
Abstract
Background
In 2019, the American Society of Extracorporeal Technology (AmSECT) approved the inaugural Standards and Guidelines for Pediatric and Congenital Perfusion Practice. These standards and guidelines were created with the intent of periodic revision to ensure continued alignment with evolving best practices. In 2023, an AmSECT subcommittee initiated this review in consideration of the current literature and contemporary clinical practices.
Methods
The subcommittee, consisting of pediatric and congenital perfusionists, conducted a systematic literature review assessing each standard and guideline to determine if current evidence supports elevation of guidelines to standards, incorporation of new guidelines or standards, or whether existing standards and guidelines should remain unchanged. AmSECT's adult Standards and Guidelines for Perfusion Practice (2023) updates were also considered. Proposed revisions were reviewed by the 2024 AmSECT International conference attendees, AmSECT Pediatric and Congenital Perfusion Committee, AmSECT Fellows of Pediatric Perfusion (FPP), and the AmSECT International Consortium for Evidence-Based Perfusion (ICEBP).
Results
Regarding pediatric and congenital specific changes, 5 guidelines were elevated to standards, and 3 new guidelines and 1 standard were introduced. Additionally, 5 patient safety-related standards and 1 additional guideline were adopted from the Standards for Perfusion Practice (2023) document.
Conclusion
Over the course of 2 years, consisting of an extensive literature review and feedback from multiple stakeholders, the 2025 update to the Standards and Guidelines for Pediatric and Congenital Perfusion Practice was approved by AmSECT leadership, ratified by an AmSECT membership vote, and subsequently endorsed by the Congenital Heart Surgeons' Society.
Keywords
Introduction
Standards and Guidelines provide a framework for best practices, quality improvement, and methodology to reduce patient harm. 1 National organizations such as the Centers for Disease Control (CDC), World Health Organization (WHO), The Joint Commission (TJC), the Institute of Medicine (IOM), and the Occupational Safety and Health Administration (OSHA) are a few organizations that implement, regulate, and promote the use of standards to improve patient safety and outcomes. Specific to cardiac surgery, the Society of Thoracic Surgeons (STS), the Society of Cardiovascular Anesthesiologists (SCA), and the American Association for Thoracic Surgery (AATS) have clinical practice guidelines that they craft and endorse as a profession.2–4 While these standards and guidelines are of value, they do not directly address perfusion practices.
The first guidelines for perfusion practice were published in 1993 by the American Society of Extracorporeal Technology (AmSECT). 5 More recently, the International Consortium for Evidence-Based Perfusion (ICEBP), in collaboration with AmSECT, updated these guidelines in 2013, 2017, and 2023 and are known as Standards and Guidelines for Perfusion Practice and endorsed by the STS, SCA, and AATS. 6 This document, although foundational, did not adequately address the physiological and technical considerations inherent in pediatric and congenital perfusion practice. Recognizing this critical gap, AmSECT commissioned the development of pediatric-specific standards and guidelines for perfusion practice. With the support of AmSECT's Pediatric and Congenital Perfusion Committee (PCPC), a subcommittee was tasked with the development of a comprehensive, evidence-based document uniquely tailored to the complex and nuanced needs of pediatric and congenital cardiac patients.7,8 These efforts culminated in the first-ever Standards and Guidelines for Pediatric and Congenital Perfusion and were ratified and published in 2019. Endorsements from the Congenital Heart Surgeons’ Society (CHSS) and the Congenital Cardiac Anesthesia Society (CCAS) were obtained.
Prior to 2019, there were no official documents to guide the practice of pediatric perfusion worldwide. This publication marked a significant advancement in standardizing care, enhancing patient safety, and reducing practice variability in pediatric perfusion. In 2021, an international survey of perfusion practices for pediatric and congenital heart surgery revealed that 98% of centers in North America adopted these standards and guidelines, indicating that the document offered significant clinical implications. 9 To ensure continued alignment with current research, evidence-based practices, and clinical innovations, periodic revision of the standards and guidelines was necessary. In 2023, an AmSECT PCPC subcommittee initiated this process.
Materials and Methods
The process for updating the Standards and Guidelines for Pediatric and Congenital Perfusion (2019) commenced following the release of the newly updated adult Standards and Guidelines for Perfusion Practice document in 2023. The AmSECT PCPC-appointed subcommittee consisted of pediatric and congenital perfusionists from varying institutions across the United States and was chosen specifically for their expertise and background in the field. The subcommittee's primary objective was to evaluate the latest evidence, gather input from key stakeholders, and provide guidance to perfusionists conducting pediatric and congenital cardiopulmonary bypass (CPB) through an updated standards and guidelines document.
The review process began with assessing the updates made to the adult Standards and Guidelines for Perfusion Practice (2023) and to evaluate their applicability to pediatric and congenital perfusion. After that, each section of the Standards and Guidelines for Pediatric Practice (2019) was individually evaluated and reviewed to determine if the current evidence and practice trends suggest changes or additions to the existing document. These sections are staffing, communication and hand-off, medical records, checklists, temperature management, anticoagulation, arterial blood pressure, blood gas management, hematocrit expectations, technology updates, cerebral and somatic oximetry, indexed oxygen delivery and consumption, ventilation strategies, blood flow targets, CPB circuitry, CPB circuit priming techniques, blood product management, ultrafiltration, and quality improvement.
When evaluating the literature, an emphasis was placed on journal articles published between 2019 and 2024 to support existing and new recommendations. Inclusion criteria consisted of peer-reviewed pediatric and cardiac surgery-specific publications only. No animal studies were included. Although the literature review prioritized recent research, key references over 10 years old were retained when newer evidence was lacking. Any relevant new literature or literature overlooked previously was presented and discussed by the subcommittee as well. After detailed analysis of over 140 publications and committee consensus, the most up-to-date publications and research were added to support recommendations for the revised pediatric and congenital standards and guidelines.
A draft of the updated standards and guidelines with highlighted changes was presented to multiple parties for comment. This process in its entirety is depicted in Figure 1. Initially, the draft standards and guidelines were presented in March of 2024 to pediatric perfusionists attending the AmSECT International Meeting in New Orleans, LA. Feedback was captured by providing a code to attendees, which directed them to a survey. The same draft revision of the standards and guidelines was submitted to the AmSECT PCPC committee in June 2024 for review. Additionally, in August 2024, a survey was sent to the Fellows of Pediatric Perfusion (FPP) listserv for feedback and in October 2024 to the ICEBP committee. All feedback was reviewed and considered by subcommittee members and incorporated into the final draft where applicable.
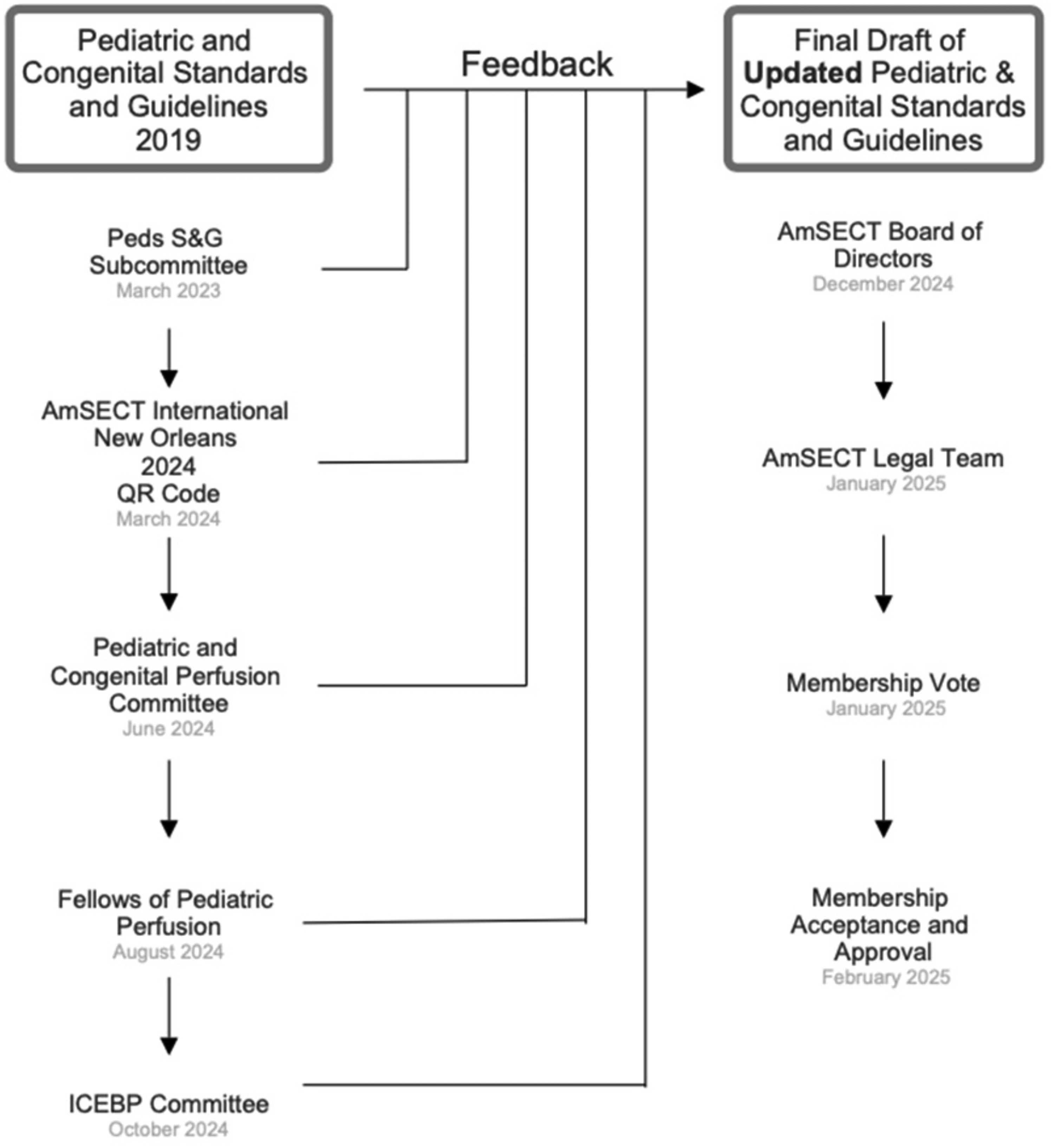
Review and Approval Process for the Revision of the Standards and Guidelines for Pediatric and Congenital Perfusion Practice. Abbreviations: AmSECT, American Society for Extracorporeal Technology; ICEBP, International Consortium for Evidence-Based Perfusion.
Once the final draft was composed, it was presented to the AmSECT Board of Directors, followed by the AmSECT legal team. After a membership vote in January 2025, the AmSECT membership approved the revised Standards and Guidelines for Pediatric and Congenital Perfusion Practice (2025). This document was endorsed by surgical peers from the Congenital Heart Surgeons’ Society (CHSS) in October 2025.
Results
As a result of this review, the subcommittee accepted many of the updates to the adult Standards and Guidelines for Perfusion Practice (2023) document. These updates encompassed revised definitions, consolidation of content, improved clarity, rewording of multiple standards and guidelines, and the inclusion of new ones (Table 1). Many of these inclusions are centered around patient safety, which transcends patient size or age. The adopted standards and guidelines from the Standards and Guidelines for Perfusion Practice (2023) included:
Summary of Current Standards and Guidelines for Pediatric and Congenital Perfusion Practice (2025) Document and Highlighted Modifications.
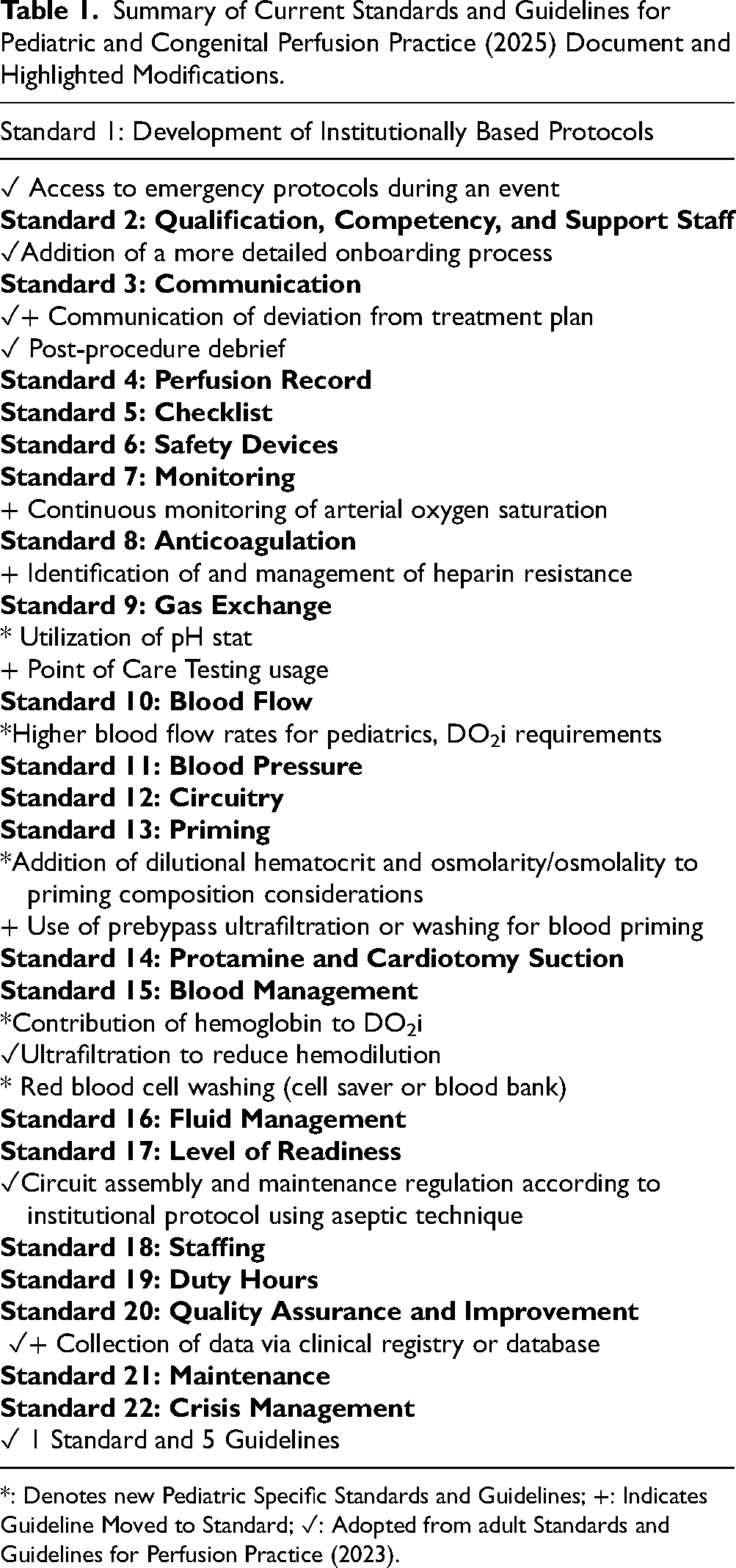
*: Denotes new Pediatric Specific Standards and Guidelines; +: Indicates Guideline Moved to Standard; ✓: Adopted from adult Standards and Guidelines for Perfusion Practice (2023).
The updated versions for both the Standards and Guidelines for Perfusion Practice (2023) and the Standards and Guidelines for Pediatric and Congenital Perfusion Practice (2025) include the defined usage of the word continually and continuously. The word “continuously” describes an action that occurs without ceasing, and the word “continually” describes an action that occurs frequently or regularly. Given the exacting nature of caring for pediatric and congenital patients on cardiopulmonary bypass, 6 standards and guidelines that previously suggested a practice to be done continually were elevated to continuous or without ceasing. Examples include monitoring of hemoglobin/hematocrit, arterial and venous oxygen saturation, and cerebral and somatic oximetry while on cardiopulmonary bypass. Continuous surveillance of critical parameters highlights the imperative for pediatric and congenital perfusionists to administer care that is both consistent and precise. This obligation is further substantiated by advancements in medical technology, which facilitate the continuous monitoring of patients' physiological parameters.
Regarding pediatric-specific updates to the Standards and Guidelines for Pediatric and Congenital Perfusion Practice, 5 guidelines were elevated to standards:
Discussion
The 2025 update of the Standards and Guidelines for Pediatric Practice reflects trends in the literature and environmental challenges experienced since 2019, specifically the COVID-19 pandemic. This revision emphasizes emergency preparedness, operative team communication and collaboration, and the development of institutional protocols for clinical and crisis management. Effective communication between the perfusionist and the operative team is a critical component of intraoperative care. Standard practices outlined in this revision include communicating deviations from intended treatment care plans and the use of an evidence-based and collaborative approach to minimizing blood loss perioperatively. Conducting post-procedural debriefs is encouraged as are efforts to promote quality and safety through perfusion-specific data collection with participation in a database and/or registry.
Surveillance of critical clinical parameters on CPB was highlighted in this revision. Several clinical parameters were updated to be monitored continuously on CPB, including arterial oxygen saturation, which was elevated to a standard. Access to point-of-care blood gas analyzers for timely and accurate evaluation was included as a standard. Additionally, consideration for DO2i was added due to the higher metabolic needs of the pediatric patient and the contribution of hemoglobin (standard) and higher flow rates (guideline) to maintain adequate DO2i. Perfusion management techniques, specifically the treatment of exogenous blood with prebypass ultrafiltration and/or the use of washed packed red blood cells (pRBCs) during the priming sequence was deemed a standard in this revision. Guidelines specify washing pRBCs with cell salvage technology or blood bank technology prior to administration at other times during CPB. Consideration for pH-stat blood gas management strategy during hypothermia for neonates and infants was also stated. In total, 5 existing guidelines were elevated to standards, and 1 new standard was introduced based on compelling evidence.
The Standards and Guidelines for Pediatric Practice (2019) were envisioned to be a “living document” and continuously reviewed at regular intervals. Following the 2025 update, the subcommittee anticipates a third revision in the next 3 to 4 years. This was the intent when reviewing the 2019 version; however, it was delayed due to the anticipated release of the adult Standards and Guidelines for Perfusion Practice (2023). In practice guidelines-related publications, it is recommended that guidelines be reassessed for validity every 3 years, as nearly half of all guidelines are outdated after 6 years.10,11 Despite the delays faced in composing the current version, the timeline was consistent with those of other organizations such as the American Heart Association, with updates taking as long as 5–8 years until publication. 12
The review cycle for evaluating the Standards and Guidelines for Pediatric Perfusion should be brief, as new data and techniques continue to evolve rapidly. Perfusion-specific registries such as The Perfusion Measures and Outcomes (PERForm) registry and the PediPERForm Learning Network registry are also driving changes to perfusion practice. 13 These registries can ascertain discrete perfusion practices on cardiopulmonary bypass and “reflect adherence to evidence-based guidelines and professionally based standards and guidelines.” 14 Additionally, registries are collaborating to link patient data from the operating room to the intensive care unit. An example of this collaboration is PediPERForm and Pediatric Cardiac Critical Care Consortium (PC4). 13 As registry data expands and inter-registry collaboration continues, identifying practice trends will become easier and may catalyze research and quality publications, reinforcing the need for frequent review of the standards and guidelines. Going forward, the subcommittee plans to convene semi-annually to evaluate emerging topics for consideration during the formal review of the document.
The Standards and Guidelines for Pediatric Perfusion (2025) added multiple new standards and guidelines following a 5-year period. Despite the inclusion of these references, conclusive evidence is lacking throughout much of the document. Limitations to this work include a lack of prospective randomized controlled studies, the use of surveys to evaluate practice trends, and a generalized lack of consensus among perfusionists regarding clinical practices. Additionally, given the small subcommittee, there is potential that the biases of the members affected the evidence evaluated and chosen. Moving forward, the next revision may include an improved system by which evidence is selected, evaluated, and ranked.
The absence of a multidisciplinary collaboration with congenital and pediatric cardiac surgeons, anesthesiologists, intensivists, and perfusionists may have limited this process. A collaborative approach could have enhanced the literature review process, breadth of information presented, and possibly offered a more comprehensive evaluation of contemporary science and clinical practices in the development of this revision. Similar guideline documents for perfusionists, such as the European Association for Cardio-Thoracic Surgery (EACTS) for European adult cardiac surgery, are developed in a multidisciplinary fashion consisting of perfusionists, surgeons, anesthesiologists, and intensivists collaborating to generate guidelines to guide clinical practice in adult cardiopulmonary bypass.15–17 However, the EACTS document differs substantially in scope and scale than Standards and Guidelines for Pediatric Practice document and matching this effort would entail a significant shift in goals and procedures established in previous revisions. However, endorsement from surgical peers was obtained from the Congenital Heart Surgeons’ Society (CHSS). Members of these organizations were not included in the subcommittee and therefore did not assist in the production of the revision or the assessment of the evidence. Opportunities to seek endorsements internationally may be possible with future revisions.
Perfusion practices are continually evolving with the introduction of new technology, devices, and clinical practices.9,18 Additionally, the exponential growth in medical knowledge, coupled with an overwhelming volume of research publications, poses significant challenges for clinicians striving to stay informed of current best practices.19,20 As such, the use of clinical practice guidelines has become an essential tool for clinicians as they are based on an exhaustive, systematic review of available literature and are composed by field experts. Additionally, published standards and guidelines not only keep clinicians apprised of the latest evidence but may promote the standardization of practice techniques. 21 Updating the standards and guidelines ensures alignment with advancements in technology and research, strengthens the profession's credibility, and may promote quality and consistency of care provided to pediatric patients undergoing cardiopulmonary bypass.
Footnotes
Acknowledgements
The authors wish to acknowledge all the perfusionists who reviewed the draft documents for this revision. Your contribution of time, expertise, feedback, and support for this endeavor has been invaluable to this effort. The integrity and strength of this document are a direct reflection of these contributions.
Author Contributions
All authors of this manuscript were responsible for developing the strategy for the review process, collecting and evaluating feedback, revising the 2025 Update to the Standards and Guidelines for Pediatric and Congenital Perfusion, and finalizing this manuscript.
Data Availability
The data supporting this work are publicly available and cited in the References section of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
IRB was unnecessary for this research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.