
Abstract
We present a unique case of spontaneous chordal rupture in a young infant with Down syndrome and unrepaired transitional atrioventricular septal defect. This resulted in abrupt onset of severe left atrioventricular valve regurgitation, cardiogenic shock, and multiorgan dysfunction. Our case highlights the need for a high index of suspicion for a ruptured chord in a young infant presenting with acute onset of pulmonary edema.
Introduction
Most common and well-recognized causes of mitral chordae tendineae rupture in adults are bacterial endocarditis, rheumatic valvar disease, trauma, systemic connective tissue disorders, and abnormalities of mitral valve (MV) apparatus.1,2 Cases have also occurred in association with thyrotoxic heart disease 3 and hypertrophic cardiomyopathy. 4 In infants, Kawasaki disease, maternally derived anti-Sjogren Syndrome Type A and Type B (SSA and SSB) antibodies, myxoid change of MV, and lymphocytic endocarditis are potential causes of MV chordae tendinea rupture. 5 Spontaneous, idiopathic rupture of the chordae tendinae remains a rare entity. We report a case of spontaneous left atrioventricular (AV) valve chordae tendineae rupture in a patient with Down syndrome (DS) and unrepaired congenital heart disease.
Case
We report the case of a 5-month-old Caucasian female with DS and transitional AV septal defect with a large primum atrial septal defect (ASD), small to moderate inlet ventricular septal defect (VSD) restricted by AV valve tissue, and mild right and left atrioventricular valve regurgitation (AVVR). She was being followed as an outpatient (Figure 1) and presented with a one day history of decreased feeding, worsening tachypnea, and increased sleepiness. Initial assessment in the emergency department was significant for decompensated shock with hypotension, sinus tachycardia, and severe respiratory distress. Laboratory results revealed metabolic acidosis, elevated troponin T [229 ng/L (normal 0–93 ng/L)], N-Terminal Pro-B-type Natriuretic Peptide (>150,000 pg/ml), and liver enzymes (Aspartate Aminotransferase and Alanine Aminotransferase 172 and 118 U/L) as well as acute kidney injury (Creatinine 1.09 mg/dl). Chest X-Ray showed worsening cardiomegaly and pulmonary edema. She was resuscitated, intubated, and started on vasopressors.
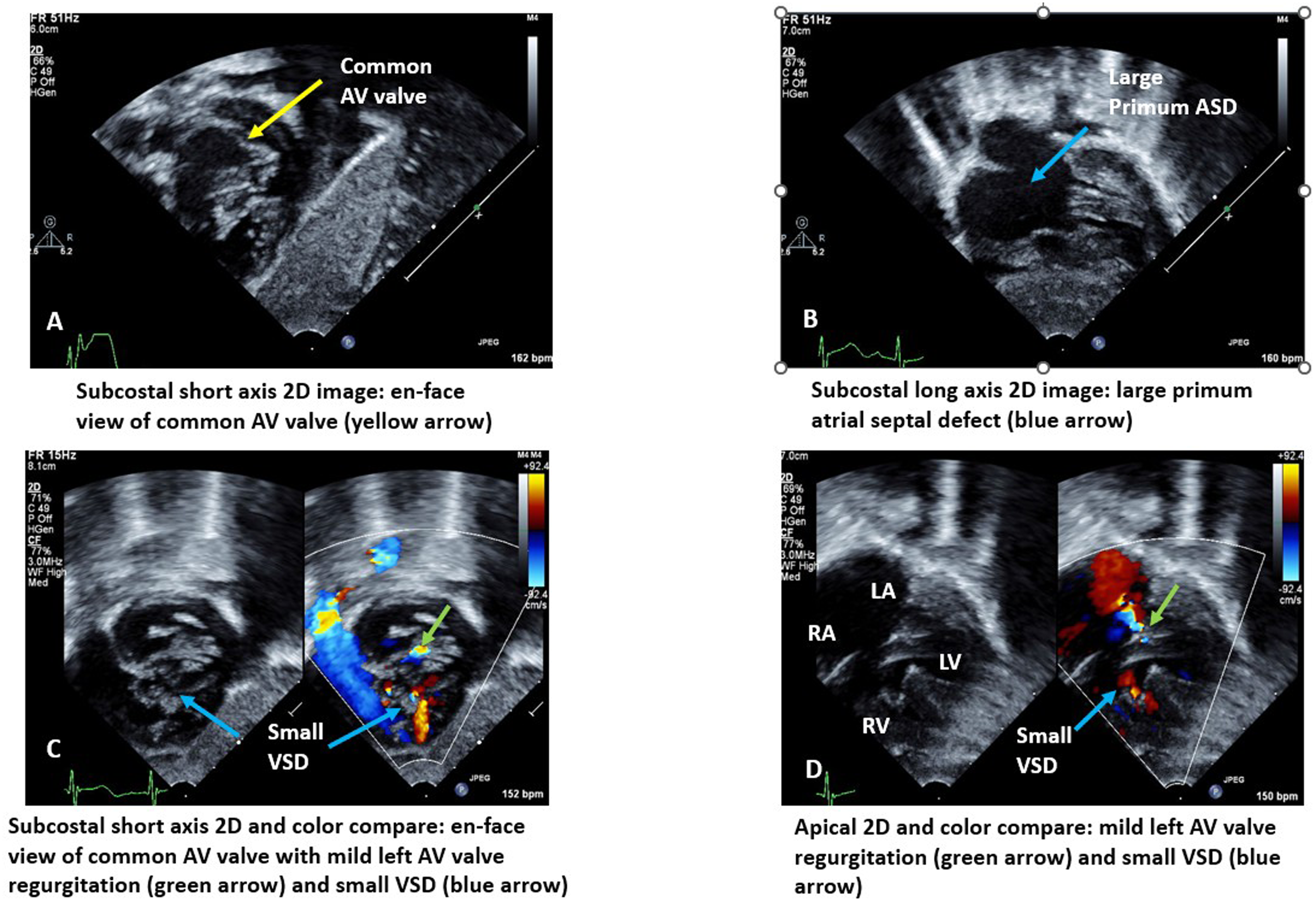
Outpatient ECHO images prior to admission for shock. (A) Subcostal short axis 2D image showing en-face view of common AV valve (yellow arrow). (B) Subcostal long axis 2D image showing large primum atrial septal defect (blue arrow). (C) Subcostal 2D and color compare: en-face view of common AV valve with mild left AVVR (green arrow) and small VSD (blue arrow). (D) Apical 2D and color compare: Mild left AVVR (green arrow) and small VSD (blue arrow). Abbreviations: AV, atrioventricular; AVVR, atrioventricular valve regurgitation; VSD, ventricular septal defect.
Transthoracic echocardiogram (TTE) revealed preserved biventricular function but interval worsening of left AVVR from mild to severe due to poor leaflet coaptation secondary to a ruptured chordae tendinae (Figure 2). She was initiated on broad spectrum antibiotics; serial blood cultures remained negative. Her disseminated intravascular coagulopathy and thrombocytopenia improved with vitamin K, fresh frozen plasma, and cryoprecipitate administration by the time of surgery. She was medically managed with continued ventilator and vasopressor support with milrinone and epinephrine infusions and diuresed with bumetanide infusion. After recovery of end organ function, she underwent repair of AV septal defect, with extensive repair of the left AV valve. Intraoperative findings confirmed a ruptured chord from the posteromedial papillary muscle without any vegetations or evidence of endocarditis. A 7-0 polypropylene suture pledgetted with autologous pericardium was used to reattach this ruptured chord back to where it came off the papillary muscle. The cleft was closed with 6-0 polypropylene suture all the way to the ventricular septum, thereby closing a small VSD noted at the base of that cleft. The common AV valve was tested, and the inferior portion of the common AV valve was noted to be tethered down due to the length of the reattached native chord being too short. As such, this repaired ruptured chord was replaced with an artificial Gore-Tex neochord exactly where the previous chord was severed and tied to an adequate height with static valve testing. There was also a scallop in the inferior part of this dysplastic valve that was closed with 7-0 polypropylene in an edge-to-edge technique. Additional repair with two commissuroplasty sutures on both commissures and one annuloplasty suture provided very good competency of the left AV valve. An autologous pericardial patch was next attached at the junction between the right and left AV valve with the surgical bites on the valve junction being taken wider than the bites on the patch to create an anterior annuloplasty to improve on the coaptation of these valves The remainder of the ostium primum ASD was closed with this same patch to complete the partial AV septal defect repair (Figure 3). Postoperative TTE showed residual mild left AVVR (Figure 2). She was discharged home with an uneventful postoperative course.
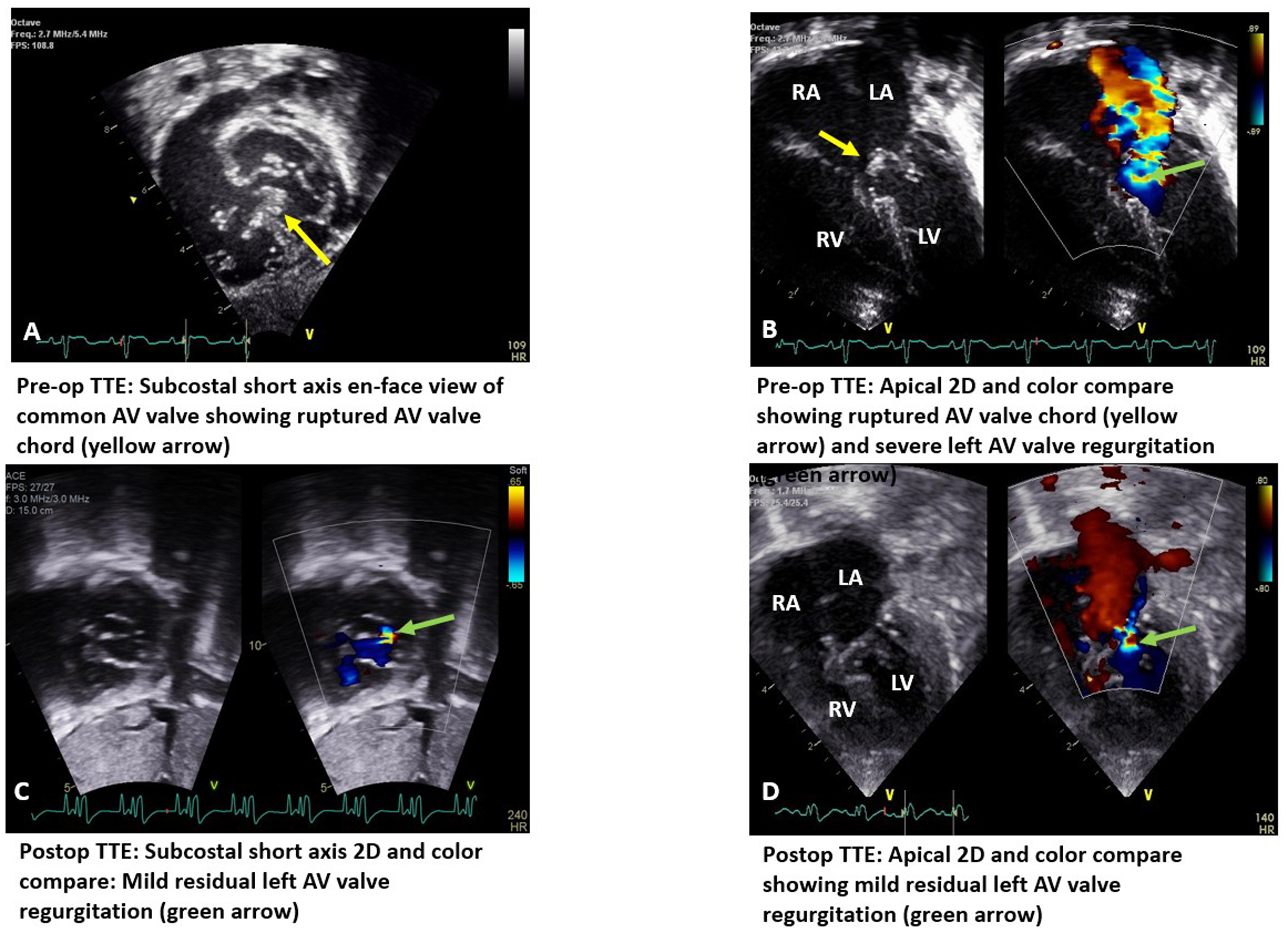
Inpatient ECHO images before and after surgical repair. (A) Pre-op TTE: Subcostal short axis en-face of AV valve showing ruptured AV valve chord (yellow arrow). (B) Pre-op TTE: Apical 2D and color compare: Ruptured AV valve chord (yellow arrow) and severe left AVVR (green arrow). (C) Postop TTE: Subcostal 2D and color compare: Mild residual left AVVR ( green arrow). (D) Postop TTE: Apical 2D and color compare: Mild residual left AVVR (green arrow). Abbreviations: AV, atrioventricular; AVVR, atrioventricular regurgitation; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TTE, transthoracic echocardiogram.
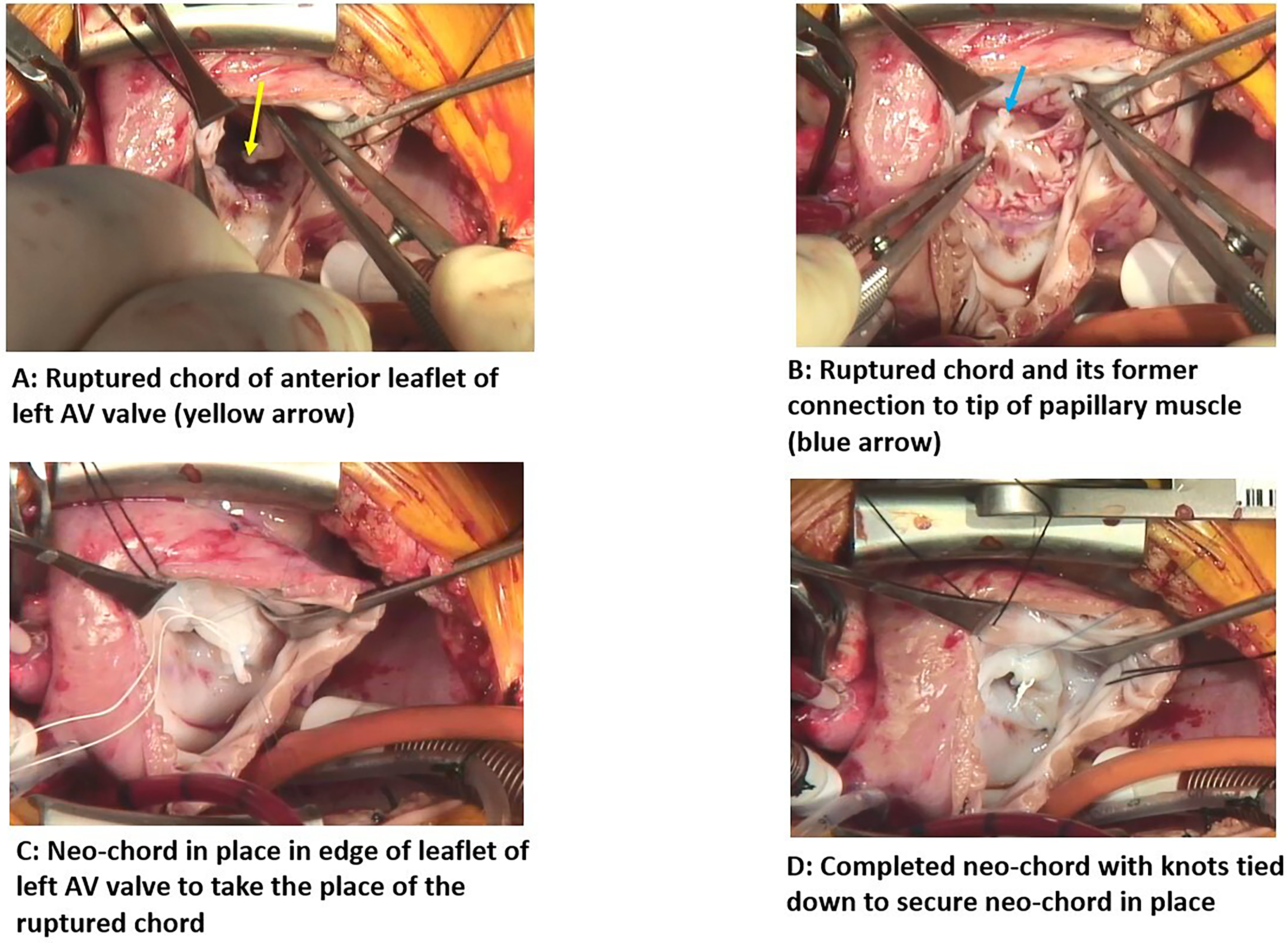
(A) Ruptured left AVV chord (arrow). (B) Ruptured chord and its former connection to tip of papillary muscle (arrow). (C) Neo-chord in place at left AVV leaflet edge to take the place of the ruptured chord. (D) Completed neo-chord with knots tied down to secure neo-chord in place. Abbreviations: AVV, atrioventricular valve.
Discussion
Spontaneous MV rupture remains a unique and rare entity, with patients presenting with sudden onset of severe cardiorespiratory shock from resulting severe mitral regurgitation, necessitating urgent intervention.6,7 In adolescents and adults MV prolapse, myxomatous degeneration, and infective endocarditis most commonly cause ruptured chordae tendinae. Most cases in infants are thought to be idiopathic. 5
The study by Shiraishi et al examined patients without congenital malformations of the mitral valve and did not appear to include any patients with congenital heart disease. 5 Although rare, the onset of acute rupture of mitral valve chordae tendinae in infants is usually around 4 to 6 months of age.5,7 Some cases occurred during spring and summer with prodromal viral symptoms, with the majority of cases being idiopathic in nature, followed by Kawasaki disease, SSA antibodies, and infective endocarditis as well as myocardial infarction and infarction of the inferior ventricular wall in Kawasaki disease.5,7 Myxoid changes of the mitral valve leaflets and chordae tendinae were seen in 39% of patients and infiltration with inflammatory cells, predominantly mononuclear cells, was seen in 64% of patients. 5 Our case is unique and to our knowledge is possibly the first reported case in the literature of idiopathic rupture of the chordae tendinae in unrepaired congenital heart disease without preceding signs of infection or evidence of endocarditis. In our patient, no tissue was available for pathologic examination given that she underwent left AV valve repair and blood cultures were negative.
Neonatal lupus, a clinical syndrome occurring from exposure to maternal autoimmune antibodies, can be associated with extranodal manifestations such as AV valve rupture with MV rupture being less common than tricuspid valve rupture. 8 Patients with DS are not at higher risk of autoimmune rheumatologic conditions such as lupus erythematosus and there was no history of exposure to maternal autoantibodies in our patient. SSA and SSB antibody testing was therefore not done.
While DS has been reported to coexist with other genetic syndromes such as Marfan Syndrome and Ehlers Danlos syndrome our patient had no features to suggest connective tissue disorder.
Prognosis in affected patients is dissatisfying given the potential need for mechanical MV replacement (27%–50%) and mortality due to cardiogenic shock.5–7 More than 3 ruptured chordae and rupture in the summer months were significantly associated with risk of artificial valve replacement. 5 However, employing artificial chordae reconstruction, paracommissural edge-to-edge repair, and Kay's annuloplasty allowed for successful repair rather than replacement in a case series of 6 patients, yielding an immediate reduction in mitral regurgitation. 9
Our patient had been followed closely to determine timing of surgical repair. The acute presentation with cardiogenic shock prompted emergent medical management and appropriate surgical repair. Transthoracic echocardiogram was crucial in confirming the diagnosis. Surgical repair although complex in our patient with concomitant repair of AV septal defect yielded excellent results obviating the need for left AV valve replacement.
Conclusion
In patients with unrepaired AV septal defect, an acute presentation with shock should raise suspicion of ruptured chord and acute onset of severe left atrioventricular valve regurgitation.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.