
Abstract
Keywords
Introduction
Congenital heart disease (CHD) remains one of the most demanding challenges in pediatric cardiac surgery, where a precise understanding of patient-specific anatomy is critical for successful intervention. Tetralogy of Fallot (TOF), the most common cyanotic CHD, involves complex structural abnormalities that profoundly distort cardiac geometry and hemodynamics.
While echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI) provide essential diagnostic insights, they lack the spatial and tactile realism necessary for surgical rehearsal and advanced training. Three-dimensional (3D) printing has enhanced anatomical visualization and education, but most printed models remain rigid, costly, and slow to produce. They often fail to reproduce delicate internal structures or the mechanical behavior of real cardiac tissue.
To address these limitations, we developed a hybrid computer aided design (CAD)–molding workflow combining MRI segmentation, 3D printing, and silicone casting to create flexible and anatomically accurate TOF models in a reproducible and cost-efficient way. This approach merges the geometric precision of MRI-derived anatomy with the tactile realism of silicone, significantly reducing production time and cost compared with conventional 3D printing.
The novelty of this work lies in its integrated design-to-molding pipeline and its structured validation by pediatric cardiac surgeons, who assessed the models for anatomical fidelity, tactile realism, and educational value. The following sections detail the fabrication process, surgeon-based evaluation, and comparative analysis with conventional 3D printing, laying the groundwork for broader implementation in medical education, preoperative planning, and clinical research.
Literature Review
A review of 40 studies published between 2016 and 2025 highlights 5 key domains where 3D printing has shown major impact: education, surgical planning, communication, barriers, and valve modeling (Supplemental Table S1). In education, numerous studies have demonstrated that 3D-printed heart models enhance understanding of congenital cardiac anatomy, improve learner engagement, and support surgical-training realism.1–10 For surgical planning, patient-specific models derived from CT or MRI data have improved spatial comprehension, preoperative-strategy design, and rehearsal of complex repairs.11–25 In communication, several reports confirmed that 3D physical and virtual models improve family and patient comprehension compared with traditional 2D imaging.24,26–28 Despite these advantages, major barriers remain, including prolonged printing time, high production cost, and limited access to flexible materials.2,4,15,29–32 Finally, advances in valve modeling—such as silicone-based and flexible 3D-printed valves—have demonstrated realistic hemodynamic behavior and promising potential for procedural simulation.7,33–35 Collectively, these 40 studies confirm the expanding role of 3D printing in congenital cardiology and medical education, yet underscore the ongoing need for models that combine anatomical precision, material flexibility, and realistic mechanical performance.
Methodology
The integration of MRI-based anatomical review with extensive surgeon feedback provides a comprehensive validation of the proposed workflow. The hybrid CAD–molding approach reliably reproduced the key morphological features of TOF, enabling realistic operative maneuvers such as infundibular resection and ventricular septal defect (VSD) closure. The flexibility and hollow structure of the model enhanced spatial understanding of intracardiac pathways and supported hands-on procedural training.
Overall, these findings demonstrate that the hybrid workflow successfully bridges medical imaging and surgical simulation. By providing anatomically faithful, operable, and reproducible heart models, this approach offers a valuable tool for surgical education, preoperative preparation, and broader training in congenital cardiac surgery.
Results
Validation of Anatomical and Tactile Fidelity
The validation of the hybrid CAD–molding models was carried out collaboratively between the engineering researchers and the pediatric cardiac surgery team from the University Hospital Center of Marrakesh (CHU Marrakesh, Morocco), who were integral members of the project consortium. Continuous feedback from these surgeons guided the optimization of segmentation accuracy, valve delineation, and material selection to ensure that the final model faithfully reflected MRI-derived anatomy.
A hands-on surgical validation workshop was conducted at the Faculty of Medicine, University of Marrakesh, on June 14, 2022, involving 60 surgeons from more than 25 national and international centers. Pediatric cardiovascular surgeons performed infundibular resection and ventricular septal defect closure—key steps in TOF repair—directly on the silicone heart models (Figure 1).
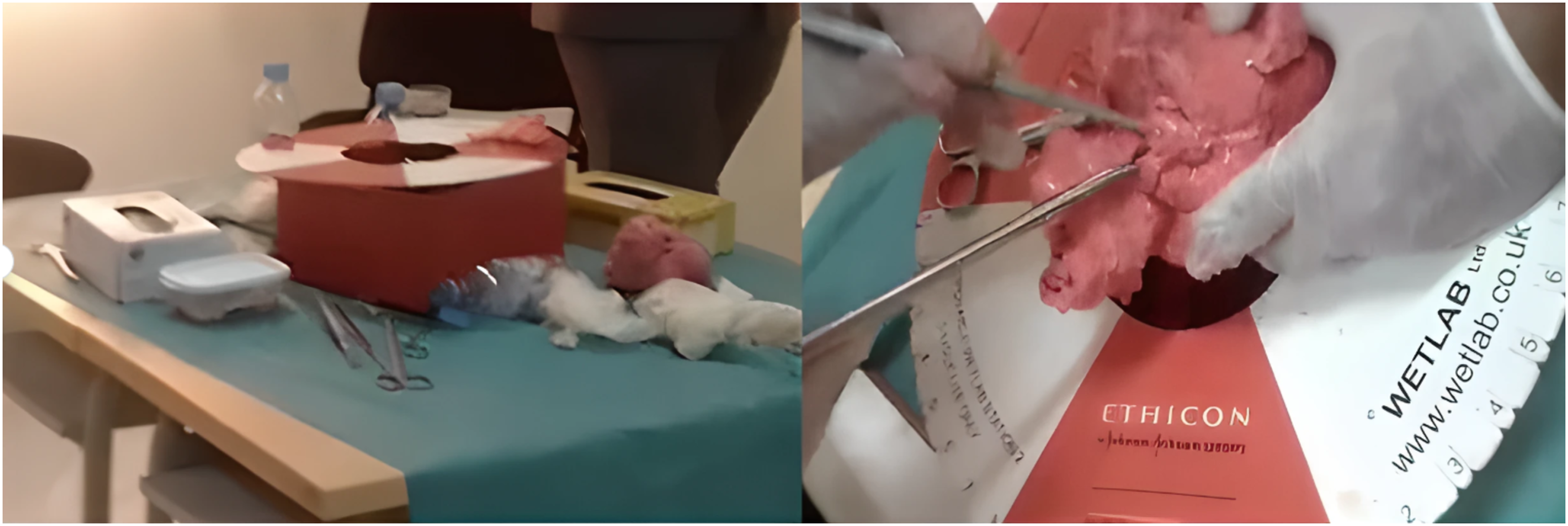
International hands-on surgical validation workshop involving 125 participants from 60 countries, during which pediatric cardiac surgeons performed key steps of Tetralogy of Fallot repair on the silicone heart models.
Direct comparison between the anonymized MRI datasets and the corresponding physical models demonstrated accurate reproduction of the major morphological features of TOF, including the VSD, pulmonary stenosis, and overriding aorta. The silicone composition provided realistic haptic feedback, enabling surgeons to perform incisions, resections, and sutures under near-physiological resistance.
The flexible and hollow structure, produced using a dissolvable internal mold, reproduced both the external and internal cardiac morphology, providing a tangible perception of blood-flow pathways and improving spatial understanding of the outflow tracts. Surgeons unanimously reported that the model faithfully replicated both the geometry and the mechanical behavior of cardiac tissue, making it highly suitable for preoperative simulation and hands-on training. They also emphasized its pedagogical value in enhancing spatial orientation and procedural confidence before real surgical interventions.
Overall, this collaborative clinical validation confirmed that the hybrid CAD–molding model faithfully reproduces MRI-based anatomy, supports realistic operative simulation, and provides a high-quality educational tool for surgical preparation and training in congenital cardiac surgery.
Surgeon and Expert Feedback
A structured post-workshop survey was distributed to participating surgeons and cardiologists, as well as specialists attending the 7th Meeting of the World Society for Pediatric and Congenital Heart Surgery and the 1st African Society for Pediatric and Congenital Heart Surgery Conference. The questionnaire evaluated 5 criteria:
Internal and external anatomical fidelity, Accuracy in reproducing TOF morphology, Tactile realism of the silicone material, Utility for preoperative corrective training, and Educational value for medical students.
Analysis of survey responses revealed the following:
82% (103/125) to 88% (110/125) of respondents rated the model anatomically faithful to real heart structures; 100% confirmed accurate representation of TOF morphology; 75% (94/125) judged the tactile realism comparable to real cardiac tissue; and 91% (113/125) affirmed that the model effectively supported corrective surgical training.
Moreover, all respondents (100%) agreed that the model enhances medical students’ comprehension of intracardiac blood flow and spatial relationships.
These outcomes collectively demonstrate that the proposed hybrid process yields clinically realistic, educationally valuable, and reproducible pediatric heart models.
Synthesis of Results
The combination of quantitative process optimization and qualitative surgeon feedback provides an integrated validation of the proposed workflow.
In summary, validation confirmed that the hybrid CAD–molding process is a cost-effective and efficient alternative to conventional multi-material 3D printing for CHD modeling. This approach ensures anatomical fidelity, realistic mechanical behavior, and broad educational applicability, offering a powerful tool for both surgical planning and hands-on simulation training in pediatric cardiology.
These results collectively demonstrate that the hybrid CAD–molding process bridges the gap between medical imaging and hands-on surgical simulation, providing a reproducible and cost-efficient workflow adaptable to various congenital cardiac pathologies.
Discussion
Importantly, MRI-to-model comparison confirmed that the physical reconstruction accurately preserved the spatial relationships that guide operative strategy in TOF—particularly the configuration of the VSD, the morphology of the right ventricular outflow tract obstruction, and the degree of aortic override. This fidelity strongly supports the model's suitability for both preoperative planning and hands-on procedural simulation.
The present study further demonstrates that a flexible and hollow TOF model derived from MRI segmentation can meaningfully enhance surgical education and the preoperative understanding of complex CHD. Unlike conventional rigid 3D-printed models, the hybrid CAD–molding approach faithfully reproduces both external morphology and internal pathways, allowing surgeons to engage with clinically relevant anatomical details. The capacity to visualize, access, and manipulate intracardiac structures within a deformable medium was repeatedly emphasized by pediatric cardiac surgeons during validation.
Our findings are consistent with emerging literature showing that operable, anatomically accurate models offer significant pedagogical advantages over rigid prints and virtual reconstructions. Prior studies have noted that rigid models are limited in their ability to simulate procedural steps such as resection or patch placement. During our international workshop, surgeons highlighted that the ability to incise, retract, and suture within a compliant material more closely replicated intraoperative conditions, thereby improving spatial orientation and procedural confidence.
Another notable advantage of the proposed workflow is its accessibility and reproducibility. By reducing fabrication time and cost while maintaining anatomical precision, this method lowers one of the major barriers to the wider adoption of patient-specific models in congenital cardiac training. The strong consensus among participants regarding the model's educational value also supports its scalability across diverse surgical settings.
Several limitations should be acknowledged. MRI resolution remains a key determinant of segmentation accuracy, and certain intracardiac structures required refinement before mold design. Moreover, although surgeon feedback was consistently positive, future work incorporating quantitative biomechanical assessments would strengthen evaluations of tactile realism.
Overall, this study highlights the clinical and educational relevance of combining MRI-based anatomical reconstruction with a malleable physical model. The hybrid CAD–molding workflow provides a practical and realistic tool for improving training, enhancing preoperative planning, and deepening anatomical comprehension in TOF.
Conclusion
This study introduces a reproducible workflow that transforms MRI-derived anatomy into a flexible and anatomically accurate TOF heart model using a hybrid CAD–molding process. The model accurately reflects key structural features of TOF and can be used for hands-on surgical simulation. The favorable feedback obtained during international validation confirms its educational and clinical relevance. Future work will focus on improving segmentation accuracy, refining material properties, and extending the method to additional congenital heart defects.
Limitations and Future Perspectives
Despite the promising outcomes of this study, certain limitations were encountered, particularly those related to the precision of the MRI imaging used. The resolution of the acquired images did not always allow for direct and detailed segmentation of intracardiac structures, requiring additional steps of smoothing and manual correction. In this context, the use of higher-resolution MRI systems would represent a major improvement, enabling the generation of more accurate models without post-processing. Furthermore, the development of an artificial-intelligence-based tool dedicated to the automatic and targeted segmentation of cardiac structures appears to be a promising avenue to significantly reduce processing time and enhance the reproducibility of the workflow. In the long term, such an AI-driven solution could also incorporate a decision-support module capable of analyzing critical parameters specific to each pathology; thereby guiding both model design and surgical strategy. Finally, multicentric validation studies will be required to objectively assess the fidelity of the hybrid models to MRI-derived data and to quantify their educational and clinical impact.
Supplemental Material
sj-docx-1-pch-10.1177_21501351261419053 - Supplemental material for An Innovative Hybrid Process for Realistic Three-Dimensional Heart Modeling and Surgical Simulation of Tetralogy of Fallot
Supplemental material, sj-docx-1-pch-10.1177_21501351261419053 for An Innovative Hybrid Process for Realistic Three-Dimensional Heart Modeling and Surgical Simulation of Tetralogy of Fallot by Aya Abiya, Fatima Bouyahia, Mouhcine El mardouli and Drissi Boumzebra in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Acknowledgments
We would like to acknowledge the Marrakech Innovation City of UCA, which has supported us in the patent application process for the procedure, currently underway.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.