
Abstract
Dextro-transposition of the great arteries is a critical cyanotic congenital heart defect in which neonatal survival depends on effective intercirculatory mixing. Balloon atrial septostomy (BAS) improves atrial-level mixing; however, many infants remain dependent on prostaglandin E1 (PGE1) following the procedure, reflecting a disconnect between successful anatomical intervention and physiological adaptation. This review synthesizes the underlying physiology, available clinical evidence, and practical considerations for PGE1 management following BAS. Available data indicate that postprocedural systemic oxygen saturation and restrictive atrial or ventricular physiology are the strongest predictors of ongoing PGE1 requirement. Early discontinuation, often prompted by procedural success, is often associated with rebound hypoxemia, suggesting that physiological stabilization may lag anatomical intervention. The continuation of PGE1 appears safe and serves as supportive management during the transitional cardiopulmonary period rather than as a marker of procedural failure or a determinant of surgical timing. A physiology-guided, individualized approach to PGE1 discontinuation is therefore recommended. Prospective multicenter studies are needed to refine clinical criteria and optimize preoperative stabilization and outcomes.
Keywords
Introduction
Dextro-transposition of the great arteries (d-TGA) is a common, critical congenital heart defect 1 for which successful repair via the arterial switch operation (ASO) hinges on effective preoperative stabilization. 2 In the immediate neonatal period, survival depends on adequate intercirculatory mixing between the parallel systemic and pulmonary circulations. This stabilization has 2 main components: pharmacological maintenance of ductal patency with prostaglandin E1 (PGE1) and, when necessary, procedural enhancement of atrial-level mixing via balloon atrial septostomy (BAS).3,4 While ductal patency augments pulmonary blood flow and pulmonary venous return, it does not substitute for an adequate atrial communication, which remains essential for effective intercirculatory mixing.
A persistent clinical dilemma in preoperative care is the management of PGE1 following a successful BAS. While BAS reliably improves systemic oxygenation, a significant proportion of infants, reported between 40% and 65%, experience rebound hypoxemia upon PGE1 discontinuation and require its reinstitution. This creates a conflict between the anatomical success of the septostomy and the ongoing physiological need for ductal patency. This apparent discordance is best understood as a reflection of the dynamic neonatal cardiopulmonary transition, particularly the evolving interplay among pulmonary vascular resistance (PVR), ventricular compliance, and interatrial flow dynamics.
For the congenital heart team, this dilemma has direct implications for preoperative care, influencing clinical stability, resource utilization, and the physiological preparedness of the neonate for major surgery. Despite being frequently encountered in clinical practice, post-BAS PGE1 dependence remains poorly characterized in the literature, with available evidence largely limited to small observational cohorts and institutional experiences. The absence of a unified, physiology-based framework contributes to variability in clinical practice, particularly in decisions about discontinuing prostaglandin therapy. In this review, we integrate physiological principles with available clinical evidence to reframe post-BAS PGE1 dependence not as a failure of septostomy, but as an adaptive response to transitional cardiopulmonary physiology.
Physiological Framework: Why Ductal Patency May Still Matter After Balloon Atrial Septostomy
The effectiveness of intercirculatory mixing in d-TGA depends more on cardiopulmonary flow dynamics than solely on the presence of anatomical connections. Balloon atrial septostomy establishes reliable atrial communication; however, the magnitude and direction of shunting across the atrial septum are influenced by multiple interacting physiological factors, including PVR, ventricular compliance, atrial pressure gradients, and the geometry and orientation of the atrial communication.
In the early postnatal period, PVR is often elevated or labile, which may limit effective pulmonary blood flow despite an adequate atrial communication. Under conditions of high or supra-systemic right ventricular pressures, the patent ductus arteriosus may demonstrate bidirectional shunting and can function as a pressure-relief pathway for the systemic right ventricle. As pulmonary vascular resistance falls, ductal patency may also augment pulmonary blood flow and increase pulmonary venous return to the left atrium, thereby promoting more effective interatrial mixing through the atrial communication. 5
Beyond pressure relationships, ventricular and atrial compliance also influence the efficiency of atrial-level mixing. Restrictive right ventricular physiology or limited left atrial compliance may impair the effective transfer of blood across the atrial septum, even when the atrial communication is large. In these situations, ductal flow may provide an additional pathway for circulatory unloading and may support pulmonary blood flow until ventricular filling dynamics and PVR evolve during the early neonatal transition.
Finally, preferential flow patterns influence the distribution of oxygenated pulmonary venous return. Efficient mixing requires that oxygenated blood entering the left atrium preferentially cross the atrial septum toward the systemic (right) ventricle. When this preferential flow is suboptimal, oxygenated blood may recirculate within the pulmonary circuit. Under these circumstances, ductal flow can supplement systemic oxygen delivery by allowing oxygenated blood from the pulmonary artery to enter the descending aorta, partially compensating for inefficient atrial-level transfer.
Together, these dynamic interactions explain why ductal patency may remain physiologically important even after the creation of a nonrestrictive atrial septal defect, particularly during the transitional neonatal circulation, when pulmonary vascular resistance, ventricular compliance, and intracardiac flow patterns are still evolving. 6
Clinical Evidence: Predictors of Post-Balloon Atrial Septostomy Prostaglandin E1 Dependence
The collective evidence from surgical and intensive care literature (Table 1) establishes a clear pattern regarding which infants are likely to remain PGE1-dependent after BAS. Across multiple cohorts, attempted trial discontinuation of PGE1 following BAS results in rebound hypoxemia requiring reinstitution in ∼40% to 65% of infants.7–13 This high prevalence highlights the disconnect between BAS procedural success and physiological readiness for ductal independence.
Summary of Studies Evaluating Prostaglandin E1 Use following Balloon Atrial Septostomy in d-Transposition of the Great Arteries.
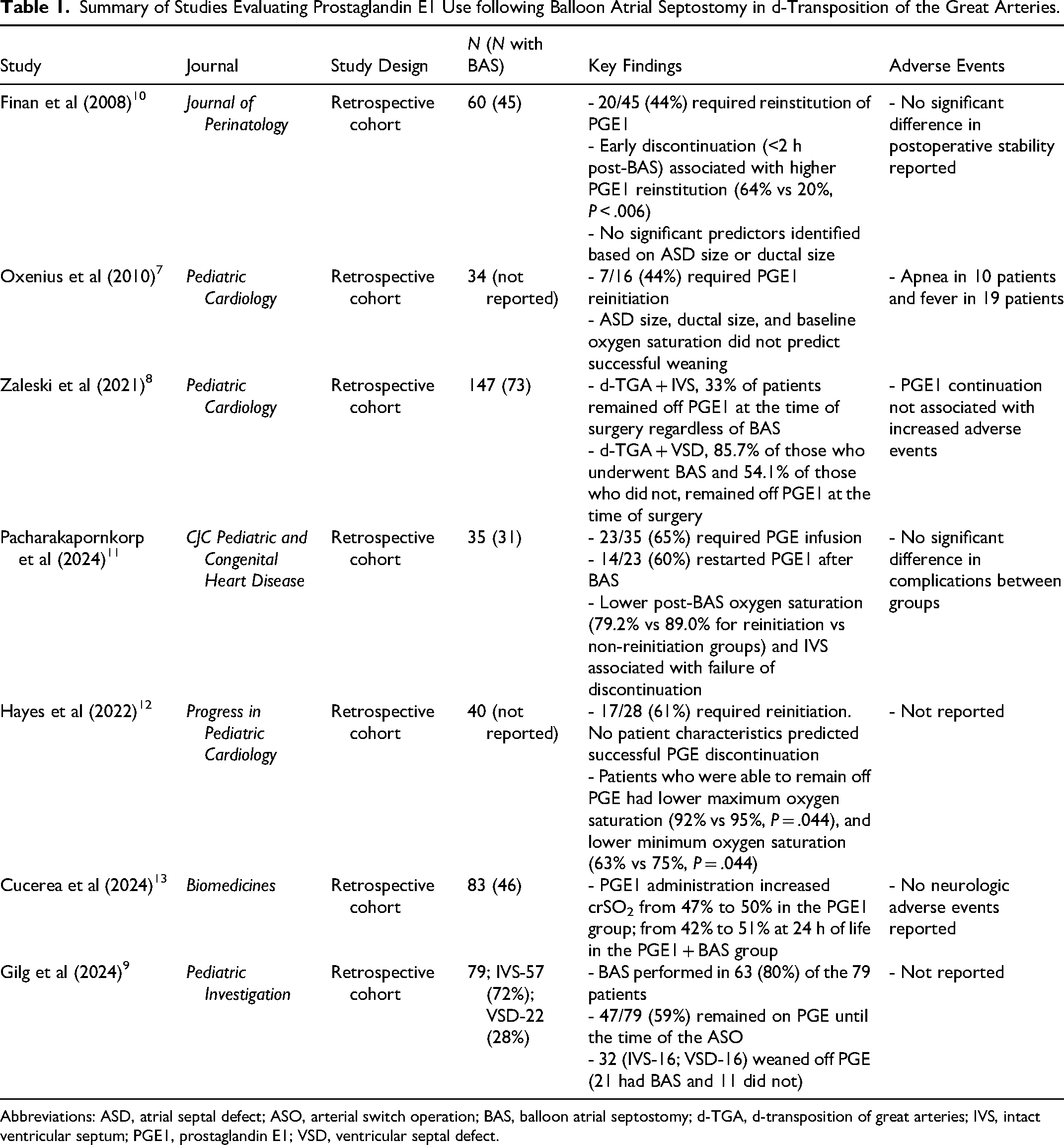
Abbreviations: ASD, atrial septal defect; ASO, arterial switch operation; BAS, balloon atrial septostomy; d-TGA, d-transposition of great arteries; IVS, intact ventricular septum; PGE1, prostaglandin E1; VSD, ventricular septal defect.
Within this data, consistent predictors of ongoing dependence emerge. The most reliable indicator is postprocedural systemic oxygen saturation; infants who stabilize with an SpO2 ≤ 80% to 85% are significantly more likely to require ongoing PGE1 support compared with those achieving higher saturations. In contrast, static anatomical parameters, including atrial septal defect size, have not demonstrated consistent predictive value for successful discontinuation of therapy.7,11
The timing of PGE1 trial discontinuation is also critical. Early attempts to discontinue PGE1, particularly within the first 12 to 24 h following BAS, are strongly associated with a significantly higher likelihood of reinstitution. 10 These findings suggest that premature attempts to stop PGE1 often occur before adequate pulmonary vascular adaptation is achieved, rather than reflecting an ineffective septostomy.8,12 Clinical practice in many centers, therefore, favors a period of physiological stabilization before attempting discontinuation, allowing PVR and ventricular filling dynamics to evolve.
Underlying cardiac anatomy also influences the likelihood of persistent dependence. Infants with d-TGA and an intact ventricular septum are more likely to remain PGE1-dependent than those with a ventricular septal defect, as the latter provides an additional mixing site that partially compensates for limited atrial transfer.8,9
Available data suggest that continued PGE1 therapy is not associated with a significant increase in adverse events among infants maintained on therapy until surgery.5,7,12,14 Furthermore, emerging observational data suggest that maintenance of ductal patency may support systemic and cerebral oxygen delivery during the unstable transitional period, further reinforcing the rationale for cautious physiological assessment before attempting discontinuation. 13
Toward a Physiology-Guided Management Strategy
Considering the available evidence, a shift from arbitrary, time-based decisions regarding PGE1 discontinuation to a structured, physiology-informed management approach is justified. Rather than presuming that a technically successful BAS should lead to immediate prostaglandin withdrawal, clinicians should recognize that physiological readiness for ductal independence may lag the anatomical intervention.
Figure 1 outlines a physiology-informed framework for post-BAS PGE1 management, emphasizing an initial period of stabilization followed by integrated clinical assessment to guide decisions regarding trial discontinuation.

A physiology-informed framework for PGE1 management following balloon atrial septostomy in neonates with d-TGA. Following BAS, a period of hemodynamic stabilization is recommended before reassessment. Decisions regarding discontinuation of PGE1 should incorporate integrated physiologic assessment, including systemic oxygenation, echocardiographic findings, and overall clinical stability. A monitored trial discontinuation may be attempted when physiologic stability is achieved. Rebound hypoxemia should prompt reinstitution of prostaglandin therapy. Continued PGE1 therapy represents a safe and physiologically appropriate bridge to the arterial switch operation, particularly in infants with risk features such as intact ventricular septum, restrictive physiology, or borderline oxygenation. Abbreviations: d-transposition of the great arteries, dextro-transposition of the great arteries; PGE1, prostaglandin E1.
Clinical decision-making should therefore be grounded in an integrated evaluation of systemic oxygenation, hemodynamic stability, and echocardiographic findings, rather than a single parameter. Importantly, failure to tolerate discontinuation should not be interpreted as a procedural limitation of BAS, but rather as an expected manifestation of ongoing transitional physiology. In such cases, continued PGE1 therapy represents a physiologically appropriate and safe strategy to maintain systemic oxygen delivery until definitive surgical repair.
Surgical and Perioperative Implications
Adopting a physiology-guided approach to PGE1 management has direct and meaningful implications for the surgical pathway in infants with d-TGA. First, avoiding premature discontinuation and subsequent rebound hypoxemia may help prevent episodes of metabolic instability and secondary end-organ stress, thereby helping ensure that neonates present for the arterial switch operation in optimal physiological condition.
Second, acknowledging that a substantial proportion of infants will remain PGE1-dependent despite a technically successful BAS allows for more realistic expectations regarding preoperative management in the intensive care unit. Recognizing ongoing prostaglandin therapy as a physiological requirement rather than a procedural failure helps avoid repeated cycles of discontinuation and reinstitution that may destabilize the neonate without providing clinical benefit.
Finally, dependence on prostaglandin therapy should not be interpreted as a determinant of surgical timing. 3 In contemporary practice, the timing of the arterial switch operation should primarily reflect the infant's overall clinical stability and the institution's surgical strategy rather than the neonate's ability to discontinue PGE1. Indeed, early definitive repair may be preferable in some circumstances, as prolonged reliance on temporizing physiological support strategies, including BAS and prostaglandin therapy, does not substitute for corrective surgery. 14
Knowledge Gaps and Future Directions
While retrospective data are compelling, well-designed prospective, multicenter studies, particularly pragmatic or protocol-based observational studies, are needed to refine oxygen saturation thresholds and physiology-based criteria that inform PGE1 discontinuation following BAS. Linking preoperative PGE1 management strategies to postoperative outcomes, including duration of mechanical ventilation, inotropic support requirements, and early neurological or neurodevelopmental markers, would be particularly valuable for the cardiac surgical and perioperative care community. Such studies could clarify whether physiology-guided prostaglandin management is associated with improved perioperative stability or postoperative recovery following ASO. In addition, defining the role of advanced monitoring modalities, such as cerebral near-infrared spectroscopy, in guiding PGE1 continuation or discontinuation represents a promising frontier that may allow more precise, real-time assessment of systemic and cerebral oxygen delivery during the transitional period.
Conclusion
For the infant with d-TGA, a successful BAS is a necessary but often insufficient step toward achieving physiological independence from the ductus arteriosus. Ongoing PGE1 dependence is a common and rational manifestation of transitional cardiopulmonary physiology. Embracing a deliberate, physiology-guided management protocol that prioritizes sustained oxygenation and overall physiological stability, rather than anatomical findings in isolation, enables the multidisciplinary team to provide optimal, stable preoperative care. Importantly, continued prostaglandin dependence should not be interpreted as a failure of septostomy or as a determinant of surgical timing. Instead, it reflects the dynamic interaction between pulmonary vascular transition, ventricular compliance, and intracardiac flow patterns in the early neonatal period. This approach ensures that the neonate with d-TGA is delivered to the operating room for the arterial switch operation in the best possible physiological condition, ready for a successful repair.
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
Not applicable.
Consent to Publication
Not applicable.
Author Contributions
JLN conceptualized, drafted the original manuscript, and participated in the review and editing. JCN conceptualized and participated in the review and editing. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.