
Abstract
Background:
Establishing the Korean Pediatric and Congenital Heart Surgery Database (KPCHSD) and linking it to the World Database for Pediatric and Congenital Heart Surgery (WDPCHS) is an important step toward creating a global network for quality care. Worldwide outcomes data are needed to support quality assurance and advocacy for necessary resources for pediatric and congenital cardiac care.
Methods:
The Korean Society for Thoracic and Cardiovascular Surgery collaborated with the World Society for Pediatric and Congenital Heart Surgery (WSPCHS) to develop and implement the KPCHSD. Variables selected for collection met the specific needs of Korean congenital heart surgery practice and were harmonized with the WDPCHS. Software was developed to link the databases in a secure environment, transfer data from KPCHSD to the WDPCHS, and produce outcomes reports.
Results:
The initial data upload from the KPCHSD to the WDPCHS was successfully completed in 2023. Over 2,500 operations from a 2-year period were transferred from the KPCHSD into the WDPCHS. Comparisons of individual center data will be made with both national and international aggregates. These comparisons will be available to individual centers via a password-protected cloud-based dashboard.
Conclusions:
Working in collaboration with our Korean colleagues, the WSPCHS has taken the next step toward developing a global network to share knowledge and expertise and to promote quality improvement in the treatment of congenital heart disease. Using this platform, countries perform data validation and completeness checks while maintaining control over their data. This aggregated data can support quality assessment and help secure the necessary resources for all countries, regardless of economic status.
Keywords
Introduction
The World Society for Pediatric and Congenital Heart Surgery (WSPCHS) has developed and implemented a platform to collect information on children undergoing operative correction of congenital heart defects. The mission of the World Database for Pediatric and Congenital Heart Surgery (WDPCHS) is to provide advanced outcomes analysis to all centers across the globe, regardless of socioeconomic status. 1 Established in 2017, to date, the WDPCHS has collected nearly 60,000 operations from 22 countries.2,3 Each center receives a biannual outcomes report comparing its data with an international aggregate. Kirklin Solutions Inc. (KIRSO) is the current data management center for the WDPCHS, responsible for data acquisition, protection, and analysis. 4
The World Database for Pediatric and Congenital Heart Surgery has traditionally collected information through the participation of individual centers. In many developing countries, obstacles to this effort have become apparent, including evolving government oversight, challenges in sending information outside the country via unreliable channels, and the resources required to submit data to multiple databases and registries within the country.5,6 Working with several pediatric and congenital surgical societies in specific countries, leadership within the WSPCHS has supported the development and implementation of national congenital heart surgery databases.4,7 Multiple advantages exist to developing a national database for congenital heart surgery, including the storage and control of information by national leadership, public awareness and transparency, accurate auditing of submitted data, and the successful acquisition of governmental and regional financial support.8–10 These national databases can then be linked to the WDPCHS, enabling the bulk transfer of patient-centered information without direct involvement from the center.
The initial attempt to create a national congenital heart surgery database linked to the WDPCHS was conducted in China. The effort was initially successful, although political obstacles have temporarily halted data transfer.11,12 South Korea was the next to successfully establish this linkage.8,13 Working with the leadership of the Korean Society for Thoracic and Cardiovascular Surgery (KSTCS) and the WSPCHS, a local information technology (IT) company, (M2 Community Co., Ltd) was hired to partner with IT personnel from KIRSO to develop a platform to collect national data and store it within the country. The current WDPCHS platform served as the foundation and was expanded to meet the specific needs of the Korean congenital heart surgery practice. In parallel with the development of the Korean Pediatric Congenital Heart Surgery Database (KPCHSD), a linkage was established, enabling the KPCHSD to transfer patient-specific information to the WDPCHS periodically. This data is then merged into the WDPCHS, and center-specific reports are provided that compare center data with national and international aggregates. Currently, 7 centers in South Korea submit data to this national database and have consented to the transfer of information to the WDPCHS. This represents approximately 3,000 cases annually, accounting for 90% of the congenital heart surgeries performed in the country. 8 The objects of this report are to present mechanisms by which countries or individual societies may develop and implement a platform to acquire and analyze outcomes data for patients with congenital heart defects. We also describe a process by which these data would be linked to a global effort to analyze such data.
Methods
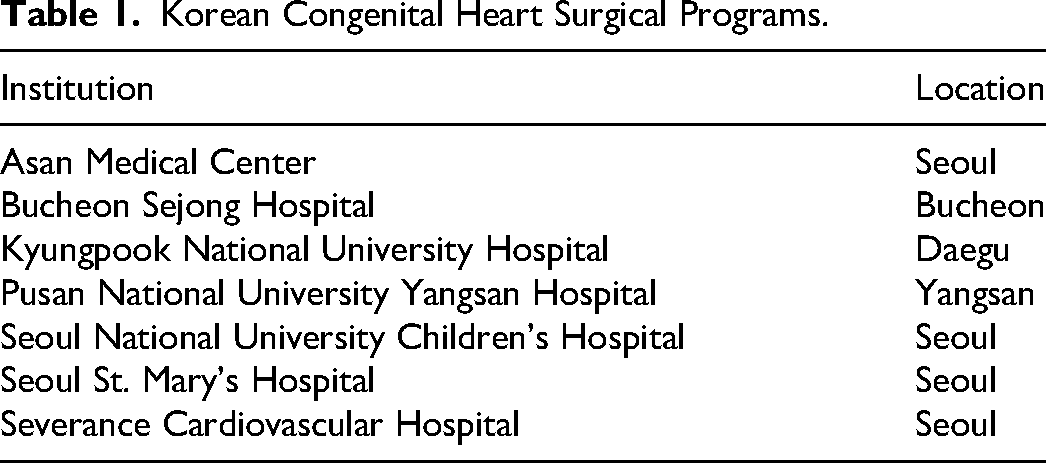
Following the establishment of the KPCHSD, 7 centers agreed to share information with the WDPCHS, accounting for 90% of congenital heart operations in the country (Table 1). Data Use Agreements and Participation Agreements were developed and signed by each center participating in the linkage project. Agreements were also signed between the WSPCHS and the KSTCS. Working in collaboration with the IT teams representing the KPCHSD, IT personnel at KIRSO developed a process for bulk transfer of deidentified data to the WDPCHS. A requirement for transfer of variables, met by the KPCHS, was that a “minimal Dataset” be acquired by KPCHSD from participating centers. This “minimal dataset” would populate the required number of variables collected for all Tier I procedures in the WDPCHS. These variables have been described in prior publications. 3
Korean Congenital Heart Surgical Programs.
To populate the data entry forms within the WDPCHS, KIRSO’s team of programmers used the list of variables to create a custom format for bulk data imports from both comma-separated value (CSV) and Extensible Markup Language (XML) files. If the uploaded files were CSV files, each would contain one dataset, represented by one line of table headers and multiple rows. To proceed with validation, any CSV file is converted to an XML file that contains all incoming data. An XSD (XML Schema Definition) file is then used to validate that all file contents are in the proper format.
If the files pass XSD validation, the data within them is then inserted into the appropriate staging table in KIRSO’s encrypted database. Each staging table's columns correspond to the collected variables, with a few notable exceptions: Local Hospital Patient ID, Local Surgery ID, Form ID, Validation Status, Validation Desc, and Skip Import On Columns. The Local Hospital Patient ID, Local Surgery ID, and Form ID columns are unique identifiers that link patients to their data across subsequent bulk data submissions. Validation Status, Validation Desc, and Skip Import On Columns provide more granular validation per record. For example, if a surgery record belongs to a patient that does not yet exist in the system, that record will receive an “ERROR” value in the Validation Status column and be excluded from the import process. A less severe violation will receive a “WARNING” value and may exclude the affected column rather than the entire record. Any excluded column is appended to a list stored in Skip Import On Columns.
Finally, valid data from each staging table is transformed to match the database schema used by the WDPCHS system to store entered data. When generating surgery forms, the system checks the procedure code; if the code is on the WDPCHS's internal list of index procedures, the generated form becomes a Tier 1 Surgery form. If the procedure code is not found on the WDPCHS's list of index procedures but still matches another valid procedure code, a Tier 2 Surgery form will be created instead. Forms generated this way are marked with a Data Source column set to “BATCH” and can be easily distinguished from manually entered data. At this stage, the KIRSO team of data analysts can now use the imported data.
With the validation of the data transfer, the KPCHSD completed the first bulk upload of variables at the end of 2023. Testing of this bulk transfer continued for the next few months to ensure the data transfer was accurate. Currently, the KPCHSD transfers data every 3 months.
Categorical variables are presented as absolute frequencies and percentages. Continuous variables are presented as medians (interquartile ranges) for skewed data. Categorical variables were compared via Pearson's chi-square test. Continuous variables were compared via Wilcoxon's rank sum test; 70% confidence intervals were used for mortality estimates as the ranges are narrower in our overall data. This allows for overall border comparisons and then more specific interpretations.
Results
Quarterly transfers of aggregation are deidentified, and predefined data elements are processed by the Korean Society database organizers at 3-month intervals. Once transferred, the data are analyzed for improper submission and the quality of the numerical variable. Data that falls outside of predefined ranges are rejected and returned for adjudication. Of the 2,884 procedures transferred from the KPCHSD, 2,747 (95%) met the minimal dataset requirement for integration into the WDPCHS. Incomplete data or data remaining to be submitted accounted for the 137 procedures not accepted. These procedures will be adjudicated in subsequent data transfers. This data were compared with a total international aggregate of 56,886 procedures submitted to the WDPCHS.
Of the total number of procedures received from the KCHSD, now referred to as the Korean aggregate, 63% were Tier I procedures (n = 1743/2747), with 37% (n = 1004/2747) classified as Tier II (REF). Among the Tier I cohort, 55% were male (n = 950/1743), with a median age at operation of 5.7 months (IQR: 2.1-35.6 months) and a median weight at operation of 6.8 kg (IQR: 4.7-13.2 kg). These values are not statistically different from the WDPCHS aggregate. Prematurity, defined as a gestational age at birth of less than 37 weeks, was present in 13.4% (n = 222) of the population. As expected, most patients were of Asian descent (2691/2747, 98%). Among the Tier I procedures submitted to the database, the most common were repair of ventricular septal defect (53%, 935/1743), repair of tetralogy of Fallot (242/1743, 13.9%), repair of atrioventricular septal defect (94/1743, 5.4%), and repair of coarctation of the aorta (69/1743, 4.0%). Figure 1 compares this Korean aggregate with the overall results of the World aggregate. Table 2 represents the specific congenital heart defect associated with each of the most frequent procedures submitted. Tier II procedures represent all procedures submitted to databases that were not classified as Tier I procedures (Table 3).
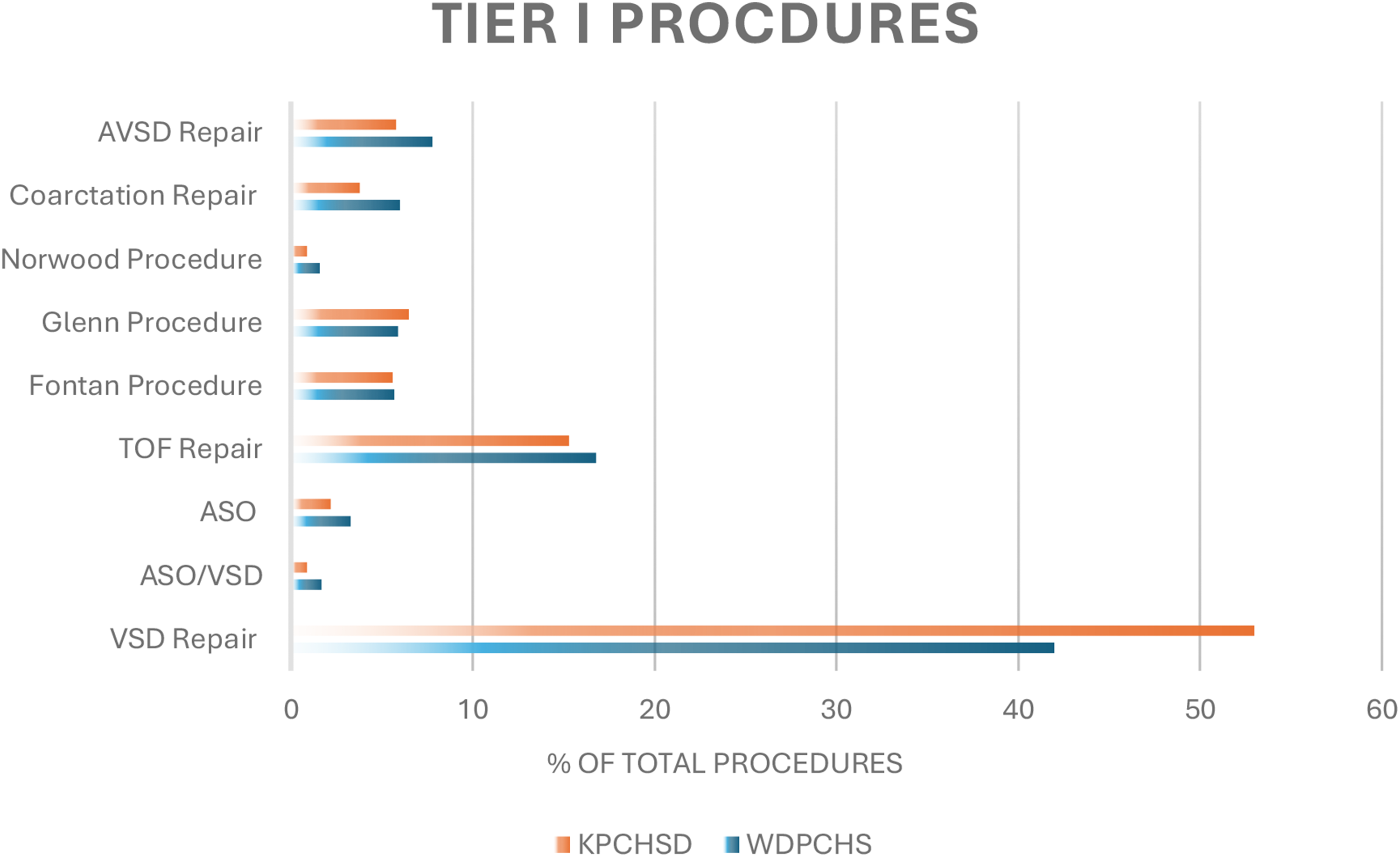
Tier I surgical procedures.
Congenital Heart Diagnosis.
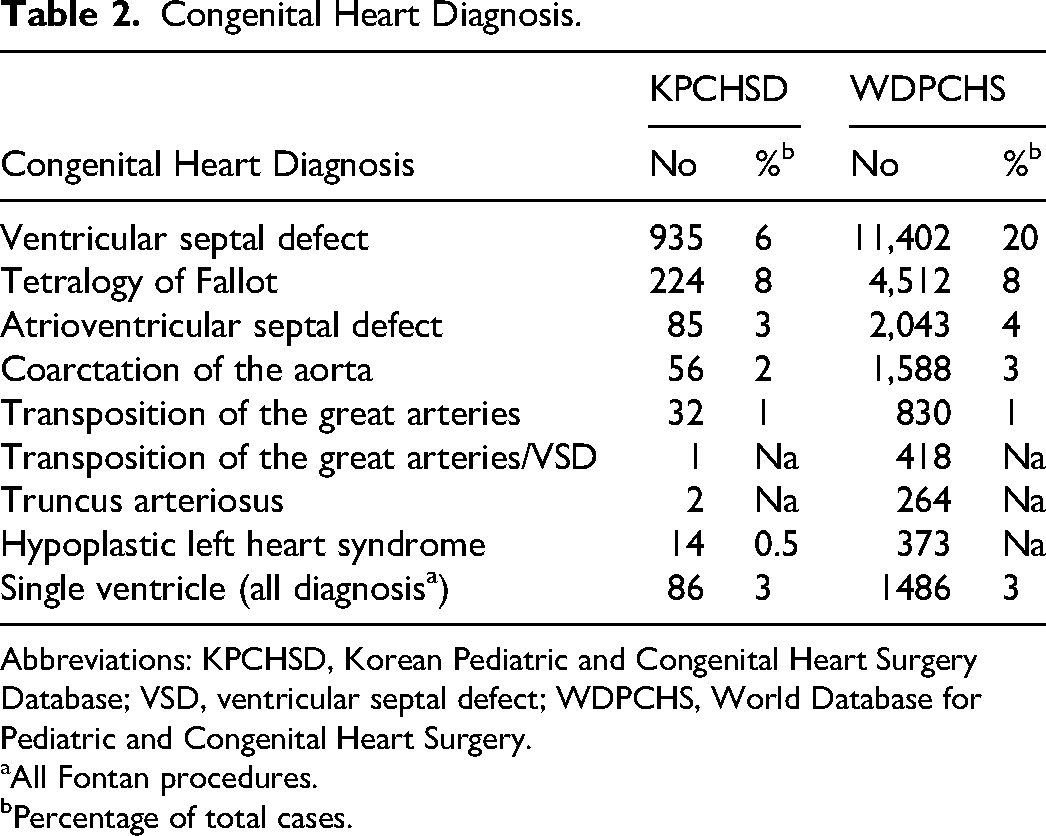
Abbreviations: KPCHSD, Korean Pediatric and Congenital Heart Surgery Database; VSD, ventricular septal defect; WDPCHS, World Database for Pediatric and Congenital Heart Surgery.
All Fontan procedures.
Percentage of total cases.
Tier II Procedures (Most Frequent).
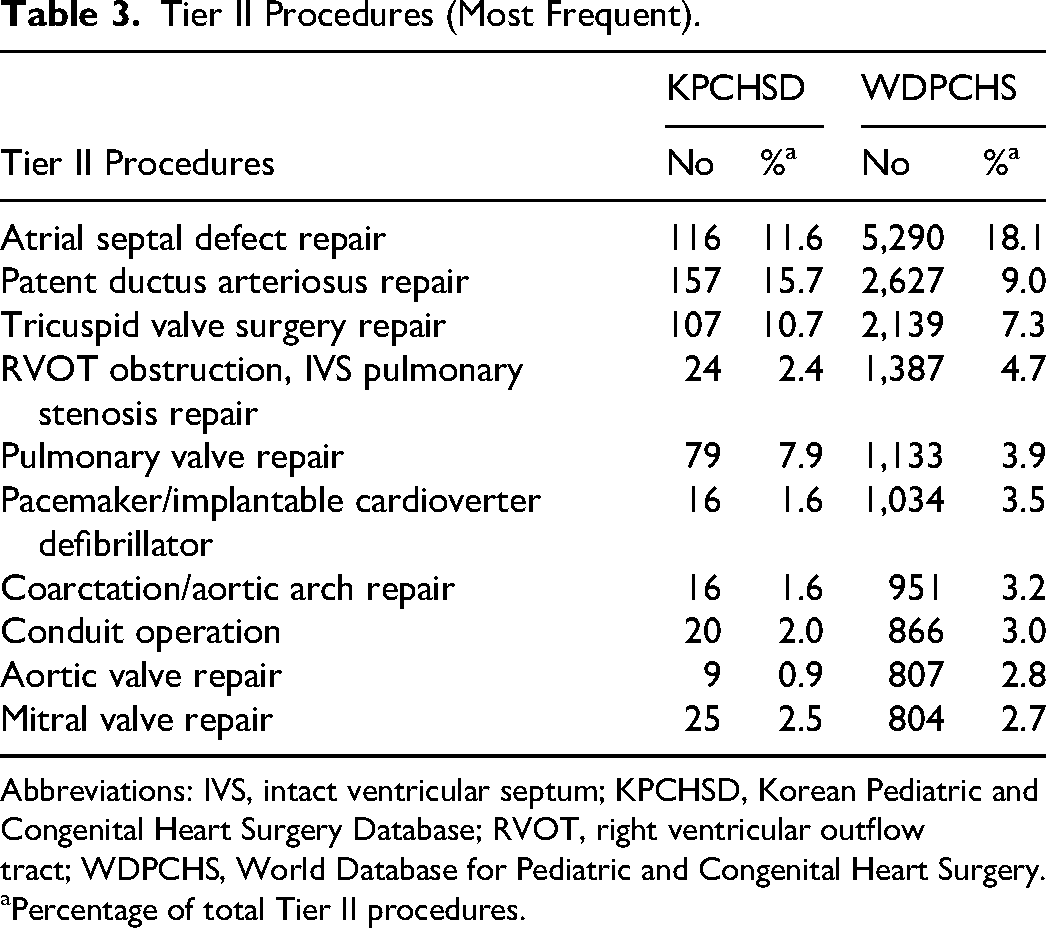
Abbreviations: IVS, intact ventricular septum; KPCHSD, Korean Pediatric and Congenital Heart Surgery Database; RVOT, right ventricular outflow tract; WDPCHS, World Database for Pediatric and Congenital Heart Surgery.
Percentage of total Tier II procedures.
Centers reported a small proportion (1%) of noncardiac congenital abnormalities associated with the primary congenital heart diagnosis. Of Tier I patients, 7.1% had a documented genetic syndrome, with the majority of these patients having Down syndrome (53%). This compares with 72% for the WDPCSH aggregate. Figures 2 and 3 show the risk categories for cases submitted, based on the STAT and RACHS-1 mortality categories, respectively. Approximately 1000 (86%) patients underwent an initial major cardiac procedure, while 1% had a reoperation with at least one prior sternotomy. The majority of surgical cases were elective (92%). Preoperative risk factors were identified in 19% of the World aggregate, but only 11% of the Korean aggregate. The most frequent preoperative risk factors were failure to thrive/malnutrition in the global aggregate (11.8%), whereas mechanical ventilation to treat cardiopulmonary failure was most common in the Korean population (4.5%) (Table 4).
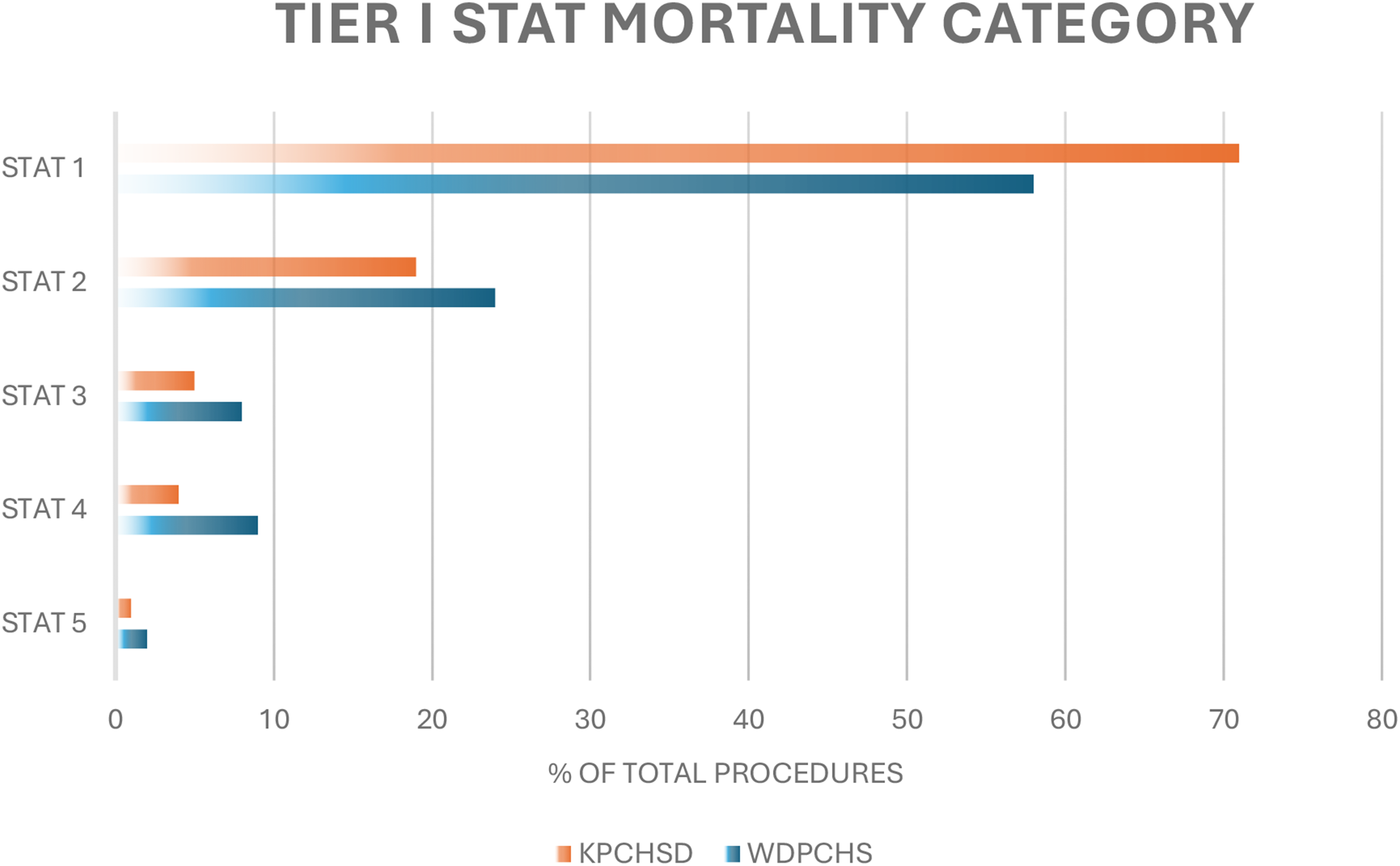
STAT mortality category.
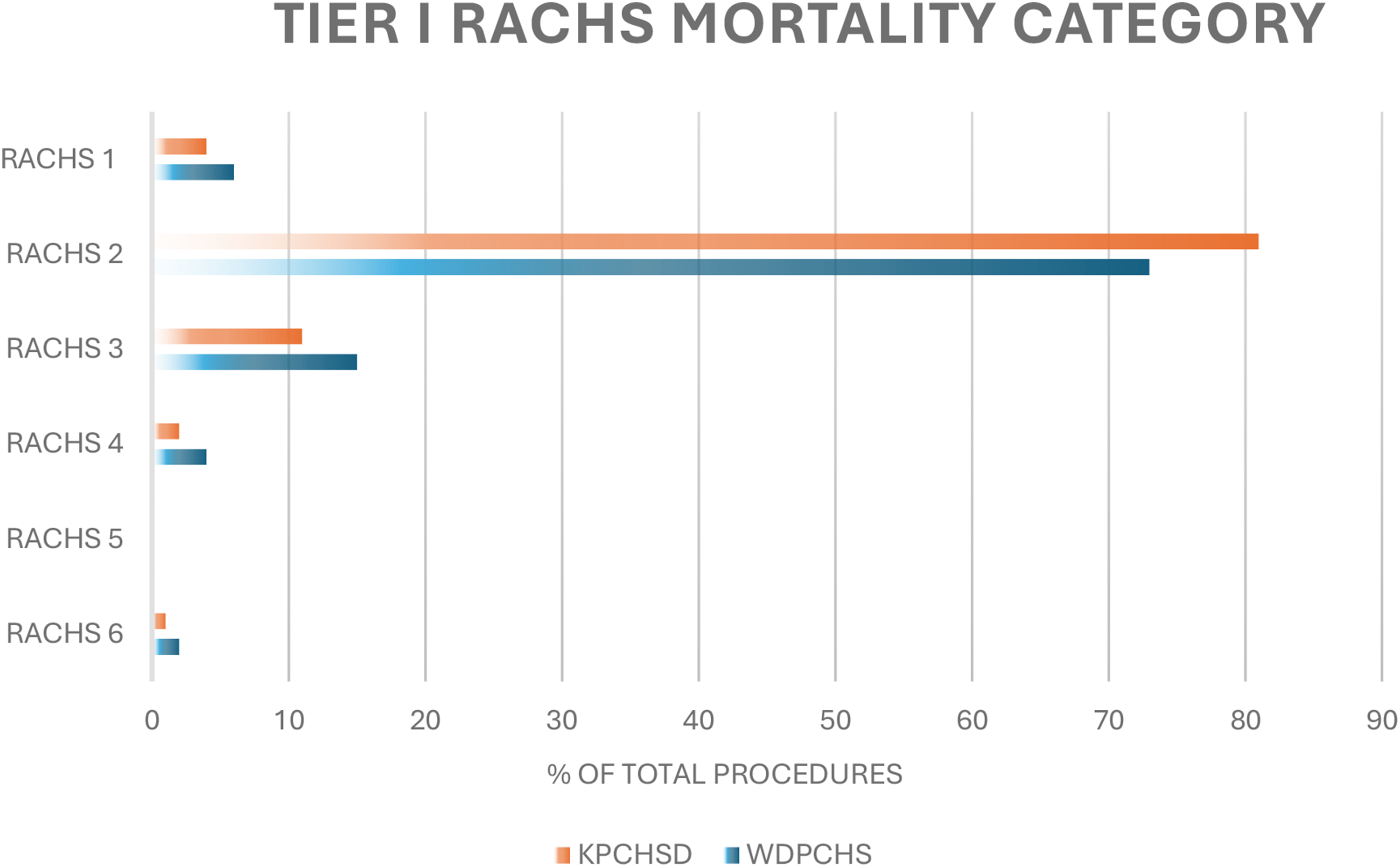
RACHS mortality category.
Preoperative Risk Factors.
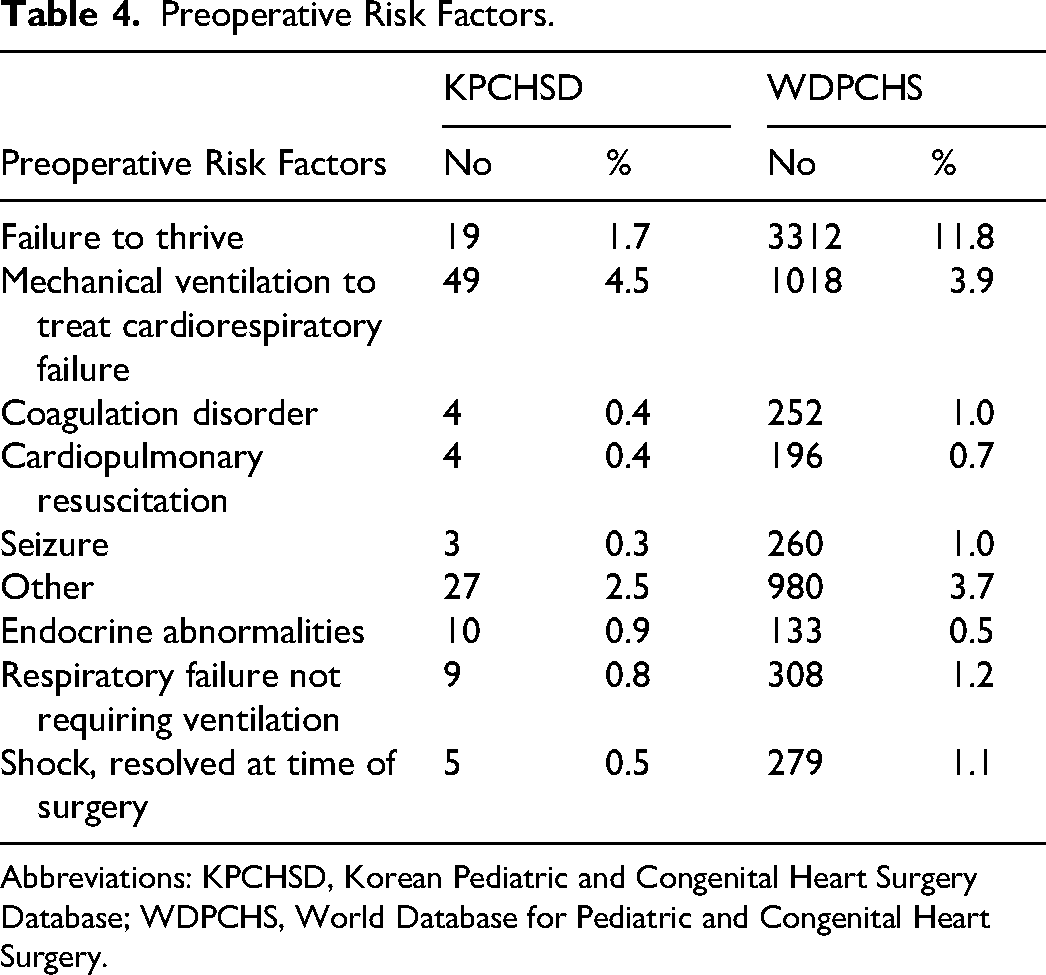
Abbreviations: KPCHSD, Korean Pediatric and Congenital Heart Surgery Database; WDPCHS, World Database for Pediatric and Congenital Heart Surgery.
Tier I Operative Details and Postoperative Complications
The database collects detailed operative information for all Tier 1 procedures. For the Korean Aggregate, the majority of operations (96%) were performed using cardiopulmonary bypass. The median cardiopulmonary bypass time was 111 min (IQR: 83-155min). Cross-clamping with the administration of cardioplegia was utilized in 97% of those utilizing cardiopulmonary bypass, with a median ischemic time of 67 min (IQR: 48-98 min). A few patients (4%) were exposed to deep hypothermic circulatory arrest with a median duration of 5 min (IQR: 1-20 min). Selective cerebral perfusion was used less often (2%) with a median duration of 28 min (IQR: 24-37 min). These times were comparable with the World aggregate. The most commonly used cardioplegia solution was a formulation of the Del Nido solution (82%), followed by Buckberg for the Korean aggregate (9%) and Custodial for the World aggregate (17%). Ninety-six percent of centers utilized intraoperative transesophageal echocardiography. The most common postoperative complications included cardiac dysfunction, respiratory insufficiency, chylothorax, arrhythmia requiring drug therapy, sepsis, mechanical circulatory support, and renal failure (Table 5).
Postoperative Complications.
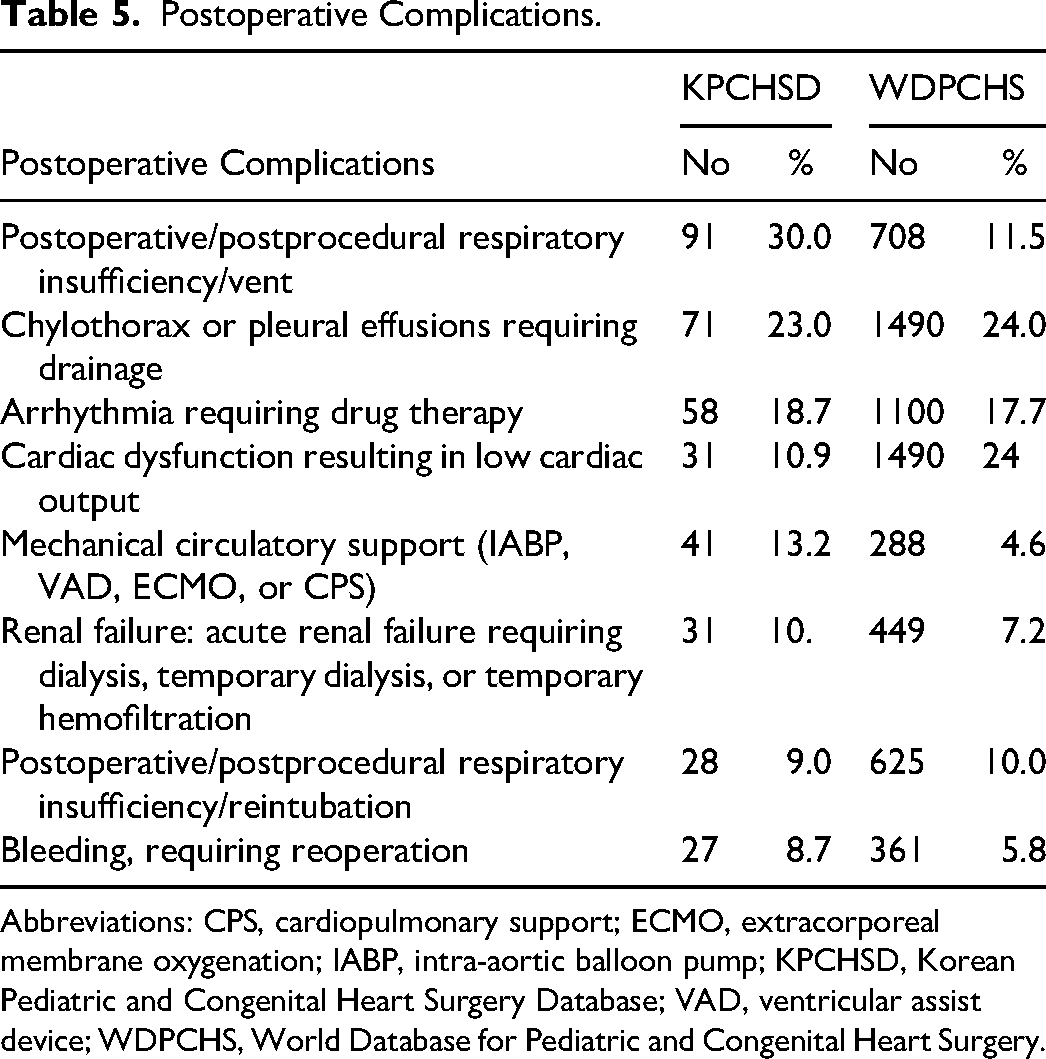
Abbreviations: CPS, cardiopulmonary support; ECMO, extracorporeal membrane oxygenation; IABP, intra-aortic balloon pump; KPCHSD, Korean Pediatric and Congenital Heart Surgery Database; VAD, ventricular assist device; WDPCHS, World Database for Pediatric and Congenital Heart Surgery.
Hospital Mortality
Overall hospital mortality for all Tier I patients in the Korean Aggregate was 1.5% (70% CI [1.2-1.8]). This is significantly lower than the 2.8% (70% CI [2.7-2.9]) for the World Aggregate (P < .001). Table 6 presents hospital mortality for the individual Tier I procedures compared with the overall WDPCHS mortality.
Tier I Mortality.
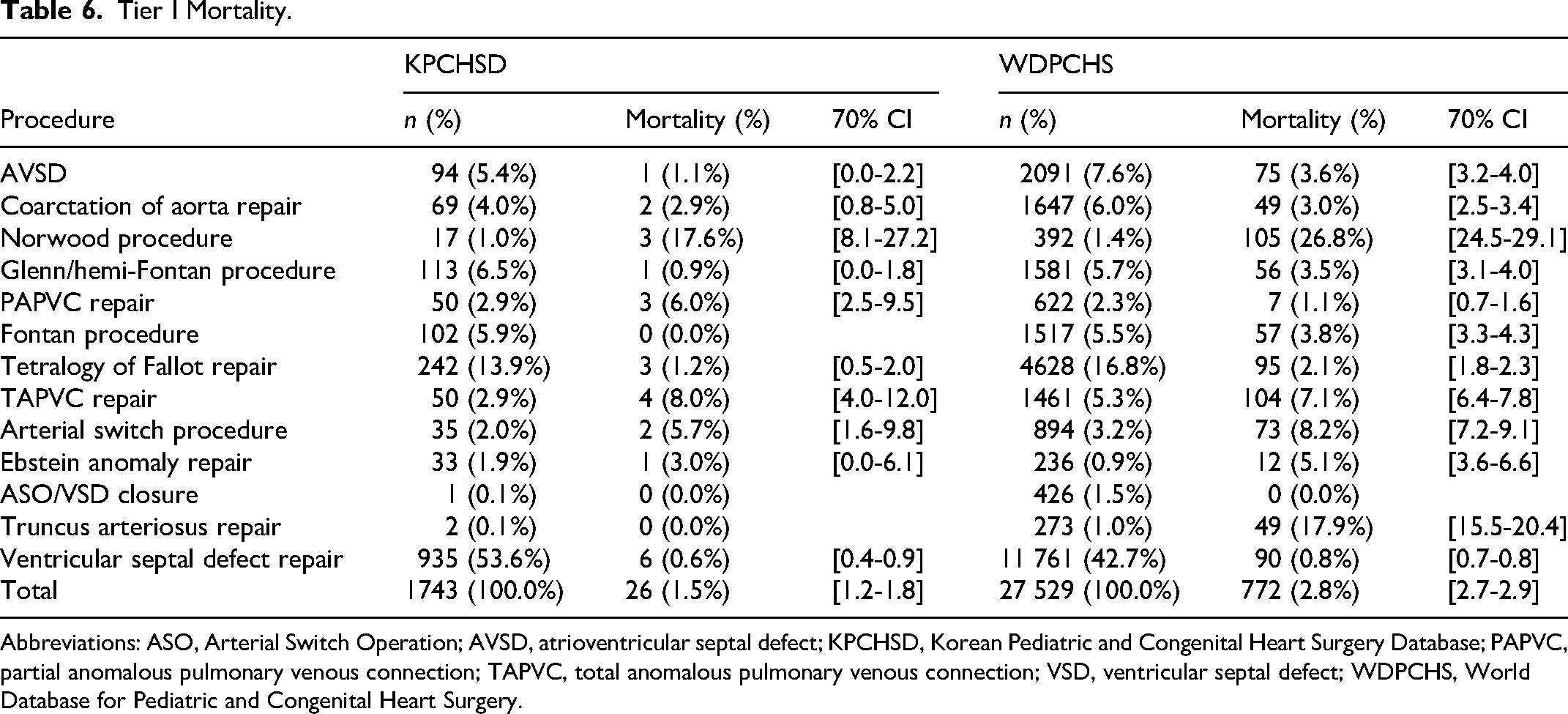
Abbreviations: ASO, Arterial Switch Operation; AVSD, atrioventricular septal defect; KPCHSD, Korean Pediatric and Congenital Heart Surgery Database; PAPVC, partial anomalous pulmonary venous connection; TAPVC, total anomalous pulmonary venous connection; VSD, ventricular septal defect; WDPCHS, World Database for Pediatric and Congenital Heart Surgery.
Discussion
Before the Korea Heart Foundation (KHF) was established in 1984, many children with congenital heart disease underwent surgical correction abroad. 13 Occasionally, international nongovernmental organizations (NGOs) conduct missions to specific centers within the country. With the financial support provided by KHF, many children with CHD were able to undergo corrective surgery within the country. By its business practices, the KHF maintained a minimal dataset on outcomes for children who underwent surgery. Prior to this effort, there was no nationwide data on the surgical outcomes of children with congenital heart disease. Recent reports have documented the surgical outcomes in children supported by the KHF. The most recent study, from 2020, analyzed outcomes for more than 6500 patients undergoing operative repair between 2000 and 2014. 13 The authors showed a decrease in overall mortality among children operated on within the country. Between 1984 and 1999, the early operative mortality for children undergoing correction for a congenital heart defect was 8.6%, with late mortality at 5.35%. In the most recent period (2000-2014), early mortality declined to 3.8%, whereas late mortality was 1.8%. Clearly, these successes within the country are multifaceted, but significant governmental support for this population was a major contributing factor.14,15 Although the data from the KHF registry provides very important information on surgical mortality, the dataset's limited granularity allowed only minimal investigation into the practice of congenital heart surgery.
In 2020, KSTCS established a national congenital heart surgery database. In close collaboration with the WSPCHS, KSTCS developed and operated a platform to collect preoperative, operative, and postoperative variables for children undergoing correction of congenital heart defects. The Society recruited 10 institutions with active congenital heart programs to participate in this effort. The first submission to the KPCHSD was received in 2021. During development, KSTCS leadership worked with staff at Kirklin Institute Inc. and the WDPCHS data center to develop a linkage process that enables the bulk transfer of a minimal dataset to the WDPCHS. Seven of these centers agreed to the transfer of data to the WDPCHS. Centers that didn’t approve of this transfer stated that their institutional requirements wouldn’t permit the transfer of data outside the country. The 7 active centers agreed to create a national aggregate for comparison with their individual outcomes data. The initial transfer occurred late in 2023. This report describes the first transfer of more than 2500 procedures from the KPCHSD to the WDPCHS.
All Korean centers that have consented to allow the transfer of deidentified patient data from the KPCHSD to the WDPCHS receive a biannual report from KIRSO. These reports include detailed preoperative, operative, and postoperative data on a select group of congenital heart surgeries. Individual center data are compared with aggregate national data (from all participating Korean centers) and with an international aggregate of all centers submitting information to the WDPCHS. The initial uploads from KPCHSD encountered several challenges, which the data center staff promptly addressed. Before the initiation of the bulk transfer from KPCHSD, several centers were sending data to WDPCHS as an independent entity. This led to significant overestimation of the number of submitted cases and duplicate procedures. The data center, working closely with the individual centers, eliminated duplications and cleaned the data. Another issue observed and adequately addressed was the appropriate interval for KPCHSD's recurrent data submissions. The initial 6-month intervals revealed that incomplete submissions (ie, lacking discharge follow-up) were never completed. Reducing the duration of recurrent submissions to 3 months significantly improved follow-up on incomplete submissions and discharge from the database.
Patients born with a congenital heart defect form a relatively homogeneous population in the country, as 98% are of Asian descent. This may provide a clearer understanding of the genetic basis of congenital heart defects. 16 The case mix complexity compares favorably with both national data aggregates and published information from other high-income countries. 17 Modifiable preoperative risk factors have a tremendous impact on postoperative outcomes following congenital heart surgery.18,19 When reviewing this closely monitored population, we see that the incidence of malnutrition or failure to thrive is significantly lower than in most centers, even when including high-income countries, accounting for only 1.7% of reported preoperative risk factors, compared with almost 12% within the World aggregate. This certainly contributes to the excellent operative outcomes and lower overall mortality (1.5%) compared with the World aggregate (2.8%).20,21 Most operative complications align with the overall global data. However, 2 postoperative complications show a higher incidence compared with the global average. Respiratory insufficiency (30% vs 11.5%) and mechanical circulatory support (13.2% vs 4.6%) were more common in the Korean cohort. Several factors may explain these differences, including a smaller sample size in the Korean group, longer postoperative ventilator support influenced by institutional practices, and more proactive use of mechanical support shortly after surgery.
This article presents a discrete comparison of the Korean National aggregate with the WDPCHS international aggregate. One of the missions of the WDPCHS was to establish validated benchmarks for outcomes in a group of congenital heart operations. These submissions come from a mix of middle- and low-income as well as high-income countries. The data are important, as they provide an overall estimate of acceptable outcomes for these procedures, but they lack the specificity needed for individual programs with fewer dedicated resources for treating congenital heart disease. This underscores the importance of establishing national and regional benchmarks using outcome data when addressing the needs of specific congenital heart programs. Efforts in Korea and the national data collected underscore the critical need to establish national mechanisms for collecting these data. 22 Notably, members of the WSPCHS are collaborating with several countries in Southeast Asia to develop a regional benchmark for these outcomes. We have successfully established the Malaysian National Congenital Heart Surgery Database in Kuala Lumpur, supported by government funding and linked to the WDPCHS. Two major centers are now submitting to this entity, with several others close to joining.
In addition to efforts to establish traditional early surgical outcomes databases, a substantial effort is underway in the Philippines to develop and implement a novel platform to collect detailed information on all patients with congenital heart defects and to follow them over the course of their lives. The Philippine National Congenital Heart Disease database uses a cloud-based system to collect data from more than 100 institutions nationwide. The goals of this effort are to collect pertinent data from birth through any procedures (eg, catheterization and surgery) and into adulthood. The primary endpoint will be survival at 30 days and hospital discharge after repair in patients with 2-ventricle anatomy and after achieving a Fontan circulation in series in patients with single-ventricle anatomy. The other key Quality Assurance endpoint of particular interest to government and private payers is the efficiency of the approach, as measured by the number of procedures, admissions, and days in hospital required to achieve the primary endpoint. These endpoints are more meaningful and practical in the current era of collaborative patient management by interventional cardiologists and cardiac surgeons. In addition, a registry based on these endpoints will incentivize programs to operate efficiently and avoid multiple palliative procedures. A pilot of this effort is set to start in the middle of 2026. Several other Southeast Asian countries, including Vietnam, Thailand, Singapore, and Indonesia, are at various stages of development of these registries.
Limitations
A methodology and description of how to create a national congenital heart surgery database and linkage to a global repository of data was described. The article is descriptive and lacks a significant statistical evaluation for comparison. We hope a follow-up review will be provided to extend the valid statistical analysis in the future. These additional data could include long-term outcome data, and the absence of formal risk-adjusted outcome comparisons.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.