
Abstract
Background
We sought to characterize the epidemiology, treatment patterns, and outcomes of neonatal Ebstein anomaly using a national database.
Methods
In this descriptive analysis, the pediatric health information system (PHIS) database was queried for the demographics, treatment, and outcomes of neonates with Ebstein anomaly using International Classification of Disease codes between 2004 and 2024. The surgical and nonoperative cohorts were each divided into two eras: era 1 = 2004-2014, era 2 = 2015-2024.
Results
Among 1323 neonates identified, 173 (13%) underwent surgical repair and 1150 (87%) received nonoperative management. Overall hospital mortality was 26.6% (46/173) (operative) and 12.8% (147/1150) (nonoperative). Nonoperative mortality significantly decreased over time (18.4% [34/185] vs 11.7% [113/965], p = .01), while operative mortality did not improve (20.5% [9/44] vs 28.7% [37/129], p = .38).
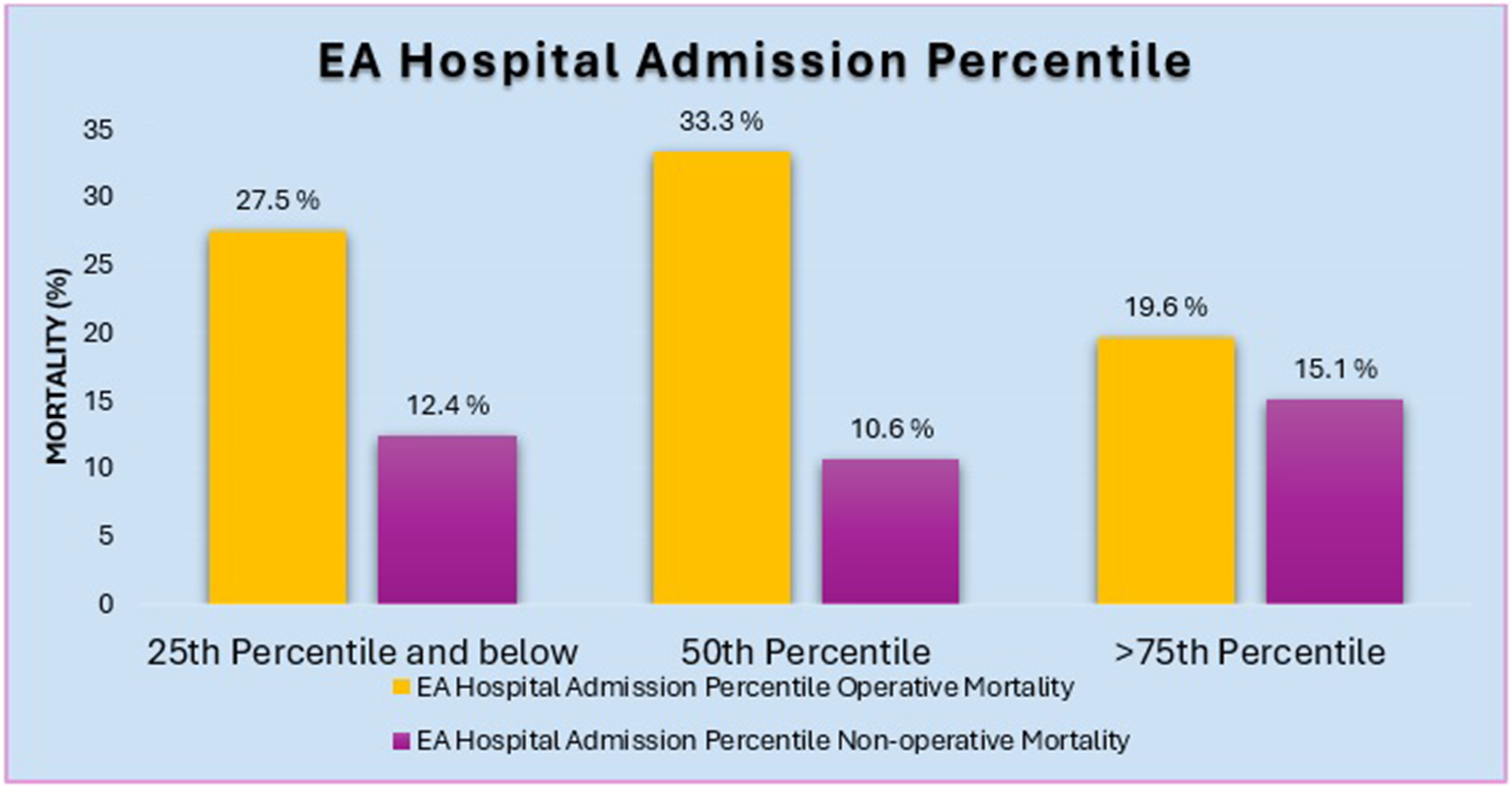
In the operative cohort, 73% (126/173) required mechanical ventilation (MV) < 14 days and 27% (47/173) required MV ≥14 days, with no mortality difference. In the nonoperative cohort, 60% (690/1150) avoided intubation. In the nonoperative cohort, compared with nonintubated patients (mortality:8.4%), mortality odds increased significantly with MV for 7 to 13 days (21%; OR 8.5, p < .01) and ≥14 days (26%; OR 7.8, p < .01). High-volume centers (≥75th percentile for Ebstein admissions) had significantly lower operative mortality compared with low-volume centers (19.6% vs 27.5%, OR 0.39, p = .04) but equivalent nonoperative mortality. Only 26.6% (46/173) of surgical patients were treated at high-volume centers.
Conclusions
Significant mortality persists in neonatal Ebstein anomaly (27% [46/173] surgical, 13% [147/1150] nonsurgical), with improvement over time only in nonsurgical patients. Nonsurgical patients requiring intubation >7 days have >20% mortality, warranting strategy reconsideration. Higher-volume centers appear to demonstrate superior operative survival, perhaps supporting patient transfer for surgical management.
Introduction
Ebstein anomaly (EA) represents less than 1% of all congenital heart diseases and poses a unique challenge for congenital heart centers due to the infrequency of and significant variation in presentation. The anatomic heterogeneity ranges from isolated tricuspid valve abnormalities to complex cases with associated lesions such as aortic atresia and double discordance, which substantially impact management and outcomes. 1 Many advances have been made in the early detection and prognostication of EA during the fetal period, including the identification of risk factors for postnatal mortality. Circular shunts have been recognized as a poor prognostic, but actionable phenomenon, as well as functional pulmonary atresia.2–5 Moreover, much experience has been gained and innovations in surgical techniques, including tricuspid valve repair, specialized biventricular repairs, and single ventricular palliation may prove to be useful in this patient population.6–9
Nevertheless, given the disease’s rarity, studies are often limited to single-center experiences and offer limited generalizability due to cohort sizes and institutional variations in practice and experience. In light of the considerable mortality and morbidity burden associated with EA, this study was designed to evaluate current practices and clinical outcomes in real-word settings.
Methods
The Institutional Review Board (IRB) of Cincinnati Children's Hospital Medical Center approved this study (IRB# 2018-6837) and the requirement for individual patient consent was waived as this was the analysis of deidentified data. The pediatric health information system (PHIS) database was queried for neonates with a diagnosis of EA using International Classification of Disease (ICD) codes between 2004 and 2024. Ebstein patients with other congenital heart diseases, such as pulmonary atresia were excluded. Other excluded diagnoses include hypoplastic left heart syndrome, double outlet right ventricle, transposition of the great arteries, and double inlet left ventricle. The operative cohort contained only those who underwent cardiopulmonary bypass during that hospital stay. Those who underwent shunt placement without bypass or patent ductus arteriosus stent placement were excluded from the study. The operative and nonoperative cohorts were divided into two eras for characterization, where era 1 is defined as 2004 to 2014 and era 2 as 2015 to 2024. In the nonoperative cohort, PHIS CTC codes were used to determine the length of mechanical ventilation (MV). Finally, Ebstein anomaly admission percentiles were calculated by dividing the total number of EA patient admissions at each institution by the number of years that institution participated in the PHIS database (Figure 1).
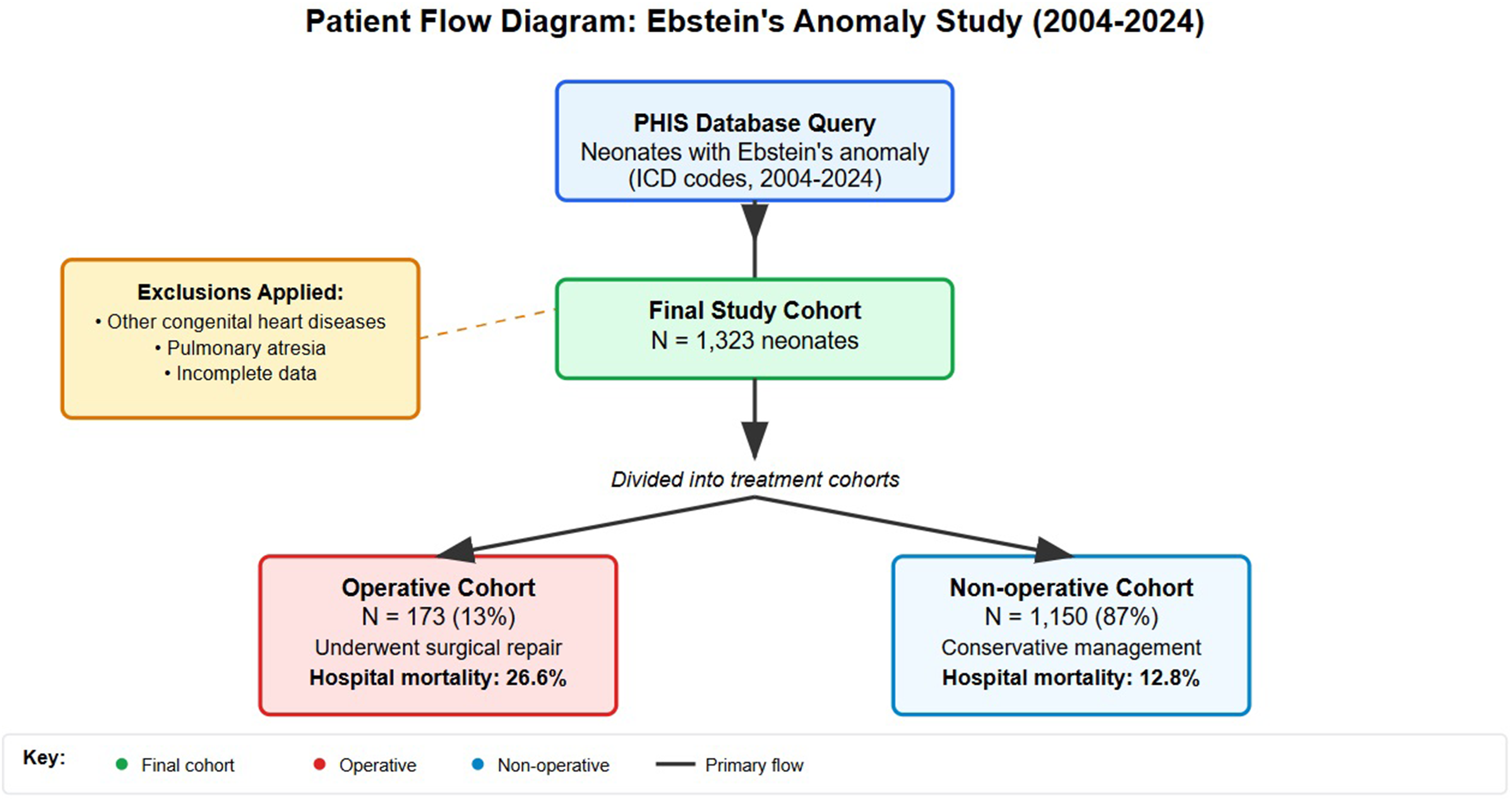
Cohort generation methodology. Excluded congenital heart diseases include HLHS, DORV, TGA, and DILV. Abbreviations: DILV, double inlet left ventricle; DORV, double outlet right ventricle; HLHS, hypoplastic left heart syndrome; PHIS, pediatric health information system; TGA, tetralogy of Fallot.
Descriptive statistics were used to report patient characteristics and outcomes, including count, median, and range. Categorical variables were compared using Fisher's exact or chi-square testing as appropriate. Continuous variables were compared with t-test, analysis of variance, or Wilcoxon Rank Sum testing as appropriate. In-hospital survival differences among the groups were compared. A p-value of less than .05 was considered statistically significant. Analyses were conducted using R (R version 4.2, http://www.r-project.org).
Results
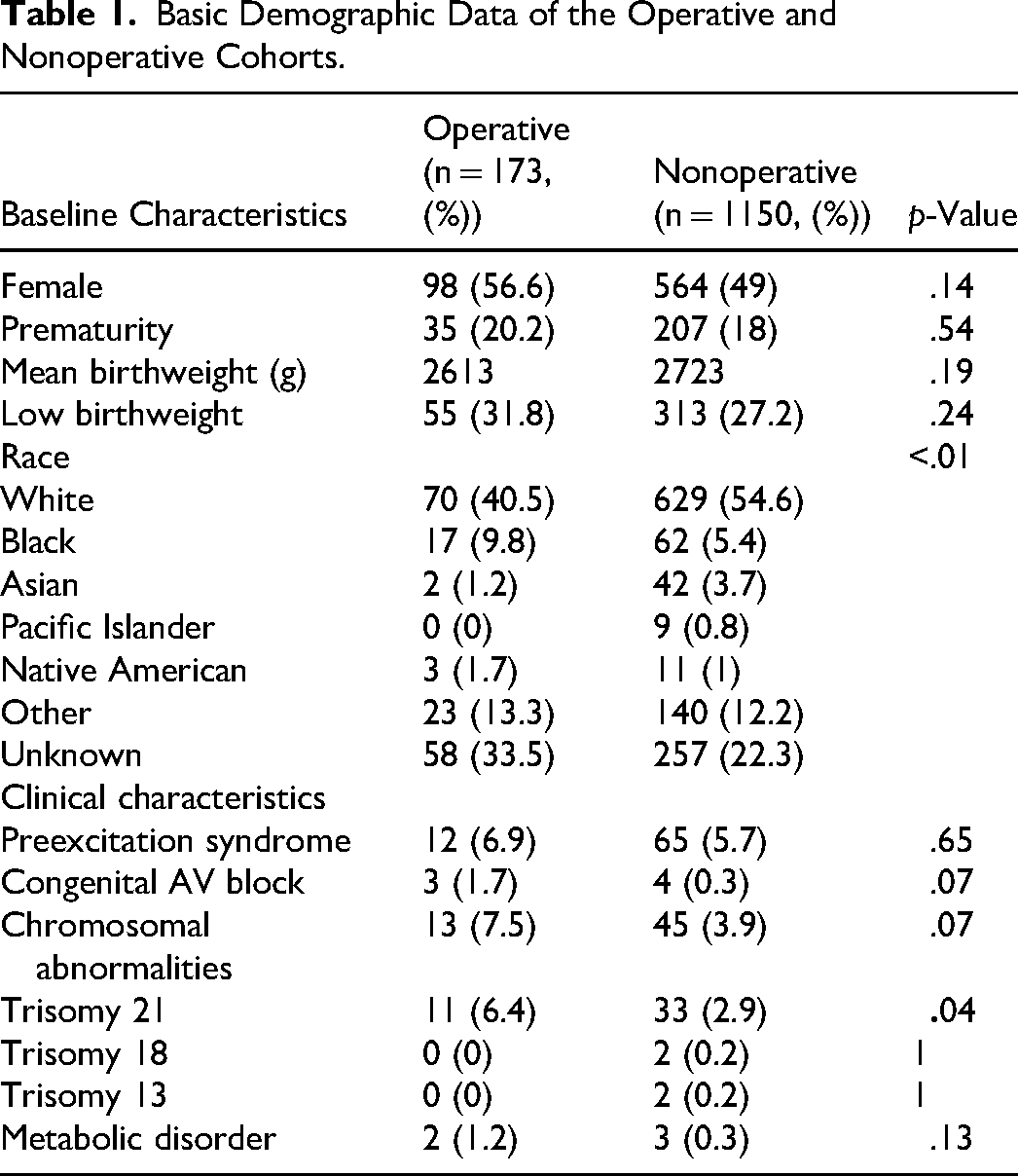
A total of 1323 neonates were identified, of which 173 (13%) underwent surgical repair with cardiopulmonary bypass and 1150 (87%) a nonoperative pathway (Table 1). For the operative cohort, we are unable to differentiate specific surgical procedures such as Starnes palliation, Knott-Craig or Cone repair, and were limited to those who required cardiopulmonary bypass. In the operative cohort, the majority were female (56.6%, 98/173), 20.2% (n = 35/173) were premature, with a mean birthweight of 2.6 kg, and 31.8% (n = 55/173) were low birthweight (< 2.5 kg). The nonoperative cohort had similar demographics: 49% (564/1150) female (p = .14), 18% (n = 207/1150; p = .54) were premature, a median birthweight of 2.7 kg (p = .19), and 27.2% (n = 313/1150; p = .24) were low birthweight. There was a higher incidence of trisomy 21 in the operative cohort, but other associated clinical diagnoses, such as preexcitation syndrome, congenital atrioventricular (AV) block, and other chromosomal abnormalities were not significantly different.
Basic Demographic Data of the Operative and Nonoperative Cohorts.
When these cohorts were separated into eras, their basic demographic data across time has remained relatively consistent. In the operative cohort, there were no significant differences between sex, prevalence of prematurity, birthweight, preexcitation syndrome, congenital AV block, inotrope usage, or chromosomal abnormalities, but there were significantly more preoperative intubated patients in Era 2 (11.4% [5/44] vs 67.4% [87/129], p < .01). The nonoperative cohort also did not have any significant differences between sex, prevalence of prematurity, birthweight, preexcitation syndrome, but there was a higher prevalence of congenital AV block in era 1 as compared with era 2 (1.6% [3/185] vs 0.1% [1/965], p = .01) (Table 2).
Basic Demographic Data by era of Operative and Nonoperative Cohorts.
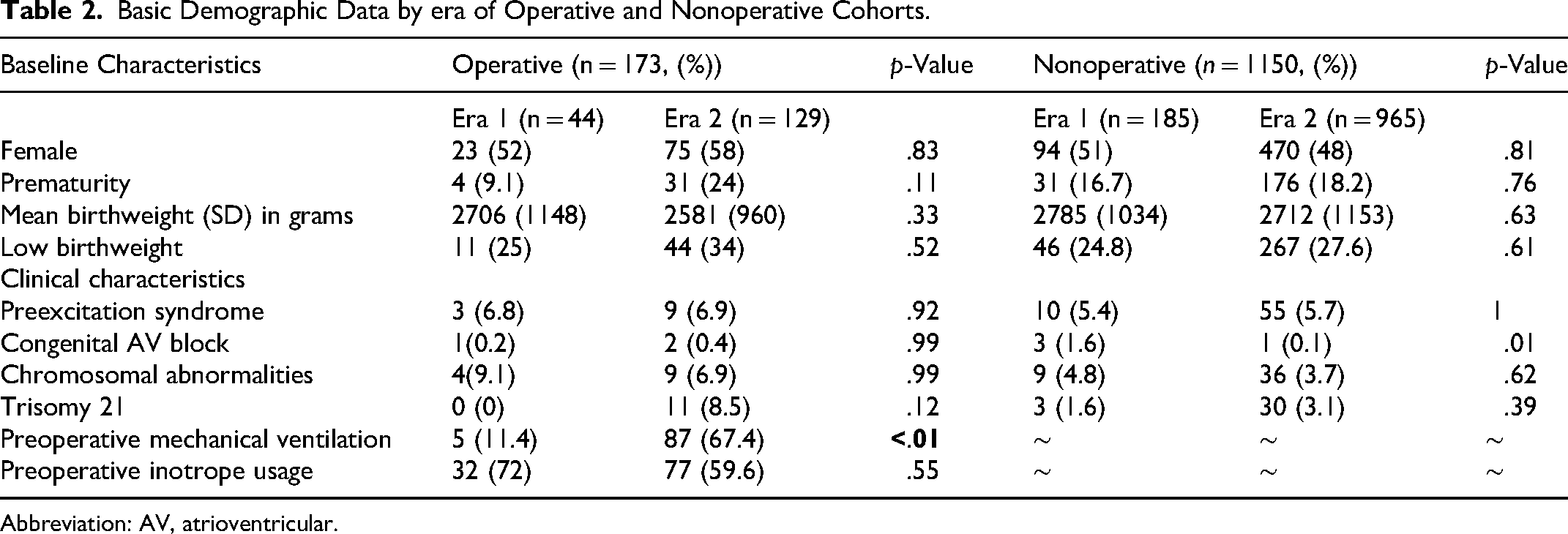
Abbreviation: AV, atrioventricular.
Inpatient outcomes by era (era 1 = 2004-2014, era 2 = 2015-2024) were compared within the operative and nonoperative cohorts. In the operative cohort, there was no significant difference between mortality (20.5% [9/44] vs 28.7% [37/129], p = .38), intensive care unit (ICU) and hospital length of stay, cost of hospitalization, median day of index operation, or postoperative complications except for delayed sternal closure (0 vs 14/129 (10.9%), p = .05). Postoperative inotrope usage was also not significantly different between eras in the operative cohort. In the nonoperative cohort, there were no significant differences between ICU length of stay, hospital length of stay, cost of hospitalization, or extracorporeal membrane oxygenation (ECMO) use. There was a significant decrease of inotrope usage in era 2 as compared with era 1 (47% [87/185] vs 34.7% [335/965, p = .04), and there has been an improvement in overall mortality recently (18.4% [34/185] vs 11.7% [113/965], p = .01). Rates of transplantation were low, with 5/173 (2.9%) transplants in total occurring in the operative cohort, with no difference of usage between era 1 and era 2 (4.5% [2/44] vs 2.3% [3/129] , p = 0.21) (Table 3).
In-Hospital Outcomes.
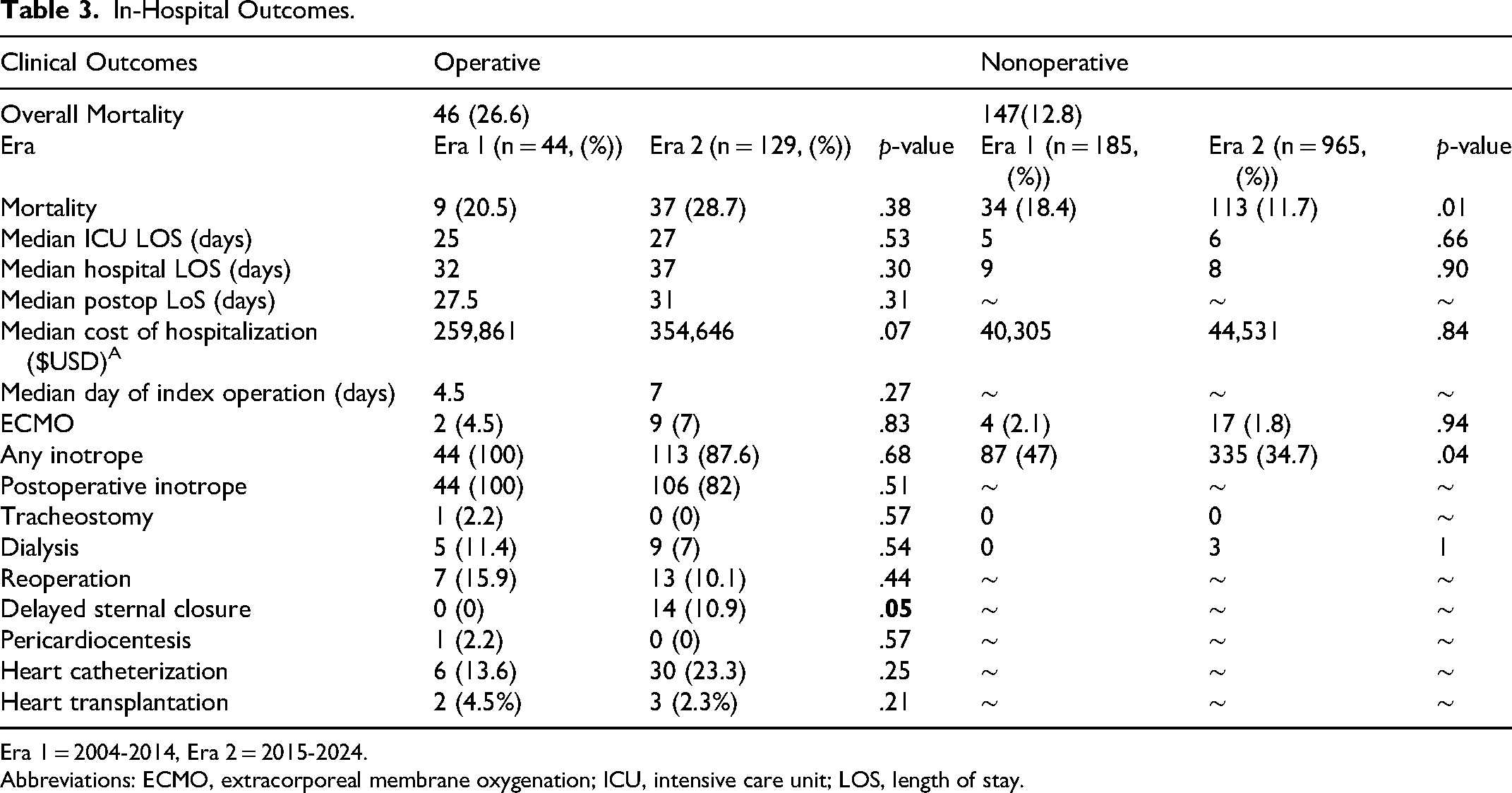
Era 1 = 2004-2014, Era 2 = 2015-2024. Abbreviations: ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; LOS, length of stay.
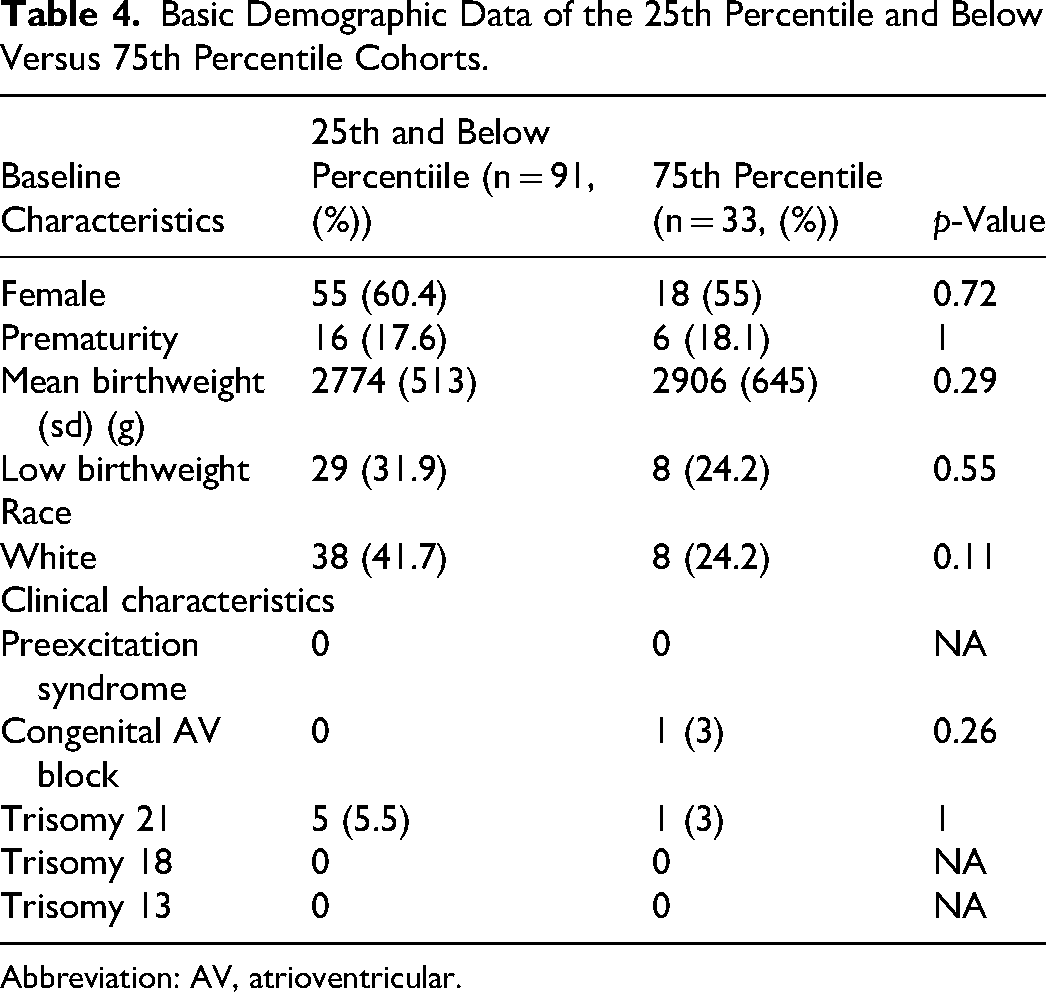
Within the operative cohort, compared with hospitals in ≤25th percentile for EA admissions, those in ≥75th percentile had significantly decreased odds of in-hospital mortality when the patient required cardiac surgery (27.5% vs 19.6% (OR 0.39 [p = .04])) on univariate analysis. Baseline demographic and clinical characteristics were compared between patients in the 25th percentile and below (n = 91) versus the 75th percentile (n = 33) (Table 4). The groups showed similar distributions across all measured variables. Gender distribution was comparable, with 60.4% female in the lower percentile group versus 55% in the 75th percentile group (p = .72). Prematurity rates were nearly identical between groups (17.6% vs 18.1%, p = 1.00). Mean birthweight was slightly higher in the 75th percentile group (2906 ± 645 g) compared with the lower percentile group (2774 ± 513 g), although this difference was not statistically significant (p = 0.29). The proportion of low birthweight infants was similar between groups (31.9% vs 24.2%, p = 0.55). Racial distribution, assessed by the proportion of White patients, showed no significant difference (41.7% vs 24.2%, p = .11). Clinical characteristics, including congenital AV block, Trisomy 21, and other chromosomal abnormalities, were infrequent and showed no significant differences between groups (all p > .05). Only 26.6% of those who underwent cardiac surgery were at hospitals that were ≥75th percentile of Ebstein admissions (Figure 2).
Hospital admission volume of Ebstein anomaly (EA) patients versus mortality.
Basic Demographic Data of the 25th Percentile and Below Versus 75th Percentile Cohorts.
Abbreviation: AV, atrioventricular.
A multivariate analysis for factors associated with mortality was conducted with the operative cohort (Table 5). Of note, factors that were independently associated with mortality were prematurity and low birthweight. Preoperative mechanical ventilation (MV), preoperative inotropes, postoperative ECMO, postoperative prolonged MV (defined as >7 days), delayed sternal closure, institutional volume, and era were not independent risk factors for mortality. However, postoperative inotrope use had a protective effect with a trend toward significance (OR 0.36 (0.11-1.09), p = .06).
Multivariate Analysis of Operative Cohort.
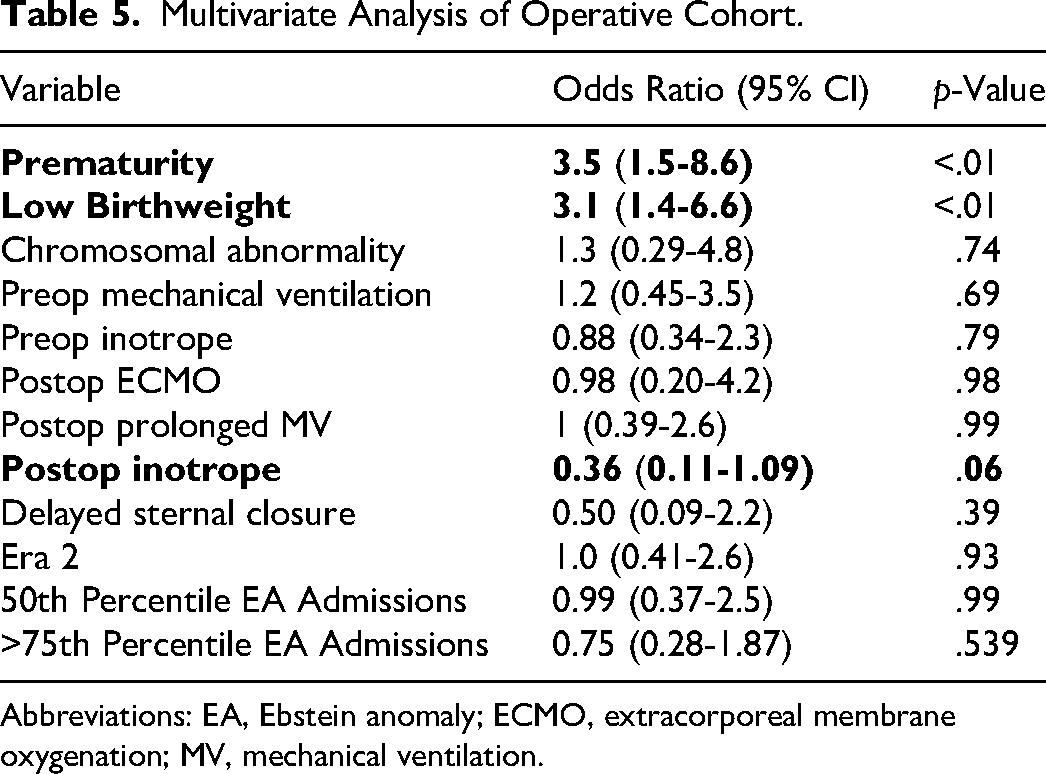
Abbreviations: EA, Ebstein anomaly; ECMO, extracorporeal membrane oxygenation; MV, mechanical ventilation.
In the nonoperative cohort, hospital volume of EA admissions was not significantly associated with mortality (Figure 2). In total, 690/1150 (60%) neonates did not require MV, 136/1150 (11.8%) required MV for 3 to 7 days, 88/1150 (7.7%) required MV for 7 to 13 days, and 105/1150 (9.1%) required MV for ≥14 days. As compared with those who did not require intubation (mortality 6.2% [43/690]), odds of mortality were significantly increased when MV was needed for 7 to 13 days and ≥14 days of MV (6.2% vs 20.5% [141/690] (OR 8.5, [p≤.01]); and 25.7% (OR 7.8, [p≤.01], respectively)) (Table 3).
A multivariate analysis for factors associated with mortality was also conducted in the nonoperative cohort (Table 6). In this analysis, prematurity (OR 3.8(2.4-5.8), p < .01), low birthweight (OR 2.7(1.8-4.2), p < .01), inotrope use (OR 7.1(4.4-11), p < .01), and ECMO (OR 5(1.9-13)), p < .01) were all independently associated with mortality. Era 2 was independently protective against mortality (OR 0.5(0.36-1.0), p = .05). Chromosomal abnormalities were found to be protective (OR 0.08(0.005-0.44)), p = .02), but it is difficult to draw conclusions from this data point, as there was a very low prevalence. Prolonged MV (defined as >7 days) (0.69 (0.41-1.1, p = 0.16) was not independently associated with mortality, nor was hospital EA admission volume.
Multivariate Analysis of Nonoperative Cohort Factors.
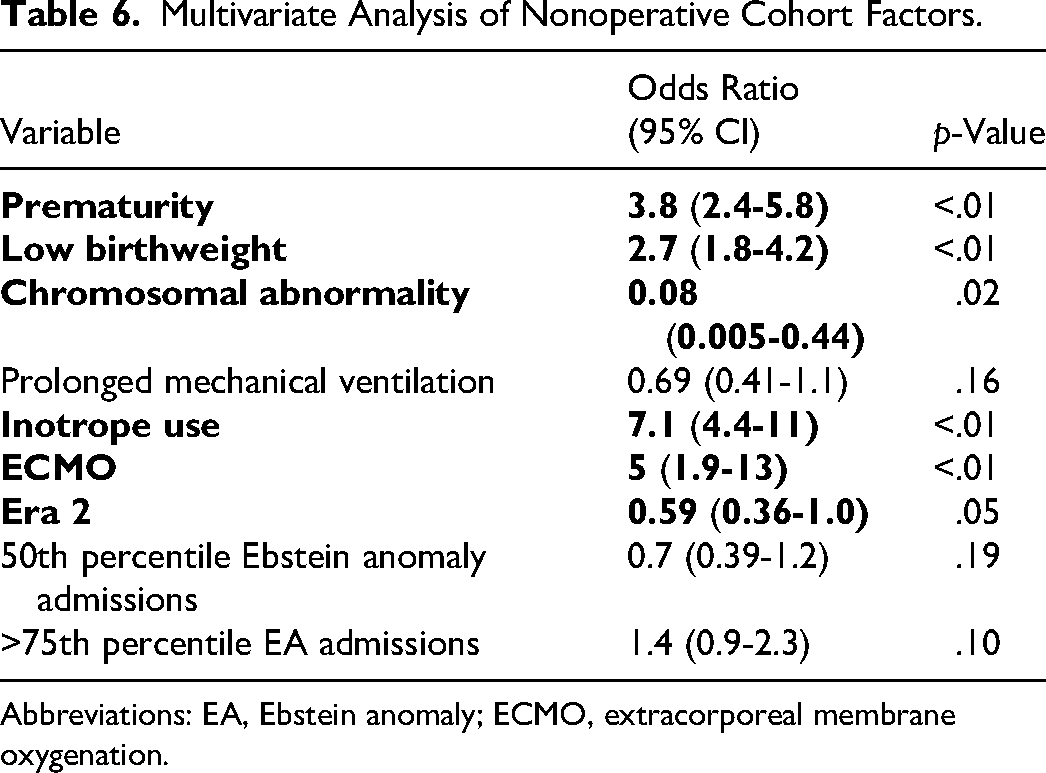
Abbreviations: EA, Ebstein anomaly; ECMO, extracorporeal membrane oxygenation.
Comment
This comprehensive multi-institutional report demonstrates the significant surgical and nonsurgical mortality in neonatal patients with Ebstein Anomaly (EA) without pulmonary atresia. The current study is unique in that it analyzes all EA admissions across two decades and allows assessment of operative and nonoperative treatment. To our knowledge, this analysis also represents one of the largest population-based cohorts of neonatal EA.
Of all neonates with EA, 13% (173/1323) underwent operative repair using cardiopulmonary bypass with a median day of operation between 4 and 7 days of age. We report an in-hospital mortality of 26.6% (46/173) for surgical patients, consistent with other studies. 10 Surprisingly, when divided by era, the more recent surgical cohort had similar mortality (29%, 37/129) to the earlier era (29% vs 21% [9/44, p = .38) despite having similar demographics. There were not many differences in the cohorts’ postoperative outcomes, except for an increased use of delayed sternal closure recently.
The 2024 American Association for Thoracic Surgery guidelines regarding operative management of EA suggest that surgical intervention be performed at specialty centers. 11 In our study, we found that neonates admitted to high-volume centers (>75th percentile) specializing in EA cases had a 30% decrease in mortality rates (27.5% vs 19.6%) on univariate analysis. Although institutional volume was not independently predictive of mortality after multivariate adjustment, the observed differences in crude mortality may suggest that unmeasured factors related to experience and care coordination may influence outcomes. For example, our findings may suggest that postoperative inotrope use serves as a marker of institutional care quality rather than an independent protective factor. Likely, high-volume centers have systematic inotrope protocols (95.7% usage rate) and likely represent one component of comprehensive perioperative management that contributes to their improved outcomes. However, only 26.6% of operative patients underwent cardiac surgery at these high-volume centers, highlighting a potential opportunity for improvement in surgical mortality. Interestingly, Freud et al 3 reported outcomes of neonatal EA patients with a higher proportion of their patients undergoing operative intervention as compared with our study, and had worse operative mortality rates (30%–50%), although they included those with pulmonary atresia. They, too, highlight the impact of low operative volume as a contributor to higher operative mortality rates. Surgical strategies include biventricular repairs such as a Knott-Craig repair or Cone repair, with or without the use of single-ventricle palliation as a bridge to biventricular repair.12–14 Due to the complexity of these repairs, the PHIS database is unable to differentiate these surgical strategies. Other single-center series focusing exclusively on biventricular repairs in neonates without pulmonary atresia have reported mortality rates <10%, highlighting the potential to improve outcomes with specialized centers and appropriate patient selection. 15 Finally, we report a transplantation rate of 3.2%, which was lower than we would expect and may be an underutilized treatment in this patient population. This phenomenon has been observed in a previous study by Eckerström et al. 16
Prenatal diagnosis of Ebstein anomaly represents an important consideration that may significantly influence surgical outcomes, although our database does not distinguish between prenatal and postnatal diagnoses. 17 When identified in utero, families can be referred to high-volume centers with specialized expertise in managing complex congenital heart disease, which allows for parental counseling to discuss treatments and expected outcomes. With increased use of fetal echocardiography in recent years, more cases of Ebstein anomaly with less severe anatomy are likely being diagnosed prenatally and admitted in the neonatal period. This may potentially shift the nonsurgical group toward simpler cases with lower mortality. The distinction between prenatal and postnatal diagnosis warrants consideration in future studies, as it may impact both case selection and the opportunity for preoperative optimization.
In the nonoperative cohort, the overall mortality was 12.8% (147/1150) with significant improvement in mortality rates recently (18.4% [34/185] vs 11.7% [113/965] , p = .01). Theera 2 mortality in the nonoperative cohort was 11.7%, comparable with another published study. 18 When we compared mortality outcomes across institutions of variable volume of total EA admissions, we found no significant difference between high-volume and low-volume centers. Combined with the decreased use of inotropes across eras without a significant difference in baseline characteristics, we interpret this as a global improvement in heart failure therapies and cardiac rehabilitation strategies. However, when we stratified outcomes based on duration of MV, we observed a progressively increased mortality, which was significant after 7 days. Indeed, mortality rates were almost equal to surgical mortality when MV was required for more than 14 days, although prolonged MV was not independently associated with mortality. Additionally, the operative group in the recent era has a significantly higher percentage of mechanically ventilated patients. Operating on more critically ill patients removes them from the nonoperative group, which may explain the decreased nonoperative mortality and potentially increased surgical mortality. Still, perhaps in this patient population, a surgical consultation could be considered in a high-volume center. Among patients with chromosomal abnormalities, particularly those with Down syndrome, elevated pulmonary vascular resistance is more prevalent and may develop earlier than in patients without chromosomal abnormalities. 19 Careful assessment of pulmonary vascular resistance is essential in this subpopulation, with surgical intervention optimally deferred until pulmonary vascular resistance returns to acceptable levels. Along those same lines, the higher prevalence of trisomy 21 in the operative cohort may reflect more severe anatomic derangement in patients with Down syndrome, potentially related to pulmonary vascular disease.
A key limitation of this study is its observational and retrospective design, which constrains the conclusions that can be drawn from the data. The retrospective nature also places the study at risk for biased data collection, particularly given our exclusion of other concomitant single ventricle diagnoses and those with pulmonary atresia. This database lacks the capacity to definitively elucidate functional versus anatomic pulmonary atresia. The PHIS database also lacks granular hemodynamic and echocardiographic data, which are routinely used for decision-making in EA patients. Surgical procedures in EA patients vary widely, and there may be unmeasured confounding by institutional factors. Furthermore, due to the variety and lack of granularity with ICD procedure codes for this lesion, we were unable to ascertain specific surgical procedures, such as Starnes palliation or cone repair, which can make mortality comparisons difficult.
In the contemporary landscape, significant surgical (27%) and nonsurgical (13%) mortality in neonates with EA persists. Unsurprisingly, prematurity and low birthweight continue to be associated with mortality regardless of strategy. While these cohorts have not changed over time, operative survival has not improved, while nonsurgical survival has significantly. Nonoperative EA neonates, who are never intubated, do very well (94% survival), unlike those who are intubated for over a week, who have a mortality >20%. Perhaps consideration of an operative strategy for this cohort should be considered if feasible. The divergent temporal trends between operative and nonoperative outcomes highlight the complexity of care decisions in this population. Persistent surgical mortality likely reflects the inherent risk in the sickest neonates who require intervention. The data should not be interpreted as suggesting medical management is superior to surgery; rather, appropriate patient selection is critical. These findings provide essential epidemiologic data for counseling families, planning healthcare resources, and identifying priorities for future research and quality improvement initiatives.
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
David L. S. Morales is a consultant for Abbott, Inc., Azyio, Inc., Berlin Heart, Inc., CorMatrix, Inc., Peca, Inc., Syncardia, Inc., and Xeltis, Inc., and a principal investigator for FDA trials sponsored by Peca, Inc. and Xeltis, Inc. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.