
Abstract
Objectives
Extracorporeal Membrane Oxygenation (ECMO) is associated with high risks of bleeding and clotting. While traditional anticoagulants like heparin and bivalirudin target the coagulation cascade, prostaglandins including PGE1 and PGI2 may offer adjunctive platelet inhibition. This study evaluated whether prostaglandin use modifies the risk of severe bleeding or clotting events in pediatric ECMO patients.
Material and Methods
We used the Pediatric Health Information System database from 2004 to 2025, and included children supported with ECMO. Primary outcomes were severe bleeding and clotting events. Generalized linear mixed model regressions adjusted for site, patient and ECMO data, and pulmonary hypertension.
Results
A total of 22,061 pediatric ECMO patients were included. Pulmonary hypertension was present in 12.4% (2736/22,061). PGE1 and PGI2 were independently associated with increased risk of pulmonary hemorrhage (PGE1: adjusted OR 1.24, P = .003; PGI2: adjusted OR 1.21, P = .047). Conversely, neither PGE1 nor PGI2 were independently associated with intracranial hemorrhage (PGE1: adjusted OR 1.01, P = .92; PGI2: adjusted OR 0.96, P = .79), stroke (PGE1: adjusted OR 1.02, P = .84; PGI2: adjusted OR 0.88, P = .38), or other bleeding or thrombotic events.
Conclusion
In this large multicenter cohort of more than 22,000 pediatric ECMO patients, neither PGE1 nor PGI2-modulated anticoagulation conferred measurable protection against the major bleeding or clotting complications.
Introduction
Extracorporeal membrane oxygenation (ECMO) provides life-saving support for children with severe cardiac or respiratory failure, with more than 1500 newborns and 2500 pediatric patients supported worldwide each year. 1 Although essential for survival in these critically ill populations, ECMO profoundly disrupts normal hemostatic balance and places patients at substantial risk for both major bleeding and thrombosis.2,3 Mitigating these complications remains one of the central challenges in pediatric ECMO management. Contemporary anticoagulation practices rely largely on unfractionated heparin or bivalirudin, 4 agents that primarily target the plasma coagulation cascade and do not directly address platelet dysfunction, a key contributor to clot formation in the ECMO circuit.5,6 This therapeutic gap highlights the need to explore alternative or adjunctive approaches that more comprehensively modulate hemostasis and may ultimately improve patient outcomes.
Both PGE1 and PGI2 inhibit platelet function by elevating intracellular cAMP levels through G-protein coupled receptor activation, which triggers protein kinase A (PKA)-mediated phosphorylation of multiple substrate proteins that suppress platelet activation, adhesion, and aggregation. 7 However, they differ significantly in their receptor selectivity, potency, and duration of action. PGI2 acts primarily through the IP receptor with high affinity and is more potent than PGE1 as an inhibitor of platelet aggregation against most agonists (ADP, adrenaline, collagen). In contrast, PGE1 exhibits dual receptor activity, binding both stimulatory IP receptors and inhibitory EP3 receptors, with higher affinity for EP3 than for IP receptors, creating a concentration-dependent balance between inhibitory and potentially pro-aggregatory effects. Both prostaglandins are widely used in children with pulmonary hypertension and have an established safety record in this population. 8 Unlike anticoagulants that impair coagulation factors, PGE1 and PGI2 modulate platelet function, making them promising adjuncts in ECMO anticoagulation.
Existing evidence suggests potential benefits of prostaglandin-based anticoagulation. A meta-analysis of 17 studies in critically ill patients receiving continuous renal replacement therapy demonstrated that PGI2-based strategies significantly reduced bleeding compared with traditional anticoagulation regimens. 9 Moreover, a randomized, double-blind, placebo-controlled phase II trial in 114 adult ECMO patients showed that adding PGE1 to heparin was safe and was associated with fewer bleeding and thrombotic events. 10 Despite these promising results, the therapeutic implications of prostaglandins in pediatric ECMO remain largely unexamined. And in practice, prostaglandins may be introduced to mitigate circuit thrombosis despite therapeutic anticoagulation rather than primarily to reduce bleeding risk.
To address this knowledge gap, the goal of this study is to evaluate whether prostaglandin-modulated anticoagulation is associated with improved bleeding and thrombotic outcomes in critically ill children supported with ECMO. By defining the potential clinical benefits of prostaglandins, this study aims to inform whether PGI2 or PGE1 should be considered as adjuncts to standard anticoagulation strategies in pediatric ECMO.
Material and Methods
Study Design and Data Source
Data for this study were obtained from the Pediatric Health Information System (PHIS), an administrative database that contains inpatient, emergency department, ambulatory surgery and observation encounter-level data from not-for-profit, tertiary care pediatric hospitals in the United States. These hospitals are affiliated with the Children's Hospital Association (Lenexa, KS, USA). Data quality and reliability are assured through a joint effort between the Children's Hospital Association and participating hospitals. For the purposes of external benchmarking, participating hospitals provide discharge/encounter data including demographics, diagnoses, and procedures. Nearly all of these hospitals also submit resource utilization data (eg, pharmaceuticals, imaging, and laboratory) into PHIS. Data are de-identified at the time of data submission, and data are subjected to a number of reliability and validity checks before being included in the database. For this study, data from 52 hospitals were included.
Study Population
All patients who were 0 to 18 years of age and had an ECMO flag recorded in PHIS from January 1, 2004, through April 3, 2025, were eligible for inclusion. We restricted the cohort to patients who received unfractionated heparin and/or bivalirudin during ECMO support.
Exposure Definitions
Anticoagulation strategies were classified into three groups: (1) standard anticoagulation, defined as unfractionated heparin and/or bivalirudin alone; (2) PGE1-modulated anticoagulation, defined as standard anticoagulation with the addition of intravenous prostaglandin E1; and (3) PGI2-modulated anticoagulation, defined as standard anticoagulation with the addition of intravenous prostaglandin I2.
For prostaglandins, data on duration, timing of initiation relative to ECMO support, and route of administration (intravenous or inhaled) were extracted. Prostaglandin exposure in PHIS reflects pharmacy billing for intravenous formulations; inhaled epoprostenol is not captured within the same medication categories in this dataset and was not considered in this analysis.
Covariates
Patient-level covariates included age (subsequently categorized as neonate < 28 days vs older children), sex, diagnoses, pulmonary hypertension diagnosis, and comorbid conditions such as congenital heart disease, respiratory failure, or inherited coagulopathies. ECMO-related variables included ECMO cannulation site (central vs peripheral vs unknown) and ECMO mode (veno-arterial vs veno-venous vs unknown). Pulmonary hypertension was treated as a key confounder, given the established use of prostaglandins in this condition.
Outcomes
The primary outcomes of the study were bleeding and clotting events, identified through diagnostic codes in PHIS. Intracranial hemorrhage was defined using ICD-9 codes 430, 431, and 432.9, as well as ICD-10 codes I60xx, I61x, and I62xx. Stroke was defined using ICD-9 codes 434.xx and ICD-10 codes I634xx (see supplemental material; Table 1). Overall bleeding complications were defined as intracranial, pulmonary, and/or gastrointestinal hemorrhages. Overall clotting complications were defined as limb ischemia, pulmonary embolism, and/or stroke. Secondary outcomes included hospital length of stay, measured in days from admission to discharge; ECMO duration, defined as the number of days with an ECMO flag; and in-hospital mortality, defined as death occurring during the same hospitalization. The tertiary outcome was total hospital charges adjusted by the Center for Medicare & Medicaid Services (CMS) price index for the hospital's location, as reported in PHIS, which served as a proxy for financial impact.
Demographics.
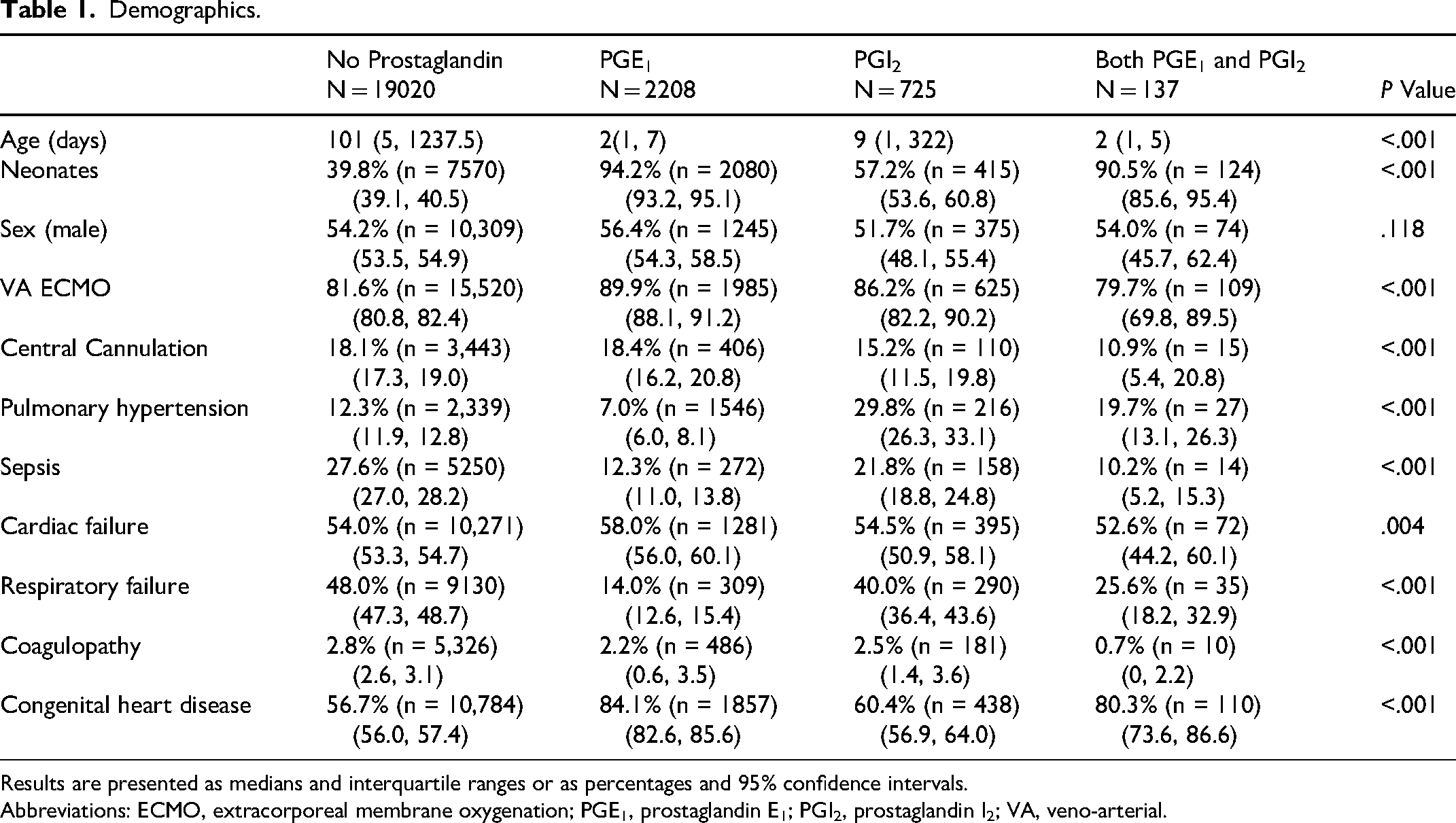
Results are presented as medians and interquartile ranges or as percentages and 95% confidence intervals.
Abbreviations: ECMO, extracorporeal membrane oxygenation; PGE1, prostaglandin E1; PGI2, prostaglandin I2; VA, veno-arterial.
Statistical Analysis
Descriptive analyses were conducted to characterize patient demographics, ECMO characteristics, and patterns of prostaglandin use. Continuous variables were summarized as median with interquartile range (IQR). Categorical variables were summarized as percentages with 95% confidence intervals (95% CIs).
To assess the independent association of PGE1 and PGI2 with clinical outcomes, multivariate analyses were conducted. Generalized Linear Mixed Models (GLMMs) were fitted with hospital as a random effect to account for clustering by site. Prostaglandin exposure was the primary independent variable, with adjustment for age (categorized as neonate < 28 days vs older children), ECMO mode, cannulation site, anticoagulation medication (heparin and/or bivalirudin), pulmonary hypertension, comorbidities (cardiac failure, congenital heart disease, respiratory failure, sepsis, coagulopathy). GLMM results were represented graphically with forest plots of the adjusted odds ratios and 95% CI. Because mortality timing varied substantially across patients, Kaplan–Meier survival curves were generated to compare hospital time-to-death across the four prostaglandin exposure groups, with differences evaluated using the log-rank test and median survival times reported. Temporal trends in prostaglandin adoption were assessed by stratifying use across calendar years.
All statistical tests were two-tailed, with a significance level of P < .05. Analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria) and SPSS 31 (IBM Corp., Armonk, NY, USA).
Results
Population
A total of 22,061 pediatric patients who received ECMO were included in the study. The median age at initiation was 50 days (IQR 3, 842). Most patients (82.0% [18,090/22,061], 95% CI 81.9, 83.4) were supported with veno-arterial ECMO (the remaining 18.0% [3971/22,061] of patients were supported with veno-venous ECMO), and 18.0% (3971/22,061) (95% CI 17.3, 18.8) underwent central cannulation. Pulmonary hypertension was present in 12.4% (2736/22,061) (95% CI 12.0, 12.9). The most common comorbidities and clinical conditions were congenital heart disease (59.7% [13,170/22,061], 95% CI 59.0, 60.3), cardiac failure (54.4% [12,001/22,061], 95% CI 53.7, 55.1), and respiratory failure (44.2% [9751/22,061], 95% CI 43.6, 44.9), sepsis (25.8% [5692/22,061], 95% CI 25.2, 26.4), and coagulopathies (2.6% [5,736/22,061], 95% CI 2.4, 2.8). Most patients were treated exclusively with heparin (86.8% [19,149/22,061], 95% CI 86.3, 87.3). A very small proportion received bivalirudin as their sole anticoagulant (0.16% [353/22,061], 95% CI 0.11, 0.22), and 11.2% (2471/22,061] of patients (95% CI 10.8, 11.7) received both heparin and bivalirudin during their course of care. Only a small minority of patients (381/22,061, 1.7%) did not receive unfractionated heparin or bivalirudin during ECMO support; among these, 7/381 (1.8%) received PGE1 and 1/381 (0.3%) received PGI2. PGE1 was administered in 10.6% (2338/22,061) of patients (95% CI 10.2, 11.0), and PGI2 in 3.8% (838/22,061 (95% CI 3.6, 4.1). Table 1 describes the population according to the use of prostaglandins, and Figure 1 shows the temporal trend of PGE1 and PGI2 over time.
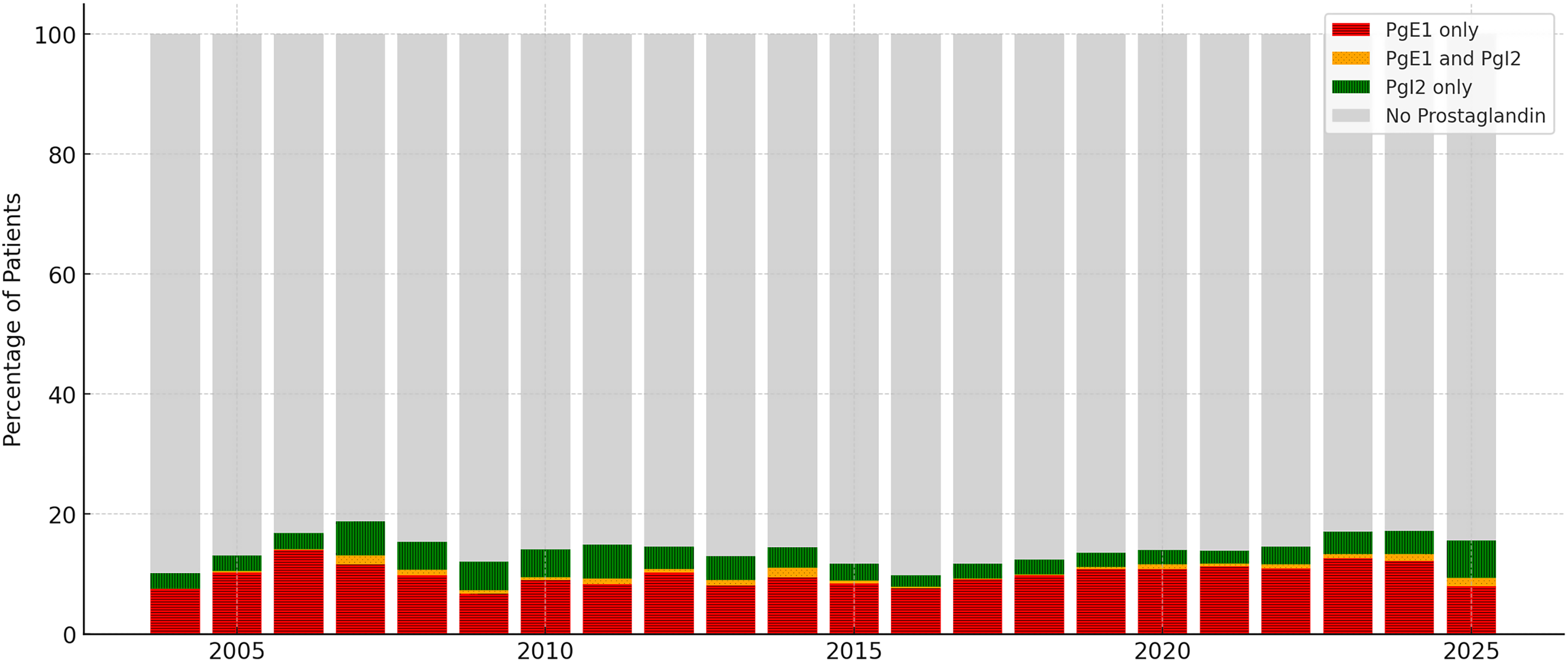
Annual proportion of ECMO patients receiving prostaglandins. Stacked bars show the percentage of patients treated with PGE1 only, PGE1 and PGI2, PGI2 only, and no prostaglandin for each ECMO start year. Abbreviation: ECMO, extracorporeal membrane oxygenation.
As shown in Figure 2, among patients treated with prostaglandins, most did not have a documented diagnosis of pulmonary hypertension. Specifically, 92.2% (2036/2208) of patients who received PGE1 had no pulmonary hypertension (95% CI 91.1, 93.3), and 71.8% (521/725) of those who received PGI2 were not diagnosed with pulmonary hypertension (95% CI 68.8, 74.8). Conversely, among patients with pulmonary hypertension, the large majority (85.6%, 16,281/19,020) did not receive either PGE1 or PGI2 (95% CI 84.3, 86.9).
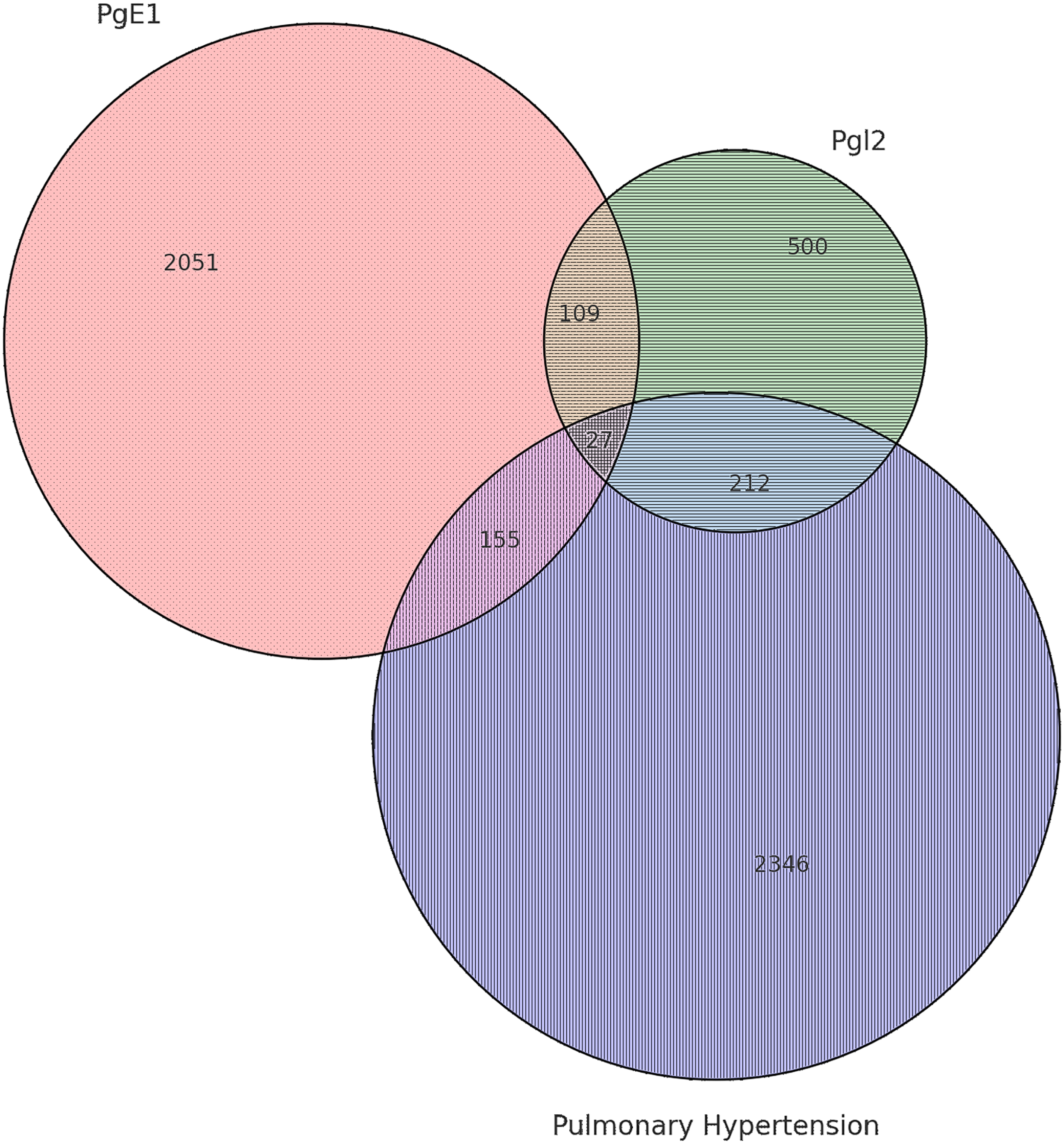
Venn diagram illustrating the overlap between pulmonary hypertension, PGE1 administration, and PGI2 administration among pediatric patients supported with ECMO. Proportional areas represent the number of patients in each group and overlap category. Abbreviation: ECMO, extracorporeal membrane oxygenation.
PGE1
Adjusting for site effect, and patient and ECMO characteristics, PGE1 was not independently associated with intracranial hemorrhage (adjusted OR 1.01, 95% CI 0.79, 1.29, P = .92; Figure 3A) or gastrointestinal hemorrhage (adjusted OR 0.97, 95% CI 0.52, 1.81, P = .93; Table 2). In contrast, PGE1 infusion was independently associated with an increased risk of pulmonary hemorrhage (adjusted OR 1.24, 95% CI 1.08, 1.43, P = .003; Table 2). PGE1 was not associated with ischemic stroke (adjusted OR 1.02, 95% CI 0.82, 1.28, P = .84; Figure 3B), pulmonary embolism (adjusted OR 0.57, 95% CI 0.27, 1.19, P = .14; Table 2), or arterial thromboembolic events (adjusted OR 0.91, 95% CI 0.74, 1.11, P = .34; Table 2).
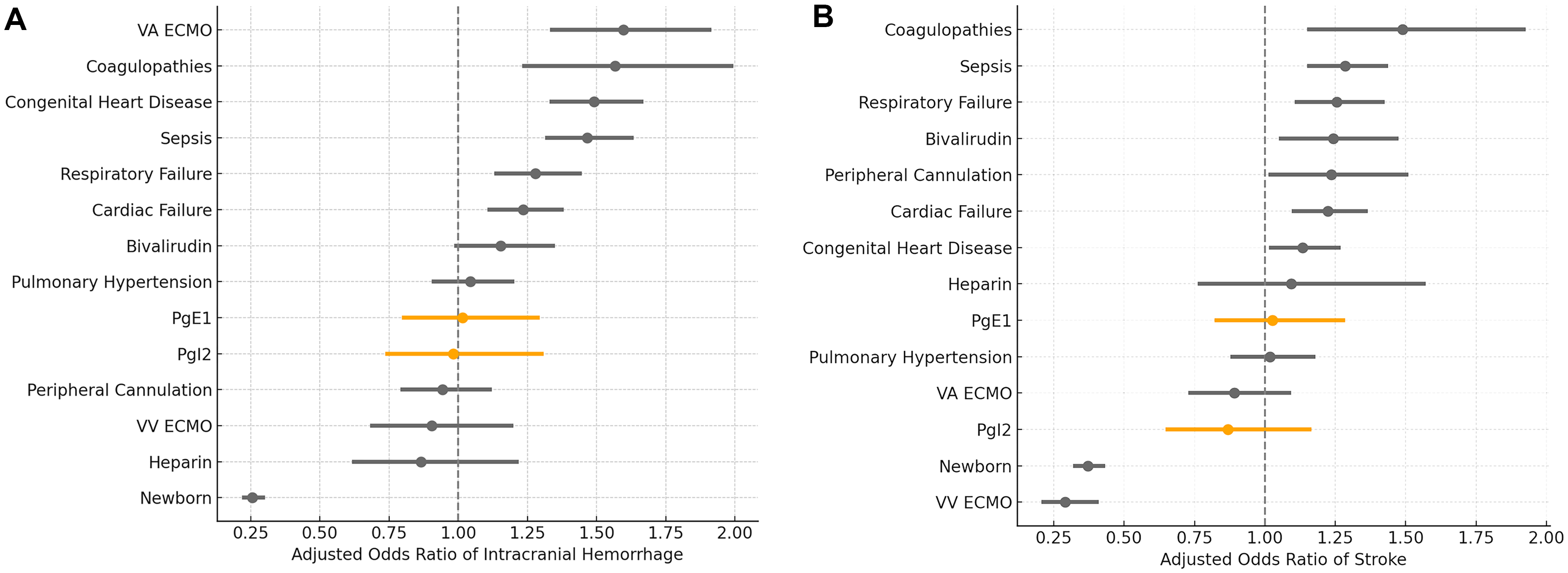
Forest plots of GLMM of intracranial hemorrhage (A) and ischemic stroke (B).
Outcomes Associated with Prostaglandin Infusion on ECMO.
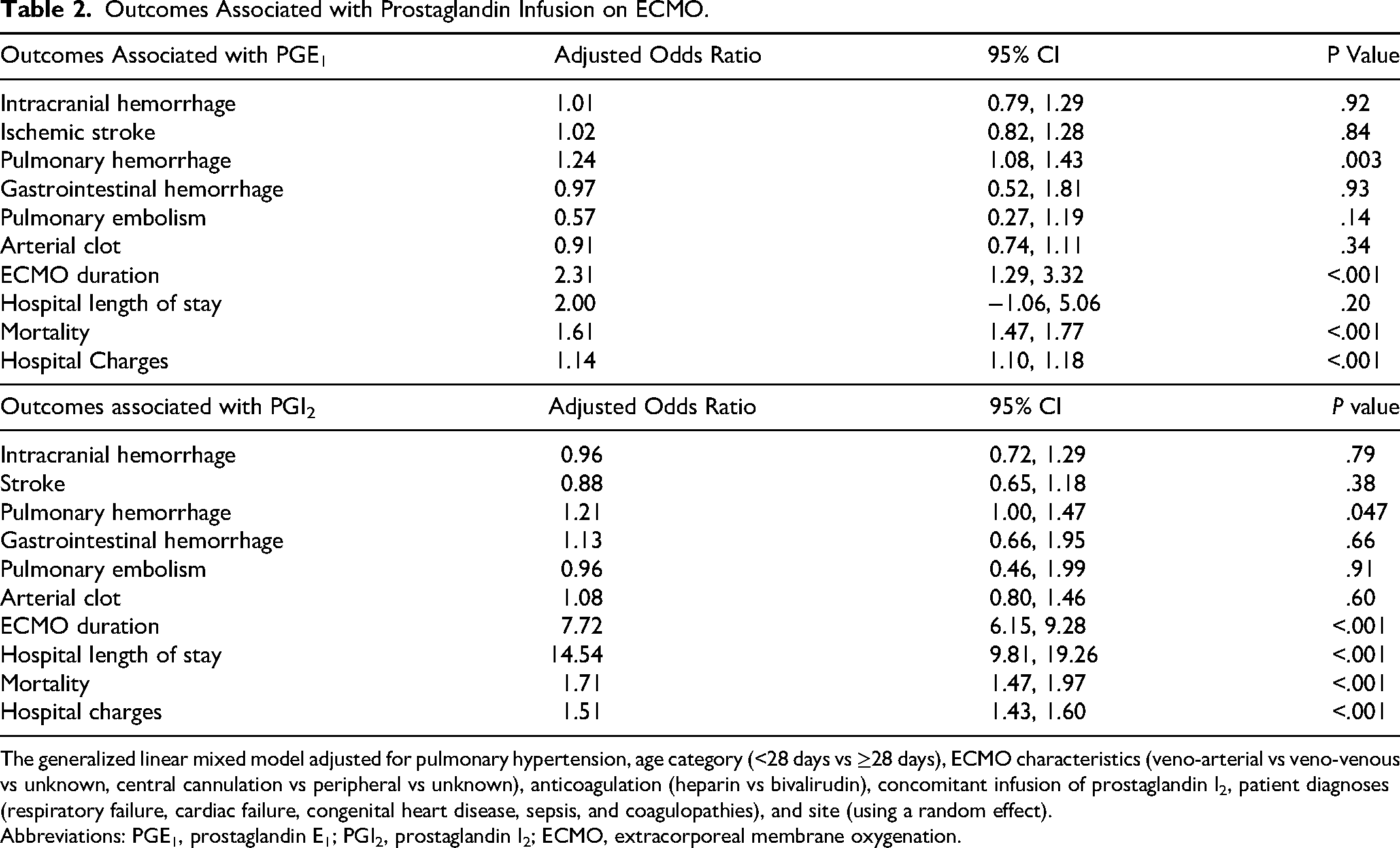
The generalized linear mixed model adjusted for pulmonary hypertension, age category (<28 days vs ≥28 days), ECMO characteristics (veno-arterial vs veno-venous vs unknown, central cannulation vs peripheral vs unknown), anticoagulation (heparin vs bivalirudin), concomitant infusion of prostaglandin I2, patient diagnoses (respiratory failure, cardiac failure, congenital heart disease, sepsis, and coagulopathies), and site (using a random effect).
Abbreviations: PGE1, prostaglandin E1; PGI2, prostaglandin I2; ECMO, extracorporeal membrane oxygenation.
PGI2
PGI2 infusion was not independently associated with intracranial hemorrhage (adjusted OR 0.96, 95% CI 0.72, 1.29, P = .79; Figure 3A) or gastrointestinal hemorrhage (adjusted OR 1.13, 95% CI 0.66, 1.95, P = .66; Table 2). PGI2 infusion was associated with a higher risk of pulmonary hemorrhage (adjusted OR 1.21, 95% CI 1.00, 1.47, P = .047; Table 2), but was not associated with pulmonary embolism (adjusted OR 0.96, 95% CI 0.46, 1.99, P = .91) or arterial thromboembolic events (adjusted OR 1.08, 95% CI 0.80, 1.46, P = .60; Table 2). PGI2 was also not associated with ischemic stroke (adjusted OR 0.88, 95% CI 0.65, 1.18, P = .38; Figure 3B).
Duration of ECMO
The median duration of ECMO was 5 days (IQR 1, 9) in patients without prostaglandins, 6 days (IQR 2, 12) in patients who received PGE1, 10 days (IQR 5, 21.75) in patients who received PGI2, and 12 days (IQR 6, 23) in patients who received both (P < .001).
Adjusting for site effect, and patient and ECMO characteristics, PGE1 and PGI2 were independently associated with increased duration of ECMO (adjusted mean difference 2.31 days, 95% CI 1.29, 3.32, P < .001; and adjusted mean difference 7.72 days, 95% CI 6.15, 9.28, P < .001, respectively).
Length of Stay
The median hospital length of stay was 35 days (IQR 17, 69) in patients without prostaglandins, 35 days (IQR 16, 78) in patients who received PGE1, 49 days (IQR 25, 94.75) in patients who received PGI2, and 35 days (IQR 16, 68.5) in patients who received both (P < .001).
Adjusting for site effect, and patient and ECMO characteristics, PGI2, but not PGE1, was independently associated with increased hospital length of stay (adjusted mean difference for PGI2: 14.54 days, 95%%CI 9.81, 19.26, P < .001; and adjusted mean difference for PGE1: 2.00 days, 95% CI −1.06, 5.06, P = .20).
Mortality
The hospital mortality rate was 39.2% (7456/19,020) in patients without prostaglandins, 47.9% (1058/2208) in patients who received PGE1, 51.3% (372/725) in patients who received PGI2, and 60.6% (83/137) in patients who received both. The median survival time was 120 days in patients without prostaglandins, 93 days in those who received PGE1, 97 days in those who received PGI2, and 47 days in patients who received both (log-rank P < .001, Figure 4).
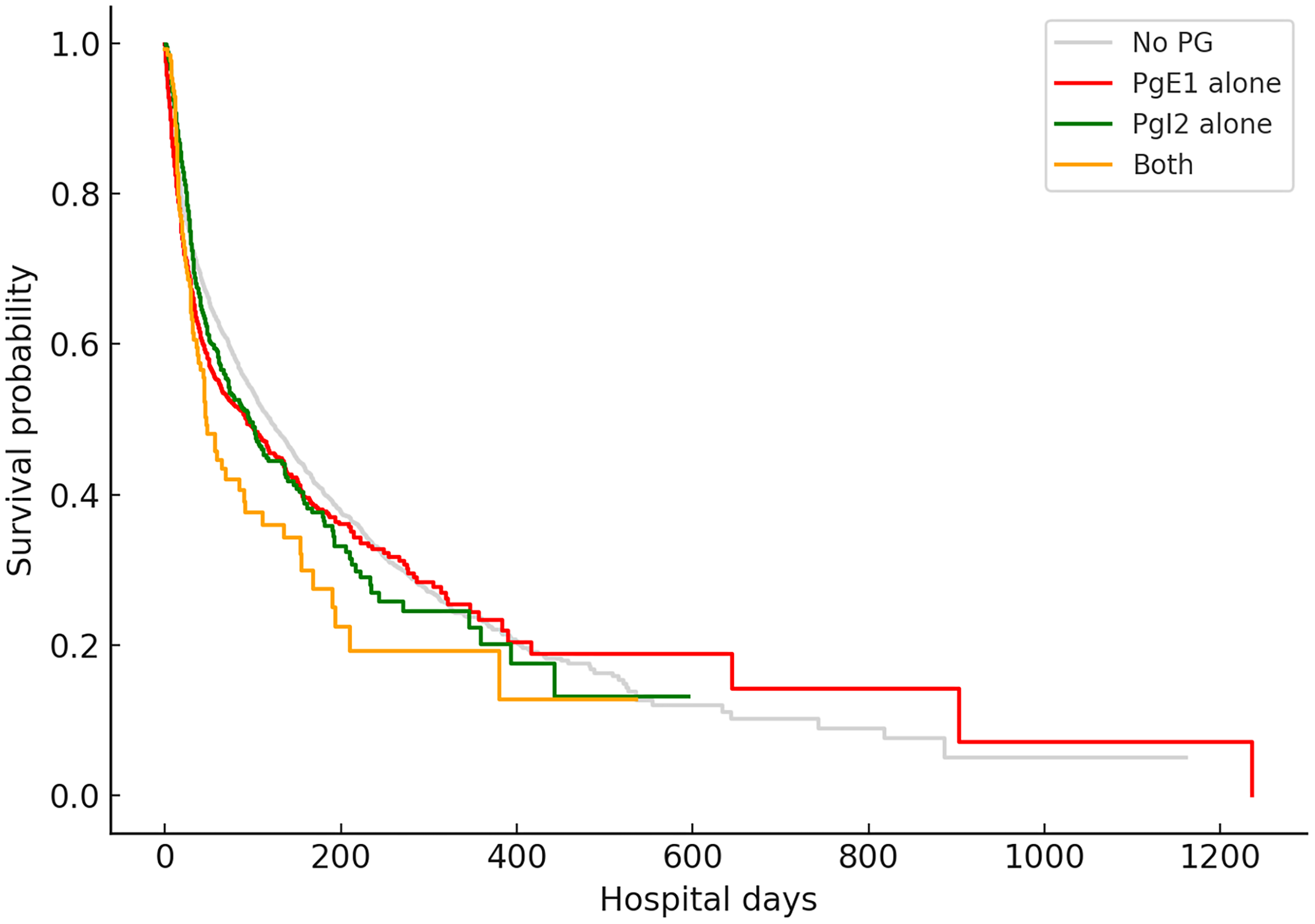
Kaplan–Meier curves for hospital survival stratified by prostaglandin exposure. Patients were grouped into four categories: no prostaglandin exposure (light gray), PGE1 alone (red), PGI2 alone (green), and combined PGE1 plus PGI2 therapy (orange). Time was measured in hospital days from admission to discharge or death. Survival distributions differed significantly across the four groups (log-rank P < .001).
Adjusting for site effect, and patient and ECMO characteristics, PGE1 and PGI2 were independently associated with increased risk of death (adjusted OR 1.61, 95% CI 1.47, 1.77, P < .001; and adjusted OR 1.71, 95% CI 1.47, 1.97, P < .001, respectively).
Costs
The median hospital charges were $4.3 M (IQR $2.3 M; $8.2 M) in patients without prostaglandins, $4.8 M (IQR $2.7 M; $9.2 M) in patients who received PGE1, $7.1 M (IQR $3.7 M; $12.1 M) in patients who received PGI2, and $6.3 M (IQR $3.5 M; $12.4 M) in patients who received both (P = .001).
Adjusting for site effect, and patient and ECMO characteristics, PGE1 and PGI2 were independently associated with higher total hospital charges (1.14 times higher total hospital charges, 95% CI 1.10, 1.18, P < .001; and 1.51 times higher total hospital charges, 95% CI 1.43, 1.60, P < .001, respectively).
Discussion
In this large, multicenter cohort of more than 22,000 pediatric ECMO patients, neither PGE1 nor PGI2 was associated with reductions in major bleeding or thrombotic complications. Both prostaglandins showed no independent association with intracranial hemorrhage, gastrointestinal hemorrhage, ischemic stroke, pulmonary embolism, or arterial thromboembolism after adjustment for patient and ECMO characteristics. However, each was associated with a modest but statistically significant increase in pulmonary hemorrhage. Beyond bleeding and clotting outcomes, prostaglandin exposure was consistently associated with markers of greater illness severity, including longer ECMO runs, longer hospital stays (for PGI2), higher total hospital charges, and higher adjusted mortality. These findings suggest that, in contemporary pediatric ECMO practice as captured in PHIS, prostaglandin-modulated anticoagulation does not confer measurable protection against the major hemorrhagic or thrombotic complications. However, in clinical practice, prostaglandins may be initiated in response to refractory circuit thrombosis or high clot burden despite therapeutic anticoagulation, which would introduce confounding by indication and bias associations toward worse outcomes.
The observed association between prostaglandin exposure and increased mortality warrants careful interpretation. In our cohort, the median time to death exceeded three months among patients receiving prostaglandins, whereas the median ECMO duration was less than 2 weeks. This temporal separation suggests that excess mortality may reflect the underlying disease severity prompting prostaglandin use rather than a direct harmful effect of prostaglandins themselves. This interpretation is reinforced by the absence of an association between prostaglandin exposure and major hemorrhagic or thrombotic complications, events that typically drive ECMO-related mortality, apart from a modest increase in pulmonary hemorrhage. An additional consideration is the potential underreporting of pulmonary hypertension in administrative datasets. As shown in our cohort, most patients who received prostaglandins did not have a documented diagnosis of pulmonary hypertension. It is plausible that clinicians initiated prostaglandins for suspected pulmonary hypertension that was not formally coded. If a substantial proportion of prostaglandin recipients had unrecognized or undocumented pulmonary hypertension, this would explain their markedly longer ECMO runs, prolonged hospitalization, and increased mortality, since pulmonary hypertension itself is strongly associated with more complex physiology, slower recovery, and greater risk of late deterioration. Under this interpretation, prostaglandin use may serve as a surrogate marker for an unmeasured severity phenotype rather than a contributor to excess mortality. Prior evidence from the only randomized controlled trial to date, conducted in adults on venovenous ECMO, similarly demonstrated a numerically higher mortality in the PGE1 arm (42% vs 17% mortality at 90 days) that did not reach statistical significance (P = .11). 10 Taken together, these findings indicate that although a causal effect of prostaglandins on mortality cannot be fully excluded, the more plausible explanation is confounding by indication, with prostaglandins preferentially administered to patients with more complex physiology or more severe underlying illness. Similarly, the absence of an observed reduction in thrombotic complications should be interpreted with caution. In clinical practice, prostaglandins may be initiated in response to evolving or established circuit thrombosis despite therapeutic anticoagulation. As such, reverse causation and confounding by indication may obscure a potential protective effect, particularly if prostaglandins are introduced after thrombotic processes have already begun. This raises the possibility that earlier initiation of prostaglandins, prior to the development of thrombotic complications, may yield different results, as suggested by randomized data in adults on VV-ECMO. 10
For clinicians interested in using prostaglandins specifically as adjuncts to anticoagulation on ECMO, safety remains a central concern. Prostaglandins inhibit platelet function, and some may worry that adding them to standard heparin or bivalirudin regimens could heighten bleeding risk. Although we did not observe an increase in major intracranial or gastrointestinal hemorrhage, the modest increase in pulmonary hemorrhage and the association with increased mortality underscore that definitive conclusions regarding safety or efficacy cannot be drawn from these data. This is consistent with the only randomized controlled trial to date, conducted in adults on venovenous ECMO, which found that adding PGE1 to heparin was associated with fewer overall bleeding and thrombotic complications compared with placebo. 10 It is important to acknowledge that we cannot determine whether bedside clinicians adjusted anticoagulation doses when prostaglandins were initiated. These findings should therefore be interpreted as hypothesis-generating rather than confirmatory with respect to safety.
This study has several limitations inherent to retrospective analyses using administrative datasets. First, PHIS does not capture the specific indication for ECMO, as diagnostic codes list diagnoses without clarifying which condition led to cannulation. The dataset also lacks granular clinical information such as laboratory values (including platelet counts, coagulation profiles, and anti-Xa levels). It further does not include medication dosing, including prostaglandin E1 dose, whose pro- and anti-platelet effects are dose dependent. Misclassification is possible because billing data may not fully reflect actual medication administration or duration, and coding errors may affect identification of bleeding or thrombotic events. We were also unable to identify patients receiving prostaglandins specifically for maintenance of ductal arteriosus patency or right ventricular decompression, populations that may carry distinct risks for pulmonary hemorrhage and confound observed associations. In addition, missing data for some variables, such as comorbidities, may limit the ability to adjust for confounding. Although analyses were adjusted for pulmonary hypertension, this diagnosis was uncommon among patients receiving prostaglandins, potentially contributing to the observed association with mortality. Because pulmonary hemorrhage was defined using administrative ICD codes, milder or transient bleeding events may not have been captured, and misclassification remains possible. PHIS does not allow determination of the clinical indication or timing of prostaglandin initiation relative to ECMO cannulation, and diagnostic codes reflect conditions documented at any point during hospitalization rather than necessarily at the time prostaglandins were started. In addition, administrative diagnostic codes cannot distinguish the severity of pulmonary hemorrhage, although there is substantial clinical variation between minimal bloody secretions in an endotracheal tube and life-threatening pulmonary bleeding. PHIS also captures only major complications, which means less severe events (such as chest tube output or bleeding at the cannulation site) are not recorded, as PHIS does not contain specific diagnostic codes for cannulation site bleeding or quantitative measures such as chest tube output, limiting our ability to assess less severe but clinically relevant bleeding complications, and potentially leading to underestimation of outcome rates. PHIS also does not provide reliable temporal linkage between surgical procedures and ECMO cannulation, preventing adjustment for the timing of cardiac surgery relative to prostaglandin exposure. As with all retrospective observational studies, causal inference cannot be drawn, and unmeasured confounders and treatment-selection biases may influence observed associations. Nonetheless, the inclusion of more than 20,000 patients across multiple centers supports the generalizability of these findings.
In conclusion, the role of prostaglandins as adjuncts to anticoagulation during ECMO remains uncertain. In this large multicenter analysis, prostaglandin E1 and prostaglandin I2 were not associated with reductions in major bleeding or thrombotic events. Associations with longer ECMO runs, prolonged hospitalization, and higher mortality likely reflect confounding by indication rather than direct harm. Given the observational design, potential for confounding by indication, and absence of demonstrated efficacy in reducing thrombotic events, these findings should not be interpreted as evidence supporting routine prostaglandin use as adjunct anticoagulation in pediatric ECMO. Prospective studies with standardized anticoagulation protocols and granular physiologic data are needed to determine whether prostaglandins confer benefit in selected patient subgroups.
Supplemental Material
sj-pdf-1-pch-10.1177_21501351261453052 - Supplemental material for Prostaglandin Administration and Outcomes in Children on Extracorporeal Membrane Oxygenation
Supplemental material, sj-pdf-1-pch-10.1177_21501351261453052 for Prostaglandin Administration and Outcomes in Children on Extracorporeal Membrane Oxygenation by Weidi Xiao, Nedaa Aldairi, Brian S. Marcus, Matthew Weiss, Allison S. Cowl, Marissa Moncata, Akash Deep and Oliver Karam in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Author Contributions
Weidi Xiao and Oliver Karam developed the initial study protocol. All authors contributed to protocol refinement and approved the final version. Marissa Moncata performed data extraction. Statistical analyses were conducted by Weidi Xiao and Oliver Karam. The initial manuscript draft was written by Weidi Xiao and Oliver Karam, and all authors critically reviewed, revised, and approved the final manuscript.
Ethical Considerations
The protocol was submitted to Yale's IRB (#2000040321), and determined to be exempt because it used de-identified data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Accessibility
This dataset is available from the Children's Hospital Association.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.