
Abstract
The adult population with congenital heart defects of varying complexity is growing rapidly. This includes a significant number of patients over the age of 18 who underwent surgery in early childhood to correct conotruncal anomalies and septal defects. While patients with a functional single ventricle palliated with the Fontan procedure are still relatively rare in developing countries, the expertise gained from managing these patients in expert centers in Europe and the United States of America, as well as the success of pediatric cardiac surgery, has drawn increasing attention to this subject. In this review article, we aim to discuss the unique pathophysiology of Fontan circulation and clinical issues in the management of adult patients, with a particular focus on identifying specific predictors of heart failure decompensation and potential complications in this population.
Keywords
Introduction
Approximately 1 in 10,000 children are born with a functional single ventricle (FSV), and the survival rate to adulthood without palliative surgery in these patients remains low. 1 The complexity of congenital heart disease (CHD) in most children with FSV precludes restoration of biventricular physiology, necessitating surgical sacrifice of the subpulmonary ventricle to maintain systemic cardiac output. This univentricular circulatory arrangement is known as the Fontan circulation, named after Francis Fontan, a pioneering French pediatric cardiac surgeon who first performed the procedure in 1968 and published 3 successful cases in 1971. 2
Originally intended for patients with tricuspid atresia, the success of this surgery led to its application being expanded to other complex CHDs, such as double-inlet left ventricle (LV), hypoplastic left heart syndrome (HLHS), and unbalanced complete atrioventricular septal defect (AVSD). The principle of this palliative repair is to redirect systemic venous blood from the caval veins directly to the pulmonary arteries. This creates a circulation in which the pressure gradient between central venous pressure (CVP) and ventricular end-diastolic pressure (EDP), along with the muscular pump, becomes the driving force for blood flow in the lungs. Consequently, pulmonary vascular resistance, systolic and diastolic function of the FSV, and competence of the systemic AV valve are the primary determinants of cardiac index and proper functioning of the Fontan circulation.
The Fontan procedure represents the final stage of univentricular palliation. Preceding stages depend on the specific congenital anatomy and the child's clinical status. Initial surgical procedures typically aim to establish reliable pulmonary blood flow while preventing pulmonary hypertension and microvascular remodeling. Common first-stage interventions include the Norwood procedure, 3 a modified Blalock-Taussig-Thomas shunt, 4 pulmonary artery banding, 5 and, in recent years, bilateral branch pulmonary artery flow restrictors. 6 The second stage is usually a bidirectional cavopulmonary anastomosis (bidirectional Glenn procedure or hemi-Fontan), 7 where superior vena caval blood drains directly into the pulmonary artery. 8 This procedure is typically performed at 4 to 6 months of age. The venous blood from the lower body continues to return to the heart via the inferior vena cava.
The final Fontan procedure completes the cavopulmonary connection. The original technique described by Fontan involved an atriopulmonary connection, channeling blood from both caval veins through the right atrium into the pulmonary artery. Although Fontan conceptualized the “ventricularization” of the right atrium, it was the Argentinian surgeon Guillermo Kreutzer who, independently in 1971, pioneered the technique of direct atriopulmonary connection without an intervening pumping chamber. 9 However, these early modifications were associated with significant complications, including intra-atrial thrombus formation and thromboembolism. To mitigate these risks, the lateral tunnel modification was introduced by de Leval et al in 1988, 10 and the extracardiac conduit technique was developed by Marcelletti et al. 11 These modern techniques exclude the right atrium from the circulation, directing inferior vena caval blood to the pulmonary artery via an intracardiac tunnel or an extracardiac prosthetic conduit.
The absence of a subpulmonary ventricle in the Fontan circulation results in chronically elevated pressures within the caval system, nonpulsatile pulmonary blood flow, and a mildly reduced systemic cardiac output. 12 Additional benefits include linear blood flow without disturbances, as well as blood flow from the coronary sinus to the lower-pressure atrium. A successful palliation provides significant benefits, such as improved arterial oxygen saturation and the elimination of chronic volume overload on the FSV. As a result, most patients can lead relatively normal lives into early adulthood. However, long-term follow-up of Fontan patients into their fifth decade reveals high rates of morbidity, including multiorgan dysfunction, premature mortality, and a frequent eventual need for heart transplantation. 13
The current global Fontan population is estimated at ∼70,000 individuals. 14 According to an epidemiological model by Plappert et al, 15 the number of Fontan patients is projected to increase by nearly 20% by 2030 (from 66 to 79 per million population). Furthermore, the proportion of adult patients within this population is expected to rise from 55% to 64%. Due to advancements in surgical techniques and medical therapy, contemporary adult Fontan patients already exhibit high survival rates. For instance, in a registry of Fontan patients older than 16 years, Dennis et al 16 report survival rates of 90% at age 30 and 80% at age 40. Notably, however, by age 40, only 41% of patients remained free of major adverse events, including Fontan failure, sustained supraventricular tachycardia, stroke, thromboembolism, or pacemaker implantation. The right dominant ventricle is associated with a poor 10-year survival rate, which is 79% in comparison with 92% survival in left dominant ventricles. 17
Heart failure (HF) is a severe complication and one of the leading causes of hospitalization and death in adults with CHD. According to the Dutch CONCOR registry, mortality rates among CHD patients hospitalized with HF reach 24% and 35% at 1 and 3 years, respectively. 18 Notably, adult Fontan patients are hospitalized significantly more frequently than adults with other forms of CHD, as reported by the Mayo Clinic. However, the cited study was unable to stratify all single ventricle patients by specific morphology, Fontan procedure type, or the presence of fenestration. 19
While circulatory failure in the general population typically results from systemic LV dysfunction, its pathophysiology in Fontan patients is more complex, involving various components of the Fontan circuit. Several conceptual frameworks for Fontan circulatory failure have been proposed. Book et al
20
described 4 distinct phenotypes:
Type I: Failure with low ejection fraction (EF). Type II: Failure with preserved EF. Type III: Failure with normal intracardiac pressures. Type IV: Failure with abnormal lymphatics.
Subsequently, the Advanced Cardiac Therapies Improving Outcomes Network (ACTION) Fontan Committee introduced a modified classification system, which provides a useful framework for discussing the principal pathophysiological problems and potential therapeutic directions. It also outlines 4 subtypes:
Type I: Cardiac/systemic ventricular dysfunction. Type II: Fontan pathway dysfunction. Type III: Lymphatic dysfunction. Type IV: Extracardiac (end-organ) dysfunction.
Although these subtypes may overlap, this classification effectively highlights the most vulnerable components of the Fontan circulation. As illustrated schematically in Figure 1, Types III and IV involve structures—namely the portal venous and lymphatic systems—that do not directly drive circulatory flow but whose function is critically dependent on central venous pressure. 21
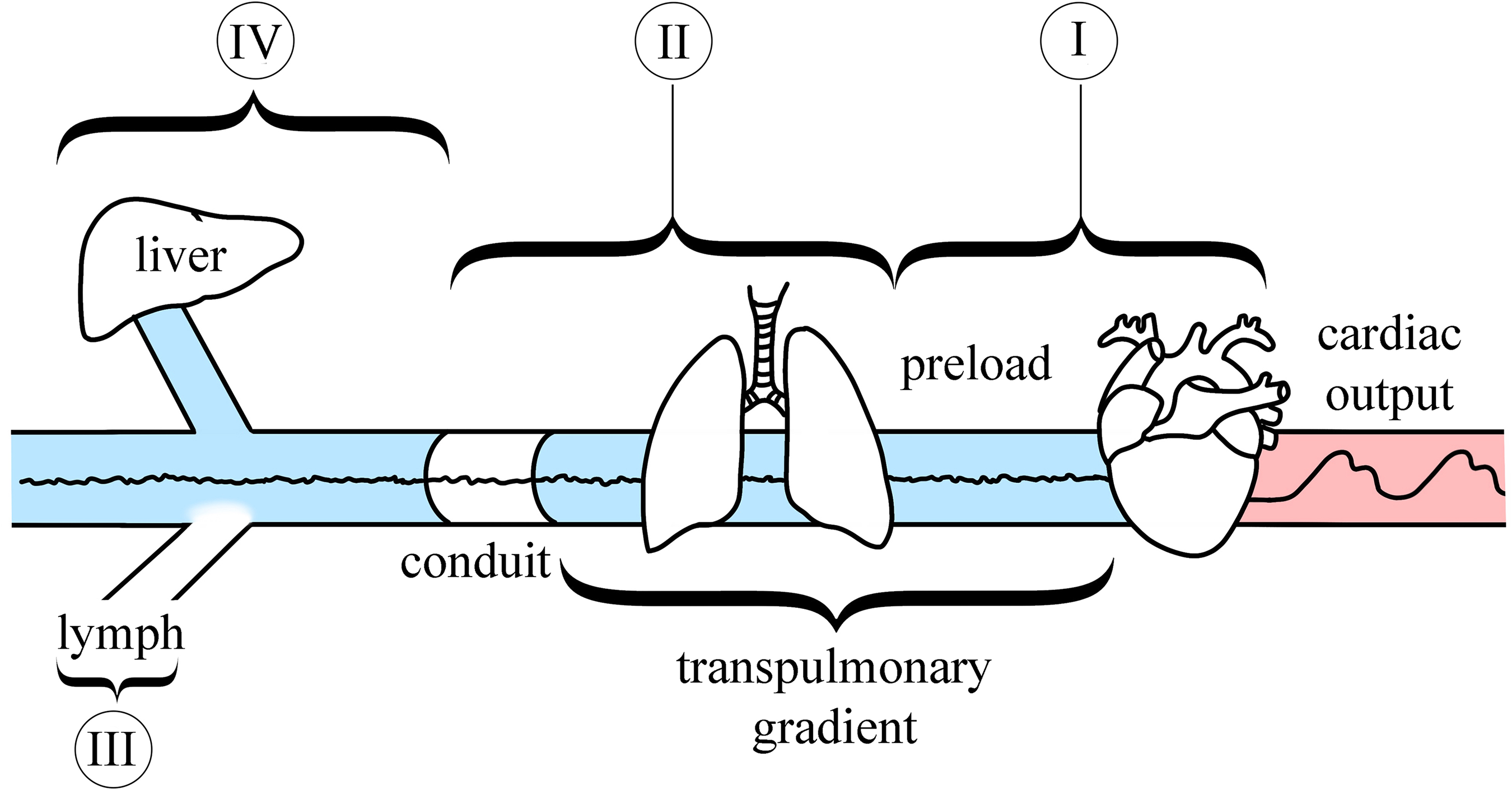
A schematic presentation of 4 types of Fontan circulation failure:
Type I: Cardiac/Systemic Ventricular Dysfunction
The initial congenital anatomy determines both the morphology of the systemic ventricular pump and the required surgical approach. The classic Fontan procedure for tricuspid atresia utilized the LV as a systemic pump; however, any CHD with left or right ventricle morphology can be palliated with the Fontan procedure. Beyond tricuspid atresia, the defects that could be completed into LV-dominant Fontan circulation are hypoplastic right heart syndrome (eg, pulmonary atresia with an intact ventricular septum), double-inlet LV, complex forms of Ebstein anomaly with severe atrialization of the right ventricle, and double-outlet right ventricle not amenable to the Rastelli operation. Conversely, the right ventricle dominant Fontan circulation is possible in HLHS and unbalanced AVSD with defects precluding adequate septation.
According to the 2021 European Society of Cardiology consensus, systolic dysfunction in Fontan patients is defined as an EF of the FSV below 50%. 22 An FSV EF below 30% indicates severe systolic dysfunction irrespective of ventricular morphology. For the first 2 to 3 decades post-Fontan, systolic function typically remains relatively stable before gradually declining. 23 Systolic FSV dysfunction is reported in 40% to 60% of Fontan patients undergoing evaluation for heart transplantation. 24 Clinically, this type of Fontan failure most closely resembles conventional HF with reduced EF, presenting with signs of elevated filling pressures, hepatic congestion, and a limited cardiac output reserve. 20 However, it is important to note that a low FSV EF may sometimes reflect reduced preload rather than intrinsic myocardial dysfunction, which could account for the frequent lack of response to inotropic therapy. 22
Systolic function and ventricular volumes are assessed using standard imaging modalities. While transthoracic echocardiography (TTE) is routinely employed, cardiac magnetic resonance imaging (MRI) is more accurate for evaluating the complex geometry of the FSV. 25 MRI-derived indices, such as the indexed end-diastolic volume of the FSV, have been shown to predict transplant-free survival. 26 Furthermore, late gadolinium enhancement on MRI provides valuable information on the presence and extent of myocardial fibrosis. In a study by Rathod et al, 27 28% of 90 Fontan patients (mean age 23.1 years) exhibited myocardial fibrosis on MRI. This finding was associated with lower FSV EF, higher indexed end-diastolic volume and myocardial mass, a greater incidence of regional wall motion abnormalities, and a higher frequency of non-sustained ventricular tachycardia.
Assessing FSV systolic function by standard TTE parameters (eg, EF and fractional shortening) is challenging due to complex ventricular anatomy. Alternative TTE parameters have been proposed, including the peak systolic velocity at the AV valve annulus (S′) by tissue Doppler imaging, 28 the myocardial performance index,29,30 and the rate of ventricular pressure rise during isovolumetric contraction (dP/dt). 31 Myocardial deformation imaging (strain) is a promising area of research. Global longitudinal and circumferential strain may be more sensitive indicators of early systolic dysfunction than EF. However, its clinical application in FSV patients remains investigational due to technical challenges. These include regional variability in measurement accuracy, the confounding effects of structural anisotropy and cardiac remodeling, and specific image acquisition requirements (eg, a frame rate of 60-90 fps).32,33 Nonetheless, studies have demonstrated good reproducibility of strain parameters and their correlation with MRI-derived right ventricular EF in patients with HLHS and a systemic right ventricle. 34
According to an American Heart Association consensus statement, diuretics are the mainstay of therapy for managing signs and symptoms of HF in the setting of progressive FSV systolic dysfunction. 14 The long-term clinical benefit of renin–angiotensin–aldosterone system inhibitors or β-adrenergic blockers in this population remains unproven. Nonetheless, treatment regimens established for biventricular physiology are often inappropriately applied to patients with failing FSV. 35
Another significant concern in Fontan patients is FSV diastolic dysfunction, defined by the ESC consensus as “a state of decreased single ventricle compliance leading to increased filling pressures.” 20 It is even more prevalent than systolic dysfunction in adult Fontan patients. 36 A study by Margossian et al 37 found that 68% of Fontan patients at age 12 met echocardiographic criteria for diastolic dysfunction. Occult diastolic dysfunction is also observed. Averin et al 38 assessed hemodynamic responses to rapid volume expansion (15 mL/kg saline bolus over <5 min). Criteria for occult dysfunction included a resting systemic ventricular EDP < 15 mm Hg that rose to ≥15 mm Hg post-expansion. The study revealed that 35% of Fontan patients exhibited occult diastolic dysfunction despite normal resting ventricular EDP. In a clinical trial of 89 adolescents and young adults, Peck et al 39 demonstrated that latent diastolic dysfunction ≥10 years post-Fontan is associated with adverse clinical outcomes and a poorer medium-term prognosis.
Potential contributors to diastolic dysfunction include abnormal FSV geometry, myocardial dyssynchrony, chronic hypoxia, fibrotic changes, and prolonged volume overload prior to the Fontan procedure, which can paradoxically lead to reduced preload reserve.40,41 This chronic preload reduction can trigger myocardial remodeling, increased ventricular stiffness, elevated filling pressures, and a progressive decline in CO. 12
The gold standard for diagnosing diastolic dysfunction is invasive measurement of the systemic ventricle EDP during cardiac catheterization. 42 Guidelines define diastolic dysfunction as a ventricle EDP or pulmonary artery wedge pressure (PAWP) ≥ 12 mm Hg at rest or ≥15 mm Hg after rapid volume expansion. 20
Exercise testing provides a comprehensive hemodynamic assessment. A study by Miranda et al 43 showed that Fontan patients had lower absolute PAWP values at rest and peak exercise compared with patients with HF with preserved EF (HFpEF), but higher values compared with those with non-cardiac dyspnea. This study included both fenestrated and non-fenestrated patients but did not account for fenestration status, a significant confounding factor for CO. Notably, the PAWP/CO slope was similarly steep in Fontan and HFpEF groups, suggesting comparable degrees of diastolic dysfunction.41,43 However, standardized methodology is lacking, and Miranda et al 43 emphasize the need to adapt PAWP diagnostic thresholds based on the patient's underlying physiology and body position during testing. Extrapolating from data in biventricular physiology, proposed criteria for significant diastolic dysfunction include a mean PAWP ≥25 mm Hg at end-expiration during supine exercise (roughly corresponding to a mean PAWP >20 mm Hg averaged over the respiratory cycle, 44 or a mean PAWP >20 mm Hg at end-expiration during upright exercise. A PAWP/CO slope >2 mm Hg/L/min, independent of body position, provides additional diagnostic and prognostic value, particularly in preload-limited states.41,45
A retrospective study by Miranda et al 46 correlated invasive and non-invasive data in 50 adult Fontan patients undergoing supine exercise catheterization, cardiopulmonary exercise testing (CPET), and NT-proBNP measurement. Fontan pressures and PAWP at rest and peak exercise strongly correlated with peak VO2 (using a < 50% predicted cutoff) and NT-proBNP levels (>300 pg/mL). Importantly, Fontan pressures and PAWP during exercise were the most reliable predictors of a composite outcome (death, transplant, HF hospitalization, or refractory arrhythmias) over ∼1 year of follow-up. A limitation was the inclusion of both fenestrated and non-fenestrated patients without stratification.
Another cross-sectional study of 195 adult Fontan patients from the Los Angeles registry identified factors associated with superior exercise tolerance. “High performers” (27 patients with peak VO2/kg >80% predicted) had lower BMI, mean Fontan pressure, higher CO, better HF class, greater physical activity, higher serum albumin and systemic arterial oxygen saturation, younger age at Fontan completion, and less severe liver fibrosis (all P < .05). 47
Noninvasive echocardiographic parameters of diastolic dysfunction in adult Fontan patients show limited correlation with invasive criteria. Reported parameters include abnormal diastolic wall strain, E/A ratio, pulmonary vein atrial reversal velocity, pulmonary systolic/diastolic flow ratio, and isovolumetric relaxation time. 40
While systolic and diastolic FSV dysfunction can develop independently due to fibrosis and chronic preload reduction, other common triggers exist.
In summary, FSV function and outflow, AVV competence, and sinus rhythm are critical determinants of a stable Fontan circulation and must be routinely assessed. While evaluating diastolic function remains challenging, with catheterization as the gold standard, recent studies suggest that integrating exercise testing with noninvasive techniques like advanced echocardiography and strain imaging can provide valuable information to aid in accurate diagnosis and management.
Type II: Fontan Pathway Dysfunction
Beyond cardiac function per se, the long-term durability and functional status of the Fontan circulation are determined by several unique hemodynamic and anatomical factors. The surgical technique is paramount. The original atriopulmonary connection is now considered inferior due to long-term risks of atrial thrombus formation and arrhythmias. Consequently, many patients with older modifications undergo conversion to an extracardiac conduit—a procedure requiring careful timing and expertise. In a series of 149 patients undergoing conversion at a high-volume center in Chicago, Backer and Mavroudis 50 reported an operative mortality of 2%, with 84% freedom from death or transplant at 10 years.
Conduit size and patency are critical for maintaining adequate preload. A study by Lee et al of 150 patients with extracardiac conduits found optimal exercise tolerance with a conduit size indexed to body surface area (BSA) of ∼12.5 mm/m2, while both larger and smaller conduits were associated with poorer functional status. 51 Over time, conduits can become relatively narrow due to somatic growth, calcification, pseudointimal hyperplasia, and luminal irregularities. Computed tomography studies show a reduction in minimal conduit area of up to two-thirds over a median follow-up of ∼13 years. 52 While acute conduit thrombosis is rare, nonocclusive thrombus may be present in up to 18% of patients within 10 years post-Fontan.53,54 Although larger conduits are generally beneficial, “oversized” conduits (≥30% larger than the inferior vena cava diameter) are associated with a higher incidence of pseudointimal hyperplasia and mural thrombus. 52
The geometric characteristics of cavopulmonary anastomoses determine the stability of transpulmonary flow and cardiac output. Angulation and very short distance between the superior anastomosis and conduit insertion, defined as the offset, may lead to non-laminar blood flow with increased energy loss, wall shear stress, and unfavorable hepatic flow distribution. 55 These factors were found to be contributors to decreased CO and thromboembolic events in computational fluid dynamics studies, which led to an advancement in surgical techniques beginning in the late 1980s. 10 To overcome this erroneous offset hemodynamic disturbance, the caval anastomoses were positioned separately to pulmonary artery branches. The blood from the inferior caval vein, which constitutes two-thirds of the venous return, being drained to the left branch through a conduit, and the minor one-third of the venous return from the superior caval vein directed to the right pulmonary branch. However, this kind of hemodynamic distribution was shown to be unfavorable in models, provided by Corno et al. 56 The authors offered the more physiological model of the Fontan circulation with the conduit draining to the right lung, which is larger. Generally, the revision of older modifications of Fontan circulation with conversion into physiological Fontan circulation is a potential surgical decision in case of circulatory failure with acceptable outcomes and mortality. 57
Pulmonary vasculature represents another critical component. Cavopulmonary anastomoses are prone to stenosis, and chronic nonpulsatile pulmonary blood flow may impair vascular development, leading to a decreased Nakata index (pulmonary artery branches diameter indexed to BSA) and worse functional status in adults. 58
The presence and size of a fenestration significantly impact hemodynamics. While a larger fenestration can decompress the venous system, it also causes systemic desaturation. A retrospective study by Miwa et al 59 suggests that a fenestration size indexed to BSA of ∼8 mm/m2 may be optimal for balancing these effects and preventing spontaneous closure.
Passive pulmonary blood flow is augmented by the respiratory and skeletal muscle pump, which generates negative intrathoracic pressure. 60 Supporting this, Perrone et al 61 demonstrated that a short-term aerobic training program improved exercise capacity, cardiorespiratory parameters, and reduced NT-proBNP levels in adult Fontan patients. Reduced exercise capacity stems not only from HF but also from endothelial dysfunction, decreased muscle mass, and impaired muscle function. Thus, developing the “muscle pump” is a key therapeutic target. An ongoing clinical trial is evaluating the impact of a supervised exercise program on morbidity and mortality in adult Fontan patients, 62 although the precise mechanisms of adaptation remain incompletely understood.
Based on invasive hemodynamic assessments, the concepts of “good,” “bad,” and “super-Fontan” circulations have emerged. In a study of 404 patients, Ohuchi et al 63 identified 77 “super-Fontan” patients with preserved multiorgan function and excellent prognosis, attributing this favorable state primarily to favorable pre-Fontan hemodynamics and daily physical activity in childhood.
Finally, the Fontan pathway is a complex structure with multiple potential points of failure that require thorough assessment during clinical deterioration. While ultrasound has limitations, contrast-enhanced CT serves as a first-line imaging modality for evaluating its major components.
Type III: Lymphatic Dysfunction
Chronic venous hypertension in adult Fontan patients predisposes them to specific end-organ damage, necessitating multidisciplinary management. As lymphatic function is critically dependent on CVP, this population is at particular risk for lymphatic complications, including protein-losing enteropathy (PLE), plastic bronchitis (PB), ascites, and chylous effusions. 64
Protein losing enteropathy, characterized by excessive enteric protein (primarily albumin) loss, occurs in 5% to 15% of Fontan patients. It leads to hypoalbuminemia, lymphopenia, hypogammaglobulinemia, and coagulopathy, resulting in edema, diarrhea, ascites, and hematologic abnormalities. 65 Diagnosis involves fecal alpha-1 antitrypsin analysis, with diagnostic thresholds of a spot level >54 mg/dL, or clearance >27 mL/24 h without diarrhea and >56 mL/24 h with diarrhea. Tc99m-labeled albumin scintigraphy can also demonstrate enteric protein loss. Given associated coagulopathies, anticoagulant therapy in these patients requires careful consideration. 66 Additionally, an acquired von Willebrand syndrome—common in Fontan patients—may be further exacerbated by concurrent cholestasis. 67
Plastic bronchitis is defined as a pulmonary lymphatic disorder involving leakage of proteinaceous material into the airways, leading to expectoration or bronchoscopic visualization of bronchial-shaped casts, which can cause respiratory distress or airway obstruction. 22 Clinical symptoms include chronic cough, wheezing, fever, and acute asphyxiation. Plastic bronchitis affects up to 4% of Fontan patients, typically within 2 to 3 years postoperatively. Key pathophysiological factors include increased lymphatic afterload and systemic venous congestion. Predictors of PB include a history of postsurgical chylothorax, postoperative ascites, prolonged chest tube drainage (>14 days) after cavopulmonary anastomosis or Fontan completion, and the presence of major aortopulmonary collaterals. 22
Chylous pleural and pericardial effusions are rarer lymphatic manifestations. 68 The development of any lymphatic complication should prompt evaluation for underlying Fontan pathway dysfunction (Type II) or ventricular dysfunction (Type I). 69
Imaging the lymphatic system presents unique challenges. Contrast-enhanced CT has limited utility, making dynamic contrast-enhanced magnetic resonance lymphangiography (via intrahepatic or intranodal injection) a first-line diagnostic modality. 70 Novel techniques are under investigation; for instance, contrast-enhanced 3D heavily T2-weighted MR imaging using gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) has recently been described. 71
Type IV: Extracardiac Dysfunction
Beyond lymphatic complications, long-standing elevation of CVP predisposes patients to other specific end-organ conditions, most notably Fontan-associated liver disease (FALD). Fontan-associated liver disease and progressive liver fibrosis in Fontan patients represent an area of growing concern, requiring further research to identify the primary predictors of disease progression. 72 A higher FALD score (≥2) is associated with increased post-heart transplant mortality. 73 However, available data suggest that following transplantation, patients do not experience progression of preexisting FALD or development of hepatocellular carcinoma. 74 While transient elastography has limited utility for clinical decision-making, acoustic radiation force impulse imaging appears more promising for identifying patients requiring intensified surveillance for hepatocellular carcinoma. 75
Renal dysfunction is also highly prevalent in adult Fontan patients. Contributing factors include hemodynamic alterations (venous congestion and reduced renal perfusion pressure), chronic hypoxia, and episodes of acute kidney injury related to surgical interventions, culminating in chronic kidney disease. The reported incidence of renal failure varies from 10% to 50%, with a median annual decline in glomerular filtration rate of ∼1.36 mL/min/1.73 m2 in the Fontan population. 76
Extracardiac vascular malformations constitute another significant source of morbidity. Patients with Fontan circulation commonly develop recanalized embryological structures, such as systemic-to-pulmonary venous collaterals and major aortopulmonary collateral arteries (MAPCAs). The former can lead to systemic desaturation and pulmonary thromboembolism, while the latter contribute to volume overload and elevated filling pressures in the FSV. 58
In addition to pulmonary vascular disease and plastic bronchitis (a lymphatic complication discussed previously), adult Fontan patients frequently exhibit restrictive lung disease, obstructive sleep apnea, and chronic cyanosis, often necessitating management by a pulmonologist or sleep specialist. 77
Fontan Failure Treatment: Targets for Therapy and Surgery
From a pathophysiological perspective, the gradual multiorgan deterioration in adult Fontan patients is driven by 3 principal factors: chronic elevation of CVP, nonpulsatile pulmonary blood flow, and the resultant low cardiac output state. In the absence of established HF treatment algorithms for this population, understanding these primary mechanisms of decompensation is crucial for tailoring individual management strategies. Therapeutic goals, encompassing both medical and surgical approaches, include preventing thrombotic complications within the circuit, supporting systolic and diastolic function of the systemic ventricle, and reducing pulmonary vascular resistance to maintain an adequate transpulmonary gradient. 78
Anticoagulation can be life-saving but requires careful consideration of the underlying hematologic abnormalities common in this cohort. For patients requiring long-term therapy, direct oral anticoagulants appear to be as effective as warfarin and represent a viable treatment option. 79
While systolic dysfunction of the FSV is the most common driver of HF progression, any clinical deterioration should prompt immediate evaluation for mechanical complications. Fontan pathway stenosis is a particularly serious concern in this context. In a study of 26 patients with Fontan obstruction, Agasthi et al 80 demonstrated that percutaneous stenting is a safe and effective treatment, with a low complication rate. Only 1 patient experienced acute kidney injury periprocedurally during follow-up 1 developed stent thrombosis and 2 required restenting.
Significant AV valve regurgitation leads to atrial enlargement and can impair ventricular diastolic function. Surgical correction is the recommended intervention for patients with failing Fontan circulation and significant regurgitation. 81 While open heart surgery is an option for selected patients, transcatheter edge-to-edge repair (eg, MitraClip) has recently been reported in adult Fontan patients. 82
Additional catheter-based or surgical interventions may be beneficial in specific scenarios. For patients with a patent conduit but progressive failure, creation or recreation of a fenestration can be considered. Conversely, fenestration closure may be necessary in cases of severe desaturation. Other potential procedures include pulmonary artery stenting, aortic arch repair, atrial septostomy, and epicardial pacemaker placement. 83
For patients with older Fontan modifications (eg, atriopulmonary connection and lateral tunnel), surgical conversion to an extracardiac conduit may be a valuable option to postpone the cardiac transplantation. 50 Figure 2 presents reconstructed CT images comparing an atriopulmonary connection with an extracardiac conduit.
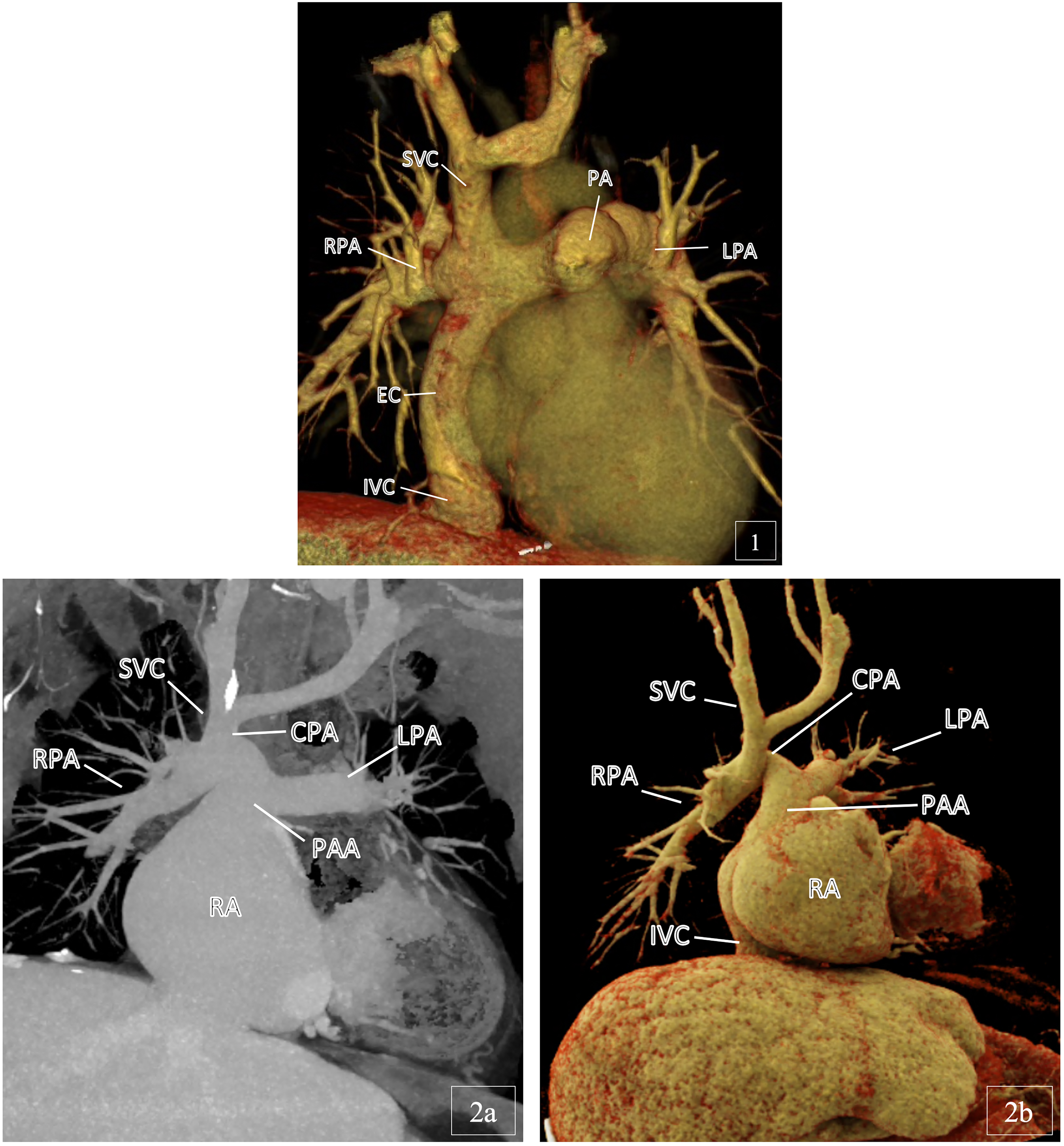
CT angiography of different Fontan circulation types.
A range of pharmacological and surgical strategies has been developed to manage lymphatic system complications in adult Fontan patients.
The treatment of PB is challenging and depends on disease severity. Options include inhalational therapies (mucolytics, corticosteroids, fibrinolytics, bronchodilators, and hypertonic saline), systemic corticosteroids, antibiotics, and anticoagulants. Bronchoscopic lavage is necessary in cases of airway obstruction by casts. 84
Conservative management of PLE involves supportive care with dietary modification, albumin and immunoglobulin infusions, diuretics, and anti-diarrheal agents like loperamide. For persistent cases, first-line therapy typically consists of angiotensin-converting enzyme inhibitors, budesonide, spironolactone, and low-molecular-weight heparin. Second-line agents include phosphodiesterase inhibitors, octreotide, and midodrine. 85
When medical therapy is ineffective, surgical lymphatic intervention may be warranted. Hraska et al
70
proposed a management algorithm for Fontan-associated lymphatic complications (PLE, PB, chylothorax, and ascites). Initial diagnosis should involve dynamic contrast-enhanced magnetic resonance lymphangiography (via intrahepatic or intranodal injection). Subsequent management depends on thoracic duct patency, with 2 main surgical approaches:
Lymphatic decompression: This can be achieved via lymphovenous anastomosis or innominate vein turn-down. The latter can be performed percutaneously or surgically using 2 techniques: direct suture of the innominate vein to the left atrial appendage, or drainage into the right atrium using an interposition graft. These procedures are conceptualized as a potential “third stage” of Fontan palliation, simultaneously decompressing the thoracic duct (by draining into a low-pressure atrial chamber) and partially reducing CVP. A potential drawback is systemic desaturation, which may necessitate partial banding of the jugular vein postoperatively.
70
Lymphatic embolization: Thoracic duct embolization or selective lymphatic embolization aims to redirect lymphatic flow away from pathological networks. Selective embolization is preferred and can be performed in select PB cases following detailed MR-lymphangiographic analysis.86,87
Resolving mechanical complications does not conclude therapy. Maintaining stable filling pressures remains a long-term goal to prevent Fontan failure and delay the need for reoperation or transplantation. 35
The timing of staged palliation is crucial. While early procedures aim to avoid prolonged hypoxemia and ventricular volume overload, some evidence suggests that performing the definitive Fontan procedure at an older age may delay the onset of complications like Fontan-associated liver disease and PLE. 36
After Fontan completion, management focuses on optimizing hemodynamics. Minimizing ventricular afterload is crucial, involving treatment of systemic arterial obstruction and the use of vasodilators for blood pressure control to prevent HF. 35 Preload can be optimized by reducing pulmonary vascular resistance pharmacologically and managing tachyarrhythmias that impair ventricular filling. Although dietary modifications and exercise may theoretically support ventricular filling, evidence for their efficacy in single ventricle patients remains limited. 14
Current treatment for HF with FSV systolic dysfunction lacks a robust evidence base. However, emerging research explores the potential utility of angiotensin receptor-neprilysin inhibitors, sodium-glucose co-transporter-2 inhibitors, and cardiac resynchronization therapy. 88 Managing diastolic dysfunction is particularly challenging. For symptomatic patients with severe diastolic dysfunction and restrictive physiology, diuretics remain the primary option for lowering filling pressures and providing relief. 14
Pulmonary vasodilators have garnered significant interest in Fontan management. This drug class includes phosphodiesterase-5 inhibitors (sildenafil and tadalafil), endothelin receptor antagonists (bosentan and ambrisentan), and prostacyclin analogs (iloprost). A systematic review of pharmacological therapy in Fontan patients, which analyzed 9 studies, found that 8 focused on pulmonary vasodilators: 4 on sildenafil, 3 on bosentan, and 1 on iloprost. 89 Although most studies were small and short-term, they generally reported positive trends in exercise tolerance and hemodynamics. A larger randomized placebo-controlled trial by Hebert et al 90 demonstrated that bosentan treatment for 14 weeks improved peak oxygen consumption, exercise duration, and functional capacity without significant adverse effects. Despite these promising results, further research is needed to establish the long-term efficacy and safety of these agents. Notably, inhaled nitric oxide has been shown to improve hemodynamics during catheterization in adult Fontan patients and may help identify responders to chronic vasodilator therapy. 91
Heart transplantation remains the definitive therapy for end-stage Fontan failure, although preexisting end-organ damage can complicate eligibility. Retrospective data from 63 adult Fontan patients at the Mayo Clinic suggest that earlier referral to a transplant center is associated with better outcomes and a higher likelihood of waitlist acceptance. 92 Another study by Chowdhury et al 93 emphasizes that successful prevention of end-organ damage hinges on individualized management tailored to the patient's clinical phenotype.
Patients with Fontan circulation and terminal HF should be assessed as candidates for mechanical assist devices, which is a bridge to cardiac transplant. While ventricular assist device implantation carries up to a 75% rate of various complications, the mortality was 18% within 1 year in the ACTION registry, which is an acceptable result compared with the extremely high mortality without intervention. 94
Heart transplantation in the Fontan circulation is technically challenging and the rates of survival within 1 and 5 years after the procedure are lower (77% and 70%) than those in non-Fontan patients (88% and 81%). 95 However, among patients with Fontan circulation who underwent cardiac transplant the overall 1-year survival reaches 90% and 5-year survival ranges between 70% and 80% in recent trials and meta-analysis. 96 Patients with advanced FALD may require a combined heart and liver transplant. According to Vizentin et al, 97 a meta-analysis of 4 studies with 67 Fontan circulation patients, the 1-year survival rate after the combined transplantation was 88% with a high rate of renal complications and 4% rate of liver graft rejection. However, all studies were carried out in the United States, while generally the experience of this procedure is very limited even in expert centers.
Therefore, the growing adult Fontan population necessitates the development of specialized, multidisciplinary care programs. A standardized transition from pediatric to adult care, including a comprehensive assessment of end-organ function, is essential. Clinical decision-making during periods of decompensation is complex, requiring synthesis of multiple anatomical, pathophysiological, and clinical factors. Scoring systems, such as the Fontan Failure score proposed by Kramer et al, may aid in prognosis and risk stratification but require further validation. 98 Figure 3 provides a schematic overview of the primary vulnerabilities in the Fontan circulation and the corresponding targets for surgical and medical intervention.
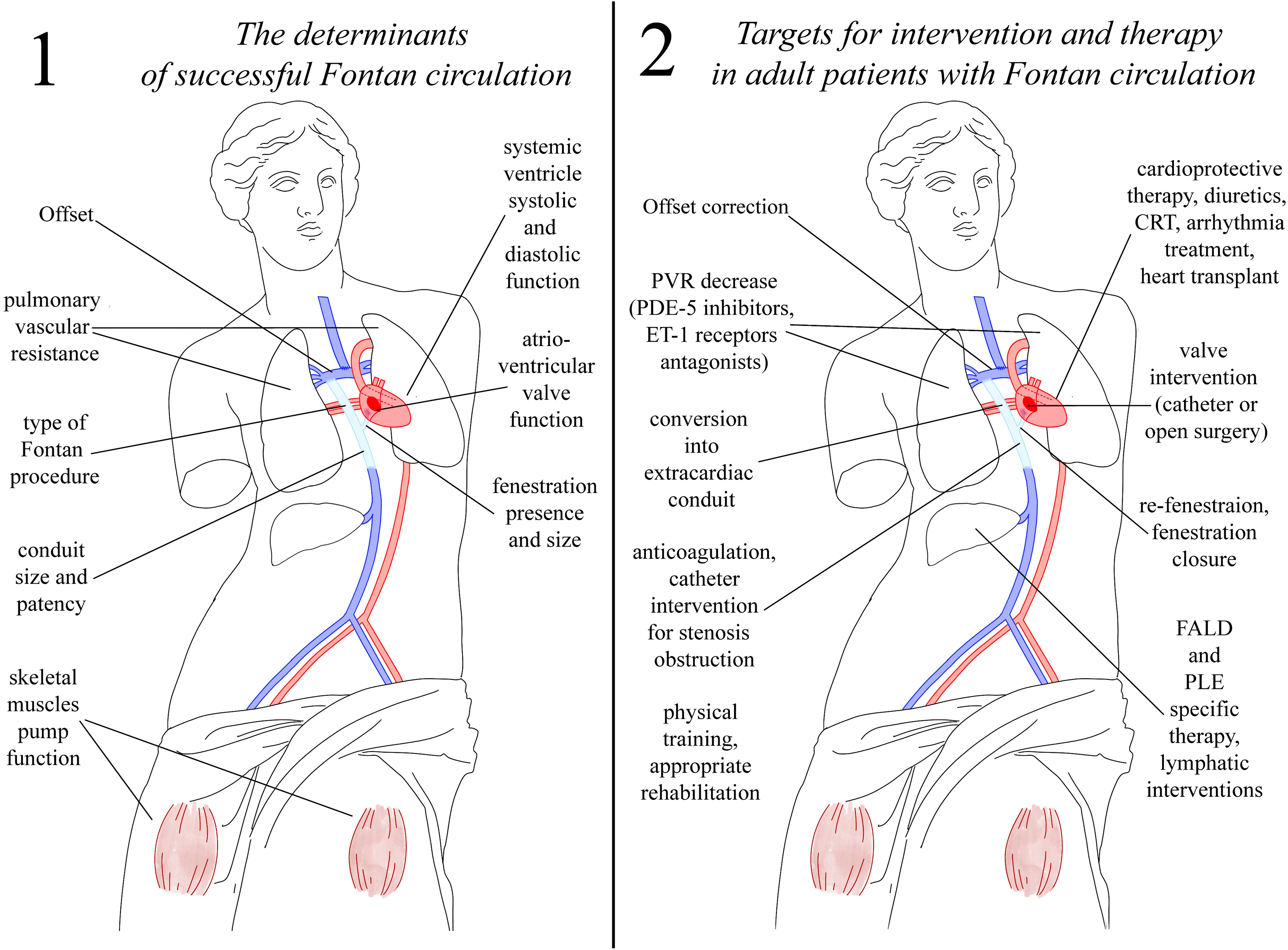
Determinants of a stable Fontan circulation and corresponding therapeutic targets.
In summary, the Fontan circulation has evolved over more than 50 years from isolated case reports to a mainstream palliative strategy sustaining over 70,000 patients worldwide—a population projected to double in the next 2 decades. 14 Despite surgical success, the substantial burden of cardiac and extracardiac complications, particularly in older patients, remains a major challenge. 99 Although specialized centers have been established in developed countries, clinical management often lacks standardized protocols and consistent interdisciplinary coordination. Critically, strategies to enhance the long-term durability of the Fontan state and delay the need for transplantation remain elusive. While accepted algorithms exist for managing common complications, the evidence base is often limited, underscoring the urgent need for further research to optimize outcomes for this growing population.
Footnotes
Abbreviations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.