
Abstract
Objective:
To describe surgical outcomes, in-hospital mortality, and variables associated with mortality in pediatric patients with congenital heart disease (CHD) at a national referral center in México over 14 years.
Methodology:
Retrospective cross-sectional study of 4494 patients under 18 years of age with CHD undergoing cardiac surgery (2010-2024) at the Instituto Nacional de Cardiología “Ignacio Chávez,” using Registro Nacional de Cirugía Cardíaca Pediátrica y Cardiopatías Congénitas (RENACCAPE) data. Comparisons used χ2, Fisher's exact, and Mann–Whitney U tests (P < .05). Analysis was univariate; RACHS-1/STAT scores were incompletely recorded and excluded from risk adjustment.
Results:
Among 4494 patients (53.5% [2405/4494] male), the predominant age groups were children 1 to 12 years (56.1% [2521/4494]), infants 1 to 11 months (19.8% [888/4494]), adolescents (17.4% [784/4494]), and neonates (6.7% [301/4494]). Down syndrome (6.2% [277/4494]) and DiGeorge syndrome (1.2% [55/4494]) were the most frequent genetic comorbidities; 85.5% (3844/4494) underwent elective surgery. Leading procedures included ventricular septal defect closure (13.6%; [611/4494] mortality 1.8% [11/611]), modified Blalock–Taussig-Thomas shunt (9.8% [440/4494]; mortality 11.1% [49/440]), total anomalous pulmonary venous connection repair (7.4% [334/4494]; mortality 8.4% [28/334]), atrial septal defect closure (6.7% [303/4494]; mortality 0.0%), and tetralogy of Fallot repair (5.9% [267/4494]; mortality 7.9% [21/267]). Norwood had the highest procedure-specific mortality (71.4% [5/7]), followed by Damus–Kaye–Stansel (60.0%) and Jatene (26.0% [32/123]). Overall mortality was 9.4% (421/4494), declining from 10.5% (2010) to 7.1% (2024), with a transient rise during COVID-19. Mortality-associated variables included neonatal/infant age, low weight, cyanotic CHD, genetic syndromes, prolonged cardiopulmonary bypass (147 vs 89 min), longer aortic cross-clamp time (83 vs 54 min), and urgent surgery (all P < .001).
Conclusions:
To our knowledge this is this largest single-center Mexican pediatric CHD series, in-hospital mortality was 9.4% with a declining trend. Procedure-specific mortalities exceeded STS benchmarks, identifying targets for quality improvement. Expanding RENACCAPE and strengthening referral networks remain priorities.
Keywords
Introduction
Congenital heart diseases (CHDs) are structural defects of the heart or great vessels that arise from embryonic life. CHDs are the most common congenital malformations worldwide, contributing substantially to infant mortality and disability-adjusted life years.1,2 In Mexico, between 12,000 and 16,000 new cases are reported each year in newborn children, being the second leading cause of death in children under 5 years of age. 3 Despite the technological improvements available for diagnosis and treatment, CHD continues to be one of the main problems for the Mexican health system. 4
Surveillance of CHD is sporadic, and only 11 countries in Latin America and the Caribbean have established a surveillance system, which differs in coverage and methodology but has made some progress. 5 In this way, national programs and registries have been created for the care and attention of patients with CHD, such as the National Program of CHDs found in Argentina 6 and the Registro Nacional de Cirugía Cardíaca Pediátrica y Cardiopatías Congénitas (RENACCAPE) in Mexico, 7 which is the first computerized system developed in 2010 to collect data on the surgical care of CHD patients in the Mexican population.
This study aims to describe the surgical outcomes and identify factors associated with in-hospital mortality among patients with CHD registered in RENACCAPE at a national referral center in Mexico over a 14-year period, and to characterize the annual volume of cardiac interventions performed at this institution.
Methodology
This descriptive, retrospective cross-sectional study analyzed the characteristics and surgical outcomes of patients with CHD treated at a national referral center (Instituto Nacional de Cardiología Ignacio Chávez, Mexico City) between January 2010 and December 2024. Data were obtained from RENACCAPE, the first national computerized registry created in Mexico in 2010 to systematically collect data on the surgical care of CHD. RENACCAPE captures prospective, standardized data entered by trained personnel at each participating institution, including patient demographics, diagnosis, procedure type, use of cardiopulmonary bypass (CPB), postoperative complications, and in-hospital mortality. Inclusion criteria were: (1) patients under 18 years of age of either sex; (2) confirmed diagnosis of CHD; (3) underwent cardiac surgery during the study period; and (4) registered in RENACCAPE with a record attributed to our institution. Exclusion criteria were: (1) patients whose records were attributed to a different center; and (2) records with critical missing data that precluded outcome ascertainment. The primary outcome variable was in-hospital mortality, and associated factors evaluated included demographic characteristics, clinical and syndromic history, geographic origin, CHD type, surgical procedure characteristics, postoperative complications, and year of surgery.
In the descriptive analysis, categorical variables are presented as frequencies and percentages, while numerical variables are presented as median and interquartile range due to nonnormal distribution (Kolmogorov–Smirnov test). In the inferential analysis, the χ2 test or Fisher's exact test was used to evaluate differences between categorical variables and mortality, and the Mann–Whitney U-test was used to evaluate differences between numerical variables and mortality. For all tests, a 2-tailed P < .05 was considered statistically significant. All statistical analyses were performed using R statistical software (version 4.5.1). The risk of selection bias among participants was considered and addressed by implementing precise inclusion and exclusion criteria.
This retrospective study received approval from the institutional committee (CI-090-2025) on December 25, 2025, and adhered to the ethical principles established in the Declaration of Helsinki, in addition to following the STROBE guidelines for the presentation of cross-sectional studies. As this is a retrospective study in which information was obtained from the RENACCAPE database and the center's electronic medical records, the risk was considered minimal. Due to the retrospective nature of the study, obtaining informed consent was not feasible. All data were safeguarded in the respective database while maintaining strict confidentiality of participants.
Results
A total of 5137 records were identified in the RENACCAPE database, of which a total of 4494 patients under 18 years of age with CHD were included during the period from 2010 to 2024, who underwent cardiac surgery at our center and met the inclusion criteria. The predominant patients were children who were 1 to 12 years of age (n = 2521/4494; 56.1%) and male (n = 2405/4494; 53.5%), followed by infants aged 1 to 11 months (n = 888/4494; 19.8%), adolescents who were 13 to 17 years of age (n = 784/4494; 17.4%), and neonates (0-28 days; n = 301/4494; 6.7%) (Table 1). The median weight was 13.3 kg (IQR: 6.3-25 kg), height 98 cm (IQR: 68-130 cm), and body surface area (BSA) 0.6 m2 (IQR: 0.3-0.9 m2). Additionally, 9.8% (n = 444/4494) of patients had a syndrome, the most common being Down syndrome (n = 277/4494; 6.2%) and DiGeorge (22q11.2 deletion, n = 55/4494; 1.2%) (Table 1).
Demographic Characteristics and Clinical History.
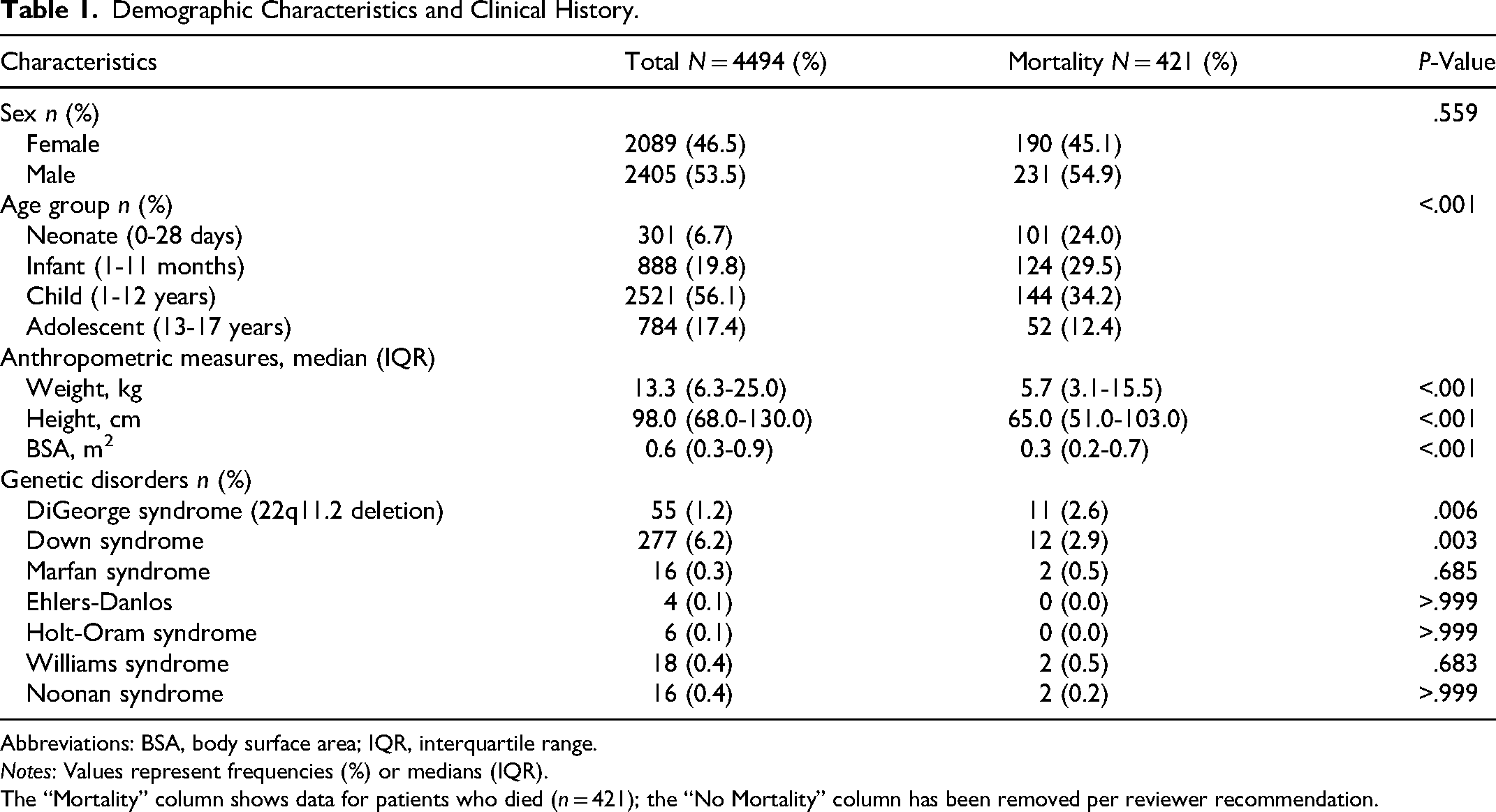
Abbreviations: BSA, body surface area; IQR, interquartile range.
Notes: Values represent frequencies (%) or medians (IQR).
The “Mortality” column shows data for patients who died (n = 421); the “No Mortality” column has been removed per reviewer recommendation.
Regarding the geographic origin, the highest absolute case volumes per state were recorded from the State of Mexico, Mexico City, Michoacán, and Oaxaca (range: 290-1061 cases per state); intermediate volumes from Veracruz, Hidalgo, Guanajuato, Puebla, and Morelos (169-284 cases); lower volumes from Chiapas, Guerrero, Querétaro, and Durango (76-144 cases); and fewer than 70 cases from the remaining states (Figure 1). The distribution of CHD found were mainly cyanotic (n = 2440/4494; 54.3%), and according to their anatomopathological and pathophysiological grouping, the most frequent diagnoses were conotruncal defects (1440/4494, 32%), septal defects with left-to-right shunt (1135/4494, 25.3%), pulmonary venous return (472/4494, 10.5%), left ventricular outflow tract obstruction (LVOTO), (429/4494, 9.5%), univentricular heart (400/4494, 8.9%), and valvulopathies (337/4494, 7.5%) (Table 2).
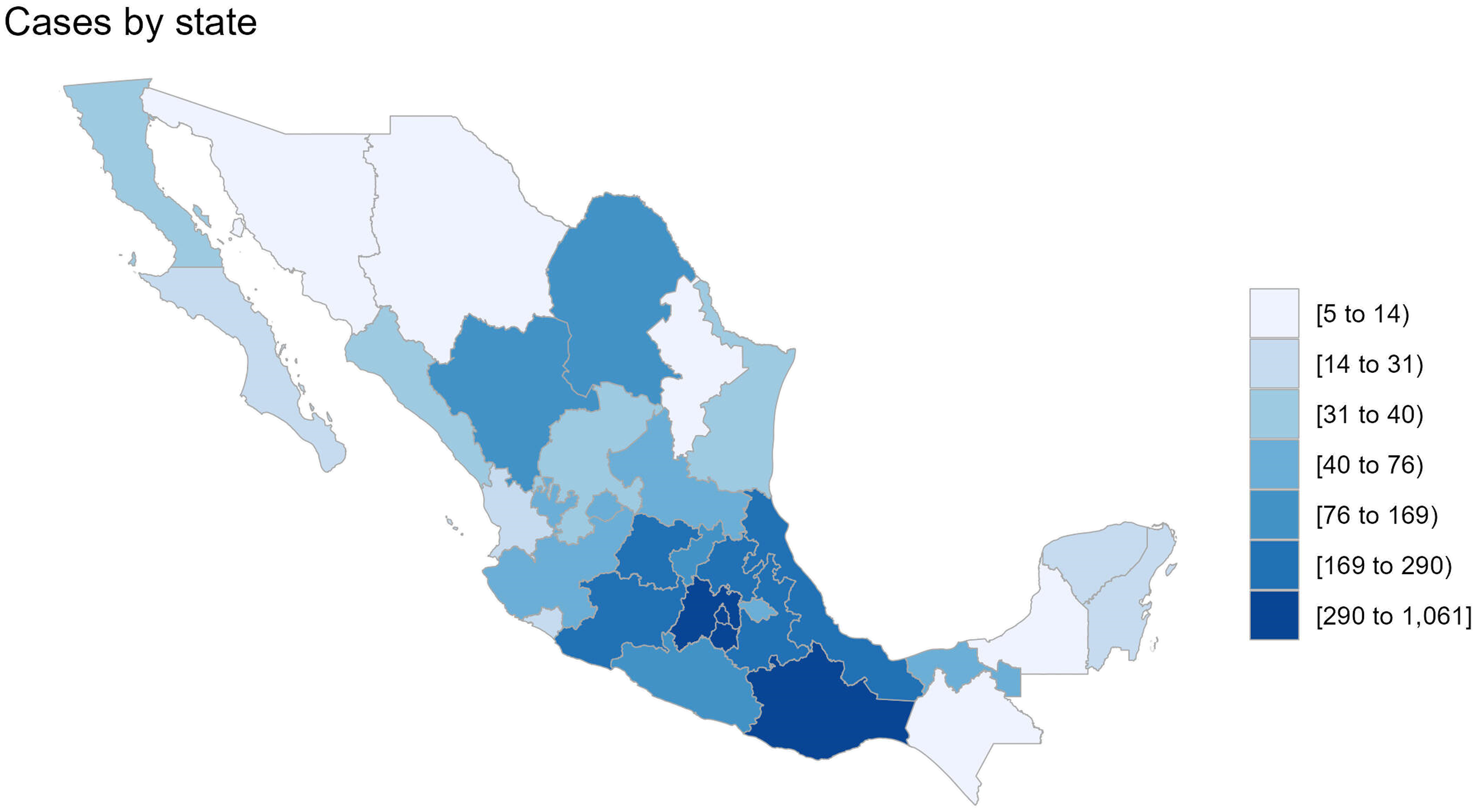
Cases of congenital heart disease by state in children under 18 years in Mexico from 2010 to 2024.
Distribution of Pediatric Congenital Heart Diseases.
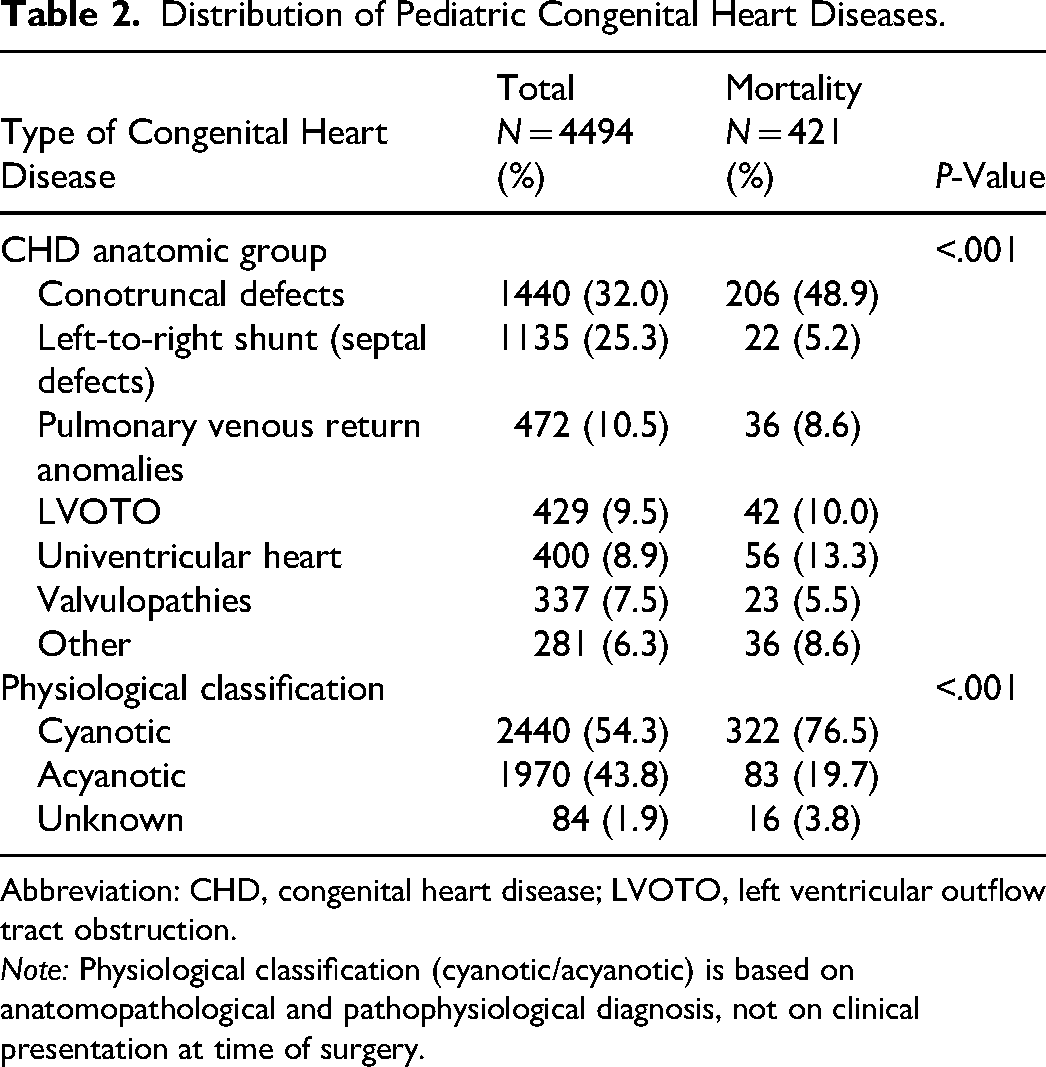
Abbreviation: CHD, congenital heart disease; LVOTO, left ventricular outflow tract obstruction.
Note: Physiological classification (cyanotic/acyanotic) is based on anatomopathological and pathophysiological diagnosis, not on clinical presentation at time of surgery.
Surgical Intervention Characteristics
Surgical interventions were mainly elective (n = 3844/4494; 85.5%), and 14.5% of cases (n = 650/4494) were urgent (Table 3). The use of CPB was required in 3549/4494 patients (79%) with a median duration of 94 min (IQR: 64-134 min), while aortic cross-clamping was performed in 3340/4494 patients (74.3%) with a median duration of 56 min (IQR: 33-85 min). In only 27 cases (0.6%) was deep hypothermic circulatory arrest used for a median duration of 20 min (IQR: 8.0-39.5 min), and 4038/4494 patients (89.9%) were admitted to a pediatric intensive care unit (PICU) (Table 3).
Characteristics of General Surgical Procedures.
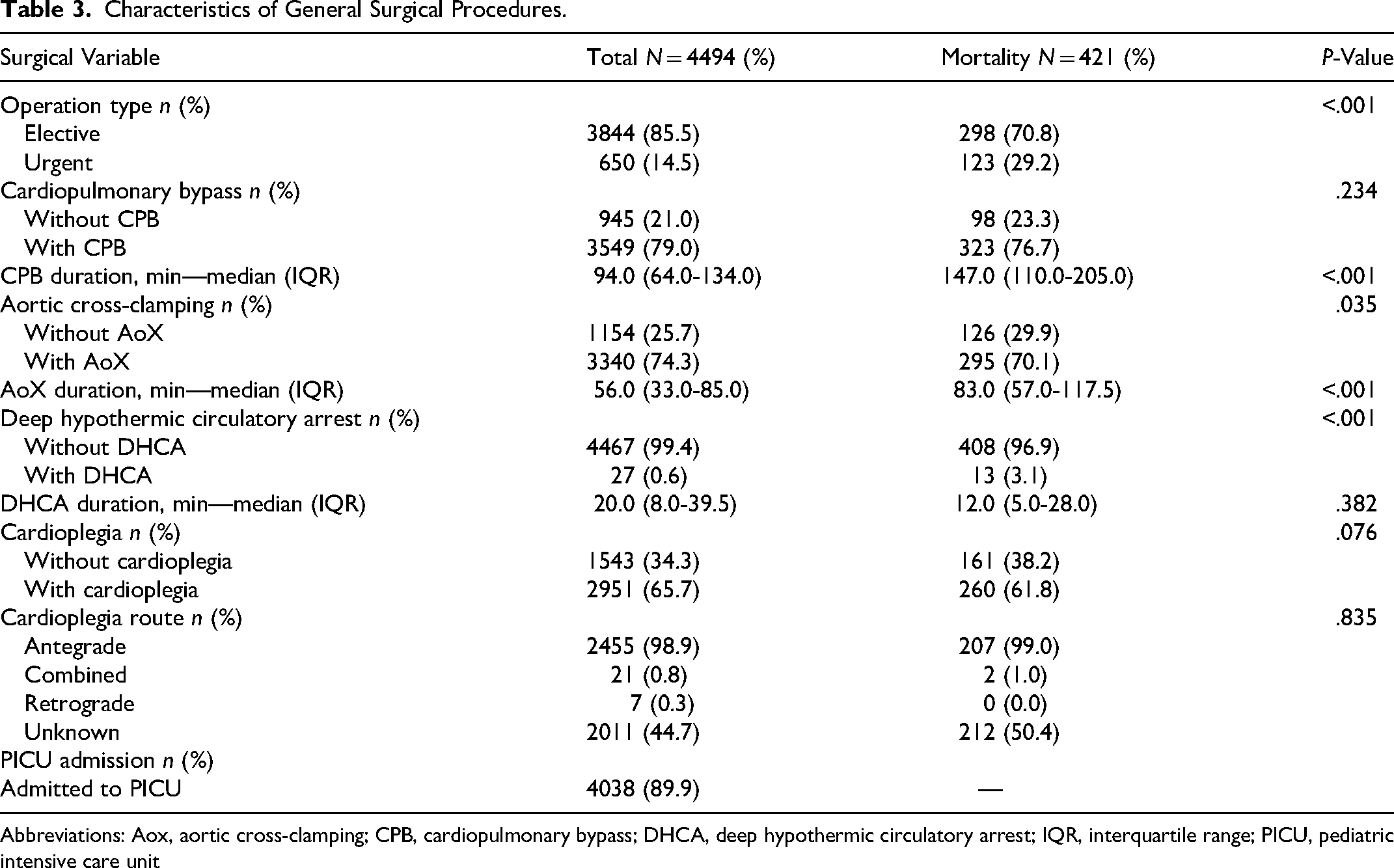
Abbreviations: Aox, aortic cross-clamping; CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest; IQR, interquartile range; PICU, pediatric intensive care unit
A list of the procedures performed along with their frequency and mortality are shown in (Table 4).
Surgical Procedures: Volume and Mortality (Top Procedures).
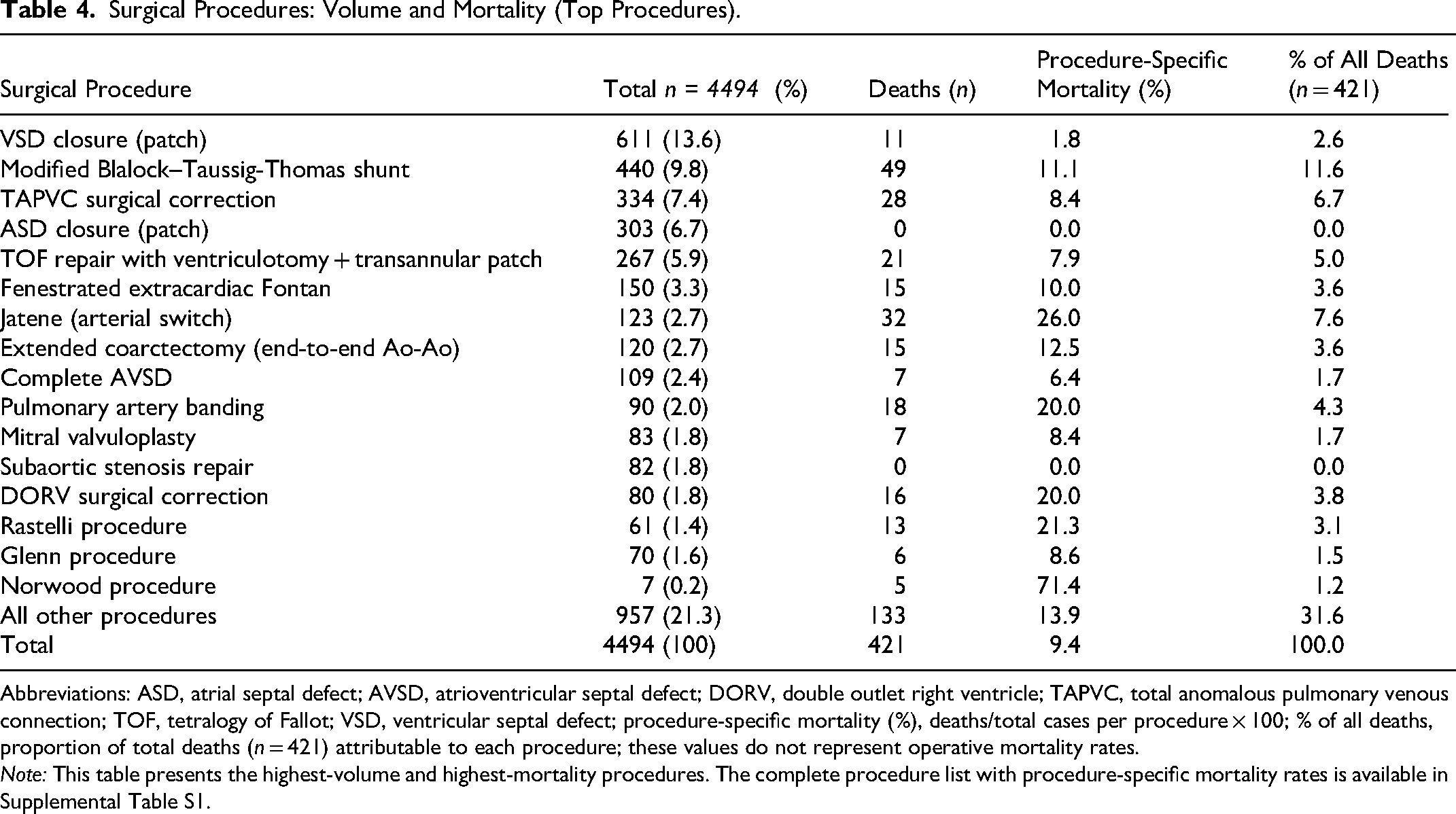
Abbreviations: ASD, atrial septal defect; AVSD, atrioventricular septal defect; DORV, double outlet right ventricle; TAPVC, total anomalous pulmonary venous connection; TOF, tetralogy of Fallot; VSD, ventricular septal defect; procedure-specific mortality (%), deaths/total cases per procedure × 100; % of all deaths, proportion of total deaths (n = 421) attributable to each procedure; these values do not represent operative mortality rates.
Note: This table presents the highest-volume and highest-mortality procedures. The complete procedure list with procedure-specific mortality rates is available in Supplemental Table S1.
Following surgical procedures, it was found that patients had a median of 3.0 days (IQR: 2.0-6.0) stay in the PICU and 12.0 days (IQR: 7.0-23.0) postoperative stay (Table 5).
Postoperative Outcomes and Complications.
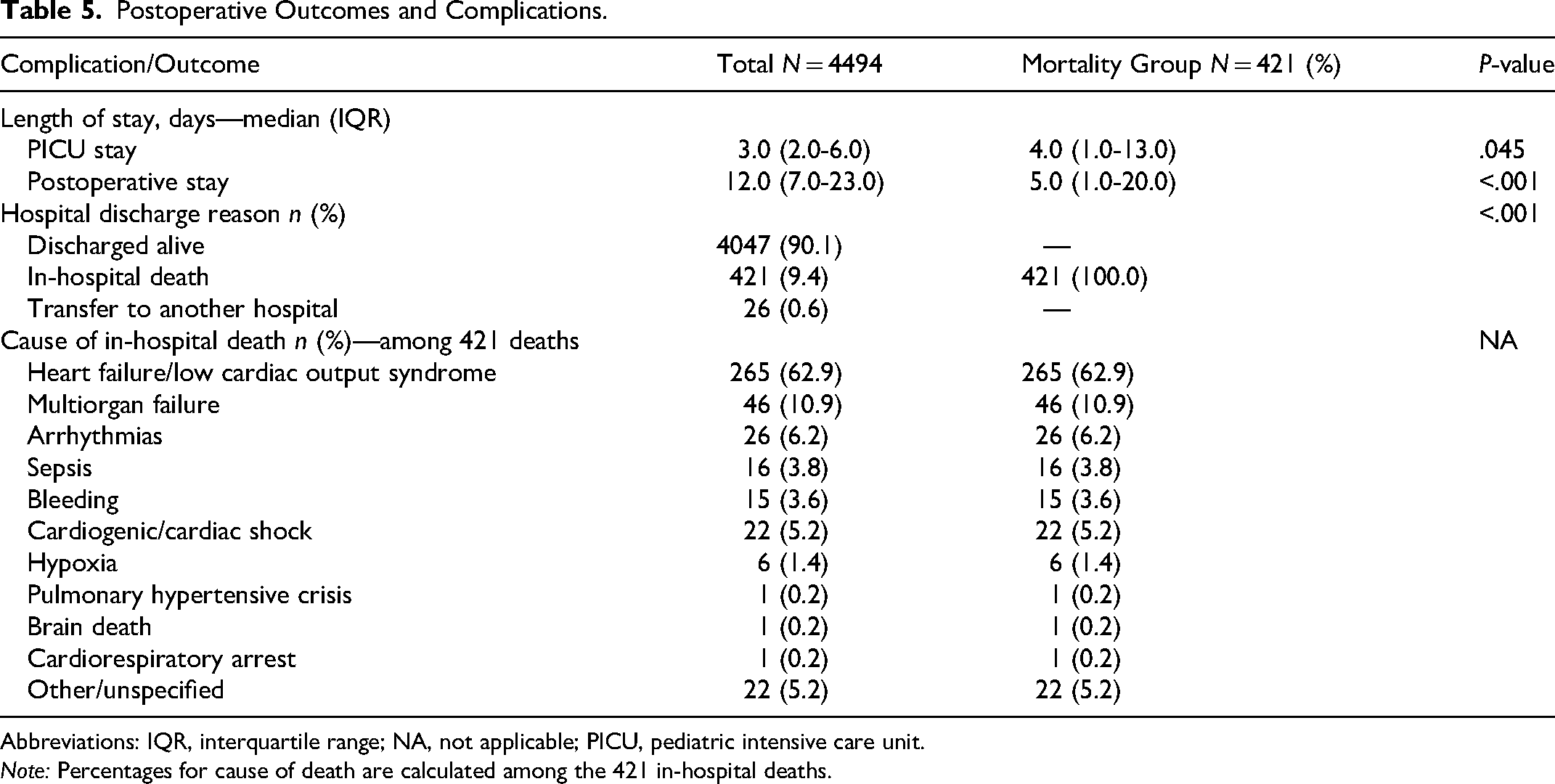
Abbreviations: IQR, interquartile range; NA, not applicable; PICU, pediatric intensive care unit.
Note: Percentages for cause of death are calculated among the 421 in-hospital deaths.
Mortality
The overall mortality of patients with CHD was 9.4% (n = 421/4494); the main cause of death was low cardiac output syndrome (n = 265/421; 62.9%), followed by multiorgan system failure (n = 46/421; 10.9%) and arrhythmias (n = 26/421; 6.2%) (Table 5).
From 2010 to 2024, the number of surgeries performed was relatively constant (256 to 380 cases per year), with 21 to 39 deaths per year (Figure 2). In 2010, mortality was found to represent 10.5% (39/371 deaths), while in 2024, a decrease corresponding to 7.1% (21/266 deaths) was observed.
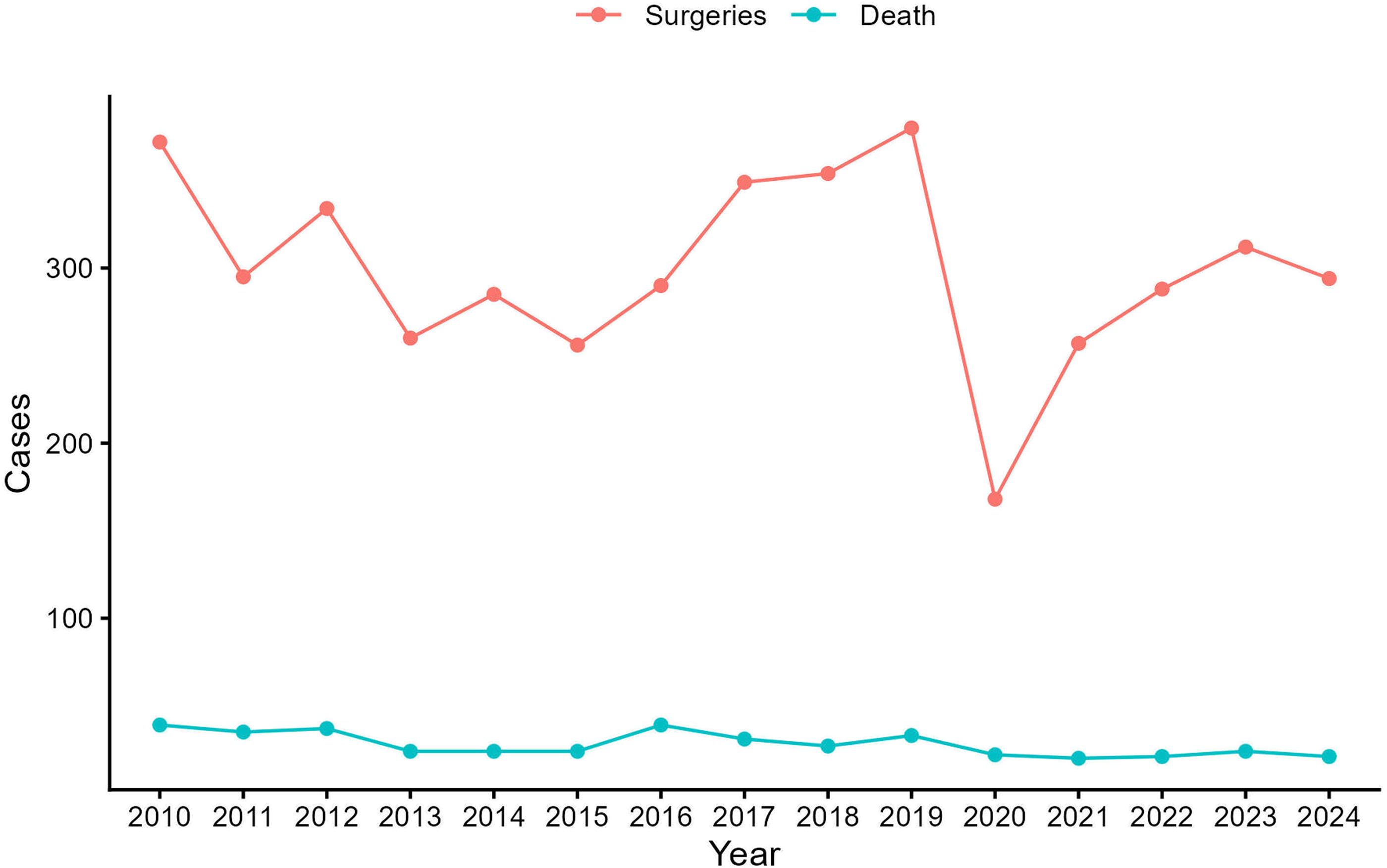
Evolution of number of surgeries and deaths from congenital heart disease in patients under 18 years from 2010 to 2024.
Cases from the State of Mexico, Mexico City, Michoacán, and Oaxaca were found to have the highest mortality, which fluctuated from 7.8% to 19.7% of deaths (33 to 83 deaths); also, patients from Veracruz, Hidalgo, Guanajuato, Puebla, and Querétaro showed mortality of 3.6% to 7.1% (15 to 30 deaths) (Figure 1). Although no differences in mortality were detected with respect to sex, significantly higher mortality was observed in children (n = 144/4494; 34.2%), infants (n = 124/421;29.5%), and neonates (n = 101/421; 24.0%) compared adolescents (n = 52/421; 12.4%) (P < .001) (Table 1). These deceased patients had a median weight (5.7 kg), height (65.0 cm), and BSA (0.3 m2) lower than patients who survived (14.0 kg, 100.0 cm, and 0.6 m2, respectively) (P < .001). Additionally, among the patients with CHD who died, 12/421 (2.9%) had Down syndrome and 11/421 (2.6%) had DiGeorge syndrome (Table 1).
When analyzing mortality according to the type of CHD, a higher number of deaths (n = 322/421; 76.5%) were found with cyanotic heart disease than acyanotic (n = 83/421; 19.7%) (P < .001) (Table 2). Furthermore, univentricular heart 13.3% (n = 56/421), LVOTO 10% (n = 42/421), pulmonary venous return anomalies 8.6% (n = 36/421), valvulopathies 5.5% (n = 23/421), left-to-right shunt heart diseases 5.2% (n = 22/421), and other types of CHD corresponded to 8.6% (n = 36/421) mortality (Table 2), with statistical significance (P < .001).
When the impact of mortality was evaluated according to the characteristics of the surgical procedures performed, it was observed that deaths occurred in elective operations in 298/421 (70.8%) patients, CPB in 323/421 (76.7%) with a median time of 147 min, and aortic cross-clamp time in 295/421 (70.1%) with a median time (83 min) higher than patients who survived (89 min and 54 min, respectively) (P < .001) (Table 3).
The surgical procedures contributing the highest absolute number of deaths were: modified Blalock–Taussig-Thomas shunt (n = 49/421; 11.6% of all deaths; procedure-specific mortality 11.1%), Jatene procedure (n = 32/421; 7.6% of all deaths; procedure-specific mortality 26.0%), surgical correction of TAPVC (n = 28/421; 6.7% of all deaths; procedure-specific mortality 8.4%), TOF repair with ventriculotomy and transannular patch (n = 21/421; 5.0% of all deaths; procedure-specific mortality 7.9%), pulmonary artery banding (n = 18/421; 4.3% of all deaths; procedure-specific mortality 20.0%), DORV repair (n = 16/421; 3.8% of all deaths; procedure-specific mortality 20.0%), extended coarctectomy (n = 15/421; 3.6% of all deaths; procedure-specific mortality 12.5%), fenestrated extracardiac Fontan (n = 15/421; 3.6% of all deaths; procedure-specific mortality 10.0%), and Rastelli procedure (n = 13/421; 3.1% of all deaths; procedure-specific mortality 21.3%). The Norwood procedure, although performed in only 7 patients, carried the highest procedure-specific mortality at 71.4% (5/7 deaths). By contrast, VSD closure (11/6122, 1.8%) and ASD closure (0.0%) showed the lowest procedure-specific mortality rates among high-volume procedures (P < .001). It is critical to note that the percentages of all deaths attributable to each procedure do not represent procedure-specific operative mortality rates; the latter are reported in Table 4 and Supplemental Table S1 and should be used for benchmarking comparisons (Table 4).
Discussion
Globally, the prevalence of CHD in children under 5 years of age exceeded 418 million cases in 2021, with a 56.2% reduction in associated mortality observed between 1990 and 2021. 8 In Spain, the reported incidence reaches 13.6 per 1000 live births 9 ; however, the absence of a population-based national registry in Mexico precludes direct epidemiological comparisons with these figures, and the present study should be interpreted as institutional rather than national data. With 4494 patients over 14 years, this constitutes the largest single-center series of pediatric CHD surgery reported from Mexico. The overall in-hospital mortality rate was 9.4% (421/4494). During 2020-2021, mortality transiently increased, coinciding with the COVID-19 pandemic. This likely reflects several compounding factors: restriction of elective surgical capacity in favor of COVID-19 patients, delayed referrals leading to more critically ill presentations, the physiological vulnerability of cyanotic CHD patients to SARS-CoV-2 infection, and limited PICU resources during peak pandemic surges.10,11 After 2022, a marked and sustained reduction was observed, reaching 7.1% in 2024, consistent with a smaller national series reporting a mean mortality of 7.5%. 7 Despite these results, when compared with international experience, notable differences persist. For example, Spain has reported an overall mortality rate of less than 3%, 12 highlighting the difficulty our country faces in reaching European standards. These discrepancies between Europe and Spain can be attributed, at least in part, to the diversity in the organization of healthcare systems, the lack of regionalization toward referral centers, and the lower availability of specialized infrastructure and resources. The factors associated with higher mortality in this cohort were early age, low weight and BSA, presence of cyanotic heart diseases, and syndromic history such as DiGeorge syndrome and Down syndrome, the latter being the most frequent genetic cause of CHD worldwide. 13 Similarly, we found that various factors related to the surgical procedure significantly impact mortality, such as the use and time of CPB and aortic cross-clamp time. These findings agree with what has been previously described in the international literature.14,15 The high vulnerability of neonates and infants, who account for more than 50% of deaths, emphasizes the need to strengthen prenatal detection and timely referral to specialized centers. Similarly, the high proportion of deaths attributable to heart and multiorgan failure highlights the need for standardized postoperative support protocols and universal access to pediatric critical care.16–20
The progress observed in the care of CHD in children under 18 years of age is the result of advances in medical technology, better surgical and intensive care practices, rehabilitation and long-term follow-up programs, as well as greater public awareness about these diseases. The regionalization of care has proven to be an effective strategy to reduce mortality and costs, as indicated by other studies. 21 Particularly, our analysis evidenced a relevant aspect: significant geographic inequality; most patients came from states close to Mexico City, which confirms the centralizing role of this hospital center and reflects the absence of consolidated regional networks. This concentration may limit timely access to children from distant states, decreasing the possibility of receiving specialized medical care in adequate time, which could contribute to differences in outcomes. Experiences from other Latin American countries have shown that centralized care models and national referral programs can promote more equitable access that allows for a reduction in mortality.5,6
Comparison of procedure-specific mortality rates with STS Congenital Heart Surgery Database benchmarks reveals important areas requiring targeted quality improvement. For low-complexity index procedures, ASD closure achieved 0.0% mortality (STS benchmark <0.5%), and VSD closure was 1.8% (STS ∼0.3%-1%), both within or near expected ranges. Total anomalous pulmonary venous connection repair (8.4%) was comparable to the STS range of 5% to 10%. However, substantial gaps were identified for several high-complexity procedures: the Jatene (arterial switch) procedure carried a procedure-specific mortality of 26.0% versus an STS benchmark of approximately 2% to 4%; the Norwood procedure reached 71.4% versus 15% to 20%; pulmonary artery banding was 20.0% versus 2% to 4%; the Damus–Kaye–Stansel procedure 60.0%; and the Rastelli procedure 21.3% versus 5% to 7%. Tetralogy of Fallot repair (7.9%), complete AVSD repair (6.4%), extended coarctectomy (12.5%), and the Fontan procedure (10.0%) also exceeded their respective STS reference ranges. These discrepancies likely reflect a combination of factors including late referral resulting in higher surgical risk at presentation, limited availability of specialized neonatal cardiac surgery infrastructure, case-mix heterogeneity not adjusted by complexity score, and resource constraints in postoperative critical care. It should be noted that RACHS-1 and STAT complexity scores are recorded in the RENACCAPE database; however, complete score data were not available for all patients in the current cohort, which precluded their systematic use for risk adjustment in this analysis. This represents a key limitation and underscores the need to prioritize complete and consistent complexity score documentation in future registry submissions. Notwithstanding, these data support the urgency of implementing risk-stratified quality monitoring and targeted capacity building, particularly in neonatal and single-ventricle surgery, at our institution.
In this regard, the data presented in this work emphasize the need to strengthen and expand RENACCAPE, incorporating more public and private hospitals, 22 and connecting it to international databases such as the World Database for Pediatric and Congenital Heart Surgery. 23 Likewise, it is necessary to establish public policies that promote early surgical care, standardization of management algorithms, and strengthening of interinstitutional referral networks. Due to the volume of care and accumulated experience, our center could become a promoter for improving care of patients with CHD in Mexico.
Conclusions
To our knowledge, this study represents the largest published single-center series of pediatric CHD surgery in Mexico, with an overall in-hospital mortality of 9.4% (421/4494) and a sustained downward trend in recent years. Univariate analysis identified the following variables significantly associated with mortality: early age (neonates and infants), low weight and BSA, cyanotic heart disease (particularly conotruncal defects and univentricular physiology), associated genetic syndromes (especially DiGeorge syndrome), and prolonged CPB and aortic cross-clamp times. These findings should be interpreted in the context of the study's observational, single-center design and the use of univariate rather than multivariate analysis; independent risk factor determination will require logistic regression modeling in future studies. Significant geographic inequity in access persists, with the large majority of patients originating from states proximal to Mexico City. These data support the need for targeted health policies to strengthen prenatal diagnosis, optimize interinstitutional referral networks, and standardize postoperative care protocols, informed by national registries such as RENACCAPE.
Supplemental Material
sj-docx-1-pch-10.1177_21501351261450531 - Supplemental material for Mortality and Risk Factors in Pediatric Cardiac Surgery for Congenital Heart Disease in Mexico
Supplemental material, sj-docx-1-pch-10.1177_21501351261450531 for Mortality and Risk Factors in Pediatric Cardiac Surgery for Congenital Heart Disease in Mexico by Yoana Leyva-López, José L. Cerano-Fuentes, Juan Calderón-Colmenero and Jorge L. Cervantes-Salazar in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Glossary of Abbreviations
Acknowledgments
We express our gratitude to the Office of Systematic Support for Advanced Research for the advice provided to successfully complete this work and obtain the Degree of Doctor in Public Health, as well as Dr Diego B. Ortega-Zhindón and Dr Yessica Charytin Hernandez-Garcia for their invaluable support in integrating the database.
Author Contributions
YLL and JLCS: conceptualization, methodology, and software; YLL and JLCS: data curation and writing—original draft preparation; YLL, JLCS, and JCC: visualization and investigation; JLCS and JLCF: supervision. JLCS and JCC: software and validation; YLL, JLCS, and JCC: writing—reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Declaration of Generative AI and AI-Assisted Technologies in the Article Preparation Process
During the preparation of this work, the authors used Claude (Anthropic) in order to assist with language editing, grammar refinement, and structural organization of the manuscript text. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.