
Abstract
Introduction
Since its introduction in the early 1970s, extracorporeal membrane oxygenation (ECMO) has been used to provide cardiopulmonary support in the postcardiotomy setting. Extracorporeal membrane oxygenation plays a very important role in addressing challenges such as preoperative hemodynamic instability, difficulties in weaning from cardiopulmonary bypass (CPB), hemodynamic instability in the intensive care unit (ICU), low cardiac output syndrome (LCOS), and cardiac arrest. 1 Extracorporeal membrane oxygenation helps give patients a pathway to recovery, a bridge to transplantation, a period for informed decision-making, or a means to obtain a conclusive diagnosis.2,3 A recent systematic review and meta-analysis showed survival of 40% to 50% in postcardiotomy ECMO in children. 4
The currently available ECMO circuit consists of a membrane oxygenator, made up of polymethylpentene, a centrifugal pump, a heat exchanger, and closed circuit without venous and cardiotomy reservoir. The ECMO oxygenators are expensive and very efficient in providing oxygenation support for days to weeks in comparison with the oxygenators that are used during CPB. The centrifugal pump is very effective in reducing hemolysis and has better preservation of platelets during ECMO support. Absence of a reservoir in the ECMO circuit reduces the hemodilution and blood stasis, thereby reducing the thrombin generation and clot formation. 5 The presence of a special membrane oxygenator and centrifugal pump in the ECMO circuit makes it very expensive. Hence, its usage is very limited in the centers of developing nations. There is a need for a much less expensive ECMO circuit in the resource-limited parts of the world, especially for short-term support in postcardiotomy shock.
In our previous report, we elaborated on our initial experience with a simple modification of a conventional CPB circuit to create a closed modified ECMO circuit using a roller pump and oxygenator. 6 In this study, we aim to estimate the outcomes with the modified ECMO circuit over the last 10 years for short-term cardiac support following surgery for congenital heart disease.
Methodology
Modified ECMO Circuit From a Cardiopulmonary Circuit
The modified ECMO circuit is essentially an extension of the standard CPB circuit from the operating room out to the ICU. It uses the standard CPB oxygenator and roller pump. The main modification is adding two Y-connectors at the inlet and outlet of the venous reservoir to create a closed circuit, diverting venous blood and avoiding the venous and cardiotomy reservoir (Figure 1). Preinstallation of the Y-connectors before initiation of CPB during surgery effectively reduces the time taken to institute the ECMO time (Integrated Modified ECMO circuit). The same oxygenator and CPB tubing were used if the ECMO was initiated in the operating room following surgery. A roller pump was employed universally, and no bladder device was utilized. Heparin-coated circuits were not used.
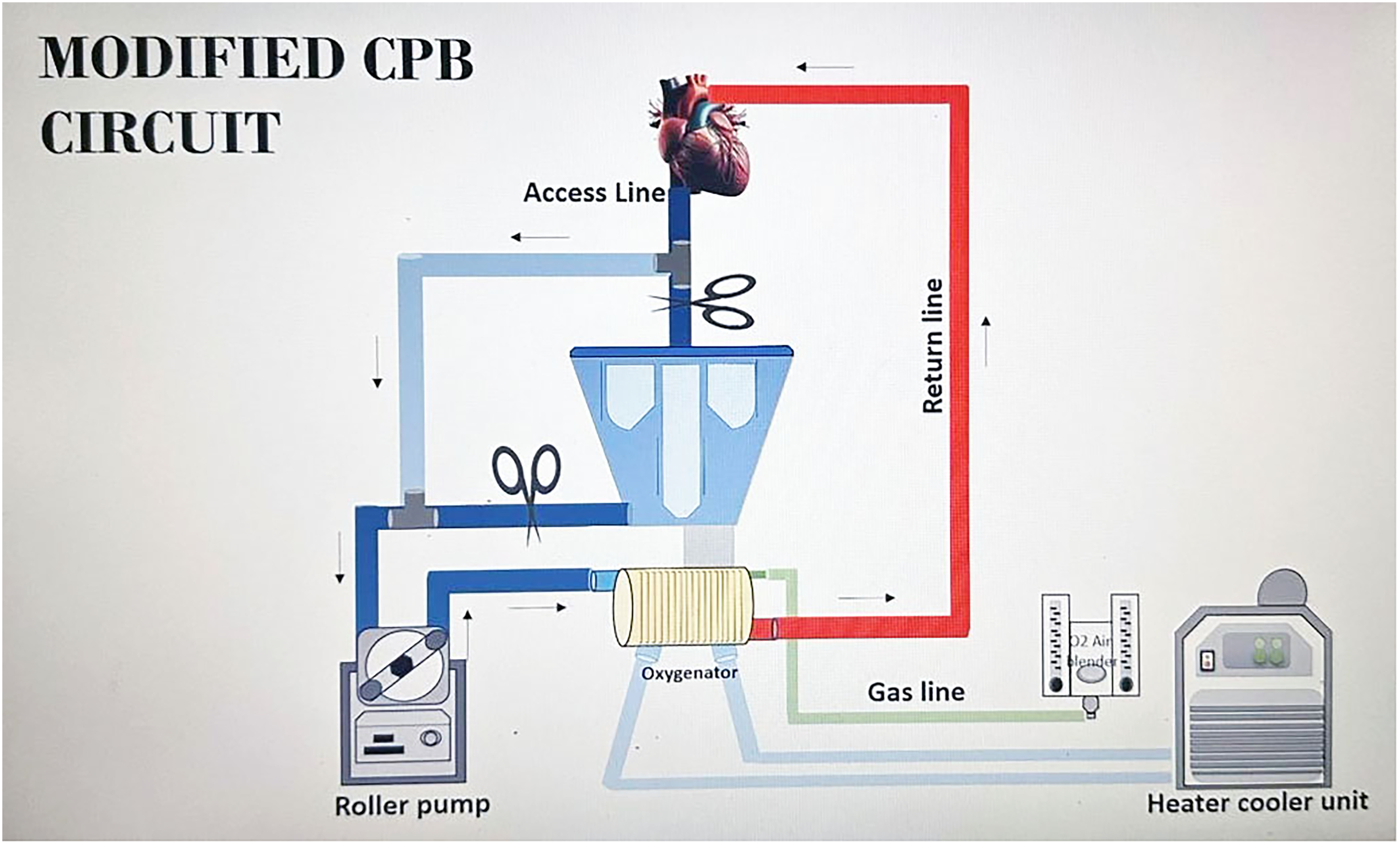
Modified CPB circuit.
The intraoperatively used roller pump and the CPB circuit including the arterial and venous lines connected solely to the oxygenator are maintained in the ICU for up to 6 hours following transfer from the operating room in high-risk cases or cases with anticipated problems following the repair of complex congenital heart disease. All cardiotomy suckers and the venous reservoir are disconnected from the circuit. Heparin is administered (1 U/mL of blood volume), and the arteriovenous loop was kept running, and the lines were monitored for evidence of new clot formation. If the patient remains stable and continued use of the circuit in the ICU is deemed unnecessary, the circuit is discarded after 6 hours.
In cases of unexpected cardiac arrest or low cardiac output in the ICU, a modified ECMO circuit incorporating a CPB circuit and oxygenator was prepared and utilized.
Initiation and Maintenance of Modified ECMO Circuit
All patients were cannulated centrally using the aorta and right atrium after administering heparin 50 U/kg of body weight (Venoarterial, VA ECMO). The sternotomy site was reopened in the ICU if the surgery was done within the past 10 days. The flow in the ECMO circuit was maintained between 100 and 150 mL/kg/minute, aiming for a cardiac index of 2.0 to 2.4. The left side of the heart was always vented in patients with no atrial communication through the right superior pulmonary vein or the left atrial appendage for better decompression of the left ventricle. The vent catheter was connected to the venous line. All patients were ventilated. Inotropes were weaned down to off as soon as good flow was established through the ECMO circuit. All patients were maintained on inodilators and afterload reduction agents. Surgical hemostasis was achieved to limit blood product usage. Coagulation was checked twice daily to have the serum fibrinogen above 150, hemoglobin of at least 10 g/dL, and platelet count of more than 100,000. Patients were observed for a couple of hours for bleeding before starting heparin infusion. After ruling out any bleeding, heparin was started at 10 U/kg/h and we aimed for an activated clotting time (ACT) in the range of 200 to 250 s. Heparin dose was titrated based on the ACT. The ACT was checked every six hours. Arterial blood gases (ABGs) were checked more frequently in the initial hours until the lactate normalized and every four hours thereafter. Oxygenator function was checked every sixth hour with pre- and postmembrane ABG. Oxygenator was visualized for any obvious clot every fourth hour. All patients were started on fourth generation cephalosporin prophylactically after blood cultures were obtained. Neurological status of the patient was assessed by looking at the pupillary reaction and gross movement of the patient after stopping the sedation twice daily. Dexmedetomidine infusion was used in all patients for sedation. Peritoneal dialysis (PD) catheter was placed. Early initiation of PD is the rule whenever there is a drop in urine output less than 1 mL/kg/h. Return of cardiac activity was assessed by looking at the arterial line waveform for ejection and normalization of sinus rhythm. Serial Epicardial 2D Echo was done by the cardiologist after reducing the flow and optimization of pre- and afterload every day while on modified ECMO. All patients were assessed for possible weaning after 24 h of support. If improvements were detected, ECMO support was continued for an additional 24 to 48 h or until the oxygenator could no longer operate effectively. In patients with underlying good anatomy and who have a high chance of recovery, ECMO was maintained until complete cardiac recovery occurred, with replacement of the oxygenator as needed. Flows were reduced gradually over a period of 8 to 12 h up to 10 mL/kg/h. Inotropes and ventilator settings were optimized before weaning from modified ECMO. All the snares were left intact, and the chest was kept open for 24 h after weaning from modified ECMO. Patients who remain stable for 7 days after being weaned off from modified ECMO are classified as having a successful ECMO wean. If no positive changes in cardiac function were observed after 24 to 48 h and especially in patients with underlying poor anatomy, such as severe pulmonary hypertension or single ventricle physiology, ECMO support was discontinued after explaining the scenario to the family.
Case Definitions
Successful decannulation was defined as patient survival without the requirement to reinitiate mechanical circulatory support within a 24 hour period after separation from ECMO.
Unsuccessful decannulation was defined as either nonsurvival of the patient or clinical deterioration necessitating the reinitiation of mechanical circulatory support within 24 h following separation from ECMO.
Renal failure: Defined as acute rise of serum creatinine to more than 50% of its preoperative level or a drop in urine output to less than 0.5 mL/kg/min for more than 8 h.
Hemodynamic deterioration: Defined as a rise in lactate level of more than 10 mmol/l, drop in the mixed venous oxygen saturation to less than 40, new onset of metabolic acidosis or worsening of metabolic acidosis in the ABG with Ph less than 7.2, and vaso inotropic score more than 15.
Critical status: Defined as the presence of one or more of the following in the preoperative period which includes cardiogenic shock, ionotropic requirement, mechanical ventilation, sepsis, and cardiac arrest.
Study Design
Following Institutional Ethics Committee approval and waiver of consent from the committee, we screened the electronic medical records for all pediatric patients who underwent cardiac surgery between June 2014 and December 2024. Thirty-four pediatric patients received modified ECMO for postcardiotomy cardiac support following congenital cardiac surgery. All patients who received modified ECMO in the perioperative period including single ventricle physiology and patients with genetic syndromes were included. Patients who received modified ECMO for respiratory failure alone were excluded. The indications for ECMO were divided into three categories, which included failure to wean from CPB in the operating room, hemodynamic deterioration in the postoperative period, and cardiac arrest in the ICU/ward.
We aimed to determine the outcomes with our modified ECMO circuit in terms of successful decannulation from modified ECMO and survival to discharge or transfer from the hospital. We also determined the incidence of complications with the modified ECMO circuit.
Data Collection
Information was gathered through the review of electronic health records following Institutional Ethics Committee approval. The following characteristics were abstracted from medical records: age, body weight at surgery, gender, anatomical diagnosis, RACHS-1 score (Risk Adjustment for Congenital Heart Surgery −1), status of pulmonary artery hypertension, and preoperative status of the patients. The intraoperative details collected included surgical procedures, the duration of CPB and aortic cross-clamping (ACC), indications for modified ECMO support, duration of support, and ability to wean from modified ECMO. Data were also collected on the modified ECMO-related complications, including renal dysfunction, bleeding, and stroke.
Statistical Analysis
Continuous data were represented as either the mean ± standard deviation or median with interquartile range based on normality of distribution. Categorical variables were reported as a frequency and percentage. Kaplan-Meier statistical analysis was used to compare patients based on successful decannulation for the outcomes; namely, duration of hospital stay and in-hospital mortality. All statistical tests were carried out using Jamovi v 2.3.21 and R plots.
Results
Demographic Details
The modified ECMO circuit was used in 34 children, 6 of whom (17.6%) were neonates. The median age at patient cannulation was 3.5 months (IQR 1-12 months) and the median body weight was 4.5 kg (IQR 3.4-7.3 kg). Overall, 25/34 (73.6%) patients were stable, and 9/34 (26.5%) were critical preoperatively. Cardiogenic shock, sepsis, and preoperative ventilator support were each seen in 11.8% of patients (4/34 patients each). Additionally, 11.8% were cardiac arrest survivors, and 23.6% (8/34 patients) required inotropes. Severe pulmonary artery hypertension was observed in 3/34 patients (8.9%). Of the patients, 58.8% (n = 20/34) were classified as RACHS-1 score of 3, and 23.5% (n = 8/34) were classified as RACHS-1 score of 4. The median CPB time was 179 min (IQR 146-248 min), and the ACC time was 112 min (IQR 80-156 min) (Table 1). No significant differences were observed in the demographics, CPB, and ACC timings between successful and unsuccessful weaning of patients from modified ECMO.
Demographics
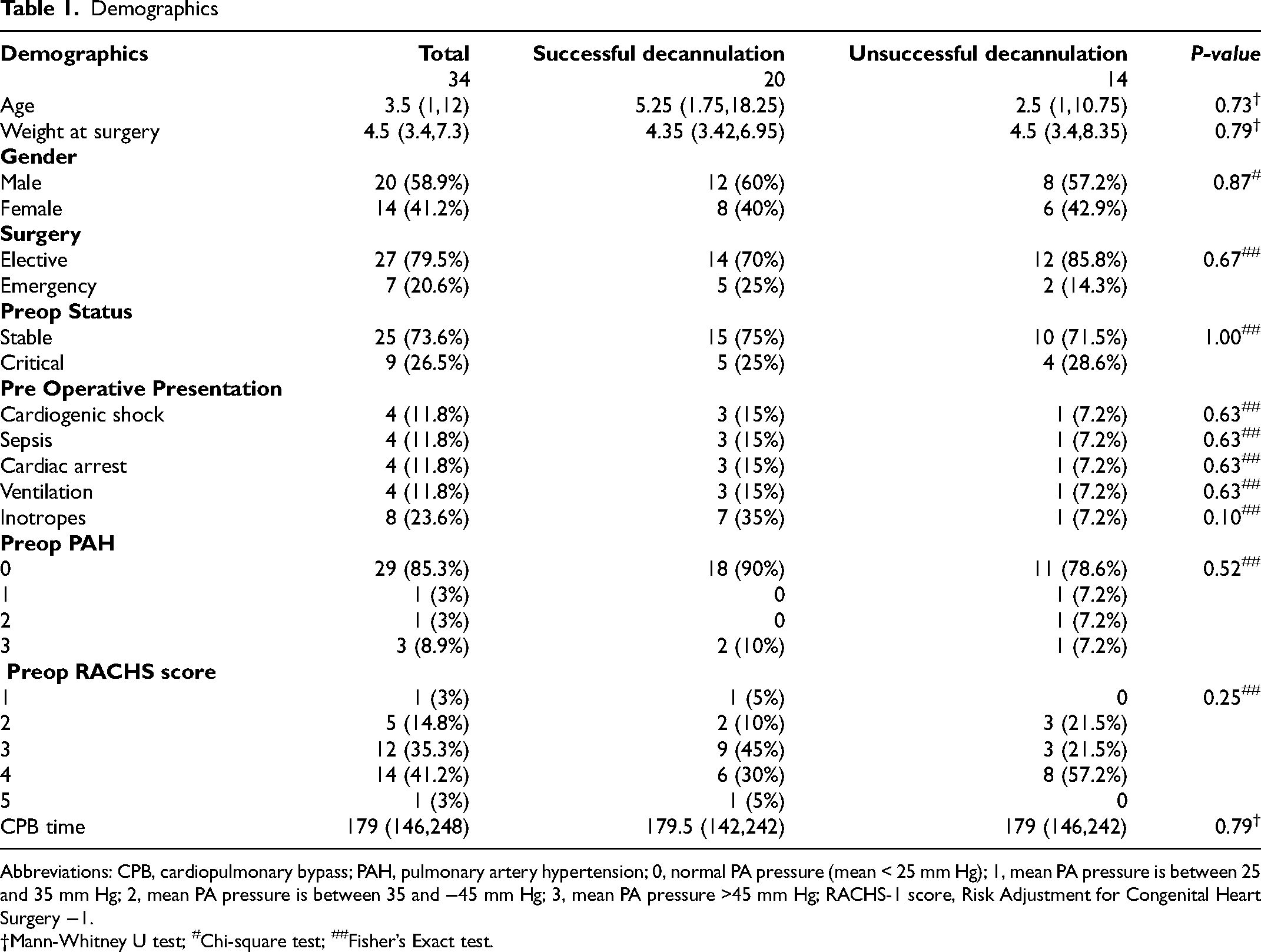
Abbreviations: CPB, cardiopulmonary bypass; PAH, pulmonary artery hypertension; 0, normal PA pressure (mean < 25 mm Hg); 1, mean PA pressure is between 25 and 35 mm Hg; 2, mean PA pressure is between 35 and −45 mm Hg; 3, mean PA pressure >45 mm Hg; RACHS-1 score, Risk Adjustment for Congenital Heart Surgery −1.
Mann-Whitney U test; #Chi-square test; ##Fisher’s Exact test.
Modified ECMO was frequently used in patients with anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) who presented with severe left ventricular dysfunction. Notably, the modified ECMO circuit successfully facilitated the weaning of five out of six patients diagnosed with ALCAPA. Additionally, the modified ECMO circuit was utilized in six patients with dextro-transposition of the great arteries (D-TGA) with intact ventricular septum, among whom four exhibited regressed left ventricles, while two had single coronary arteries. In particular, a nine-month-old child with D-TGA and intact ventricular septum underwent delayed arterial switch operation, receiving elective support from modified ECMO for 4 days before being successfully weaned. Furthermore, modified ECMO was implemented in three patients postrepair for Tetralogy of Fallot. All three had transannular patches and developed severe right ventricular dysfunction. The modified ECMO circuit was utilized for various other complex congenital anomalies following surgical intervention (Table 2).
Diagnosis of Congenital Heart Disease, Type of Repair, and Outcome With Modified ECMO.

Abbreviations: ALCAPA, anomalous origin of left coronary artery from pulmonary artery; ASD, atrial septal defect; ASO, arterial switch operation; AVSD, atrioventricular septal defect; AV valve, atrioventricular valve; BD Glenn, bidirectional Glenn; CCTGA, congenitally corrected transposition of great arteries; DORV, double outlet right ventricle; D-TGA, D-transposition of great arteries; ECMO, extracorporeal membrane oxygenation; LAD, left anterior descending coronary artery; LIMA, left internal mammary artery; LPA, left pulmonary artery; PDA, patent ductus arteriosus; PS, pulmonary stenosis; RPA, right pulmonary artery; TAPVC, total anomalous pulmonary venous connection; TOF, tetralogy of fallot; VSD, ventricular septal defect.
Modified ECMO Duration and Complication
Modified ECMO was implemented for postcardiotomy support primarily for three reasons: inability to wean from CPB in 11/34 patients (32.3%) hemodynamic deterioration in 12/34 patients (35.3%), and extracorporeal cardiopulmonary resuscitation following cardiac arrest in 11/34 patients. (32.3%).
The median time interval from surgery to ECMO initiation for patients who had LCOS in the ICU was 10.14 h (range, 15 min to 31.5 h). The median duration of ECMO was 39 hours (IQR 24-56). The duration of open chest and ventilation hours was 72 (41.7-102) hours and 91 (47.2-193.5) hours, respectively. Patients with successful weaning had a significantly longer duration of open chest and ventilation compared with those who had unsuccessful weaning.
The most common complications associated with modified ECMO included renal failure in 38.2% (13/34) of patients and bleeding in 35.2% (12/34) of patients. Renal failure was observed in 53% (7/20) of the successful weaning group and 46% (6/14) of the unsuccessful group; 45% (9/20) of bleeding incidence was observed in the successful weaning group. Peritoneal dialysis was performed on 47% (16/34) of patients, including for renal failure and fluid removal. Of the complications that were of interest the incidence of stroke (5.8%, 2/34) and seizure (8.8%, 3/34) were relatively low (Table 3). Of the 34 patients 1 (2.9%) had dry gangrene of the great toe, attributed to the administration of a high dose of inotropic support following weaning.
Indication and Complications of Modified ECMO.
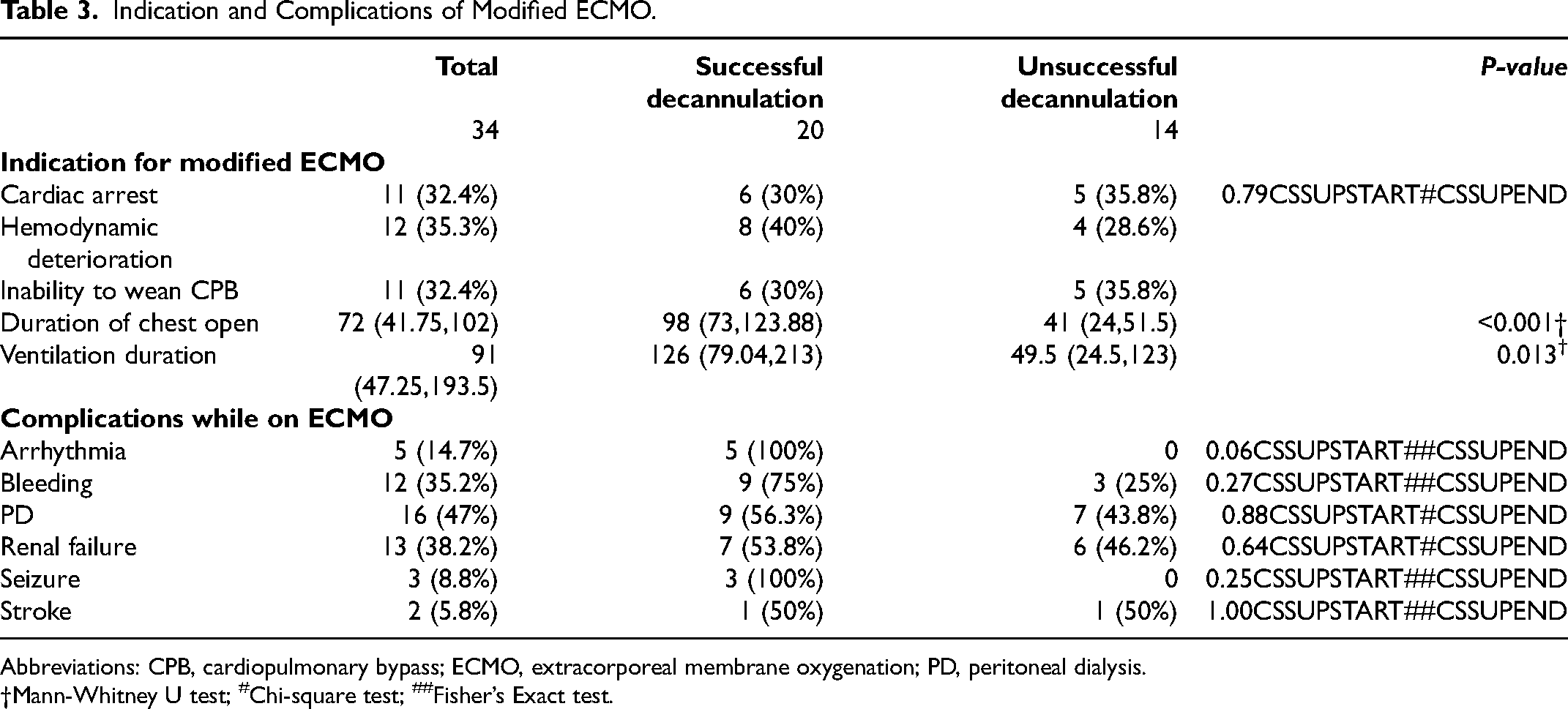
Abbreviations: CPB, cardiopulmonary bypass; ECMO, extracorporeal membrane oxygenation; PD, peritoneal dialysis.
Mann-Whitney U test; #Chi-square test; ##Fisher’s Exact test.
Outcomes of Modified ECMO Circuit
Overall, 20/34 patients (58.8%) were successfully weaned from modified ECMO, and among these patients, 11 (32.3%) survived to be discharged. In hospital mortality following successful weaning was 45% (n = 9/20). Among neonates (n = 6), 50% (3 patients) were weaned from modified ECMO, and 16% (1/6 patient) survived to discharge (Table 4).
Outcomes of Patients on Modified ECMO
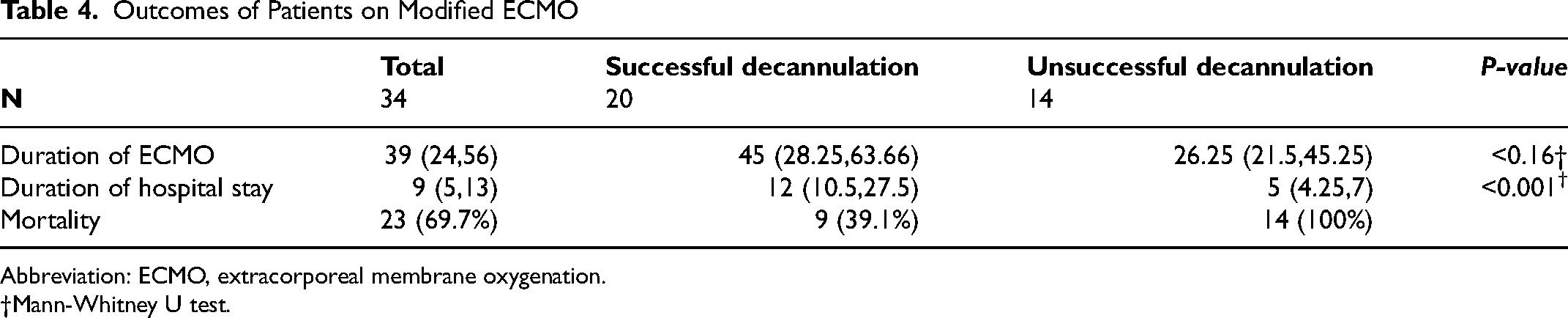
Abbreviation: ECMO, extracorporeal membrane oxygenation.
Mann-Whitney U test.
Duration of Hospital Stay, Duration of Modified ECMO, and Impact on the Outcome
The average hospital stay for patients who were successfully weaned from modified ECMO was significantly longer (P < .001) compared with those who were unsuccessfully weaned from modified ECMO (Figure 2, Table 4). Patients who were discharged alive had a significantly shorter duration on the modified ECMO (P = .04) than those who did not survive (Figure 3).
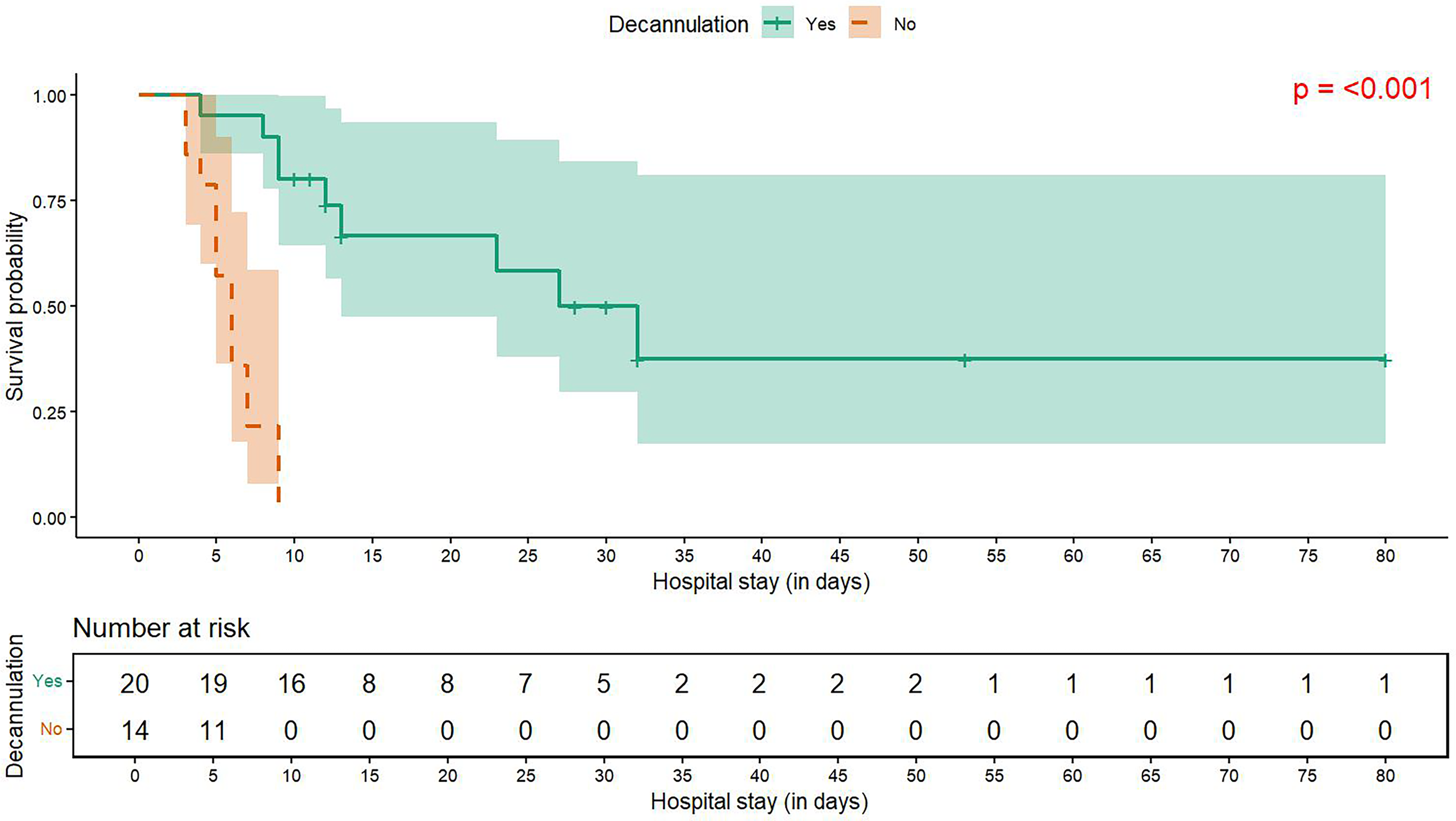
Kaplan–Meier survival curves showing in-hospital survival among patients supported with ECMO, stratified by decannulation status. Solid and dotted lines represent decannulated and non-decannulated groups.
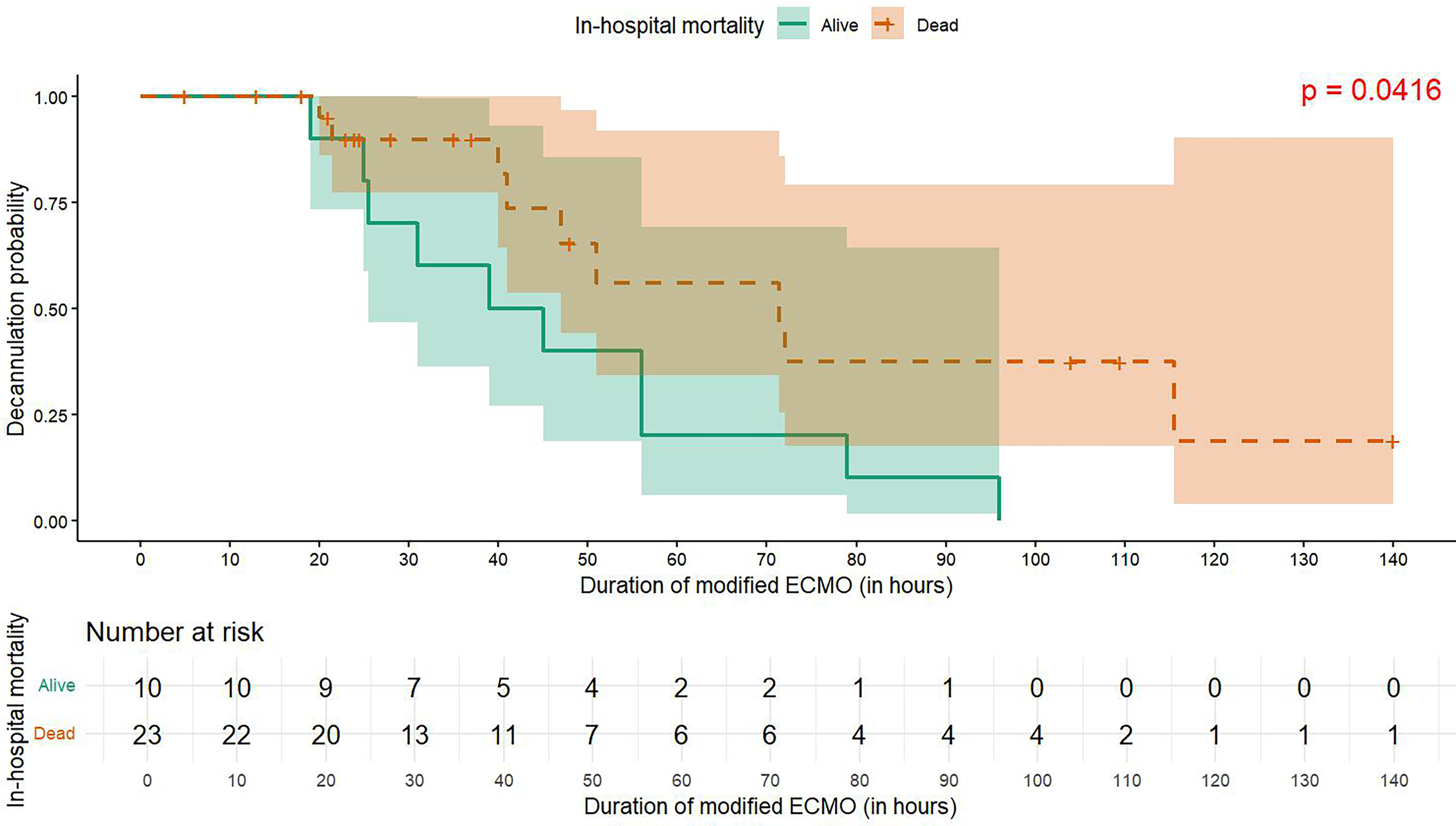
Kaplan–Meier curves showing decannulation probability during ECMO support, stratified by in-hospital mortality outcome. Solid and dotted lines represent survivors and non-survivors.
Follow-up
A total of 11 patients survived to discharge, out of which 10 survived until the last follow-up in January 2025. Among the survivors, the median follow-up duration was 1.75 years, with the longest being 6.58 years and shortest, 5 months.
Discussion
Extracorporeal membrane oxygenation is a crucial intervention for providing cardiac support following cardiotomy, as demonstrated by data from the 2024 Extracorporeal Life Support Organization (ELSO) international registry. 7 The data show that 73% of children survived after decannulation from cardiac ECMO support with 55% surviving to discharge. However, the use of ECMO is limited by its high cost, especially in developing countries and areas with limited resources. The average cost of pediatric ECMO treatment in an ICU for approximately 45 days in the United States is approximately $324,841. 8 This is not affordable for many children in developing nations. Therefore, we initiated modifications to the CPB circuit for short-term postcardiotomy support, offering a cost-efficient alternative. The main modification is the use of the CPB oxygenator and arteriovenous circuit without the use of the venous reservoir and cardiotomy suckers thereby making it a closed system (modified ECMO). The CPB oxygenator is more cost-effective compared with the conventional ECMO oxygenator. However, it is not recommended for prolonged use, and it is advisable to use it only for 6 to 8 h. By incorporating the CPB oxygenator into the modified ECMO circuit, the estimated cost of operating the modified ECMO system derived from a CPB circuit is approximately $1000 to $2000 for a 7-day period in our center.
The modified ECMO support was introduced in 2015 in our unit as a lifesaving measure. This circuit was initially presented with several challenges. However, since its implementation, the results have consistently improved. In 2018, we successfully discharged our first patient after implementing a modified ECMO circuit. The modified ECMO circuit was used in three situations, including hemodynamic deterioration in the operating room or in the ICU, inability to wean from CPB, and after cardiac arrest in the ICU. In this cohort of patients, the modified ECMO is most successful for patients with hemodynamic deterioration in the ICU rather than for cardiac arrest, and for failure to wean from CPB.
Although consensus regarding the optimal timing for initiating ECMO in the perioperative period remains elusive, evidence shows elective and early initiation of ECMO as early as in the operating room increased the success rate.9–11 Fux and collaborators have shown that a lactate value above 10 mmol/L at implant is associated with 90% in-hospital mortality, with no survival when lactate levels were >15 mmol/L. 12 Another publication supporting a pre-ECMO initiation lactate level of greater than 6.45 mmol/L was associated with higher mortality. Patients who showed decreasing lactate after postcardiotomy ECMO support had higher success rates of weaning off ECMO. 13
Our success rate of weaning from modified ECMO has improved over the years because of the team's preparedness for the need of ECMO in high-risk cases and preoperative incorporation of the modification into the CPB circuit, and getting ready for the ECMO (integrated modified ECMO circuit). As a unit policy, a new modified CPB circuit is always maintained on standby as an ECMO system in the ICU to provide readiness for emergency situations. This setup enables quick use of the circuit if needed, allowing timely response during emergencies. The delay in initiating the ECMO after cardiac arrest continues to be a major bottleneck impacting the outcomes.
The most frequent complication observed in this series was acute renal failure, occurring in 38% (13/34) of patients, which was similar to the 2020 ELSO registry. 14 The high incidence of renal failure may be attributed to increased activation of inflammatory mediators, resulting from the extended use of oxygenators, hemolysis due to use of the roller pump in the circuit and nonheparin-coated circuits.15–17 The occurrence of renal failure after successful decannulation had an impact on the survival probability of patients in our cohort. The mortality rate seen in our series is almost similar to ELSO registry.7,14 As compared to other studies, the incidence of renal failure requiring renal replacement therapy while on ECMO had a strong association with mortality.18–22
Bleeding was the next most common complication. The causes for bleeding were multifactorial. The factors associated with bleeding were observed to be anticoagulation related, platelet dysfunction due to use of the roller pump and consumption of fibrinogen into the circuit. Currently available literature supports acquired von Willebrand syndrome and reduction of factor XII in patients undergoing ECMO.23–25 Additionally, postponing the use of heparin in the ICU could be an effective strategy in minimizing bleeding. 26 A study by Hamzah et al showed reduced risk of bleeding with bivalirudin in comparison with heparin. 27
Access to the bivalirudin continues to be a challenge, along with monitoring the anticoagulation effect of bivalirudin using ROTEM (rotational thromboelastometry).28,29
The use of ECMO in children with complex congenital heart disease is associated with poor neurological outcome (20%-60%). 30 However, fatal brain injury leading to brain death is less than 1%. The most common neurological complications are ischemic stroke (30%), seizure (20%), and intracranial hemorrhage (26%).31,32 The neurological complication observed with the modified ECMO circuit in our cohort was much less than what is reported in the literature. It may be due to central cannulation and minimal duration of ECMO. Carotid cannulation has a higher incidence of neurological injury than central cannulation. 33 None of the patients in this cohort underwent carotid cannulation. All patients received dexmedetomidine, as it has been shown to protect the hippocampus against ischemic damage by acting on alpha 2 adrenergic receptors when used for sedation in children with ECMO.34,35
Survival outcomes on ECMO are influenced by various factors such as body weight, age, indication, and timing of initiation. 36 Notably, neonates weighing less than 3 kg undergoing postcardiotomy ECMO exhibit increased mortality, attributed to factors including underdeveloped myocardium and pulmonary vascular hypertension.9,37 Patients with single ventricle physiology have poor outcomes compared with patients with biventricular circulation.37– 39 Given the size of this cohort, risk factor analysis was not performed in this study. However, the prolonged hospital stay of patients who were successfully weaned was accompanied by a higher incidence of adverse events, which ultimately affected the survival rate at discharge in successfully weaned patients
Modifications of the CPB circuit for short-term circulatory support have been reported in the literature; however, variations exist among these modifications, and none have been extensively studied with a large sample size. This makes it difficult to draw any direct comparisons. Das et al reported using the standard open CPB circuit for postcardiotomy support in nine pediatric patients. The survival rate to decannulation was 33.3% (N = 3), and the survival rate to discharge was 22.2% (N = 2). Bleeding was the main complication (44.4%), leading to disseminated intravascular coagulation and significant intracranial hemorrhage, which required stopping CPB support. 40
Similarly, Kreutzer et al reported their 4-year experience with a modified CPB circuit, bypassing the reservoir with a nonprimed ECMO bladder, for short-term cardiac support in eight patients from 2001 to 2004. Their median support duration was 3.1 days, with 62.5% (N = 5) survival to decannulation and 50% (N = 4) survival to hospital discharge with no subsequent mortality. Their target ACT was similar to ours at 180 to 200 s, due to the use of a closed circuit. 41 As with Kreutzer et al, we also maintain a lower ACT, and in turn reduce the bleeding complications.
The modified ECMO circuit is not suitable for prolonged use as compared with conventional ECMO. However, it plays a valuable role in supporting myocardial recovery after extended ischemic periods during complex repairs, stabilizing end-organ perfusion in cases of low cardiac output in the ICU and provides time for the families to make decisions following cardiac arrest, particularly in resource-limited settings. Further studies with larger cohorts will help increase evidence in this area and establish a sustainable modified ECMO model.
Conclusion
The modified ECMO technique using a conventional CPB circuit that we have described is a valuable resource for short-term mechanical support postcardiotomy in children with congenital heart disease in resource-limited environments. Early initiation and following robust protocols along with preparedness of the entire cardiac team is crucial for a positive outcome.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.