
Abstract
Background
Anomalous aortic origin of the right coronary artery (AAORCA) with an intramural course is a rare but potentially life-threatening anomaly due to its association with exertional ischemia and sudden cardiac death. Surgical correction aims to eliminate the ischemic mechanism. This study reports a single-center experience with adult patients who underwent right coronary artery (RCA) reimplantation for AAORCA.
Methods
A retrospective review was conducted of symptomatic adult patients with AAORCA who underwent RCA reimplantation between June 2017 and August 2024. Baseline clinical features, perioperative outcomes, and follow-up data were assessed.
Results
Forty patients (85% [34/40] male; median age 44 years) were included. The most common presenting symptom was exertional chest pain (82.5%, [33/40]), followed by dyspnea (45%, [18/40]) and syncope or presyncope (30%, [12/40]). Coronary computed tomography angiography (CCTA) was performed to diagnose the high-risk coronary features. All patients underwent RCA reimplantation into the right sinus of Valsalva. One patient also received a saphenous-vein graft to the distal-RCA. There was no in-hospital or follow-up mortality. At a mean follow-up of 30.3 ± 20.5 months, 8/40 patients (20%) reported recurrent symptoms, including chest pain (10%, [4/40]), dyspnea on exertion (5%, [2/40]), and palpitation (5%, [2/40]). Surveillance CCTA or invasive angiography performed in 14 patients, including 8 symptomatic patients, confirmed the widely patent RCA with no ostial stenosis or kinking. Post operative exercise testing in all these patients was negative.
Conclusions
In adults with AAORCA and an intramural or interarterial course; reimplantation of the RCA into the right-sinus of Valsalva achieves excellent early- to midterm outcomes, with low mortality, symptom resolution, and durable coronary patency.
Keywords
Introduction
Anomalous aortic origin of the right coronary artery (AAORCA) from the left sinus of the aortic root is a rare congenital anomaly, occurring in 0.1% to 0.3% of the general population. 1 This anomaly alters both the origin and course of the right coronary artery (RCA) and is often detected incidentally in asymptomatic individuals or during the evaluation of chest pain and other cardiovascular symptoms using cardiac imaging modalities such as echocardiography, coronary computed tomography angiography (CCTA), cardiac magnetic resonance imaging (MRI), or coronary angiography. 2
Although most patients with AAORCA are asymptomatic, characteristics such as intramural course, slit-like opening, and acute angle of the RCA have been associated with increased risks of sudden cardiac death (SCD), myocardial ischemia, syncope, and arrhythmias, especially in young competitive athletes. 3 Other anatomic variants of AAORCA, including prepulmonic, subpulmonic, retroaortic, and retrocardiac courses, have also been described; however, these generally carry a lower risk of adverse outcomes. 4
Surgical management has been advocated for high-risk anatomical variants, with several operative strategies described in the literature. These include unroofing of the intramural segment, translocation and reimplantation of the anomalous RCA, coronary osteoplasty, and coronary artery bypass grafting (CABG). 5 Coronary unroofing in many institutions has been the surgical procedure of choice, followed by CABG. However, these techniques have several limitations, which prompted the emergence of the RCA translocation and reimplantation technique.
Translocation and reimplantation involves the relocation of the anomalous RCA onto the right coronary sinus, while CABG uses arterial or venous conduits to bypass the anomalous RCA, often with the ligation of the native RCA. Case reports and small series have demonstrated the safety and efficacy of these approaches, with favorable short- and midterm outcomes. 6 However, no randomized clinical trials or large observational studies have established the superiority of one technique over another, reflecting the rarity of the condition.5–7
Despite increasing recognition of AAORCA in contemporary imaging practice, data on surgical outcomes in adult patients remain limited, as most published cohorts are either pediatric or mixed-age populations. Right coronary artery translocation was originally advocated for cases with an interarterial course with a short intramural component to avoid compression of the proximal RCA between the aorta and pulmonary trunk. However, RCA translocation, although technically challenging, appears to be an appropriate surgical strategy for most anatomical variations. The outcome and durability of RCA translocation in adult patients, who differ from pediatric patients in their vessel compliance, atherosclerotic risk, and hemodynamic conditions, remains less well characterized. In this study, we report the clinical profiles, surgical details, and early- to midterm outcomes of adult patients with AAORCA who underwent RCA reimplantation at our center.
Methods
Study Design and Setting
This was a single-center retrospective review of patients operated for AAORCA at a tertiary cardiac center between June 2017 and August 2024. This study was reviewed and approved by the Institutional Review Board (IRB# 27-6/2024). All cases were performed by the senior author at Queen Alia Heart Institute, Jordanian Royal Medical Services. Owing to the retrospective design and the use of de-identified clinical data, the requirement for individual patient consent was waived in accordance with institutional policy and the Declaration of Helsinki.
Patient Selection and Data Collection
In our institute, patients who present with cardiac symptoms (chest pain, arrhythmias, syncope, dyspnea, myocardial infarction, or SCD) are initially investigated with transthoracic echocardiography (TTE) to evaluate for cardiac function, cardiac valves, regional wall motion abnormality, and coronaries. Patients with suspicion of coronary artery disease or anomalous origin of coronary artery underwent CCTA and/or coronary angiography to confirm the diagnosis to evaluate the coronary anatomy and coronary artery disease (Figure 1). Clinical, electrocardiographic, and echocardiographic characteristics were recorded. Data were collected for preoperative CCTA and invasive angiography if performed. All imaging studies were reviewed by a cardiologist and cardiovascular radiologist to confirm the anomalous origin, trajectory, and ostial morphology and to exclude obstructive coronary disease prior to operative planning. Data were collected for the operative details, hospital course, and follow-up from the medical records.
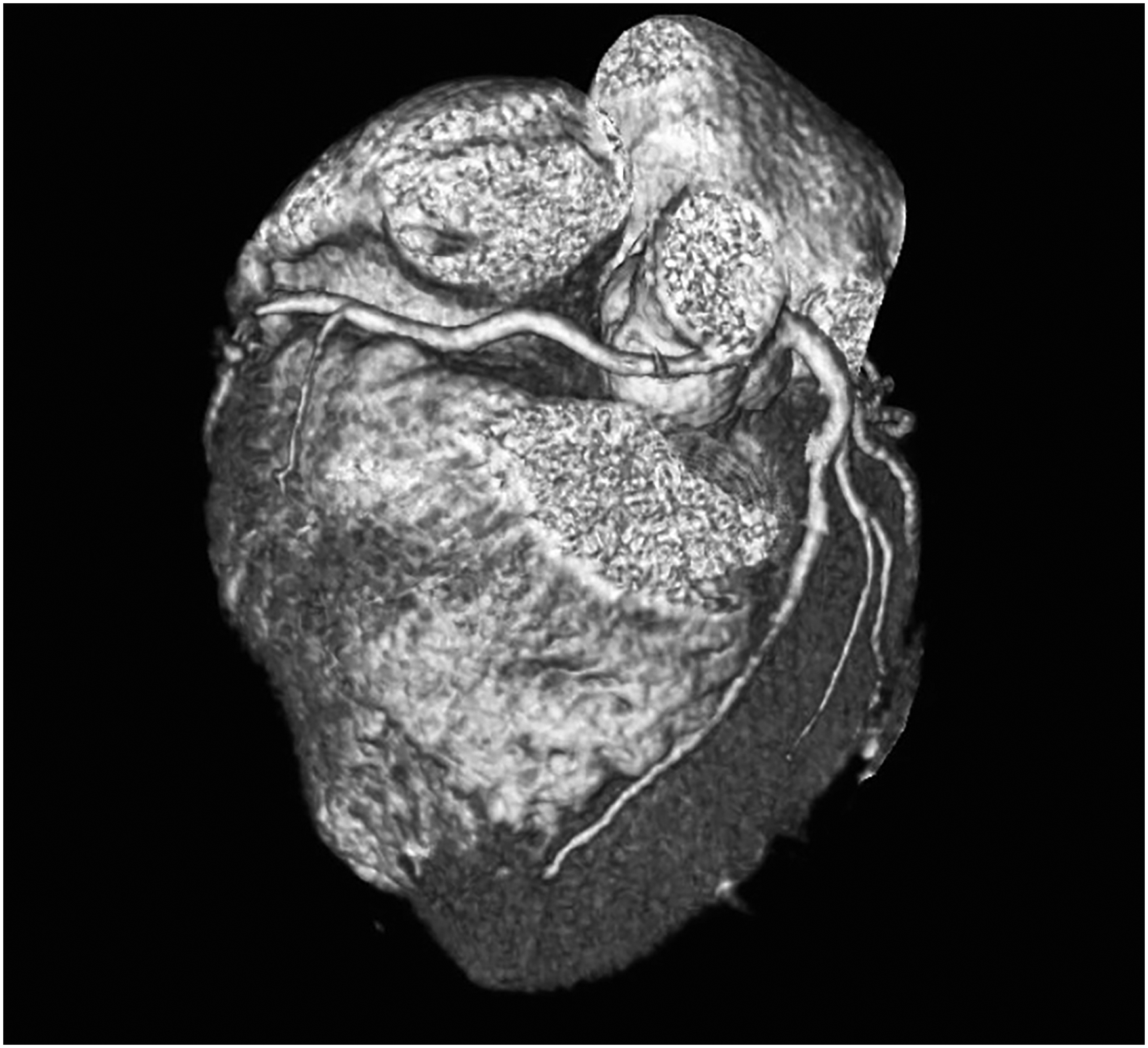
Preoperative coronary computed tomography angiography demonstrating anomalous origin of the right coronary artery from the left coronary sinus with an interarterial course.
Surgical Technique
All procedures were performed through a median sternotomy under standard cardiopulmonary bypass (CPB) with ascending aortic and right atrial cannulation. Myocardial protection was achieved using antegrade cold blood cardioplegia. After cardioplegic arrest, the anomalous RCA was identified and mobilized circumferentially for a length of 1.5 to 2.0 cm from its takeoff from its intramural portion to achieve adequate mobilization. Then we selected the site of reimplantation, either high in the right coronary sinus of the aortic root or on the anterior surface of the proximal ascending aorta to avoid undue kinking of the RCA. We always mark the superior aspect of the RCA to maintain proper orientation and avoid rotation before implantation. At this time, we transected the most proximal aspect of the RCA as it emerges from the aortic root and the residual stump was oversewn with 6-0 Prolene. We always make a small transverse aortotomy 2 cm above the sinotubular junction to prevent inadvertent injury to the aortic cusp during the creation of the neo-ostium. A neo-ostium was then created with a 4-mm aortic punch. The proximal end of the RCA stump was spatulated for a length of 7 to 8 mm to widen the anastomosis and provide a smooth, wide-angle takeoff from the aorta for hemodynamic optimization. This anastomosis was completed with 7-0 Prolene suture using a parachute technique, ensuring a wide, tension-free, and nonkinked anastomosis (Figure 2). We always pay attention to positioning the heel of the spatulated RCA toward the atrioventricular groove to prevent kinking. Subsequently, the aortotomy was closed in 2 layers using 4-0 Prolene suture. We always check the RCA anastomosis and its lie by giving an injection of warm cardioplegia in the aortic root. Finally, the heart was deaired, the aortic cross-clamp removed, and CPB was discontinued in a standard fashion. After weaning from CPB, transesophageal echocardiography was performed to check the biventricular function and flow in both the coronary ostia. The RCA flow dynamics was also confirmed with Doppler ultrasound. One patient developed ventricular tachycardia after being weaned from CPB that prompted further evaluation and revealed a significant distal RCA lesion not detected on preoperative CCTA. Since this segment was farther away from the reimplantation anastomosis, a saphenous vein graft was placed distal to the site of lesion to ensure adequate distal perfusion. No patient had any significant electrocardiogram abnormality.

Postoperative coronary computed tomography angiography demonstrating successful reimplantation of the right coronary artery into the appropriate sinus of Valsalva.
Statistical Analysis
Descriptive statistics were used to summarize the study data. Continuous variables were expressed as mean ± standard deviation or median with interquartile range (IQR), depending on the data distribution. Categorical variables were presented as frequencies and percentages. All analyses were performed using R software (version 4.3.2; R Foundation for Statistical Computing).
Results
During the study period, 40 symptomatic patients were referred for the surgical management of AAORCA and were included in the study. The presenting symptoms were chest pain on exertion (n = 33/40, 82.5%), dyspnea on exertion (n = 18/40, 45.0%), syncope or presyncope during exertion (n = 12/40, 30.0%), and palpitations (n = 2/40, 5.0%). Eighteen of 40 patients (45%) presented with isolated symptoms while 22/40 patients (55%) had 2 or more symptoms at presentation. Median age of the patients was 44 years (IQR: 34-48) and 34/40 patients (85%) were male. Fifteen of 40 patients (37.5%) had a history of hypertension, 17/40 patients (42.5%) were obese, and 14/40 patients (35%) were active or reformed smokers. Twelve of 40 patients (30%) had a family history of premature cardiovascular disease. On electrocardiography, Q-waves were observed in the inferior leads in one of 40 patients (2.5%). Initial diagnosis of AAORCA was made on TTE in all 40 patients (100%). Left ventricular ejection fraction (LVEF) was >55% in 39/40 patients (97.5%), and one patient had LVEF of 45%. Right ventricular function was normal in all the patients (Table 1). There were no associated intracardiac anomalies. Coronary computed tomography angiography revealed a slit-like coronary opening in 26/40 patients (65%), and a variable length of the intramural course of RCA in all 40 patients (100%). Twenty-one (52.5%) of 40 patients had an acute takeoff of the RCA from the left coronary sinus. One patient with LVEF of 45% had 50% to 60% obstruction in the distal RCA. Sixteen of 40 patients (40%) who were >40 years age underwent invasive coronary angiography to evaluate for coronary artery disease.
Patients Characteristics and Preoperative Course (n = 40).
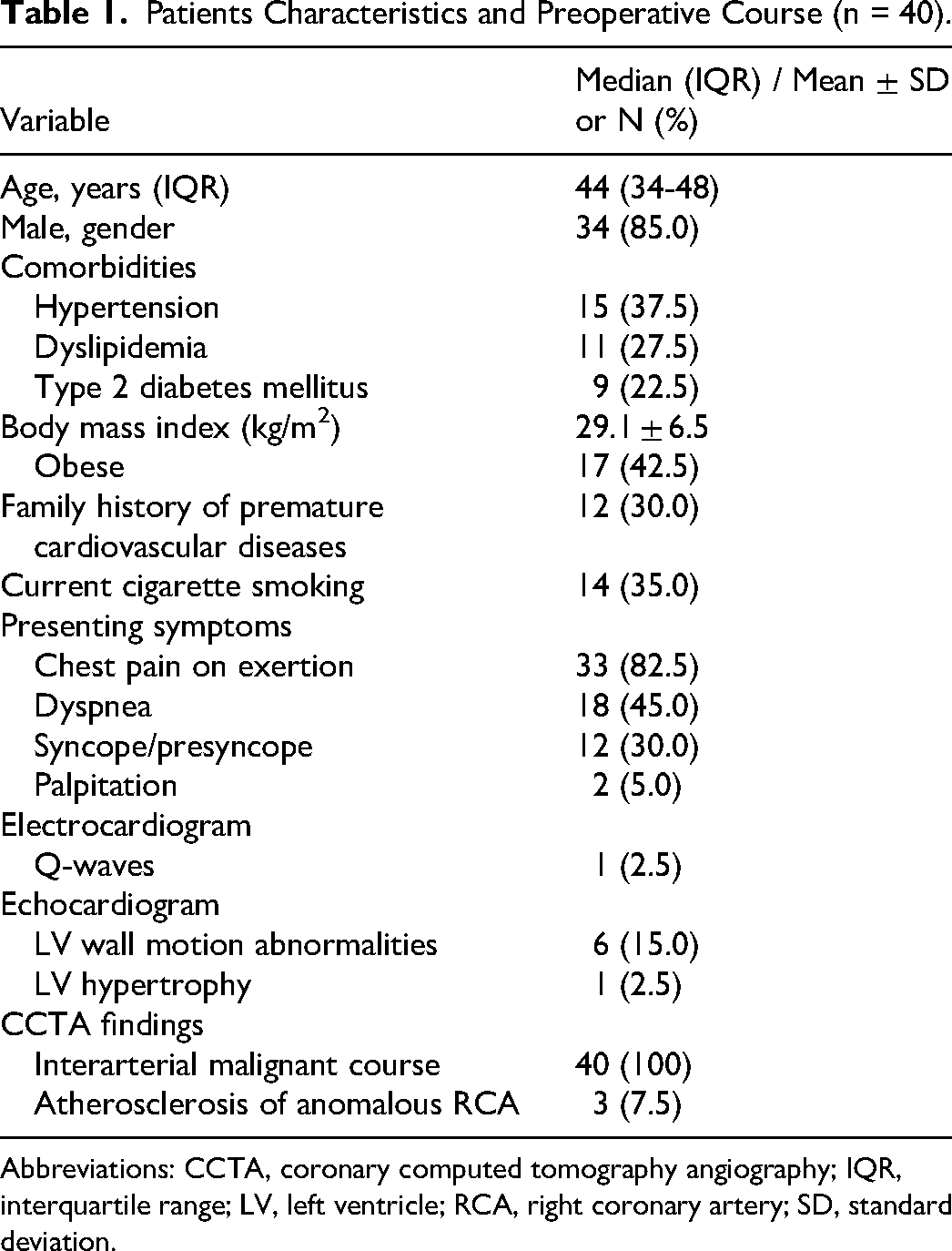
Abbreviations: CCTA, coronary computed tomography angiography; IQR, interquartile range; LV, left ventricle; RCA, right coronary artery; SD, standard deviation.
All the patients tolerated the surgery well, and there was no operative or in-hospital mortality. The median duration of intensive care unit stay was 2 days (IQR: 1-3 days), and hospital stay was 10 days (IQR: 7-13). Five of 40 patients (12.5%) developed atrial fibrillation and were successfully managed with medical therapy. No patient had ventricular arrhythmia. One of 40 patients (2.5%) experienced an embolic stroke that was treated conservatively with complete functional recovery (Table 2).
Operative and In-hospital Outcomes (n = 40).
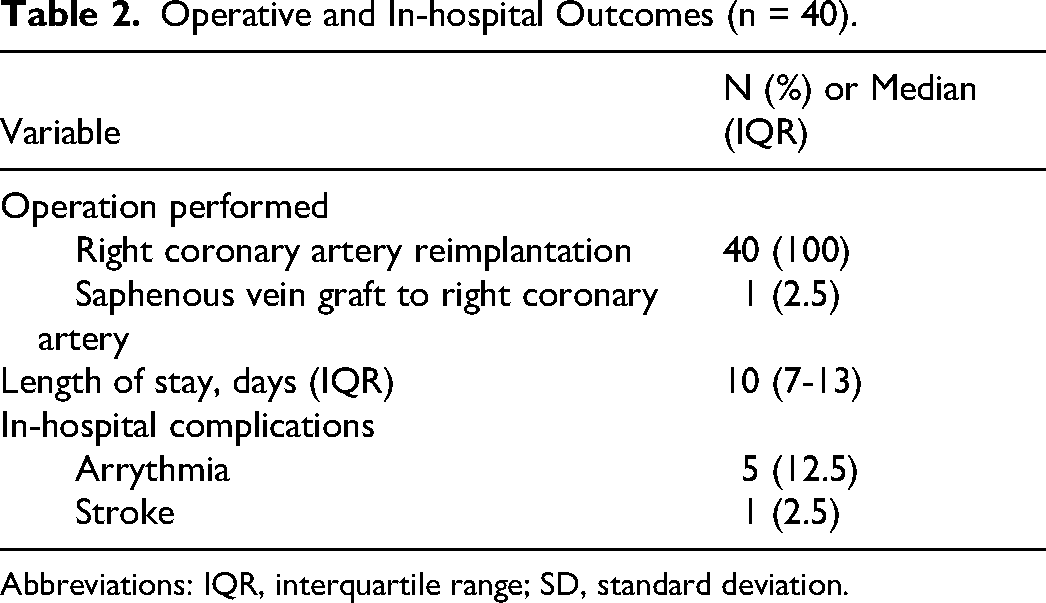
Abbreviations: IQR, interquartile range; SD, standard deviation.
Follow-up was complete (100%), and mean duration of follow-up was 30.3 ± 20.5 months. Nine of 40 patients (22.5%) were followed for more than 40 months, and there were no mortalities at last follow-up. All the patients were followed with clinical history, examination, and yearly TTE. All patients reverted to their active life and 22/40 patients (55%) were involved in active sports. Eight of 40 patients (20.0%) reported recurrent symptoms during follow-up, including chest pain (n = 4/40, 10%), dyspnea on exertion (n = 2/40, 5%), and palpitations (n = 2/40, 5%). Biventricular function on TTE remained preserved at their preoperative level in all patients. There were no regional wall motion abnormalities, and good flow was seen in both right and left coronary ostia. Exercise testing was performed in 6 patients with chest pain (4 patients) and exertional dyspnea (2 patients). Exercise testing was negative for inducible ischemia, and there was no exercise limitation. Surveillance CCTA was performed in 14/40 patients (35%), including 8/40 patients (20%) who developed symptoms during follow-up. Six of 40 patients (15%) underwent invasive coronary angiography for a suspicious lesion on CCTA. Investigations demonstrated a widely patent reimplanted RCA ostium with no evidence of kinking or narrowing. No patient had new pathology in the left or right coronary circulation. All patients with postoperative symptoms and negative studies responded well to reassurance and analgesics. Two patients with palpitation underwent ambulatory Holter monitoring and revealed no arrhythmia. Outcomes during follow-up are summarized in Table 3.
Intermediate-Term Follow-Up Results (n = 40).
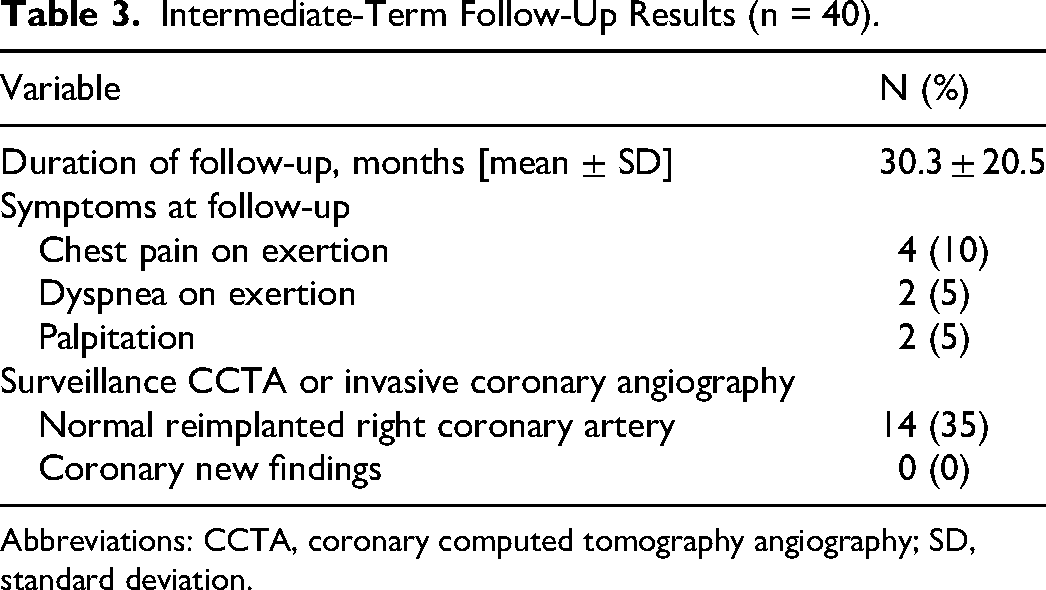
Abbreviations: CCTA, coronary computed tomography angiography; SD, standard deviation.
Discussion
Historically, patients with AAORCA and an interarterial course were considered to be a high risk anatomical subgroup. The interarterial course of the RCA can lead to a scissor-like interruption of the coronary blood flow during exertion. This was considered to be the main driver of ischemia. 7 However, growing evidence proves that the low-pressure pulmonary artery cannot develop a substantial counterforce to occlude the anomalous RCA. Recent studies have proposed a 2-tier concept of coronary ischemia based on their hemodynamic relevance. As per the 2-tier concept, a slit-like coronary ostium and the proximal narrowing of the coronary artery are the fixed components that are responsible for the static reduction in the cross-sectional area of the RCA while the acute take-off angle and the intramural course are the dynamic components responsible for coronary ischemia. 8
With the evolution of our understanding of the development of coronary ischemia in patients with AAORCA, it is now recommended that only symptomatic patients (ischemic chest pain, syncope secondary to ventricular arrhythmia, or history of aborted SCD) with high-risk characteristics need surgical correction. Management strategy for asymptomatic patients who have negative stress test (stress echocardiography or stress nuclear perfusion test) remains controversial. There is still ongoing debate regarding the management of asymptomatic competitive athletes as to whether these patients should be allowed to participate in competitive sports after careful counseling, or if surgery should be offered as the risk of surgery is very low and SCDs have been reported even in asymptomatic patients. 4 The goal of multimodality diagnostic imaging is to detect the high-risk anatomic features and myocardial ischemia, as well as to provide information for possible myocardial fibrosis/scar, which may be a substrate for ventricular tachyarrhythmias. Echocardiography is usually the first investigation that gives a clue about the presence of AAORCA. In suspected patients, CCTA is the investigative modality of choice that not only delineates the presence of high-risk features but also detects the presence of associated coronary artery disease. 1 It is recommended that patients with high-risk features should undergo an invasive evaluation with coronary angiography and intravascular ultrasound and fractional flow reserve testing under a dobutamine and volume challenge to delineate the hemodynamic relevance of the AAORCA. In our series, all patients underwent CCTA to evaluate for high-risk features. However, we performed invasive coronary angiography only sparingly when symptomatic patients did not show the presence of high-risk features on CCTA or the patient was >40 years age. In our series, only 40% (16/40) of patients underwent invasive coronary angiography. With our improved experience and good outcomes, we now prefer to operate on any symptomatic patient with AAORCA who has high-risk features in CCTA.
Among available surgical approaches, coronary unroofing and coronary reimplantation are the most commonly performed procedures. As per a recent study by the Congenital Heart Surgeons' Society, coronary unroofing is the most widely used surgical technique. 9 Coronary unroofing addresses the anatomic high-risk feature such as slit-like ostium and the intramural course. However, an acute take-off angle is usually only partially corrected, and there may be residual coronary stenosis between the unroofed segment and the distal coronary artery, especially in patients with a short segment intramural course.10,11 Further, in cases where the AAORCA traverses below or next to the commissure, it may be difficult to unroof the coronary artery along its entire length without running the risk of aortic regurgitation.
Coronary artery bypass grafting is another technique to manage AAORCA that addresses all anatomic high-risk features without the manipulation of the aortic valve. However, there is an increased risk of coronary bypass graft failure due to the competitive flow through the native anomalous segment. Hence, the proximal ligation of the anomalous coronary artery is a crucial step for CABG patency.8,10,12 However, this results in complete dependence of the anomalous supplied myocardium on a graft with uncertain durability, especially in young patients. 12 Therefore, CABG should be reserved only for older patients and patients with concomitant, significant coronary artery disease within the anomalous vessel.
Coronary translocation or reimplantation of the AAORCA in the right sinus of Valsalva is a suitable method in patients with either a short or absent intramural course, where the coronary unroofing technique is limited.10,13,14 For coronary translocation, the proximal coronary artery is carefully mobilized from the epicardial fat. Then RCA can be either harvested as an aortic button and reimplanted in the right sinus of Valsalva using an aortic punch or a medial trap-door technique. Then, the aortic button site is repaired with a small prosthetic patch.8,10 Alternatively, the anomalous RCA can be harvested by transecting it just as it emerges from the aortic wall. The proximal stump is then overseen and the coronary artery reimplanted by an end-to-side anastomosis as described previously. 15 Coronary transection and translocation correct the anomalous intramural course, eliminate the slit-like orifice, and correct the tangential takeoff. Coronary translocation is technically challenging, involves extensive coronary artery dissection and manipulation, and is associated with complications; for example, neo-ostial obstruction, kinking, and flow disruption. In addition, long-term results of circumferential anastomosis remain unknown.8,10,16
Various studies have reported encouraging results of RCA reimplantation. A retrospective series by Cubero et al 17 reported 13 patients (mean age 39 years) with AAORCA who underwent reimplantation. The authors reported that there was no operative mortality. All patients were asymptomatic at a mean follow-up of 65 months and returned to exercise without limitations. Another multi-institutional retrospective series from Australia reported the medium-term outcome of reimplantation for AAORCA in 16 patients (age 17-70 years). There was no operative mortality. Reimplantation was successful in 15 of 16 (94%) patients. All successfully repaired patients were asymptomatic during follow-up. Follow-up CCTA performed in two-thirds of patients showed no stenosis, kinking, or compression. No patients required additional interventions attributable to the RCA. 14 Smaller adult reports—including Izumi et al (2 adults) and Saleem et al (2 young adults/athletes) also demonstrated complete symptom resolution and durable patency of the reimplanted RCA.15,18 Across all adult-predominant series, there has been no procedure-related mortality and no reported cases of ostial restenosis or proximal anastomotic failure.15–18
Pediatric and institutional mixed-age experiences also support the long-term durability of reimplantation. Mainwaring et al, in a broader institutional experience dominated by younger patients, reported preserved valve function and sustained RCA patency following reimplantation, reinforcing the structural soundness of the anatomical relocation. 19
To our knowledge, this is the largest reported series of RCA reimplantation in adults with high-risk AAORCA. Our series is also the largest single-center experience of RCA reimplantation in adults. Our findings reinforce the findings from previously published series and case reports and reiterate the durability and physiologic soundness of reimplantation in anatomically high-risk AAORCA patients at early- to midterm follow-up. In the absence of follow-up mortality, persistent ostial patency on follow-up imaging, and sustained symptom resolution, we believe that reimplantation of the RCA to its native sinus of Valsalva effectively eliminated the ischemic mechanism. However, we cannot confirm our claim in the absence of stress test.
Our study has several limitations inherent to its retrospective design, small sample size, and single-center experience. We also did not perform preoperative functional testing, including cardiac magnetic resonance imaging, fractional flow reserve, intravascular ultrasound, or stress testing in any patient. Further, in the absence of a standardized postoperative imaging protocol, silent anatomical changes in asymptomatic patients cannot be entirely excluded. Although ours is a dedicated adult cohort, results are limited to early- to midterm outcomes. Nevertheless, the present cohort reflects the real-world surgical population most affected by symptom-producing AAORCA, adults with malignant anatomy, and provides meaningful anatomic and physiologic follow-up. We propose larger multicentric registries including adults with long-term follow-up to strengthen the available evidence.
Conclusion
Anomalous RCA originating from the left coronary sinus is a rare but, potentially life-threatening anomaly. In symptomatic adults with AAORCA and an intramural or interarterial course, reimplantation of the RCA into the right sinus of Valsalva achieves excellent early- to midterm outcomes, with low mortality, symptom resolution, and durable coronary patency. This technique, although technically challenging, effectively addresses both fixed and dynamic abnormalities, including slit-like ostium, acute take-off angle, and intramural course. Our results reinforce that RCA implantation is also an available strategy with reliable results at early- to midterm follow-up.
Footnotes
Abbreviations
Authors’ Note
Use of Large Language Mode: The authors stated that no large language models were used in the preparation of this manuscript.
Author Contributions
Dina Sabha contributed to data collection, data analysis, and drafting. Mohammad Alomari, Pankaj Garg, and Bahi Hyasat contributed to study design, data analysis, drafting, supervision, and final approval. Laith Hyasat contributed to data collection and literature review. Saif Yamin contributed to data analysis support and manuscript editing. Rana Alkirmeen contributed to imaging review and interpretation. Ayman Hammoudeh contributed to surgical data verification and manuscript review. Pankaj Garg and Bahi Hyasat contributed to senior surgical oversight, critical revision, and final approval.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data may be made available from the corresponding author upon reasonable request.