CA, June 25-28, 2025.
Case
A female neonate was delivered to a G3P3 mother at GA 38 + 2/7-weeks via cesarean section due to fetal distress and hydrops fetalis. The Apgar scores were 4 at 1 min, 5 at 5 min, and 7 at 10 min. A routine fetal echocardiogram at 32 weeks’ gestation showed normal cardiac anatomy. However, by 38 weeks, sonography revealed significant fetal ascites, polyhydramnios, and mild pleural effusion. Fetal echocardiogram at that time demonstrated severe tricuspid regurgitation (TR) (Figure 1A). At birth, the infant was hypotonic and apneic, with an initial heart rate below 100 bpm. Her body weight was 3300 gm. The postnatal echocardiogram confirmed severe TR and a flail tricuspid leaflet with ruptured chordae tendinae (Figure 1B). The TR pressure gradient was 16 mm Hg. A large patent ductus arteriosus (PDA) and functional pulmonary atresia were also present. After initial stabilization with mechanical ventilation, inhaled nitric oxide, 100% oxygen, inotropic agents, and drainage of pleural effusion and ascites, she underwent surgery on day 5 of life. Institutional review board and informed consent were waived due to single case report.
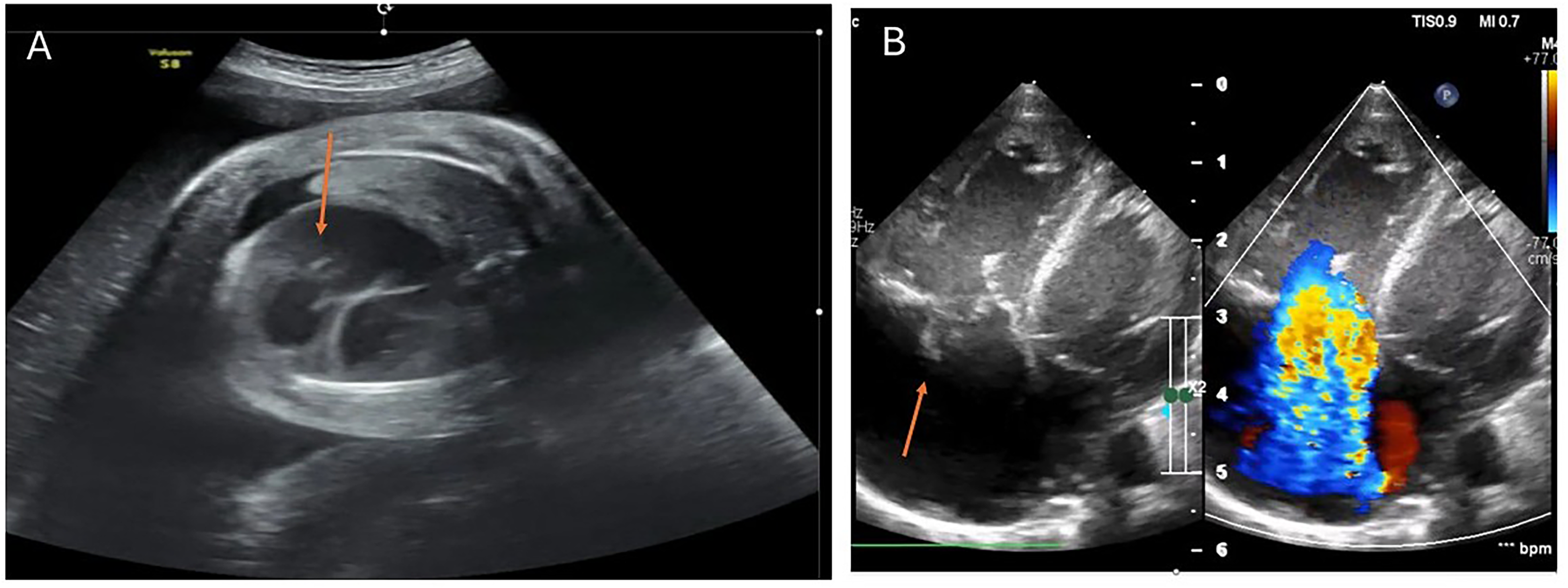
The prenatal (A) and postnatal (B) echo showed severe regurgitation and ruptured chordae tendinae (arrow) of the tricuspid valve.
Surgery was performed with standard cardiopulmonary bypass followed by aortic cross clamp. The ruptured end of the chordae tendinae could be identified on the anterior and posterior leaflets of the tricuspid valve (Figure 2). The corresponding tip on the papillary muscle was identified. Two pairs of artificial cords were attached using 6-0 Gortex® suture. Additional leaflet approximation and annular reduction procedures were needed to achieve patency of the tricuspid valve. The atrial septal defect (ASD) was closed with a small fenestration. Part of the right atrial free wall was resected for reduction of the right atrial size before closing the right atrium (Video). The pulmonary valve was checked through a main pulmonary arteriotomy, and a three leaflet valve with an acceptable size was observed. The narrowed main pulmonary artery was augmented with the resected right atrial (RA) wall. The PDA was ligated.
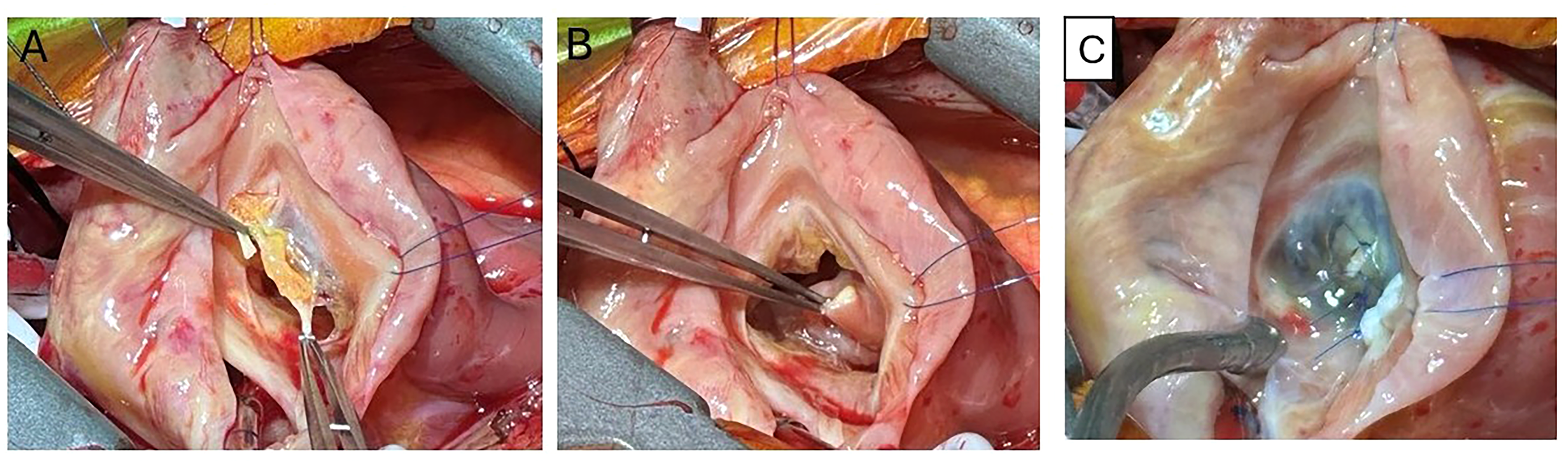
Intraoperative photos of the ruptured chordae tendinae of the tricuspid valve anterior leaflet (A) and the tip of the papillary muscle (B) and the result of the saline test after repair (C). Video Legend: This video describes the surgical techniques for repairing a neonate with severe tricuspid valve regurgitation due to intrauterine chordae tendinae rupture.
The patient was weaned from cardiopulmonary bypass and delayed sternal closure was performed on day 2 after edema subsided. The postoperative course was smooth, and the patient was extubated on day 7. One year after surgery, TR is mild and the fenestration of the interatrial septum spontaneously closed.
Discussion
Congenital TR is a challenging condition for neonatal cardiac surgeons. When TR is severe, intrauterine heart failure develops and hydrops fetalis or still birth may occur. Rupture of the tricuspid valve chordae tendinae is rare compared with rupture of the mitral valve chordae tendinae. In adult patients, extensive experience exists with artificial cords for mitral valve repair; however, neonatal experience, particularly for the tricuspid valve, remains limited. 1 Among the published reports, Roy Chowdhury et al described one of the largest series of neonatal tricuspid valve repairs for perinatal chordal rupture using PTFE neocords, with favorable midterm outcomes demonstrating the durability of this technique. 2 Their findings support the feasibility and safety of PTFE neocord reconstruction in neonates and addresses previous concerns regarding long-term function and growth potential of neocords in this age group.
In our case, the surgical technique using 6-0 Gore-Tex® artificial cords and concomitant annuloplasty was similar, confirming that early reconstruction can restore normal tricuspid valve function and biventricular circulation when native chordal tissue is deficient. Congenital tricuspid regurgitation caused by chordal or papillary muscle rupture in neonates is extremely rare, but several reports have demonstrated the feasibility of early surgical repair. 3 The technique of using 6-0 Gortex® suture was similar to the congenital mitral valve chordae tendinae rupture. 4 Anagnostopoulos et al described successful neonatal mitral and tricuspid valve repair following in utero papillary muscle rupture, supporting the role of early reconstruction in restoring valve function. 5 Loftus et al emphasized that neonatal flail tricuspid valve, although uncommon, can be effectively managed with timely surgical intervention to prevent hemodynamic collapse. 6 Pan et al further reported a case of neonatal tricuspid regurgitation due to chordal rupture that was successfully repaired with artificial cords, demonstrating its safety and durability in the short term. 3 Together with our experience, these findings suggest that artificial cordsand concomitant annuloplasty provide a practical and effective surgical strategy when native chordal tissue is inadequate, although long-term outcomes in neonates remain to be established. This experience showed the possibility of repairing neonatal TR due to chordae tendinae rupture. Right atrial reduction surgery decreases RA volume and may improve lung volume.
The other surgical option is a Starnes procedure 7 as initial palliation for severe Ebstein anomaly. We think this should be reserved for patients after a failed TV repair attempt. The fenestrated ASD helps to overcome right ventricular dysfunction and high pulmonary vascular resistance in the neonatal period. In this case, spontaneous closure of the fenestration was observed in follow-up.
Although this is an extremely rare presentation, our experience suggests that the management strategy used in this case may be applicable to similar patients, and that tricuspid valve repair can be a feasible and effective option.
Supplemental Material
Footnotes
Authors’ Note
Data Accessibility Statement: The information of this study is not publicly available due to patient confidentiality but is available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Authors’ Statement
Informed consent was obtained from the patient's parents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.