
Abstract
Left ventricular (LV) fibromas in children can pose major surgical challenges when epicardial coronary arteries are involved. We report the case of a 3-month-old female diagnosed with a large intramyocardial LV fibroma causing mitral valve compression and traversed by the left circumflex coronary artery. Multimodality imaging, including cardiac magnetic resonance imaging and coronary angiography, was essential for surgical planning. Progressive tumor growth, causing compression of the left lung and worsening mitral regurgitation, prompted partial tumor resection with mitral valvuloplasty at 23 months of age at Boston Children's Hospital, preserving the intratumoral left circumflex artery. Six years later, the patient remains asymptomatic, with stable residual tumor size, preserved LV function, and no clinically significant arrhythmias. This case illustrates the durability and safety of a conservative, coronary-sparing surgical strategy in selected pediatric patients with ventricular fibromas involving major coronary arteries.
Keywords
Introduction
Cardiac fibromas are the second most common primary cardiac tumors in children, typically arising within the ventricular myocardium, most frequently on the left ventricle (LV) free wall or interventricular septum. These tumors lack a capsule and may infiltrate the surrounding myocardium. 1 Cardiac magnetic resonance imaging (MRI) enables an accurate diagnosis in most cases. 2 While early surgical resection is generally recommended for tumors causing arrhythmias or hemodynamic compromise, involvement of epicardial coronaries may pose significant technical challenges. We present a case of a large LV fibroma traversed by the left circumflex artery (LCx), managed with a coronary-sparing surgical approach.
Clinical Summary
A 3-month-old female was referred for evaluation of a grade II/VI systolic murmur, best heard at the left sternal border. She was asymptomatic, with appropriate weight gain and, besides the murmur, had a normal cardiovascular examination. Amniocentesis, performed following an elevated first-trimester screening risk (1:136), indicated a higher likelihood of chromosomal abnormalities. The cytogenetic analysis was normal.
Electrocardiogram demonstrated ST-T segment changes, including negative T waves in lead I, V5, and V6. Transthoracic echocardiogram revealed a large, heterogeneous, oval-shaped intramyocardial mass located in the free wall of the LV, measuring 40 × 24 mm in its longest axis. The mass protruded into the LV cavity, significantly reducing its volume and exerting moderate compression on the posterior leaflet of the mitral valve, resulting in mild regurgitation. Standard LV linear measurements could not be reliably obtained because the distortion of LV geometry by the tumor limited the reproducibility of end-diastolic and end-systolic diameter measurements. There was no evidence of LV outflow tract obstruction, and LV ejection fraction (LVEF) was preserved. Cardiac MRI performed at the age of 4 months revealed a well-circumscribed mass, extending from the mitral annulus to the apex of the LV, isointense on both T1 and T2-weighted sequences, with mild central heterogeneity and discrete late gadolinium enhancement (LGE); however, suboptimal inversion time selection was suspected (Figure 1). The lesion showed no signs of fat suppression, and first-pass perfusion imaging revealed hypoperfusion. Based on these features, the findings were consistent with a diagnosis of cardiac fibroma.
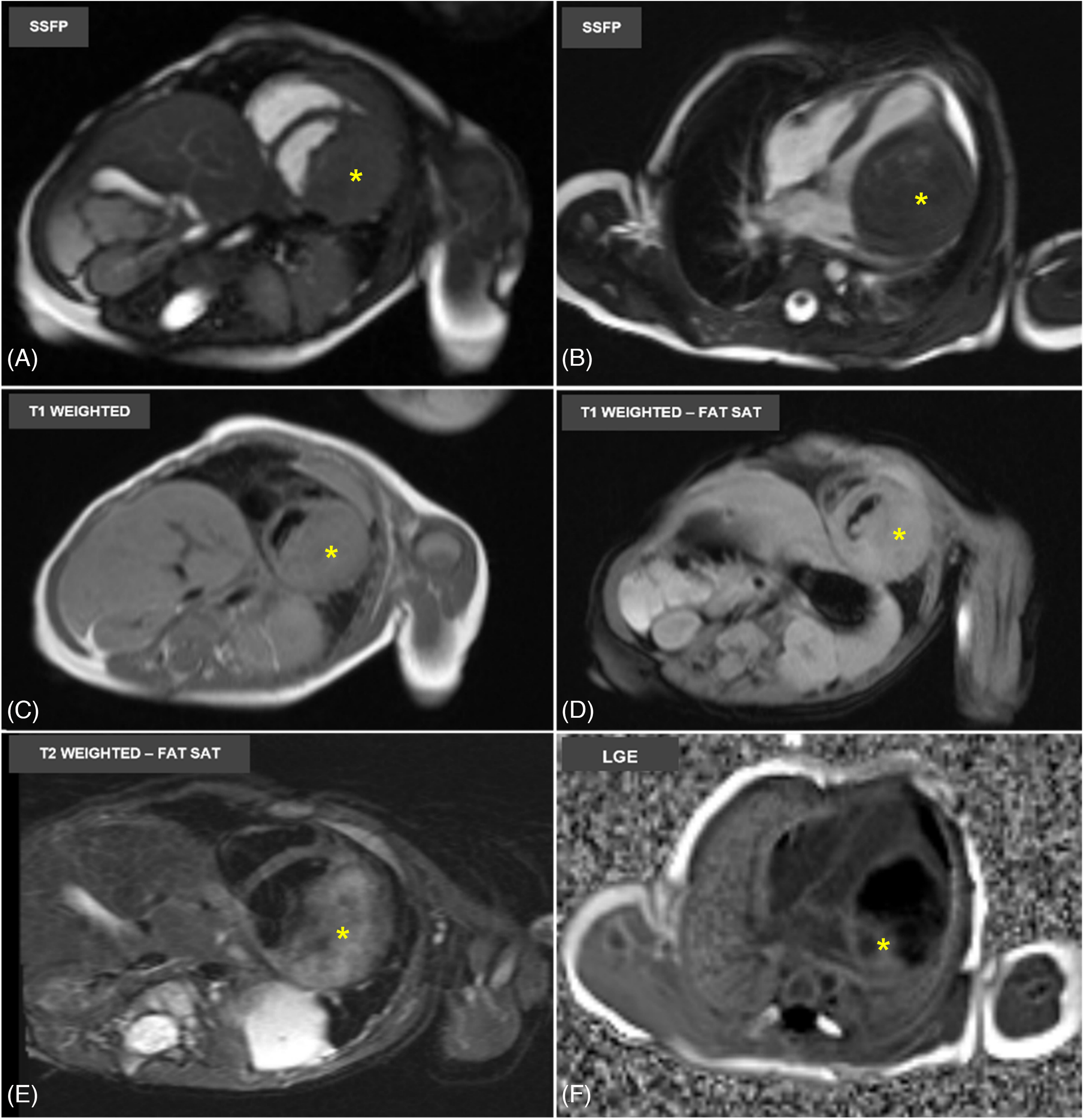
Cardiac Magnetic Resonance Imaging of a Large Left Ventricular Fibroma in a 4-Month-Old Infant. The Cine Steady-State Free Precession Images in Short Axis (A) and 4-Chamber (B) Views demonstrate a Large, Well-Defined Intramyocardial Mass (Identified by a Yellow Asterisk) located along the Lateral Wall of the Left Ventricle, Displacing the Posterior Mitral Valve Leaflet. On T1-Weighted Imaging (C), the Lesion appears Isointense to the surrounding Myocardium. Fat Saturation Sequences on T1 show no fat suppression within the Mass (D). T2-Weighted Fat-Saturated Images (E) reveal a Mild Heterogeneous Signal. Late Gadolinium Enhancement Images (F) demonstrate Mild Rim Enhancement of the Mass.
A 24-hour Holter monitoring was also performed at 4 months, which showed 8 short periods of idioventricular rhythm, mostly during the night, along with rare ventricular and supraventricular premature contractions. ST-segment depression (maximum −3 mV) with negative T waves was observed in V5.
Genetic testing identified a variant of uncertain significance in the TSC1/TSC2 genes, classified as probably benign. Serial imaging up to 17 months of age demonstrated a progressive increase in tumor size, reaching 53 × 38 mm, without evidence of LV outflow obstruction or deterioration of systolic function. Mitral insufficiency progressed to moderate severity. Additionally, imaging revealed persistent atelectasis, suggesting compression of the left lung by the tumor. Formal pulmonary function testing was not performed preoperatively, given the patient's age. Subsequent Holter evaluations at 6 and 17 months demonstrated isolated unifocal premature ventricular contractions and continued ST-segment depression (maximum −3.5 mm) in V5. Given the tumor growth, along with worsening mitral regurgitation, persistent repolarization abnormalities suggestive of myocardial ischemia, and extracardiac pulmonary compression, a multidisciplinary discussion concluded that surgery was indicated.
Cardiac catheterization at 22 months revealed that the LCx traversed the tumor, where it demonstrated systolic compression without fixed luminal obstruction (Figure 2).
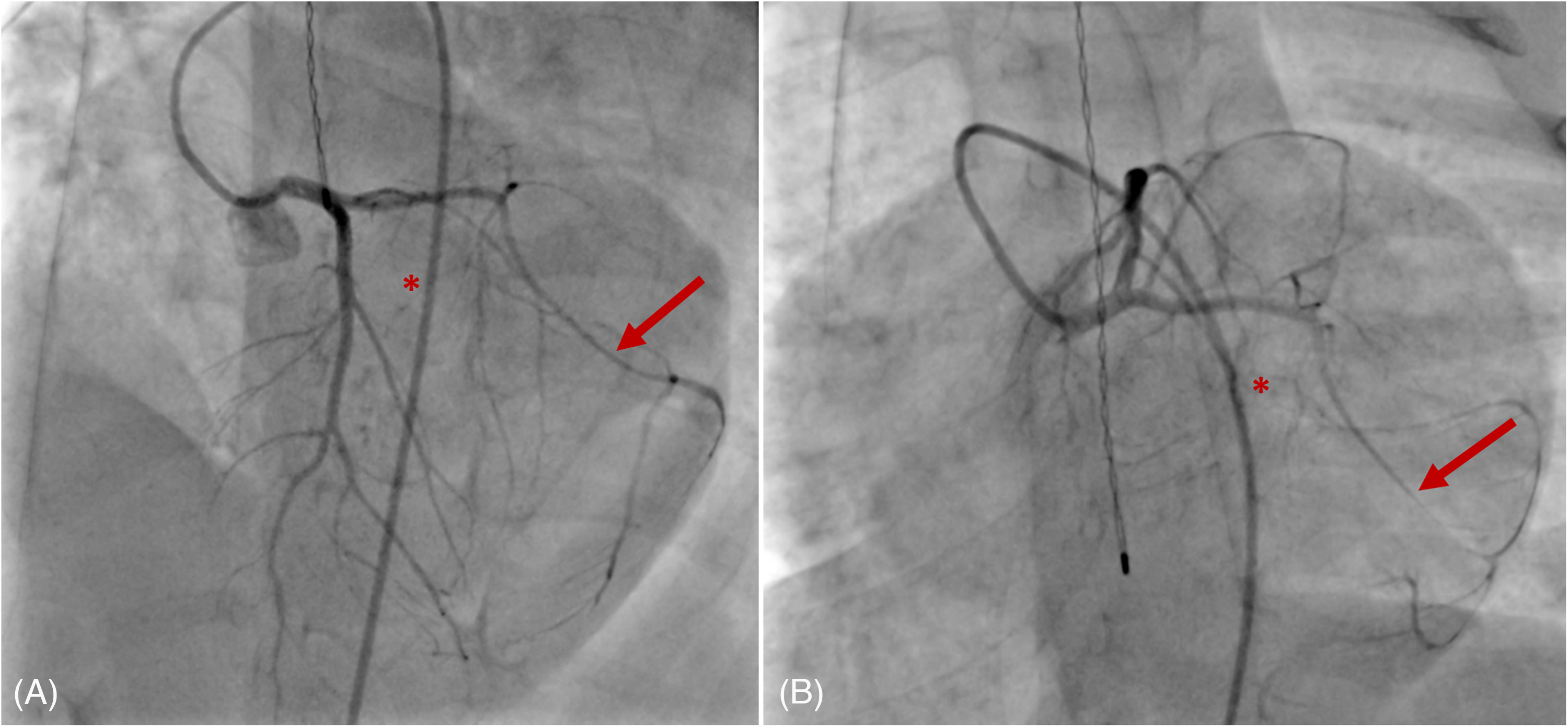
Preoperative coronary angiography demonstrating the Intratumoral course of the Left Circumflex Artery. (A) Left Anterior Oblique (LAO) Projection with cranial angulation showing a patent Left Circumflex Artery (Red Arrow) as it courses along the Lateral Left Ventricular Wall. (B) LAO Projection with caudal angulation demonstrating the Intramyocardial trajectory of the Left Circumflex Coronary Artery (Red Arrow) through the region corresponding to the Fibroma (Red Asterisk), where it exhibits diffuse Systolic Compression.
Given the intratumoral course of the artery and the absence of a safe surgical plane, complete excision was deemed to carry an unacceptably high risk of coronary injury and postoperative ventricular dysfunction. Accordingly, at 23 months of age, the patient underwent coronary-sparing partial tumor resection with concomitant mitral valvuloplasty at Boston Children's Hospital. Following median sternotomy and initiation of cardiopulmonary bypass, a large, multilobulated cardiac tumor was encountered, originating from the posterobasal LV free wall. Critical to the resection was the identification of a single feeding coronary vessel, consistent with a branch of the LCx, with 2 distal branches coursing along the posterior margin. To preserve this vasculature, a plane was developed using sharp dissection from the apical toward the basal tumor. Upon reaching the coronary territory, a deliberate subtotal resection strategy was employed. The main tumor mass was circumferentially excised, while a protective cuff of tumor tissue encapsulating the LCx and its branches was left to avoid vascular injury. This resulted in a residual tumor island at the base. The resulting LV defect was reconstructed in multiple layers with interrupted 4-0 Prolene suture, and tension was relieved by scoring the epicardium over the retained basal nodule. Subsequent mitral valve analysis revealed a tethered and immobile posterior leaflet due to short, dense chords inserting into a rudimentary anterior papillary muscle, coupled with anterior leaflet prolapse. The repair was accomplished in a 2-stage maneuver after initial commissural closure proved insufficient. Upon rearrest, the posterior leaflet was first mobilized by sharp dissection and delamination of the papillary muscle head, which improved chordal mobility. The anterior commissure was then closed more centrally toward the valve orifice using interrupted 6-0 Prolene sutures. This restored valvular competence with only mild residual central regurgitation on postrepair transesophageal echocardiography. Histopathological examination confirmed a fibroma with focal calcifications. She was discharged on day 6, at which time echocardiography demonstrated mild mitral regurgitation and mild global left ventricular systolic dysfunction. The patient was prescribed aspirin for 3 months and enalapril for 6 months.
Postoperative chest imaging demonstrated resolution of the previously noted left lung atelectasis, and the patient had no respiratory symptoms or recurrent pulmonary infections during follow-up. Over a 6-year follow-up, the patient has remained asymptomatic, including during age-appropriate exercise and stress testing. Exercise stress tests performed at 5 and 7 years of age demonstrated normal exercise capacity for age, no ischemic ST-segment changes, and no exercise-induced arrhythmias. Echocardiogram maintained mild mitral valve regurgitation, a residual tumor with unchanged dimensions, and stable global and regional LV function. Annual Holter monitoring revealed persistent but improved repolarization changes and has not demonstrated recurrence of idioventricular rhythm or clinically significant ventricular arrhythmias. Follow-up cardiac MRI at the age of 6 (Figure 3) demonstrated a residual intramyocardial mass with extensive late gadolinium enhancement (LGE) consistent with the collagen-rich composition of fibroma, revealed after optimized acquisition parameters, without interval growth or perfusion defects. Left ventricular ejection fraction was mildly reduced at 54%. Considering the patient's asymptomatic status and absence of ischemic features, dedicated coronary computed tomography angiography for long-term surveillance has been deferred but is planned as part of ongoing surveillance.
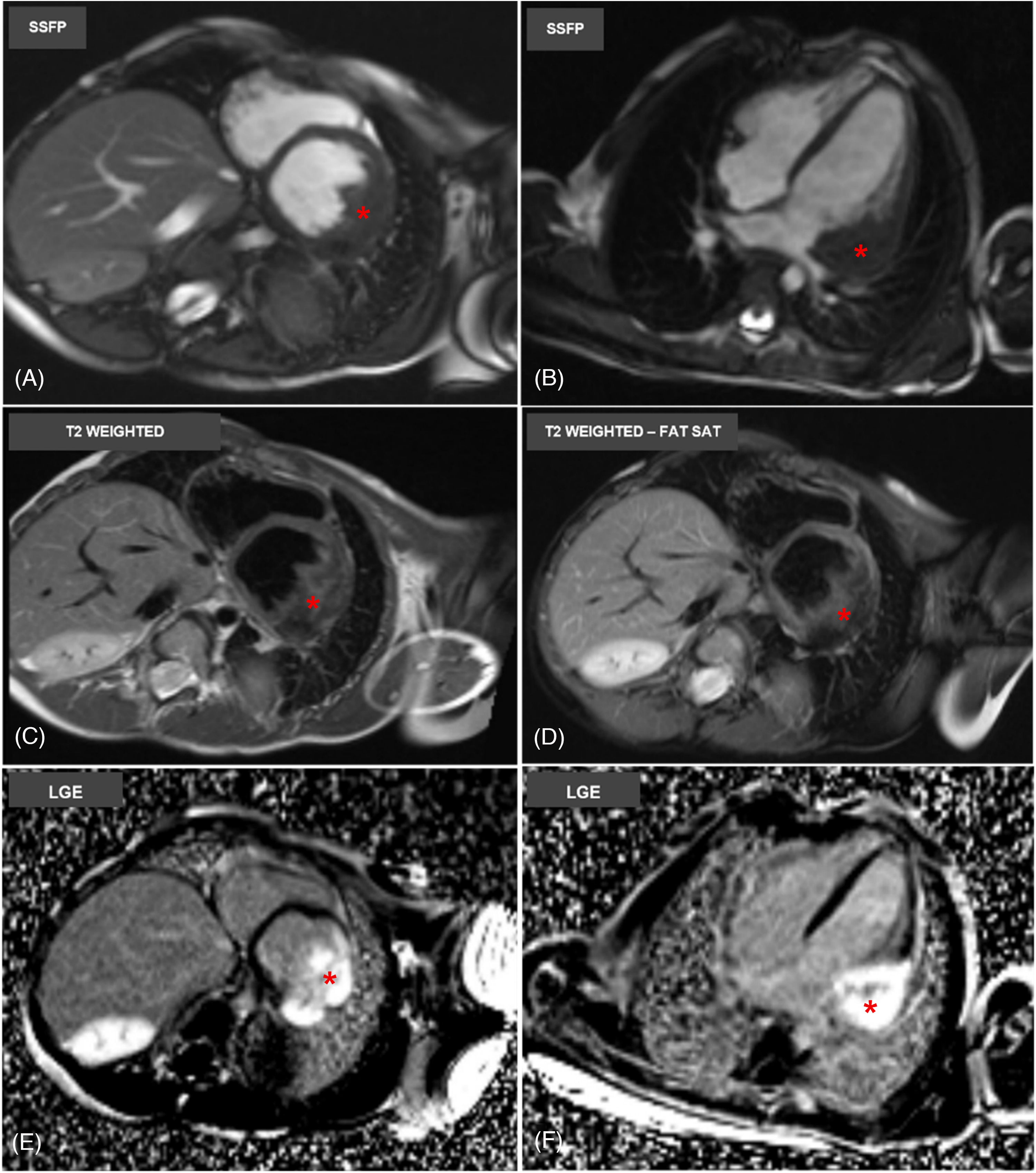
Follow-up cardiac magnetic resonance imaging at 6 years of age. Cine steady-state free precession images in short axis (a) and 4-chamber (b) views show a stable residual intramyocardial mass (identified by red asterisk) located in the basal to mid-lateral left ventricular wall. On T2-weighted imaging (c), the lesion maintains heterogeneous signal intensity. Fat-saturated T2 images show no evidence of fat within the mass (d). Late gadolinium enhancement images (e and f) in both short-axis and 4-chamber views reveal persistent intense enhancement with a central hypointense core.
Discussion
Cardiac fibromas, while histologically benign, present significant management challenges when they involve critical structures. Their size and location can result in life-threatening complications such as ventricular outflow obstruction, arrhythmias, and sudden cardiac death. 3 Coronary artery compression from fibromas has been well-documented and is hypothesized to be a mechanism for LV dysfunction following fibroma resection. 4 As spontaneous regression is rare, surgical resection is generally recommended at the time of diagnosis, particularly in the presence of hemodynamic compromise.
A thorough multimodal evaluation is critical for both diagnosis and surgical planning. Transthoracic echocardiogram provides an initial assessment of tumor size, location, and its impact on ventricular function or flow dynamics. Cardiac computed tomography may identify characteristic central calcification, which reflects poor blood supply, and help evaluate coronary artery proximity. Evidence has shown that cardiac MRI with LGE provides superior tissue characterization and high diagnostic accuracy, often eliminating the need for biopsy.2,5 Coronary angiography remains the definitive tool for defining tumor-vessel relationships when epicardial coronaries are involved, as demonstrated in our case. For long-term surveillance, CCTA serves as an excellent noninvasive alternative to assess vessel patency.
The timing of surgical intervention in asymptomatic or minimally symptomatic patients requires careful consideration. Current algorithms recommend surgery for tumors demonstrating progressive growth, hemodynamic compromise, significant valvular distortion, or malignant arrhythmic potential.6,7 In this case, the decision to proceed with surgery at 23 months was driven by multiple factors meeting these criteria, warranting intervention despite preserved systolic function. Pulmonary compression with persistent atelectasis represented an additional extracardiac indication for tumor debulking, which was expected to improve following relief of mass effect.
While complete resection is preferred, it is not always feasible when the tumor involves or encases the coronary arteries. Although prevalence data are limited, case series suggest that a minority of fibromas, particularly those near the anterior wall or septum, may encase or displace coronary arteries, 8 most commonly the left anterior descending artery due to its proximity.
Our case highlights the successful application of a conservative, coronary-sparing strategy in a pediatric patient with an LCx-involved fibroma. This approach reflects the favorable outcomes reported in the literature for subtotal resections.6,8 In a cohort of 52 patients reported by Gikandi et al, 7 major epicardial coronary arteries were abutted in 41 cases, and tumor debulking was performed in 34. Over a median follow-up of 2.4 years, there were no instances of mortality, cardiac arrest, or heart transplantation. The 15-year risks of reoperation and clinical ventricular tachycardia/fibrillation were 6.7% and 2.4%, respectively, with no significant differences in LVEF. Notably, worse prognoses have been associated with transmural resections, which are linked to postoperative left ventricular dysfunction due to compromised endocardial blood supply.
Additionally, in this case, the preoperative finding of systolic LCx compression resolved after debulking, even though the artery remained encapsulated within the residual tumor. This observation is consistent with the proposed mechanism that coronary compression in ventricular fibromas results from increased intramural pressure generated by the tumor's bulk during systole. 4 By reducing tumor volume, debulking relieves this compressive force and restores normal phasic flow.
Arrhythmia management in patients with cardiac fibromas requires individualized risk stratification. 3 While residual tumors can be arrhythmogenic, the absence of malignant arrhythmias postoperatively, along with preserved ventricular function and a stable clinical status, did not support additional interventions such as primary prevention implantable cardioverter device implantation in this patient. The incorporation of serial exercise stress testing into routine follow-up provided further reassurance regarding the absence of exercise-induced myocardial ischemia or malignant arrhythmias. Importantly, postdebulking Holter monitoring showed no significant ventricular arrhythmias, underscoring the potential anti-arrhythmic benefit of mass reduction even without complete excision.
This case underscores the importance of integrating advanced imaging with operative judgment to balance effective tumor debulking against preservation of myocardial integrity and coronary perfusion, an essential principle in contemporary pediatric cardiac surgery.
Footnotes
Informed Consent Was Obtained From the Patient's Legal Guardian
The data supporting the findings of this study are contained within the article. Additional clinical data are not publicly available due to patient privacy considerations but may be made available from the corresponding author upon reasonable request and with appropriate ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.