
Abstract
Background
Optimal oxygenation strategies during cardiopulmonary bypass (CPB) in children with cyanotic congenital heart disease remain controversial. Although hyperoxia has traditionally been used to compensate for chronic hypoxemia, concerns exist regarding reoxygenation injury and oxidative stress. This systematic review and meta-analysis aimed to compare perioperative normoxic versus hyperoxic strategies during CPB in this population.
Methods
We performed a literature search in MEDLINE, Embase, and the Cochrane Library from inception to November 2025. Random-effects models were used to pool risk ratios (RRs) for binary outcomes and mean differences for continuous outcomes. Heterogeneity was assessed using the I2 statistic, and risk of bias was evaluated using the RoB 2 tool.
Results
Five randomized controlled trials comprising 241 children were included, with 121 patients allocated to normoxia and 120 to hyperoxia. There were no statistically significant differences between groups in all-cause mortality (RR 1.31; 95% confidence interval [CI] 0.37-4.67; P = .67; I2 = 0%). Postoperative recovery outcomes, including intensive care unit (ICU) stay, ventilation time, length of hospital stay, and duration of inotropic support, were also comparable. Operative parameters (CPB time and aortic cross-clamp time) and safety outcomes, such as neurological complications, arrhythmias, and cardiac arrest, did not differ significantly between strategies.
Conclusion
In children with cyanotic congenital heart disease undergoing surgery with CPB, normoxic, and hyperoxic oxygenation strategies were associated with statistically similar mortality, recovery, operative, and safety outcomes. These findings suggest that carefully monitored normoxic strategies may represent a safe and physiologically sound alternative to routine hyperoxia during CPB.
Keywords
Introduction
Children with cyanotic congenital heart disease frequently require early surgical repair with the use of cardiopulmonary bypass (CPB).1,2 During CPB, perfusionists, cardiothoracic surgeons, and anesthesiologists regulate oxygen delivery to the blood and tissues by adjusting pump flow and inspired oxygen fraction (FiO2), thereby modulating arterial oxygen saturation (SaO2) and partial pressure of oxygen (PaO2).3,4 Traditionally, many centers have adopted hyperoxic strategies, maintaining oxygen levels well above physiological ranges in an attempt to compensate for chronic hypoxemia and provide adequate tissue reserve during CPB. 5 However, this approach exposes patients chronically adapted to low oxygen levels to an acute hyperoxic environment in the setting of systemic inflammation and ischemia reperfusion.5,6
From a pathophysiological standpoint, hyperoxia may increase the production of reactive oxygen species, amplify reperfusion injury, and potentially contribute to myocardial dysfunction, neurological injury, and worse postoperative outcomes.7,8 Conversely, there is concern that more physiological, normoxic strategies might be insufficient in children with long-standing hypoxemia, especially neonates, leading to tissue ischemia, hemodynamic instability, and neurological complications.9,10 Randomized and observational studies in the pediatric setting remain relatively small and heterogeneous, with varying definitions of normoxia and hyperoxia, different age ranges, and diverse diagnoses, such as tetralogy of Fallot and other cyanotic lesions.11,12 As a result, clinical practice is highly variable across institutions, and there is no clear consensus on the optimal oxygenation strategy during CPB in children with cyanotic congenital heart disease.6,13
In light of this ongoing uncertainty, we performed a systematic review and meta-analysis of randomized controlled trials (RCTs) directly comparing normoxia versus hyperoxia during CPB in children with cyanotic congenital heart disease. In this context, we aimed to synthesize the available evidence from RCTs comparing different oxygenation strategies during CPB in this same patient population. Specifically, we sought to determine whether an intraoperative approach targeting normoxia, as opposed to hyperoxia, is associated with differences in all-cause mortality, postoperative recovery, operative parameters, and safety outcomes.
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted in accordance with the Cochrane Handbook and reported following PRISMA guidelines.14,15 The protocol was registered in PROSPERO (CRD420251240511). 16
Eligibility Criteria
Inclusion in this meta-analysis was restricted to studies that met all of the following eligibility criteria: (1) enrollment of pediatric patients with cyanotic heart disease undergoing surgical repair; (2) RCT design; (3) direct comparison of normoxemia versus hyperoxemia during CPB, and (4) reporting of at least one outcome of interest. Studies were excluded if they (1) were published in a language other than English or (2) included overlapping patient populations.
Search Strategy and Study Selection
We systematically searched PubMed, Embase, and Cochrane Library databases from inception to November 22, 2025. The detailed search strategy for each database is provided in Supplemental Table 1. We also searched the references of the included studies and previous systematic reviews and meta-analyses, aiming for the inclusion of additional studies. 17 Two authors (LBG and LMD) independently conducted the search, imported results into Rayyan, a web-based systematic review tool, and triaged the studies. After the exclusion of duplicates and titles/abstracts unrelated to the clinical question, the eligibility of each remaining study was assessed based on the review of the full-text articles. Disagreements were resolved by a third author (RENNO).
Data Extraction
Two authors (LMD and LBG) independently extracted data from the included studies using a standardized form, including general study characteristics (first author, year of publication, study period, trial registration, and country), intervention details (target PaO2 ranges for the normoxia and hyperoxia groups), participant characteristics (number of patients, age at surgery, sex distribution, and primary diagnosis), categories of oxidative stress biomarkers, and reported outcomes.
Outcomes
The outcomes of interest were: (1) all-cause mortality, (2) intensive care unit (ICU) stay, (3) ventilation time, (4) postoperative length of stay, (5) CPB time, (6) aortic clamp time, (7) duration of inotropic support, (8) neurological complications, (9) cardiac arrest, and (10) arrhythmia.
Risk of Bias and Certainty Assessment
Two independent reviewers (FSP and LMD) assessed the risk of bias of randomized trials using the Risk of Bias 2.0 tool (RoB 2). 18 Disagreements were solved by consensus. Publication bias could not be assessed adequately because the power of this test is insufficient to discriminate between chance and true funnel plot asymmetry when analyzing fewer than 10 studies. 19 We evaluated the certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool, classifying it as high, moderate, low, or very low certainty. 20
Statistical Analysis
We used the restricted maximum likelihood random-effects model to calculate pooled risk ratios (RRs) for binary outcomes and mean differences (MDs) for continuous outcomes, both with 95% confidence intervals (CIs). Significance was regarded as a P value <.05. Between-study heterogeneity was assessed using the Cochran Q test and I2 statistics, and we considered a P value of <.10 and an I2 > 25% as significant for heterogeneity. For outcomes with significant heterogeneity, we performed leave-one-out sensitivity analysis to identify influential studies and their effect on the pooled estimates. We conducted all the statistical analyses using R statistical software (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
Study Selection
As detailed in Figure 1, the initial search identified 680 results. After removal of duplicate records and assessment of the studies based on title and abstract, 9 full-text studies remained for full review according to prespecified criteria. Of these, 5 RCTs, spanning from 2002 to 2025, were included.4,21–23 Supplemental Table 2 lists the excluded studies from the full-text screening stage and the reasons for their exclusion.
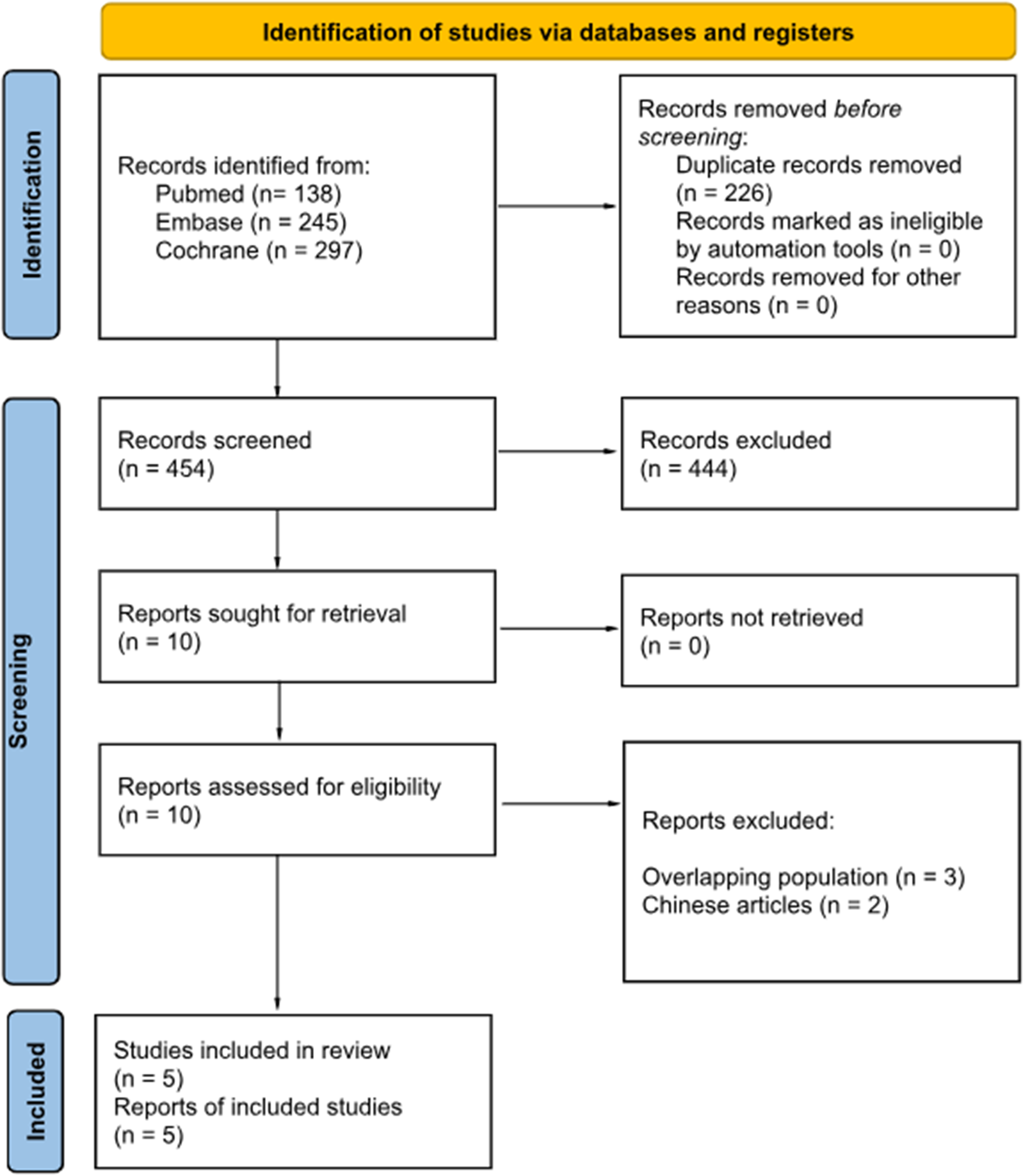
PRISMA flow diagram of study screening and selection. The articles were found from Pubmed, Embase, and Cochrane central.
Patient Characteristics
A total of 241 children with cyanotic heart disease were included across the 5 RCTs, with 121/241 (50.2%) allocated to the normoxia group and 120/241 (49.8%) to the hyperoxia group during CPB. Overall, 53.1% (128/241) of participants were male. One study included only neonates, with a mean age of 5 days, whereas the remaining 4 studies enrolled pediatric patients with a mean age of 15.4 months. The main demographic and clinical characteristics are summarized in Table 1. Tetralogy of Fallot (ToF) was the most frequent diagnosis, with 41/121 patients (33.9%) in the normoxia group and 42/120 patients (35.0%) in the hyperoxia group. Primary diagnoses are summarized in Supplemental Table 3.
Baseline Characteristics of Patients Across the Included Studies.
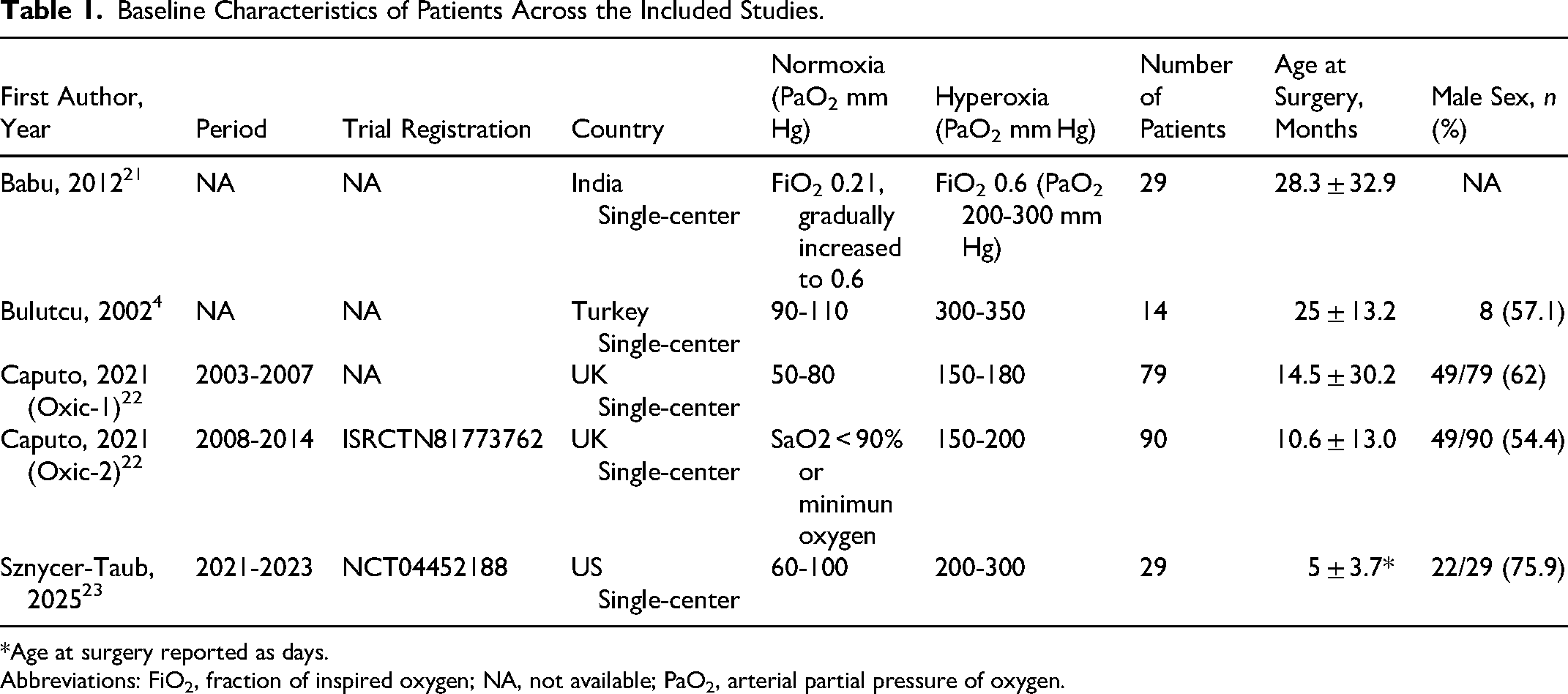
*Age at surgery reported as days.
Abbreviations: FiO2, fraction of inspired oxygen; NA, not available; PaO2, arterial partial pressure of oxygen.
Pooled Analysis
All-Cause Mortality
There were no statistically significant differences between groups for all-cause mortality (RR 1.31; 95% CI 0.37 to 4.67; P = .67; I2 = 0%; Figure 2).
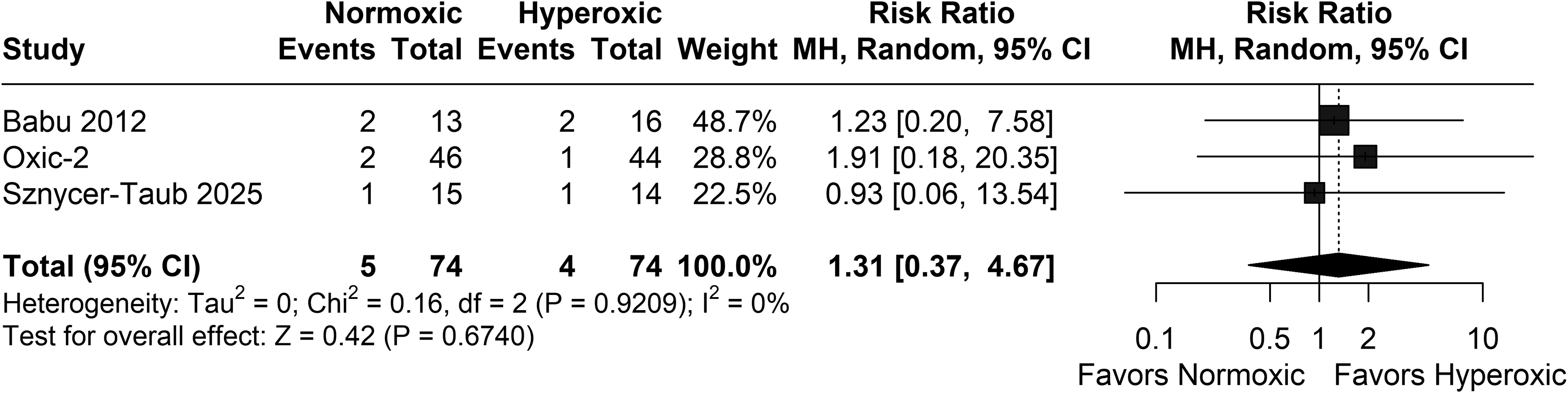
Normoxia versus hyperoxia groups for all-cause mortality. There is no statistically significant difference between the groups for mortality. Abbreviations: CI, confidence iterval; MH, mild hypoxia.
Postoperative Recovery
There were no statistically significant differences between groups for ICU length of stay (MD 14.28 h; 95% CI −36.63 to 10.06; P = .25; I2 = 25%; Supplemental Figure 1A), ventilation time (MD −4.11 h; 95% CI −12.62 to 4.40; P = .34; I2 = 30%; Supplemental Figure 1B), postoperative length of stay (MD 1.24 days; 95% CI −0.11 to 2.60; P = .07; I2 = 0%; Supplemental Figure 1C) and duration of inotropic support (MD 0.26 h; 95% CI −8.35 to 8.86; P = .95; I2 = 0%; Supplemental Figure 1D).
Operative Parameters
There were no statistically significant differences between groups for CPB time (MD 1.52 min; 95% CI −14.94 to 17.98; P = .86; I2 = 68%; Supplemental Figure 2A), and aortic clamp time (MD 1.43 min; 95% CI −6.51 to 9.36; P = .72; I2 = 40%; Supplemental Figure 2B).
Safety
There were no statistically significant differences between groups for neurological complications (RR 1.68; 95% CI 0.55 to 5.15; P = .36; I2 = 0%; Supplemental Figure 3A), arrhythmia (RR 1.24; 95% CI 0.52 to 2.98; P = .63; I2 = 43%; Supplemental Figure 3B), and cardiac arrest (RR 0.33; 95% CI 0.07 to 1.57; P = .16; I2 = 0%; Supplemental Figure 3C).
Sensitivity Analysis
For ventilation time, CPB time, and aortic clamp time, the exclusion of any individual study shifted the results from nonsignificant to favoring one of the interventions. However, the studies driving the high heterogeneity were identifiable in all 3 outcomes: for ventilation time, exclusion of the study by Babu et al markedly reduced heterogeneity, 21 whereas for CPB time and aortic clamp time, exclusion of the Oxic-2 trial substantially decreased heterogeneity. 22 Leave-one-out analyses are detailed in Supplemental Figures 4 to 6.
Risk of Bias and Certainty Assessment
As summarized in Supplemental Figure 7, the review synthesized small, prospective pediatric RCTs evaluating oxygen management during CPB in specialized academic cardiac centers. All trials showed comparable baseline and perioperative characteristics, clearly defined oxygen protocols, and exclusively in-hospital or ≤24h oxidative biomarker endpoints, supporting low risk of bias for outcome measurement and missing-data in the analyzed cohorts. Protocol deviations were infrequent, transparently safety-motivated, and fit a clinically plausible modified-ITT feasibility context. The rationales supporting each domain judgment are provided in Supplemental Table 4.
The certainty of evidence according to GRADE ranged from moderate to low across all outcomes, primarily due to imprecision and inconsistency, as detailed in Supplemental Table 5. Certainty was downgraded for inconsistency owing to substantial heterogeneity in pooled estimates, which was partly attributed to nonuniform definitions and indirect assessment proxies for normoxia/normoxemia, and for imprecision reflecting wide confidence intervals crossing the null, limited effective sample sizes, and low event counts. All of these factors further restricted confidence in the effect estimates.
Discussion
In this systematic review and meta-analysis of 5 RCTs including 241 children with cyanotic congenital heart disease undergoing surgery with CPB, we found no statistically significant differences between normoxic and hyperoxic strategies with respect to all-cause mortality, postoperative recovery parameters, operative variables, or major safety outcomes. Mortality rates were low in both groups, and no evidence of superiority was detected between oxygenation strategies. Similarly, ICU stay, duration of mechanical ventilation, hospital length of stay, and time under inotropic support did not differ significantly between normoxia and hyperoxia. CPB and aortic cross-clamp times were also comparable, as were the incidences of neurological complications, arrhythmias, and cardiac arrest.
These results do not support the longstanding assumption that high oxygen levels are necessary to compensate for chronic hypoxemia in this population.24,25 In many centers, hyperoxia remains the default approach during cardiopulmonary bypass, largely driven by concern about tissue hypoperfusion and the perceived safety margin provided by supraphysiological oxygen tensions.26,27 Our pooled analysis does not support a clear clinical advantage of hyperoxia in terms of short-term outcomes. Instead, the absence of differences in mortality, recovery, and major adverse events suggests that carefully monitored normoxic strategies may be a reasonable and potentially more physiologic alternative. Although some individual trials have reported differences in biomarkers of oxidative stress or inflammation, the available randomized data do not indicate that these translate into measurable differences in early postoperative outcomes at the bedside.28–30
Oxygen delivery (DO2) is a key determinant of tissue oxygenation during CPB and is primarily regulated by pump flow and arterial oxygen content, which depend on hematocrit and arterial oxygen saturation. 31 In patients with chronic cyanosis, longstanding hematological adaptation may partially compensate for lower arterial oxygen saturation, 32 supporting the rationale for normoxic perfusion strategies when DO2 is adequately maintained. Available pediatric studies, although not specifically focused on cyanotic congenital heart disease, consistently associate indexed DO2 thresholds in the range of approximately 340 to 360 mL/min/m2 with a reduced risk of acute kidney injury in congenital heart surgery.33,34 Consequently, maintaining DO2 above this range may define a safe perfusion zone during bypass. However, the absence of studies specifically addressing DO2 thresholds in cyanotic populations represents an important limitation.
The sensitivity analyses provide additional insight into the variability observed across studies. For mechanical ventilation time, exclusion of the trial by Babu et al markedly reduced heterogeneity, raising the possibility that local ventilatory protocols, extubation criteria, or specific patient characteristics may have driven some of the between-study differences. 21 Similarly, for CPB duration and aortic cross-clamp time, removal of the Oxic-2 trial substantially decreased heterogeneity, suggesting that differences in operative conduct or oxygenation targets in that study may have influenced the pooled estimates. Even when these outlier trials were excluded, however, the overall pattern remained neutral, without consistent evidence of superiority of either normoxia or hyperoxia.35,36
A strength of this meta-analysis is the exclusive inclusion of RCTs specifically enrolling children with cyanotic congenital heart disease, a group in whom the question of oxygenation strategy is particularly relevant. Tetralogy of Fallot was the most frequent diagnosis, reflecting real-world practice, and the inclusion of both neonates and infants mirrors the age spectrum typically considered for early corrective surgery.37,38
Several limitations should be acknowledged. First, the overall sample size and, in particular, the number of clinical events were modest, leading to wide confidence intervals and limited power to detect small or moderate differences between strategies, especially for rare endpoints such as mortality, neurological complications, and cardiac arrest. Second, definitions and monitoring of “normoxia” and “hyperoxia” varied across trials, relying on different combinations of FiO2 settings, peripheral oxygen saturation, and PaO2 targets. This lack of standardization may have attenuated true differences between groups and contributed to residual heterogeneity. Third, perioperative and intensive care protocols, such as ventilator weaning criteria, ICU discharge policies, and inotropic weaning, were not uniform among centers and directly influenced time-based outcomes. Fourth, our analysis was based on study-level aggregated data, precluding detailed exploration of high-risk subgroups, more refined dose-response relationships between oxygen levels and outcomes, and potential interactions between age, underlying anatomy, and oxygenation strategy.
Finally, although we applied predefined inclusion criteria and conducted sensitivity analyses, residual bias and unmeasured confounders cannot be entirely excluded. In particular, variations in the conduct of perfusion across the included studies may have influenced the observed outcomes and should be carefully considered when interpreting the results. In this context, we emphasize the need for future larger, multicenter, RCTs with standardized perfusion protocols, extending beyond oxygenation parameters alone, to enhance the generalizability of the evidence.
Conclusions
In this meta-analysis of 5 RCTs including children with cyanotic congenital heart disease undergoing surgery with CPB, normoxic, and hyperoxic oxygenation strategies were not associated with statistically significant differences in all-cause mortality, postoperative recovery, operative parameters, or major safety outcomes.
Furthermore, future larger, multicenter, RCTs with standardized perfusion protocols, extending beyond oxygenation parameters alone, are warranted to improve the consistency and generalizability of the evidence.
Supplemental Material
sj-docx-1-pch-10.1177_21501351261449205 - Supplemental material for Perioperative Normoxia Versus Hyperoxia in Cyanotic Congenital Heart Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-pch-10.1177_21501351261449205 for Perioperative Normoxia Versus Hyperoxia in Cyanotic Congenital Heart Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials by Leonardo Braga Gonçalves, Lucas Monteiro Delgado, Rachid Eduardo Noleto da Nobrega Oliveira, Erlon de Ávila Carvalho, Madeline Loftin and Davi Freitas Tenório in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Author Contributions
RENNO and LBG: Conceptualization.
LBG and LMD: Methodology and literature search.
LBG, LMD, and RENNO: Data extraction and formal analysis.
RENNO, LBG, LMD, and EAC: Writing—original draft.
LBG, LMD, RENNO, EAC, ML, and DFT: Writing—review and editing.
ML and DFT: Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed in this study are derived from previously published articles included in the systematic review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.