
Abstract
Anomalous cardiac venous drainage is a rarely reported condition typically associated with atresia of the coronary sinus ostium. We present a very unusual case of a newborn with dual drainage of the cardiac veins to both the coronary sinus and to a vertical vein draining into the innominate vein. The patient developed myocardial ischemia in response to obstruction of the vertical venous pathway.
Introduction
Anomalous cardiac venous drainage is a rarely reported condition typically associated with atresia of the coronary sinus (CS) ostium.1,2 The current literature on this subject is comprised largely of single case reports and indicates that anomalous drainage of the great cardiac vein is either into the superior vena cava via a vertical vein (most common)3,4 or directly into the left atrium (less common). 5 Pediatric cases invariably are found in conjunction with the presence of complex congenital heart disease.6–8 In contrast, the majority of adults with anomalous cardiac venous drainage are identified as an incidental finding. 9
Impairment of coronary venous drainage due to obstruction or stenosis can increase coronary venous pressure, compromise myocardial perfusion, lead to impaired myocardial contractility, and in severe cases result in myocardial infarction. 10
We present a case of a newborn with tetralogy of Fallot (TOF) and a left pulmonary artery arising from a patent ductus arteriosus (PDA). This patient was subsequently found to have dual drainage of the great cardiac vein into both a vertical vein connecting to the innominate vein and a separate pathway to the CS.
Case Presentation
A male newborn was delivered at term, weighing 3.5 kg. Vital signs were stable. Transthoracic echocardiography demonstrated TOF and a left pulmonary artery arising from a PDA. An incidental note was made of an abnormal vessel draining into the innominate vein. Prostaglandin E1 (PGE1) infusion was started to provide blood flow to the left pulmonary artery. A computed tomography (CT) scan was performed and demonstrated dual drainage of the cardiac veins with a vertical vein draining to the innominate vein and a cardiac vein draining to a relatively small CS ostia.
On the eighth day of life, the patient underwent unifocalization of the left pulmonary artery into the main pulmonary artery without ventricular septal defect (VSD) closure using cardiopulmonary bypass. Surgical examination confirmed the presence of a small cardiac vein draining into the innominate vein. Intraoperative transesophageal echocardiography (TEE) demonstrated good function of both the left ventricle (LV) and right ventricle (RV) and this was confirmed by two postoperative echocardiograms. The early postoperative clinical course was uneventful.
Two weeks following the procedure, the patient presented with acute dysfunction of the RV. Cardiac catheterization was performed and revealed stenosis of the anomalous cardiac vein (Figure 1A and 1B). It was inferred that this stenosis of the anomalous cardiac vein was directly related to the development of dysfunction of the RV. Balloon angioplasty was performed using a 3.5 mm Solaris balloon (Figure 2). During the procedure, complete closure of the anomalous cardiac vein occurred secondary to clot formation (Figure 3), leading to massive myocardial dysfunction with ST elevation. Alteplase (ATP) was immediately injected directly into the anomalous cardiac vein, and rapid improvement in cardiac function was observed. After a few minutes, a contrast agent was administered, showing the return of circulation in the anomalous cardiac vein (Figure 4). In the following days, echocardiography showed gradual improvement in RV function.
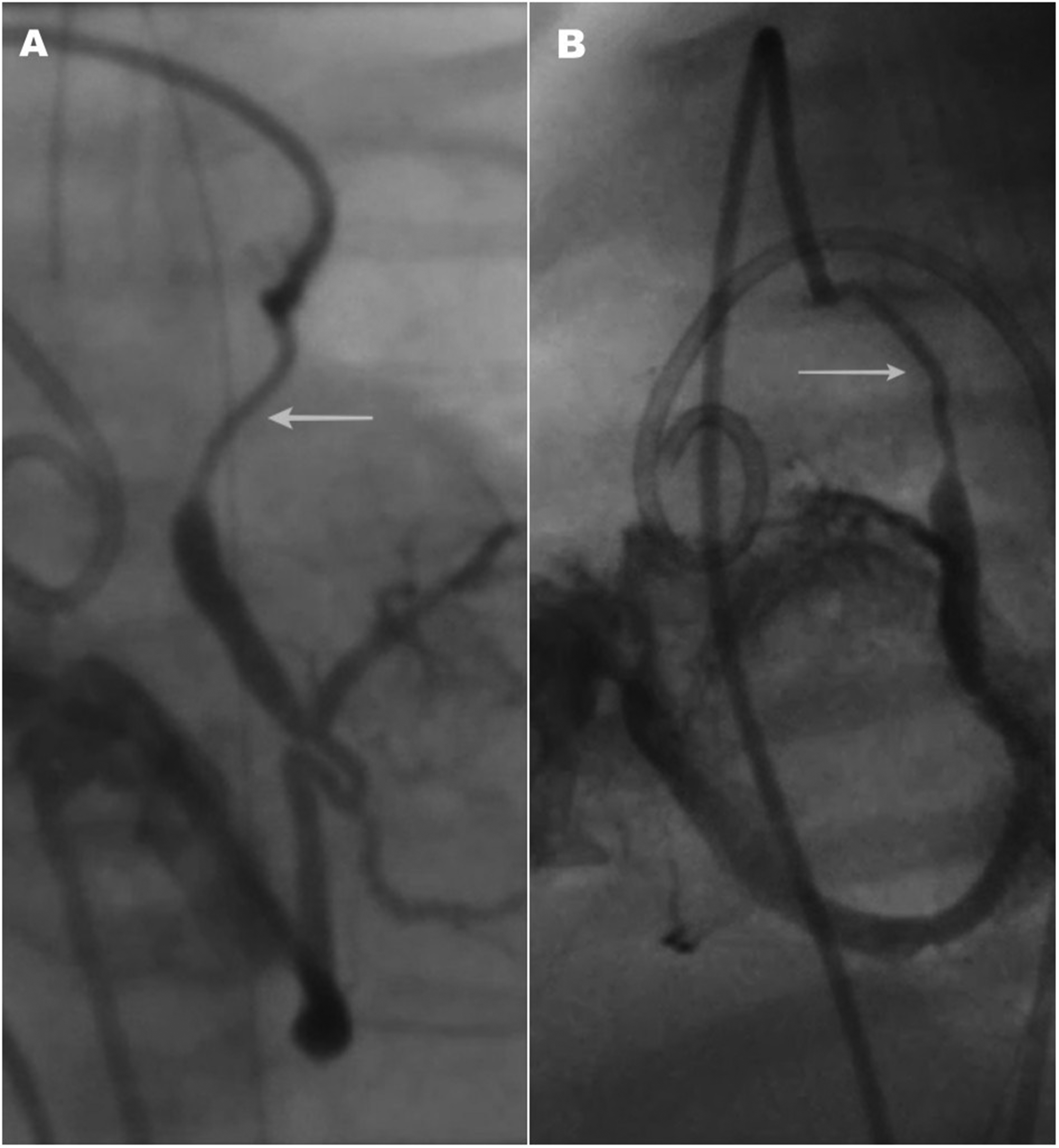
(A) Selective angiography of the anomalous cardiac vein (anteroposterior view). White arrow marks the obstructed distal part of the vessel. (B) Selective angiography of the anomalous cardiac vein (lateral view). White arrow marks the obstructed distal part of the vessel.
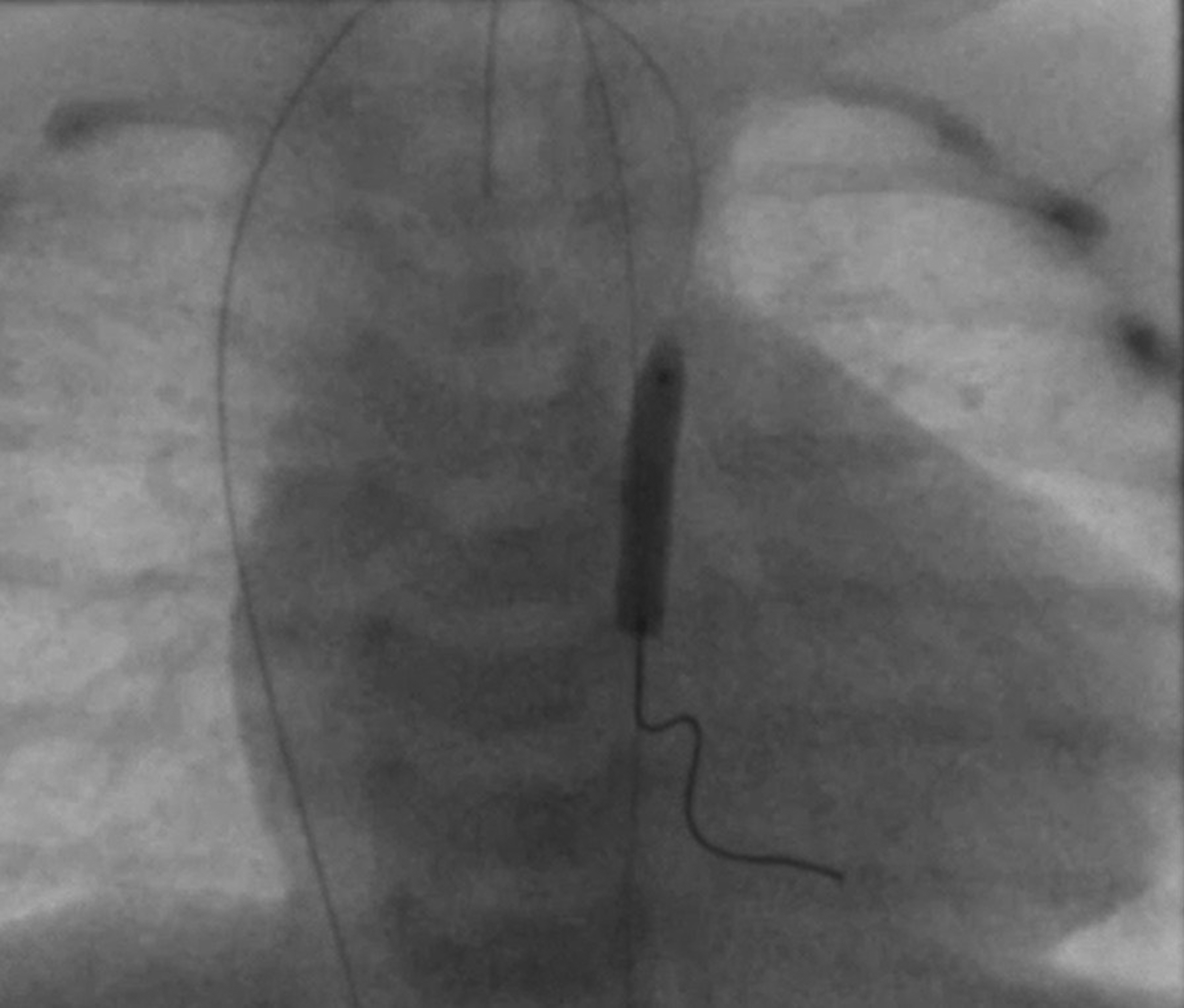
Balloon angioplasty of the anomalous cardiac vein (anteroposterior view).

Brachiocephalic vein selective angiography after balloon dilation. White arrow marks the tip of the coronary guidewire placed in the occluded anomalous cardiac vein.

Brachiocephalic vein selective angiography post treatment. White arrow marks recanalized anomalous cardiac vein.
During the following month, a decision was made to perform full correction of the defect. The postoperative course was uneventful. A few months later, during routine echocardiography, there was no flow in the anomalous cardiac vein. The patient underwent a CT scan which confirmed closure of the anomalous vein with developing collaterals to other veins of the heart. The function of both ventricles remained normal and the patient was discharged home in good condition.
Discussion
This case report describes a very rare variant of anomalous cardiac venous drainage with a vertical vein draining to the innominate vein and a separate vein draining to a relatively small CS ostia. This was clinically silent until the postoperative period when the patient developed impaired RV function with evidence of myocardial ischemia. It is unclear why this occurred when it did (2 weeks postoperatively), but we would hypothesize that it was a consequence of a postoperative inflammatory process adjacent to the vertical vein. The clinical course highlights how exquisitely sensitive cardiac function was to an acute increase in coronary venous pressure. The observation that the myocardial ischemia specifically affected the RV would infer that the RV was drained by the vertical vein whereas the LV drained to the CS. In this patient, ligation of the anomalous cardiac vein would likely have resulted in irreversible myocardial dysfunction. It is also notable that while acute occlusion resulted in myocardial ischemia, a gradual narrowing allowed for the formation of collateral circulation with good heart function.
The literature on anomalous cardiac venous drainage in pediatric patients is quite limited and largely concentrated in patients with complex congenital heart disease. Several pediatric case reports refer to patients with single ventricle and describe the importance of redirecting the vertical vein connection prior to a bidirectional Glenn to avoid physiologic obstruction of the cardiac veins.6,7 In the case reported by Rust et al., 8 obstruction of CS flow in a patient with an atrioventricular septal defect resulted in profound myocardial dysfunction. These case reports would support the premise that obstruction of coronary venous drainage can result in serious adverse consequences.
In summary, anomalous cardiac venous drainage is a rare anatomic entity but it is imperative to identify when performing congenital heart interventions as there is the potential for encountering serious adverse consequences if this drainage is inadvertently obstructed.
Footnotes
Author’s Statement
The authors confirm that written informed consent for publication of clinical details and images was obtained from the patient's parents/legal guardians.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.