
Abstract
Introduction
The Fontan procedure revolutionized single-ventricle palliation by enabling passive pulmonary blood flow. Fenestration, an atrial-level shunt, reduces early postoperative complications by decompressing the circuit but causes systemic desaturation. Despite early benefits, fenestration's long-term impact on survival and morbidity remains uncertain.
Methods
Reconstructed meta-analysis data from Kaplan-Meier curves of studies published up to December 25, 2024, following PRISMA guidelines was performed. Eligibility included Fontan patients with documented fenestration status and survival outcomes. Hazard ratios were estimated using Cox regression analysis with random effects, and proportional hazards violations were addressed with flexible parametric models.
Results
Eight studies met our eligibility criteria and included 2,827 unmatched patients and 804 matched Fontan patients included in the Kaplan-Meier curves (1308 + 402 with fenestration and 1519 + 402 without fenestration). Fenestration was associated with significantly lower overall survival (HR 1.58; p = 0.006) and had increased thromboembolism risk. Subgroup analysis showed lower survival among patients without documented active fenestration closure. Regression findings imply that the effectiveness of fenestration is influenced by baseline hemodynamic severity.
Conclusions
Fenestration in the Fontan procedure is associated with relatively lower long-term survival and increased thromboembolic risk. The benefits of fenestration may be greatest in patients with severe hemodynamic compromise, supporting a tailored rather than uniform approach to its application.
Introduction
The Fontan procedure, first described in 1968, revolutionized the surgical management of patients with functionally univentricular hearts.1,2 By directing systemic venous return to the pulmonary arteries, the Fontan circulation enables passive pulmonary blood flow in the absence of a subpulmonary ventricle. Modifications of the Fontan circulation, including the extracardiac conduit and lateral tunnel total cavopulmonary connections, have enhanced surgical outcomes and long-term palliation over the past decades. 3 One of these modifications that is still being debated is fenestration, a surgically created atrial-level communication permitting a right-to-left shunt. Fenestration aims to decompress the Fontan circuit, enhance preload, and augment early postoperative cardiac output, particularly in patients with elevated pulmonary vascular resistance or borderline ventricular function.4,5 However, these benefits come at the cost of systemic desaturation. 6
Studies have linked fenestration to reduced early postoperative morbidity, including lower rates of prolonged pleural effusion, shorter intensive care unit stays, and improved early hemodynamic tolerance.4,7 For instance, Lemler et al. demonstrated superior early outcomes in fenestrated Fontan patients in a randomized controlled trial, 4 while Fu et al. reported lower postoperative pulmonary artery pressures and zero early mortality in fenestrated patients. 8 These findings underscore fenestration's protective role in mitigating early Fontan failure. However, the long-term implications of fenestration remain controversial. Due to the cost of systemic desaturation, persistent fenestration is associated with chronic hypoxemia, paradoxical embolism, and venovenous collateral formation, which may impair quality of life and increase thromboembolic risk. 9
Institutional practices vary, with some centers routinely employing fenestration in high-risk patients, while others reserve it for selective or rescue use.10,11 This variability reflects ongoing uncertainty, as retrospective and prospective studies, including limited randomized trials, have yielded inconsistent findings on early and long-term outcomes. To clarify these uncertainties, we conducted a meta-analysis assessing long-term outcomes of fenestrated versus non-fenestrated Fontan procedures, evaluating their effects on survival, morbidity, and hemodynamic performance.
Material and Methods
The study protocol was registered under the PROSPERO (CRD42024627424) and The Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) criteria were followed. 12
Search Strategy and Study Selection
A comprehensive literature search was conducted in PubMed, Cochrane Library, ClinicalTrials, and Embase to identify relevant studies published between January 1990 and December 25, 2024. The search was limited to studies involving human subjects and articles published in English.
Following the initial search, duplicate records were removed. Titles and abstracts were screened to identify studies that met the inclusion criteria. Full-text articles were then retrieved and assessed for eligibility. Two authors conducted the selection process, and disagreements were resolved through consensus with a senior author. Only studies with full texts were considered for inclusion. Ethical approval was not required as this study was a systematic review and meta-analysis of previously published data.
Eligibility Criteria
Using the Population, Interventions, Comparison, Outcome, and Study (PICOS) strategy, studies were deemed eligible for inclusion if they focused on pediatric patients (<18 years of age) undergoing the Fontan procedure, with explicit documentation of fenestration status. Only studies that reported survival outcomes with longitudinal follow-up analysis, including Kaplan-Meier survival estimates, were considered. Eligible study designs encompassed multicenter cohort studies, observational analyses, case-control studies, and randomized controlled trials, provided they presented comprehensive baseline characteristics and outcome data relevant to the research objectives. The selection process adhered to rigorous methodological standards, excluding non-original research such as literature reviews, systematic reviews, editorials, commentaries, letters to the editor, and animal studies. In addition, studies lacking a comparative group or those failing to report survival outcomes pertinent to fenestration status were excluded.
Definition and Outcomes
We categorized pediatric patients undergoing the Fontan procedure into those who received fenestration (Fenestration group) and those who did not (Non-Fenestration group). Within the Fenestration group, a subgroup analysis was performed based on whether patients underwent active fenestration closure during follow-up, forming the Closed Fenestration group and the Open Fenestration group (no documented fenestration closure). The primary outcome was long-term survival. Secondary outcomes included arrhythmia, thromboembolism, and protein-losing enteropathy (PLE).
Data Extraction and Statistical Analysis
Data from the eligible selected studies were extracted, including demographics, comorbidities, risk factors, and outcomes for both groups. This process was carried out by two authors. Baseline continuous variables were summarized in mean (SD), whereas dichotomous variables were described in frequencies.
To reconstruct individual patient data (IPD), the curve approach was adopted. This method reconstructs IPD from published Kaplan–Meier survival curves.13,14 Specifically, the two-stage algorithm described by Liu et al. was employed, 15 utilizing the R package IPD from KM (version 0.1.10). In the first stage, time and survival probabilities were extracted from each treatment arm's (Fenestrated Fontan and Non-Fenestrated Fontan) Kaplan–Meier curves. In the second stage, these data were combined with the reported numbers at risk at specific time points to reconstruct IPD. The reconstructed datasets from all included studies were merged to create the final analysis dataset.
Cumulative incidences of outcomes in both treatment arms (Fenestrated Fontan and Non-Fenestrated Fontan) were visualized using Kaplan–Meier estimates, generated with the R packages survival (version 3.2.13). Hazard ratios (HRs) with 95% confidence intervals (CIs) for differences between treatment arms were estimated using Cox proportional hazards (Coxph) regression models. These models incorporated study-level random effects and were implemented via the R package Coxph (version 4.0.2). The proportional hazards assumption was assessed using the Grambsch and Therneau test and diagnostic plots based on Schoenfeld residuals. 16
If the proportional hazards assumption was violated, either by statistical testing or by visual inspection of the Kaplan–Meier curves, flexible parametric survival models were applied. These models, also known as Royston–Parmar models or generalized survival models, incorporate B-spline functions to flexibly model the baseline hazard and allow time-varying effects (Supplement).17,18 In this study, the baseline hazard was modeled with four degrees of freedom, including three internal knots and two boundary knots positioned at the quartiles of the event distribution. Analyses were performed using the R package rstpm2 (version 1.5.2). Interaction terms between treatment group and time were included to estimate time-varying hazard ratios with 95% confidence intervals throughout follow-up.
Restricted mean survival time (RMST) was calculated to assess lifetime differences between Fenestrated and Non-Fenestrated Fontan groups in terms of overall survival. 19 Restricted mean survival time quantifies the average survival time within a prespecified follow-up period, and corresponds to the area under the survival curve, capturing absolute survival differences between arms. The difference in RMST between groups reflects the estimated lifetime gain (if positive) or loss (if negative) attributable to fenestration.
Subgroup analyses were conducted based on fenestration status (open or closed). Mixed-effects meta-regression was performed using the DerSimonian and Laird estimator to explore potential modifiers, including age, sex, ventricular dominance, pulmonary pressures, atrioventricular valve regurgitation, pulmonary vascular resistance, conduit type, annual operative volumes, and the ratio of Fenestrated to Non-Fenestrated procedures. Meta-regression evaluated the relative effect of fenestration on survival (treatment effect modification), rather than the prognostic value of individual risk variables. Scatter plots were constructed to illustrate these relationships, with the size of each point proportional to the corresponding sample size.
Between-study heterogeneity was assessed using the I2 statistic, with heterogeneity categorized as low (I2 < 25%), moderate (I2 between 25% and 50%), or high (I2 > 50%). 20 Statistical significance was defined as a two-tailed p-value of less than 0.05. All statistical analyses and graphical representations were performed using R Studio (version 4.4.0).
Risk of Bias and Certainty of Evidence
Two investigators independently assessed the risk of bias using ROBINS-I (Risk of Bias in Non-Randomised Studies of Interventions), which was systematically used to assess included studies for risk of bias. 21 In cases of disagreement, senior author consensus was involved. The certainty of evidence was evaluated using the GRADEpro-GDT tool (Grading of Recommendations, Assessment, Development, and Evaluation) and categorized as very low, low, moderate, or high. 22
Results
Study Selection
A systematic search yielded 1,427 publications. After removing 764 duplicates, 611 studies were excluded based on title and abstract screening for relevance, inclusion criteria, and fenestration status. Full-text review was conducted for 52 studies, of which 21 were excluded due to unavailable time-to-event data and 23 for being secondary research or non-English publications. Ultimately, eight studies met the eligibility criteria for inclusion in the meta-analysis. The PRISMA flow diagram is presented in Figure 1. 23
PRISMA flow diagram of the meta-analysis. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis.
Patient and Study Demographics
Eight studies comprising 2,827 unmatched patients (1308 fenestrated, 1519 non-fenestrated) and one study with a 1:1 propensity score–matched cohort of 814 patients (407 per group) were included. Matching accounted for key clinical and surgical variables, including gender, age at Fontan operation, surgical era, presence of hypoplastic left heart syndrome, ventricular morphology, pre-Fontan atrioventricular valve regurgitation, pre-Fontan pulmonary artery pressure, Fontan modification type, isomerism, and concomitant atrioventricular valve or pulmonary artery surgery at the time of Fontan. The mean age was 5.5 years in the fenestrated group and 5.2 years in the non-fenestrated group. Women were almost equally represented in both groups (43% [653/1519] and 42% [549/1308]). Extracardiac conduit use was numerically higher in non-fenestrated patients (60% [911/1519] vs. 52% [680/1308]), while left ventricular dominance was comparable (40% [523/1308] vs. 42% [638/1519]). Hemodynamically, fenestrated patients had a numerically higher mean pulmonary artery pressure (13.1 mmHg vs. 12.0 mmHg) and pulmonary vascular resistance (1.8 WU/m2 vs. 1.5 WU/m2). The study characteristics and baseline demographics are summarized in Tables 1 and 2.
Characteristics of the Included Studies.
*For data on Mortality, aNo clear time frame, mMatched data, #Excluded atriopulmonary Fontan. iOne Patient excluded due to lack of follow-up.
Patient Demographics and Characteristics.
Excluded atriopulmonary Fontan; NA, Not available.
Overall Survival
A total of 2,709 patients who underwent the Fontan procedure were included in the survival analysis, with 1,280 (47%) receiving fenestration and 1,429 (53%) in the non-fenestrated group. Kaplan-Meier survival analysis (Figure 2a) demonstrated a significantly lower overall survival in the fenestrated group compared with the non-fenestrated cohort (HR 1.58, 95% CI [1.14–2.20]; p = 0.006 | I2 = 59%; p = 0.023), GRADE certainty: low (Table 3). Cox proportional hazards assumptions were met (Grambsch-Therneau test, p = 0.91) (Supplementary Figure 1).
(a) Kaplan Meier: Overall survival (20-year) unmatched cohort. (b) Kaplan Meier: Overall survival (20-year) matched cohort.
Assessment of Certainty of Evidence (GRADE) for Studies Comparing Fenestration Outcomes in Fontan.
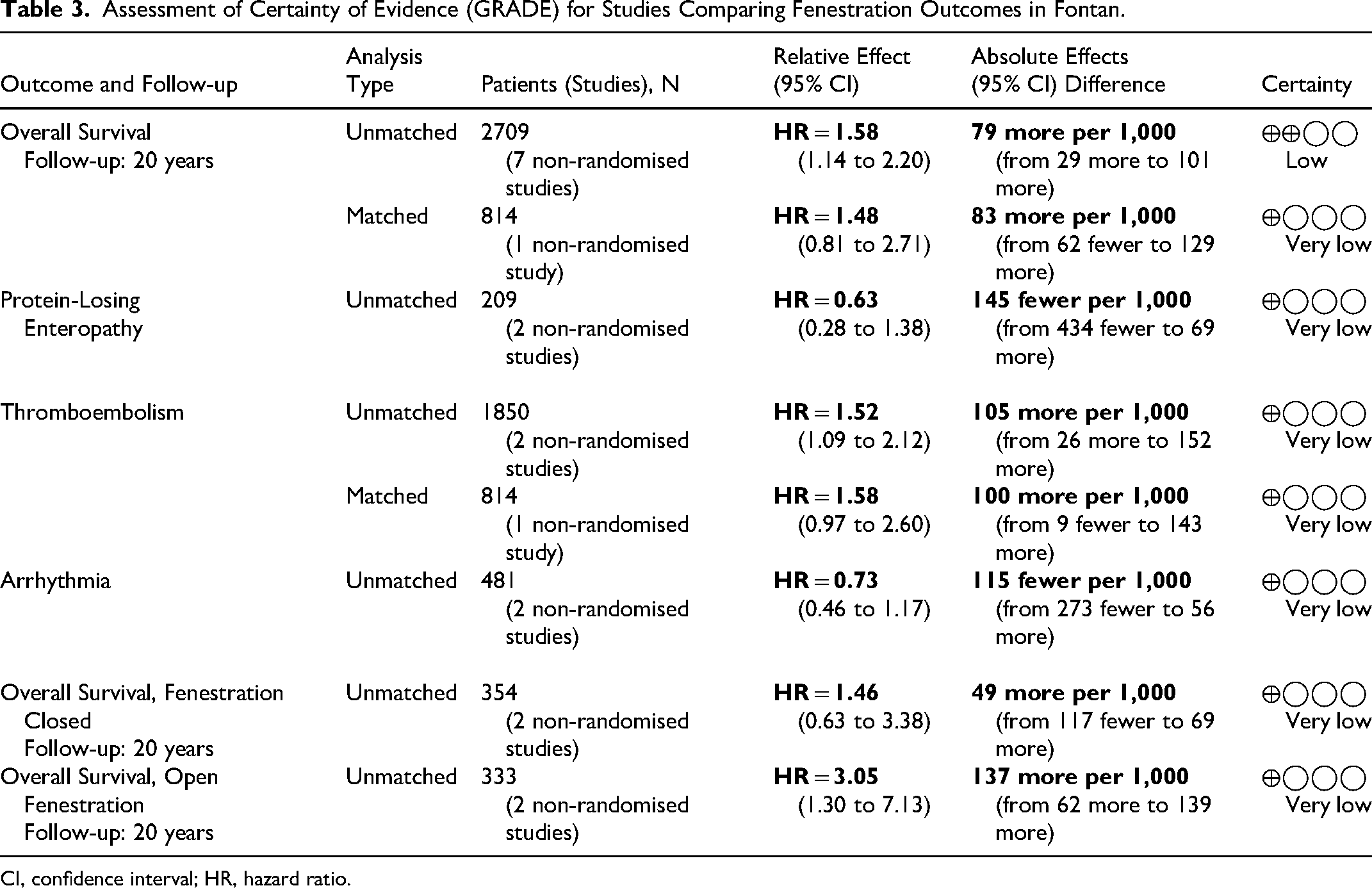
CI, confidence interval; HR, hazard ratio.
Restricted mean survival time analysis (Figure 3) demonstrated shorter observed survival times among patients who underwent fenestration. Patients in the fenestrated group experienced a significantly shorter overall survival by an average of 267 days (95% CI: 95–438 days) compared with the non-fenestrated cohort (p = 0.002).
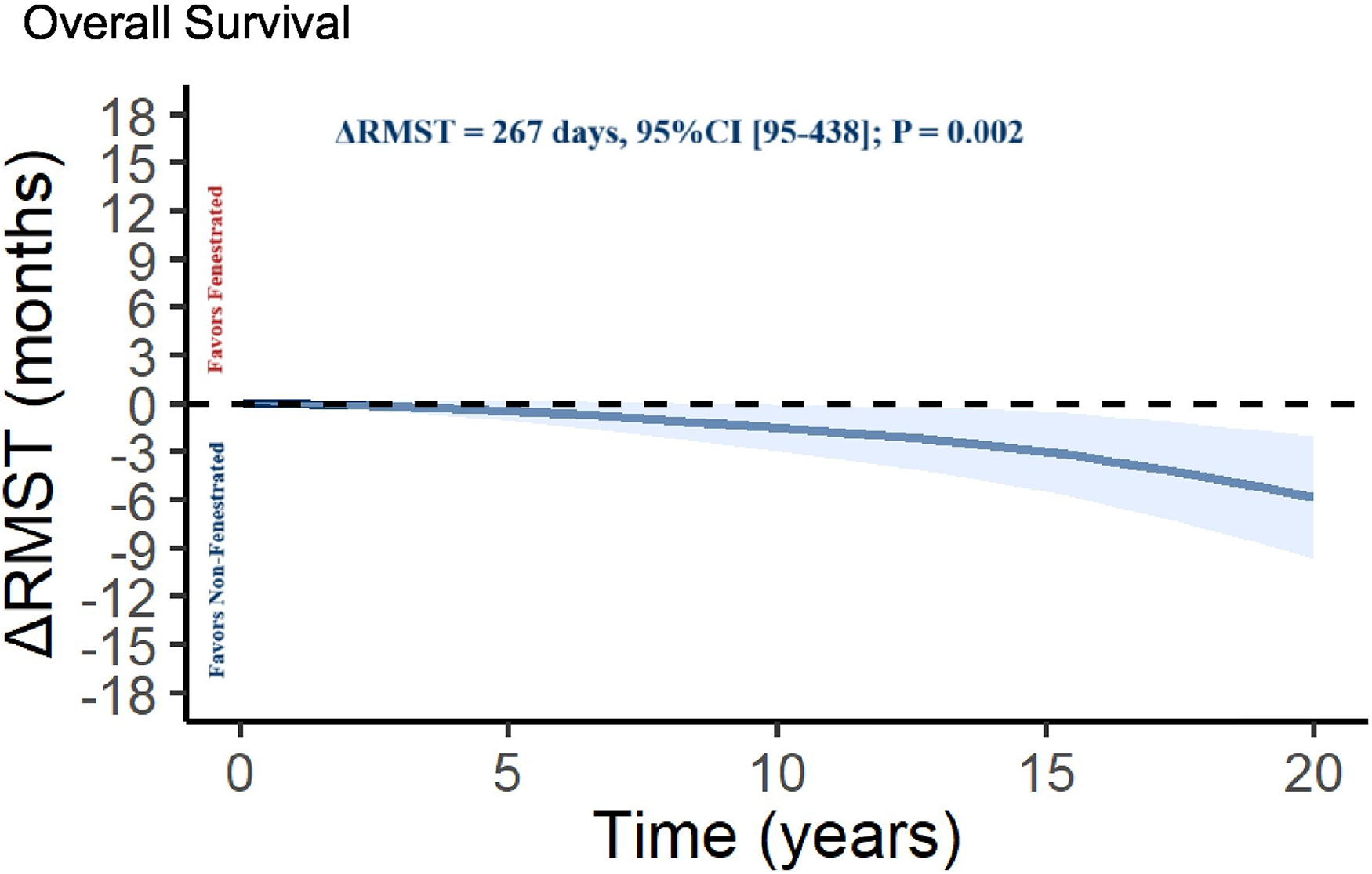
Restricted mean survival time (RMST) difference between fenestrated and non-fenestrated Fontan groups (shaded areas represent 95% confidence intervals; ΔRMST > 0 favors fenestration; ΔRMST < 0 favors non-fenestration. | RMST = Restricted mean survival time, representing the average event-free survival time over 20 years of follow-up. Estimates reflect differences in cumulative survival time between groups.).
Systemic Fontan Morbidities
Analyses of Fontan-associated morbidities, including PLE, thromboembolism, and arrhythmias, are depicted in Supplementary Figures 2–4. In the unmatched cohort, fenestration was associated with a significantly increased risk of thromboembolism compared with the non-fenestrated cohort (HR 1.52, 95% CI [1.09–2.12]; p = 0.01| I2 = 0%; p = 0.352) (Supplementary Figures 2a), GRADE certainty: low. In the matched cohort, a similar trend was observed but statistical significance was not achieved (HR 1.58, 95% CI [0.97-2.60]; p > 0.05) (Supplementary Figures 2b), GRADE certainty: very low. There was no statistically significant difference between the two groups in the incidence of arrhythmias (HR 0.73, 95% CI [0.46–1.17]; p = 0.20| I2 = 80%; p = 0.024) or PLE (HR 0.63, 95% CI [0.28–1.38]; p = 0.24| I2 = 84%; p = 0.013), GRADE certainty: very low.
Sensitivity Analysis
Figure 4 illustrates the pooled Kaplan-Meier survival curves analyzing overall survival based on fenestration closure status. Data from 424 patients who underwent the Fontan procedure were pooled from two studies, including 91 patients with fenestration closure, 70 without documented active fenestration closure, and 263 in the non-fenestrated group. Patients without documented active fenestration closure exhibited significantly lower survival compared with the non-fenestrated cohort (HR 3.05, 95% CI [1.30–7.13]; p = 0.01), GRADE certainty: very low. In contrast, no statistically significant difference in survival was observed between patients with fenestration closure and those without fenestration (HR 1.46, 95% CI [0.63–3.38]; p = 0.38), GRADE certainty: very low.
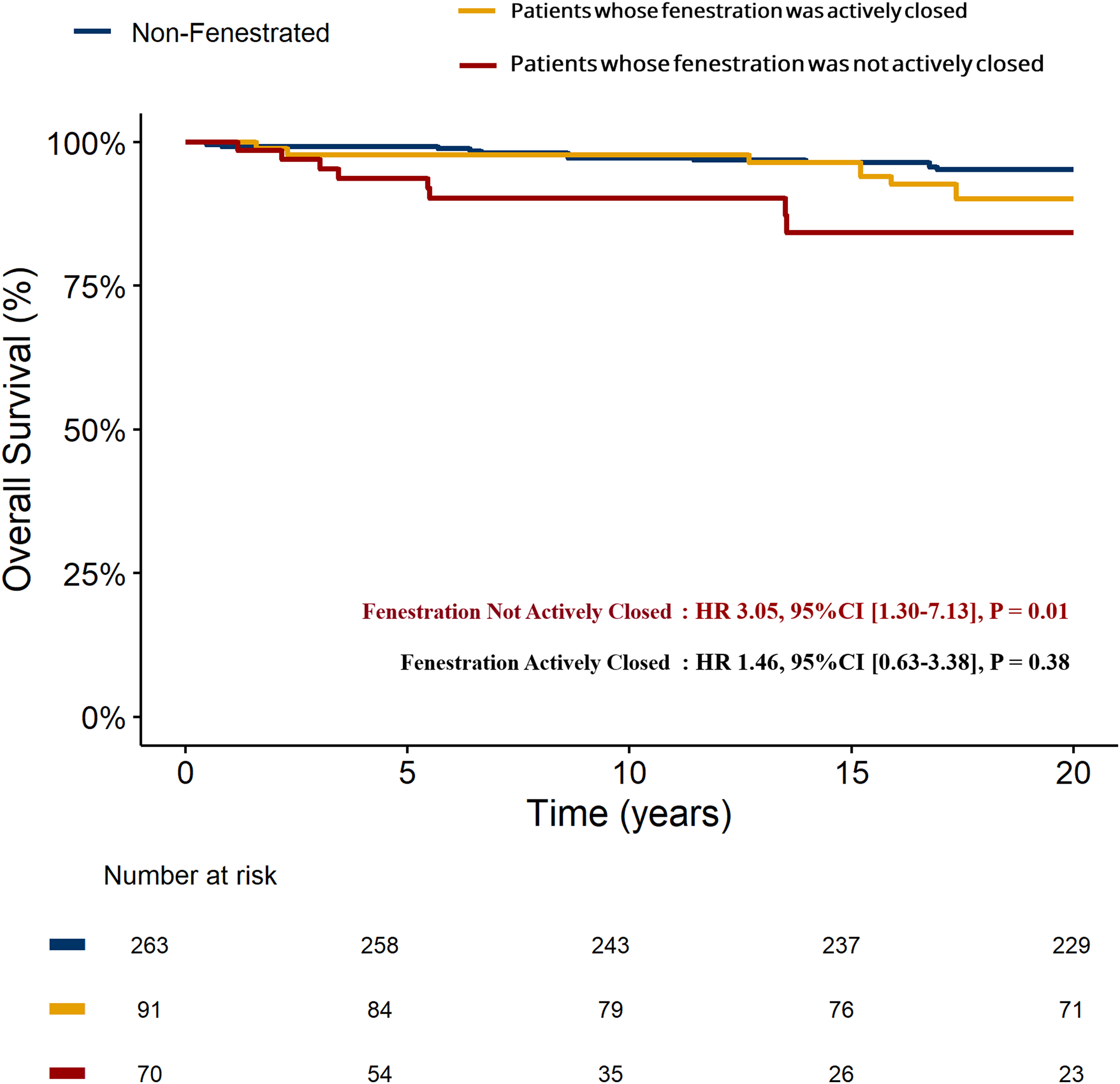
Kaplan–Meier survival analysis by fenestration status.
Meta Regression
Meta-regression identified statistically significant associations between overall survival following the Fontan procedure and two covariates: mean pulmonary artery pressure (PAP) and atrioventricular (AV) valve regurgitation (AVVR). Higher mean PAP (β = –0.526, p = 0.006) and greater prevalence of AVVR (β = –0.066, p = 0.028) demonstrated lower hazard ratios favoring fenestration, suggesting greater relative survival benefit among higher-risk Fontan patients (Supplementary Figure 5a&b).
Conversely, no statistically significant associations were found for age, female sex, left ventricular dominance, pulmonary vascular resistance, extracardiac conduit use, annual operative volume, annual fenestration volume, or the ratio of fenestration among Fontan procedures (Supplemental Table 1). This indicates that these variables did not significantly influence the pooled survival outcomes associated with fenestration.
Risk of Bias and Certainty of Evidence
The risk of bias assessment identified key methodological concerns. One study had a serious risk of confounding, and three had moderate risk. Four studies showed moderate selection bias, while all studies had a moderate risk due to missing data. Given the observational design of the included studies, the potential influence of confounding, selection bias, and missing data must be carefully accounted for when interpreting the findings (Supplementary Figure 6).
The certainty of evidence, evaluated using the Cochrane GRADEpro-GDT tool (Table 3), was determined to be low for the outcomes of overall survival. Additionally, the certainty of evidence for systemic Fontan morbidities, including PLE, arrhythmia, and thromboembolism, as well as overall survival based on fenestration status, was rated as very low. These assessments were primarily driven by the reliance on observational data and the inherent risk of bias within the included studies, highlighting the need for cautious interpretation of the findings.
Comment
The Fontan procedure remains the cornerstone surgical intervention for patients with single-ventricle physiology. 4 Since its inception, modifications such as fenestration, an intentional atrial-level communication, have been introduced to optimize hemodynamics and improve patient outcomes. While fenestration offers theoretical benefits, including reduced central venous pressure and enhanced preload, its long-term implications have been a subject of ongoing debate.
Fenestration has been associated with improved early postoperative outcomes. Studies have demonstrated that patients undergoing fenestrated Fontan procedures experience shorter hospital stays, reduced chest tube drainage, and fewer postoperative interventions compared with their non-fenestrated counterparts.4,7 These benefits are particularly pronounced in high-risk patients, where fenestration serves as a protective mechanism against elevated pulmonary vascular resistance and borderline ventricular function.
However, these early advantages come at the cost of systemic desaturation due to right-to-left shunting. Patients with fenestrated Fontan circuits often exhibit lower arterial oxygen saturation levels in the immediate postoperative period. 31 While this hypoxemia is generally well-tolerated, it underscores the trade-off between hemodynamic stability and oxygen delivery inherent in fenestrated designs.
Surgeon preference and technical feasibility also appear to influence the use of fenestration. In our included studies, the proportion of patients receiving an extracardiac conduit was numerically higher in the non-fenestrated group (60% [911/1519] vs. 52% [680/1308]). This may reflect the relative technical difficulty of creating a fenestration in the extracardiac conduit compared with the lateral tunnel. As highlighted in a recent commentary by D’Udekem, the ease of creating a fenestration in the lateral tunnel, a simple punch hole stands in contrast to the more complex and less reliable process required to fenestrate an extracardiac conduit on the beating heart, which can necessitate cross-clamping and additional dissection. 32 These practical considerations likely shape operative decisions more than philosophical differences in the belief about fenestration benefits.
In addition, the trend toward higher pulmonary artery pressures and pulmonary vascular resistance in fenestrated patients (13.1 mmHg vs. 12.0 mmHg and 1.8 vs. 1.5 WU/m2, respectively) suggests a pattern of selective fenestration in patients with elevated Fontan pressures. This reinforces the notion that fenestration is often employed not as a routine measure, but as a targeted strategy for patients deemed physiologically at higher risk.
Overall Survival
Our reconstructed time-to-event meta-analysis focusing on long-term outcomes demonstrated an association between fenestration and lower overall survival compared with the non-fenestrated cohort (HR 1.58, 95% CI [1.14–2.20]; p = 0.006). However, meta-regression demonstrated that the relative survival associated with fenestration was more favorable in studies including patients with greater hemodynamic compromise, specifically higher pulmonary artery pressures and more significant atrioventricular valve regurgitation. These findings suggest that fenestration may confer greater relative benefit when applied in the setting of adverse Fontan physiology, while offering limited additional advantage when applied broadly to lower-risk Fontan populations. Contrastingly, a propensity score–matched analysis using the Australia and New Zealand Fontan registry by Daley et al, reported no significant difference in long-term survival between fenestrated and non-fenestrated patients. 9 However, our synthesis integrating a broader evidence base through reconstructed time-to-event data revealed contrasting results. This divergence may stem from differences in methodology, length of follow-up, or variation in patient populations and institutional practices. It highlights how certain outcome disparities may not be fully captured by single datasets and underscores the complexity of assessing long-term outcomes in this heterogeneous patient population.
Systemic Fontan Morbidities
Thromboembolism is a recognized complication in patients with Fontan circulation, with fenestration potentially exacerbating this risk due to the presence of a right-to-left shunt. Our analysis indicated a significantly increased risk of thromboembolism in the fenestrated group (HR 1.52, 95% CI [1.09–2.12]; p = 0.01). This finding aligns with previous studies that have reported higher incidences of thromboembolic events in fenestrated patients. The mechanism is likely multifactorial, involving factors such as blood stasis, endothelial dysfunction, and paradoxical embolism through fenestration. Management strategies, including anticoagulation therapy, must be carefully considered in fenestrated patients to mitigate this risk. However, the optimal anticoagulation regimen remains undefined, necessitating further research in this area.33–35
Protein-losing enteropathy and arrhythmias are significant morbidities associated with the Fontan circulation. Our meta-analysis did not demonstrate a statistically significant difference in the incidence of PLE (HR 0.63, 95% CI [0.28–1.38]; p = 0.24) or arrhythmias (HR 0.73, 95% CI [0.46–1.17]; p = 0.20) between fenestrated and non-fenestrated groups. These findings suggest that fenestration may not substantially influence the development of these complications. However, the literature suggests that fenestration may offer transient protection against arrhythmias in the early postoperative phase. 31 Our findings, however, indicate that this effect diminishes over the long term, further supporting the notion that Fontan complications are multifactorial and evolve over time.
Fenestration Closure
The decision to close a fenestration postoperatively is often based on clinical judgment, balancing the benefits of improved oxygenation against the potential loss of hemodynamic stability. Our sensitivity analysis revealed that patients without documented active fenestration closure exhibited significantly lower survival compared with the non-fenestrated cohort (HR 3.05, 95% CI [1.30–7.13]; p = 0.01). Conversely, no statistically significant difference in survival was observed between patients who underwent fenestration closure and those without fenestration (HR 1.46, 95% CI [0.63–3.38]; p = 0.38). These findings suggest that non-closure of fenestration is associated with less favorable long-term outcomes, whereas timely closure may mitigate this risk. However, it is important to acknowledge that patients who do not undergo closure may represent a subgroup with morbid conditions or poor hemodynamic profiles, which may independently affect survival outcomes. However, the optimal timing and patient selection criteria for fenestration closure remain areas for further investigation.
Influence of Other Factors
Our meta-regression identified mean PAP and AVVR as variables associated with differences in survival between fenestrated and non-fenestrated patients. Studies including patients with higher pulmonary pressures and greater valve regurgitation demonstrated lower hazard ratios favoring fenestration, indicating that patients with more advanced hemodynamic compromise appeared to derive greater relative survival benefit when fenestration was used. In contrast, studies with lower pulmonary pressures and minimal valve regurgitation showed a reduced relative advantage. These findings reflect variation in treatment effect rather than suggesting a protective effect of elevated PAP or AVVR themselves. Other examined factors, including age, sex, ventricular morphology, pulmonary vascular resistance, and operative technique, did not show significant association with survival differences, underscoring the prominence of baseline hemodynamic status in shaping the benefit of fenestration.
These observations highlight the importance of individualized patient selection for fenestration at the time of Fontan completion. While early postoperative advantages of fenestration are well recognized, our results indicate that its long-term benefit may be most meaningful in patients with higher physiologic risk. Routine use in lower-risk patients may offer limited additional advantage. A tailored approach incorporating detailed preoperative hemodynamic assessment and contemporary imaging may help refine patient selection and maximize benefit. Continued evolution in perioperative evaluation and surgical planning will further support precision-based use of fenestration in modern Fontan practice.
Limitations
This meta-analysis has several limitations. The included studies were all retrospective and observational in nature, most conducted at single centers across North America, Europe, Asia, and Oceania. Despite the inclusion of propensity score–matched analyses, residual confounding and selection bias remain possible. Heterogeneity in patient selection, surgical technique, and institutional practices may limit the generalizability of our results. Additionally, this study relied on reconstructed time-to-event data derived from Kaplan–Meier survival curves published in the original articles. As such, we did not have access to individual-level clinical information, including imaging or catheterization data, and could not independently verify long-term fenestration patency in any cohort. Moreover, the absence of individual patient data constrained the depth of subgroup analyses and may have obscured important interactions. Inconsistent follow-up duration and incomplete outcome reporting further affect interpretability. While our reconstructed time-to-event analysis enhances methodological rigor, its conclusions are ultimately shaped by the retrospective, heterogeneous, and non-randomized nature of the underlying evidence.
Furthermore, this study employed advanced statistical techniques, including reconstructed time-to-event analyses and meta-regression modeling, which, while powerful, may be unfamiliar to many readers and require specialized expertise for interpretation. These methods allow estimation of survival patterns when raw patient-level data are unavailable but remain subject to assumptions inherent to curve reconstruction and regression modeling. Meta-regression was performed to explore study-level effect modification and sources of between-study heterogeneity, but it is intrinsically ecological in nature and should not be interpreted as reflecting individual-level associations. In addition, the number of studies contributing to specific covariates was limited (e.g., five studies reporting PAP and four reporting AVVR), which falls below the commonly cited threshold of approximately 10 studies per covariate and may increase the risk of overfitting or unstable estimates. Accordingly, meta-regression findings should be interpreted as exploratory and hypothesis-generating. Previously published meta-analyses have used similar methodologies.36,37 The complexity of these techniques introduces potential analytical uncertainty and reinforces the importance of cautious interpretation.
Conclusion
This meta-analysis, based on reconstructed time-to-event data, suggests that fenestration in the Fontan procedure may be associated with relatively lower long-term survival and increased thromboembolic risk in select patients. These risks appear more pronounced when fenestration is applied broadly across patient profiles. However, in patients with more severe baseline hemodynamic compromise, such as elevated PAP or AVVR, fenestration may confer a relative survival advantage. Patients who underwent fenestration closure demonstrated more favorable outcomes compared with their counterparts, emphasizing the need for individualized, hemodynamically guided fenestration and timely closure.
Supplemental Material
sj-docx-1-pch-10.1177_21501351261450496 - Supplemental material for Impact of Fenestration on Survival and Morbidity Following Fontan Surgery: A Time-to-Event Meta-Analysis of Reconstructed Kaplan–Meier Data
Supplemental material, sj-docx-1-pch-10.1177_21501351261450496 for Impact of Fenestration on Survival and Morbidity Following Fontan Surgery: A Time-to-Event Meta-Analysis of Reconstructed Kaplan–Meier Data by Rohit Ganduboina, Jef Van den Eynde, Xander Jacquemyn, Omar Abdel Kerim and Sandeep Sainathan in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Acknowledgments
None.
Author Contributions
Conceptualization: Rohit Ganduboina, Sandeep Sainathan; Methodology: Rohit Ganduboina, Sandeep Sainathan; Validation: Rohit Ganduboina, Sandeep Sainathan; Formal analysis, Investigation: Rohit Ganduboina; Data curation: Rohit Ganduboina; Writing-Original draft: Rohit Ganduboina, Jef Van den Eynde, Xander Jacquemyn, Omar Abdel Kerim, Sandeep Sainathan; Visualization: Rohit Ganduboina; Writing- Review and editing: Rohit Ganduboina, Jef Van den Eynde, Xander Jacquemyn, Omar Abdel Kerim, Sandeep Sainathan; Editing: Rohit Ganduboina, Jef Van den Eynde, Xander Jacquemyn, Sandeep Sainathan; Supervision, Project administration: Sandeep Sainathan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data underlying this article are available in the article and in its online supplementary material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.