
Abstract
Introduction:
Pediatric asthma is a common condition that requires early detection of obstructive ventilatory defects (OVDs) for optimal management. While the forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratio is widely used in spirometry, it may lack sensitivity in children, especially in detecting mild or early obstruction. This study aimed to assess the utility of the forced expiratory flow (FEF) at 50% of FVC to the half of FVC (FEF50/0.5FVC) ratio as a complementary tool for identifying OVD in asthmatic children.
Methods:
This was a retrospective study conducted on 165 asthmatic children (aged 5–15 years). Spirometric data including FEV1, FVC, FEV1/FVC, FEF50, FEF at 25%–75% of FVC (FEF25%–75%), and peak expiratory flow were analyzed. The FEF50/0.5FVC ratio was calculated for each child. OVD was defined as an FEV1/FVC ratio below the lower limit of normal, based on Z-scores. Statistical analysis included t-tests, Pearson’s correlation, and receiver operating characteristic (ROC) curve analysis to compare the diagnostic efficiency of the FEF50/0.5FVC ratio with traditional spirometric measures.
Results:
OVD was identified in 25.5% of participants. The FEF50/0.5FVC ratio was significantly lower in the OVD group (1.23 ± 0.24) compared with the normal spirometry group (2.08 ± 0.5, P < 0.0001). A strong correlation was observed between the FEV1/FVC ratio and FEF50/0.5FVC (r = 0.88, P < 0.001). ROC analysis showed that the FEF50/0.5FVC ratio had superior diagnostic accuracy for OVD (area under the curve = 0.948, 95% confidence interval 0.899–0.996) compared with other spirometric indices, with a sensitivity of 91% and specificity of 90.2% at an optimal threshold of 1.56.
Conclusion:
FEF50/0.5FVC ratio is a promising tool for detecting OVD in asthmatic children, demonstrating high sensitivity and specificity. It may outperform traditional spirometric measures in identifying subtle airway obstructions, offering a valuable addition to routine asthma diagnostics, particularly in pediatric patients with early-stage or mild asthma.
Introduction
Pediatric asthma is one of the most prevalent chronic respiratory diseases 1 in children, and its frequency has increased significantly over the past few decades. According to a 2022 report by the American Lung Association, approximately 7.0% of boys and 5.4% of girls are currently affected by asthma, though prevalence rates vary by state. 2 As a major public health problem, it impacts children’s quality of life, 3 often causing symptoms such as wheezing, coughing, and breathlessness. These symptoms can limit physical activities, disrupt sleep, 4 and lead to frequent hospitalizations. Early diagnosis of asthma is crucial for effective management of the disease and prevention of long-term complications, which underscores the importance of appropriate diagnostic tools. Spirometry is a standard method for evaluating lung function in asthmatic patients, enabling the detection of obstructive ventilatory defects (OVDs). 5
Various spirometric parameters, including forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and the FEV1/FVC ratio, are commonly used to detect OVD. The FEV1/FVC ratio is a key indicator in diagnosing OLDs such as asthma, as it measures the proportion of air exhaled during the first second relative to the total volume that can be forcibly exhaled, providing insight into the severity of airway obstruction. 6 However, this index has limitations. Despite its effectiveness in diagnosing more severe forms of airway obstruction, it may not be sensitive enough to identify mild or intermittent asthma, especially in children.7,8
Asthma often involves small airway obstruction, a key feature of small airway disease (SAD), that may not be captured by conventional spirometric measures (FEV1, FVC). SAD is increasingly recognized as an important contributor to early airflow limitation and disease progression. 9 This has led to growing interest in exploring alternative spirometric indices that could identify subtle airflow limitations associated with SAD. One such index is the FEF50/0.5FVC ratio, which integrates the forced expiratory flow at 50% of FVC (FEF50) with half of the FVC, offering a combined measure of mid-expiratory flow and lung volume. FEF50 represents the flow of air midway through the forced exhalation, and it can provide insights into the behavior of smaller airways that are typically affected in the early stages of asthma. 10 By focusing on the mid-portion of the exhalation, the FEF50/0.5FVC ratio may offer a more refined evaluation of airway function, potentially revealing airflow obstruction that might go undetected by conventional indices.
The objective of this study was to assess the value of the FEF50/0.5FVC ratio in detecting OVD in asthmatic children, compared to traditional spirometric measures.
Methods
This retrospective study was conducted on a population of asthmatic children referred to the Department of Physiology and Functional Explorations at Abderrahmene MAMI Hospital in Ariana, Tunisia. The study included children aged 5–15 years with a clinical diagnosis of asthma who had undergone full spirometry between January 2021 and December 2023. Only children in a stable phase of the disease, with no acute exacerbations in the 4 weeks preceding the study, were included. Children with respiratory comorbidities other than asthma, or severe comorbidities (e.g., cardiovascular or neuromuscular disorders) were excluded. In addition, children unable to perform reliable spirometry or with missing data were also excluded.
Ethical approval was obtained from the institutional review board of Abderrahmene MAMI Hospital (Approval No. 35/2025) prior to the initiation of the study.
Asthma control was assessed by the Asthma Control Questionnaire, a validated tool for assessing asthma control in children and adolescents aged 6–17 years.11,12
It contains seven items measured on a 7-point scale, from 0 (no impairment) to 6 (extreme impairment), using the past 7 days as a recall period with all items equally weighted. 13
The mean score of the six items was computed ranging from 0 to 6. A mean score ≤0.75 was categorized as “well controlled,” ≥1.5 as “uncontrolled,” and scores falling between these thresholds as “somewhat controlled.”
Spirometric measurements included not only FEV1, FVC, the FEV1/FVC ratio and FEF50 but also peak expiratory flow (PEF), and FEF at 25%–75% of FVC (FEF25%–75%), as these are important markers of airway obstruction in asthmatic children.14–16 The Global Lung Initiative (GLI) reference equations 17 were used to calculate predicted values for spirometric parameters. FEV1, FVC, PEF, and FEF25-75 were expressed as a percentage of the predicted values, based on age, height, sex, and ethnicity, while the FEV1/FVC ratio, the FEF50/0.5FVC ratio, and FEF50 were presented as absolute values.
The FEF50/0.5FVC ratio was calculated for each child. OVD were defined as a reduced FEV1/FVC ratio below the lower limit of normal, which was determined using Z-scores according to the American Thoracic Society and the European Respiratory Society guidelines. A Z-score of −1.64 or lower was used to indicate significant deviation from normal values. 18
Statistical analysis
Statistical analyses were performed with SPSS version 25.0 software. Categorical data were expressed using frequencies and percentages, while continuous data were expressed using mean values and standard deviation. The Student’s t-test was used to examine the differences in spirometric parameters between asthmatic children with normal spirometry and those with OVD. Pearson’s correlation coefficient was used to analyze the association of the FEV1/FVC with FEF50/0.5FVC and common spirometric markers of obstruction in asthmatic children (FEV1, PEF, and FEF25%–75%).
Receiver operating characteristic (ROC) curves were generated for the FEF50/0.5FVC ratio and FEV1, PEF, and FEF25%–75% using the presence of OVD as a reference. ROC curves were compared based on the area under the curve (AUC) and were used to determine the optimal threshold for FEF50/0.5FVC based on the best combination of sensitivity and specificity. A P value <0.05 was considered significant.
Results
We identified 192 asthmatic children referred to our department in the specified period. A total of 27 participants were excluded. Thus, the study included 165 children who met the criteria (Fig. 1). Among them, 66.67% were well controlled, and 4.24% were uncontrolled. Regarding treatment, one-third of the population (33.33%) were receiving a maintenance treatment, 42% were exclusively using an inhaled short acting beta‐2 agonists, and 25% were not undergoing any treatment (Table 1).
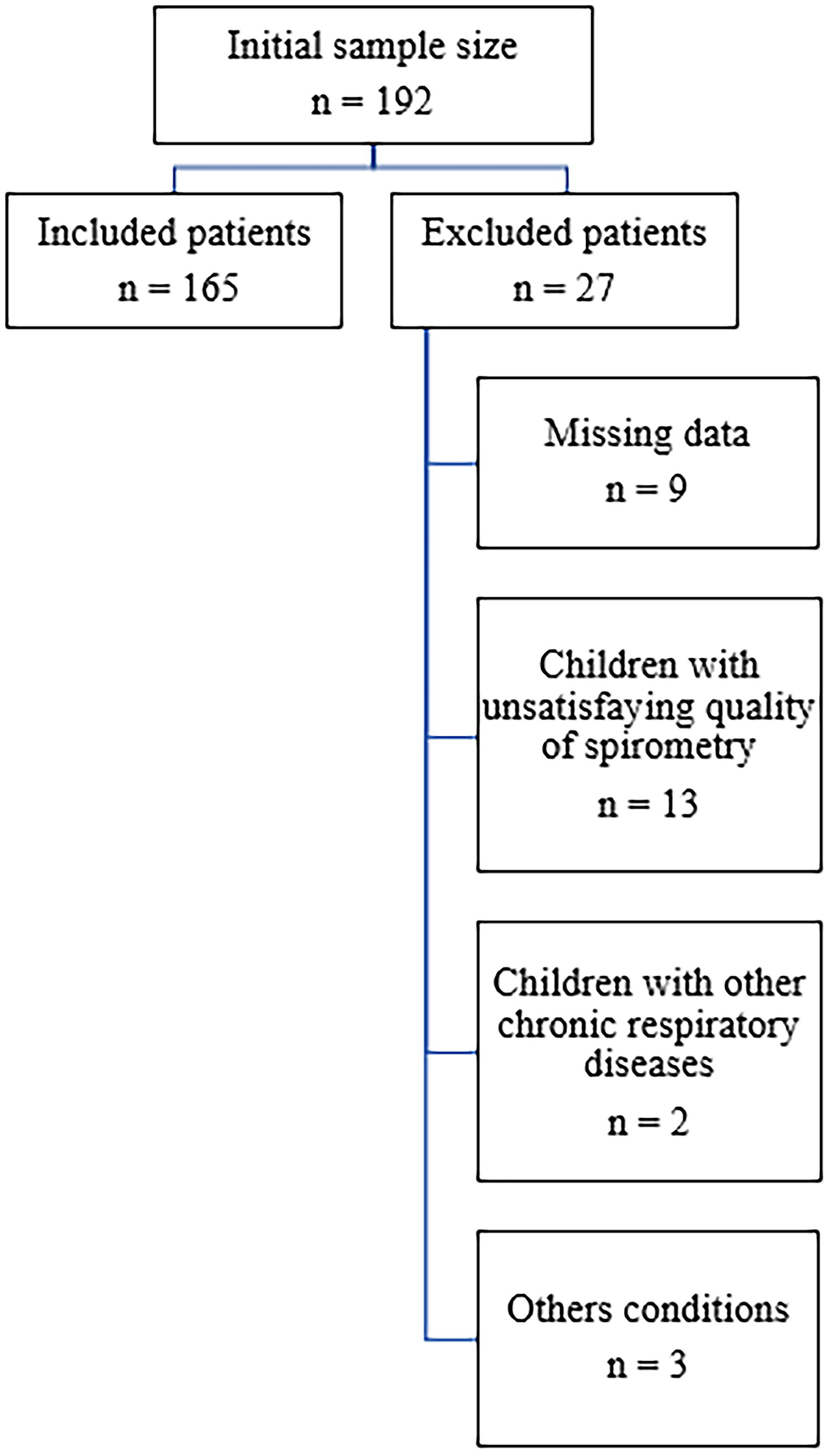
Enrolment of asthmatic children.
Characteristics of the Study Population
ACQ, asthma control severity; FEF25–75, forced expiratory flow at 25–75% of FVC; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; ICS, inhaled corticosteroids; OVD, obstructive ventilatory defect; PEF, peak expiratory flow.
Spirometric analysis identified OVD in 25.5% of participants. FEV1 and FVC values were greater than 80% in 89.7% and 94.5% of participants, respectively (Table 1).
When comparing participants with normal spirometry to those with OVD, significant differences emerged. First, the OVD group was significantly older (9.76 ± 2.94 years) than the normal spirometry group (8.57 ± 2.84 years; P = 0.017). However, there was no significant difference in sex distribution (P = 0.29) or parental smoking status (P = 0.37) between the two groups (Table 2).
Comparison Between Asthmatic Children with Normal Spirometry and Those with Obstructive Ventilatory Defect
Bold p-values indicate statistical significance (p < 0.05).
ACQ, asthma control questionnaire; BMI, body mass index; FEF25–75, forced expiratory flow at 25–75% of FVC; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PEF, peak expiratory flow; OVD, obstructive ventilatory defects.
Spirometric parameters revealed substantial differences between the groups. As expected, FEV1 and the FEV1/FVC ratio were significantly lower in the OVD group (83.44 ± 14.34 and 0.71 ± 0.06, respectively) compared with the normal group (98.22 ± 12.19 and 0.86 ± 0.06, respectively; P < 0.0001). However, no significant difference in FVC was observed between the two groups (P = 0.22).
Moreover, the FEF50/0.5FVC ratio had a mean value of 1.23 ± 0.24 in the OVD group compared with 2.08 ± 0.5 in the normal group (P < 0.0001) (Table 2).
Correlation analysis revealed that FEV1/FVC ratio was significantly correlated with FEF50/0.5FVC ratio (r = 0.88; P < 0.001), FEV1 (r = 0.53; P < 0.001), FEF25–75 (r = 0.70; P < 0.001) and PEF (r = 0.45; P < 0.001) (Fig. 2).
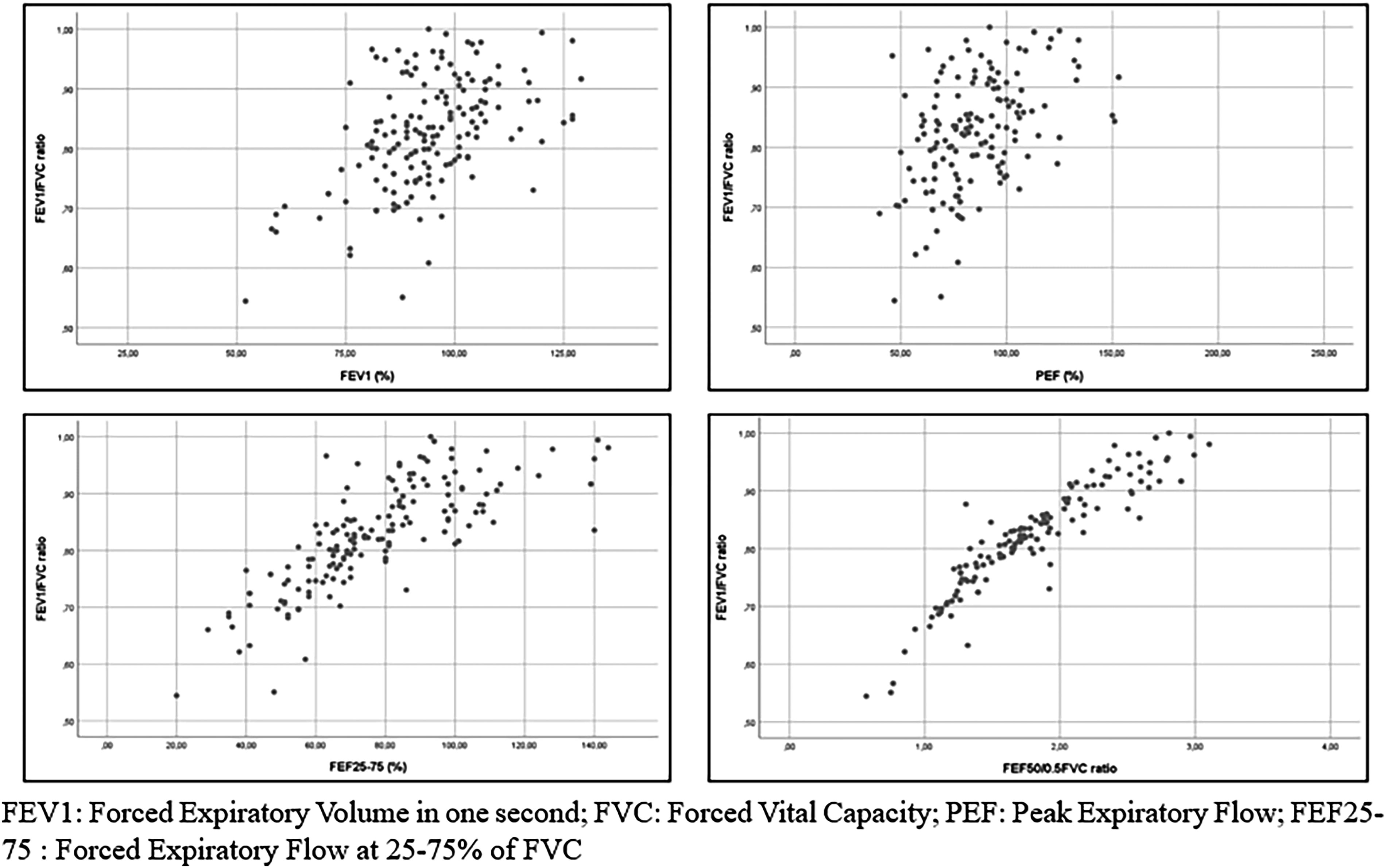
Correlations of FEV1/FVC ratio with FEV1(%), PEF (%), FEF25–75(%).
When using ROC analysis, we found that the performance of FEF50/0.5FVC ratio in discriminating participants with OVD was better than that obtained for the other spirometric parameters. Indeed, the AUC for FEF50/0.5FVC ratio was higher than that obtained for FEV1, FEF25–75, and PEF with an AUC of 0.948 (95% CI: 0.899–0.996) (Fig. 3 and Table 3)
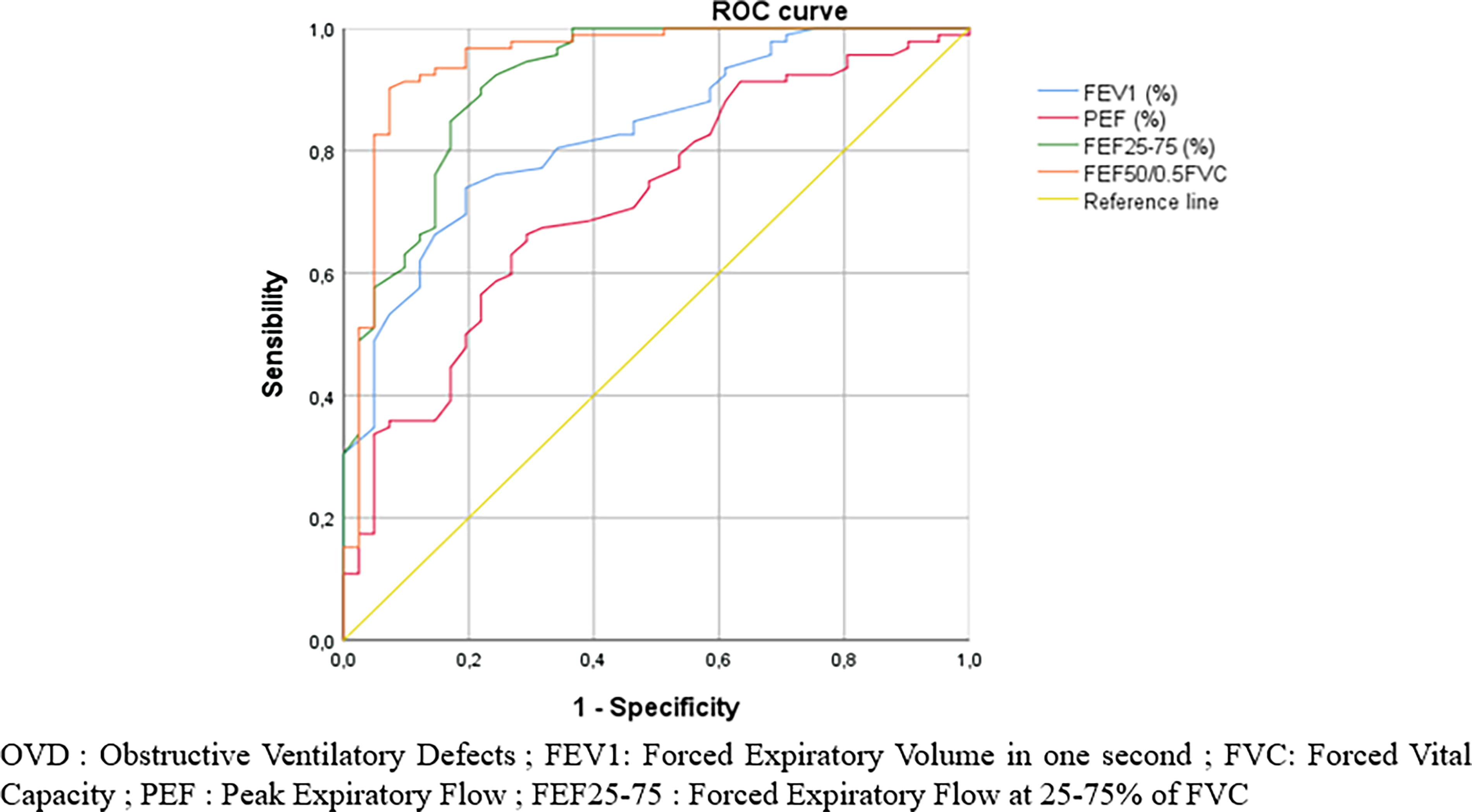
Receiver operating characteristic curves of FEV1(%), PEF(%), FEF25–75(%) and FEF50/0.5FVC values for obstructive ventilatory defect.
AUCs Of the ROC Curves for FEV1(%), PEF(%), FEF25-75(%) and FEF50/0.5FVC for Obstructive Ventilatory Defect
Bold value indicates the highest AUC among the tested parameters.
AUC, area under the curve; CI, confidence interval; FEF25–75, forced expiratory flow at 25–75% of FVC; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PEF, peak expiratory flow; ROC, receiver operating characteristic.
The optimal threshold for this ratio was determined to be 1.56, offering a sensitivity of 91% and a specificity of 90.2% for the detection of OVD.
Discussion
The results of this study demonstrated that the FEF50/0.5CVF ratio could be a reliable tool for identifying OVD in asthmatic children. Indeed, with sensitivity and specificity approaching 90%, this ratio performs as well as, if not better than, traditional spirometric parameters.
Asthma in children is not only a frequent respiratory pathology but also a significant public health concern due to its chronic nature and impact on children’s quality of life.19–21 In clinical practice, spirometry remains the cornerstone of asthma diagnosis and management, helping to assess lung function and detect OVD.22–24
The FEV1/FVC ratio is a key indicator of airway obstruction, 25 as it represents the proportion of air exhaled during the first second of a forced expiration (FEV1) in relation to the total exhaled volume (FVC). It primarily reflects the condition of large and medium-sized airways. In obstructive diseases like asthma, a lower FEV1/FVC ratio indicates airway narrowing, but it may not effectively capture obstruction in smaller airways, especially in cases of mild or intermittent asthma.26–28 This limitation has led to a revised understanding of asthma pathophysiology. While traditionally considered as primarily involving the large airways, emerging evidence identifies the small airways as a significant site of airflow obstruction. 9
The FEF50/0.5FVC ratio could address this limitation by focusing on airflow at mid-lung volumes. The FEF50 measures forced expiratory flow when 50% of the FVC has been exhaled, which highlights smaller airway function more accurately.29,30 The 0.5FVC term normalizes the flow rate for lung size, enhancing the detection of subtle changes in smaller airways.
In pediatric asthma, small airways are often more affected.31–33 SAD is a critical early marker to asthma pathophysiology across all severities, with rates ranging from 53%–90% depending on severity.34,35 It has been linked to nocturnal symptoms, exercise-induced bronchoconstriction, and increased airway hyperresponsiveness, all of which contribute to asthma morbidity and reduced quality of life. 36 Similarly, a recent study conducted by Abdo et al., 35 showed that small airway dysfunction is strongly associated with poor control of the disease.
Our study conducted on 165 asthmatic children revealed several important findings that highlight the value of the FEF50/0.5FVC ratio. First, the analysis comparing children with normal spirometry to those with OVD demonstrated significant differences across several key spirometric parameters, including FEV1, FEV1/FVC, FEF25-75, and PEF. These findings confirm that traditional spirometric parameters do effectively capture the presence of airflow obstruction in more pronounced cases. However, the significant reduction in FEF50/0.5FVC values in the OVD group compared with the normal spirometry group highlights this ratio’s potential to detect subtler forms of obstruction that might be missed by traditional measures.
The correlation analysis between the FEV1/FVC ratio and the FEF50/0.5FVC ratio (r = 0.882, P < 0.00001) further reinforces the reliability of the latter in detecting airflow limitation. This strong positive correlation suggests that both ratios are consistently aligned in identifying OVD, with the FEF50/0.5FVC ratio adding an extra layer of diagnostic sensitivity. Notably, while the FEV1/FVC ratio has long been established as a standard marker of obstruction, the FEF50/0.5FVC ratio may offer more nuanced insight, particularly in asthmatic children with intermittent or mild forms of the disease.
The ROC curve analysis conducted in this study adds further weight to the diagnostic utility of the FEF50/0.5FVC ratio. With an AUC of 0.948, the FEF50/0.5FVC ratio demonstrated excellent discriminatory power in identifying OVD among asthmatic children. An AUC of this magnitude suggests that the FEF50/0.5FVC ratio is highly accurate in distinguishing between normal and obstructive spirometric patterns. Importantly, the ROC analysis also revealed that the FEF50/0.5FVC ratio outperformed other spirometric measures, including FEV1, PEF, and FEF25–75, in terms of diagnostic accuracy. This result is particularly interesting because it highlights the limitations of relying solely on traditional parameters such as FEV1 or PEF for diagnosing OVD in pediatric asthma. While these parameters are important, the FEF50/0.5FVC ratio’s superior AUC suggests that it might be a more sensitive and specific marker, particularly for detecting subtle airflow limitations. The determination of an optimal threshold of 1.56 for the FEF50/0.5FVC ratio, with corresponding sensitivity and specificity values of 91% and 90.2%, respectively, makes a point of the validity of this ratio as a diagnostic tool. These high values suggest that the FEF50/0.5FVC ratio can reliably identify OVD while minimizing false positives and negatives, making it a highly practical addition to routine spirometry.
Advanced techniques such as multiple breath washout and oscillometry provide enhanced detection of SAD compared with FEF25–75. 37 In a recent study conducted by Postma et al., 38 a SAD score, assessed using both impulse oscillometry and spirometry, showed significant associations with asthma control, history of exacerbations, and disease severity. Similarly, Kraft et al. 39 demonstrated, in longitudinal 1-year follow-up data from the ATLANTIS 38 study that SAD, measured by impulse oscillometry, lung volumes, multiple breath washout, and FEF25–75, was longitudinally associated with asthma control, exacerbations, and quality of life.
However, given the cost and limited availability of advanced techniques, simpler and more accessible methods, such as spirometry-derived metrics, could serve as valuable alternatives. 40 The FEF50/0.5FVC ratio is particularly well-suited to detect SAD by capturing airflow limitations in mid-lung volumes, where early changes in small airway function are more pronounced. Unlike the FEV1/FVC ratio, which may overlook these subtle abnormalities, the FEF50/0.5FVC ratio offers a more sensitive and specific measure for identifying early or mild obstruction. This makes it a cost-effective and practical tool for comprehensive assessment of OVD and early intervention, particularly in pediatric asthma, where SAD significantly influences disease management and outcomes.
However, the use of FEF50/0.5FVC to assess bronchial obstruction is still poorly documented in the literature. In a single study 10 conducted in 2010, the FEF50/0.5FVC ratio has been proposed as a useful parameter in diagnosing OLD in adults, showing a positive correlation with FEV1/FVC in OLD patients. 10
However, most studies have demonstrated the usefulness of other spirometric measures in asthmatic children. Studies on FEF50 in asthmatic children reported its role in assessing small airway function. In fact, Mahut et al. found that FEF50 correlated more strongly with specific airway resistance than FEV1, implying its utility in detecting early airflow obstruction. 41 In addition, significant differences in FEF50 values have been shown between healthy and asthmatic children, pointing to the potential of this spirometric parameter as a diagnostic tool. 42 Further, FEF50 was associated with blood eosinophil counts in exercise-induced bronchospasm in children with mild asthma. 43 In regard to FEF25-75, it has been demonstrated that this spirometric parameter strongly correlates with standard spirometric measures including FEV1 and FEV1/FVC ratio in asthmatic children. 15 Moreover, children who had an impaired FEF25–75 but a normal FEV1 were more likely to experience uncontrolled asthma than those with both parameters within the normal range. 44 While PEF measurements are commonly used to evaluate airway obstruction in asthmatic children, their reliability is debated. Although, this parameter can be a useful screening tool with high specificity and negative predictive value for excluding OVD, it has moderate sensitivity and positive predictive value as a diagnostic test. 45
Study limitations
Despite the promising findings of this study, there are several limitations that should be acknowledged:
Inability to assess FEF50 as a percentage of predicted value: one limitation of this study is the inability to calculate FEF50 expressed as a percentage of the predicted value. The GLI equations
17
do not provide predicted values for FEF50, which restricted our ability to analyze this parameter in relation to predicted norms. Collinearity in logistic regression analysis: another limitation is the issue of multicollinearity in the logistic regression analysis. This statistical issue can complicate the interpretation of the relationship between the FEF50/0.5FVC ratio and OVD, potentially affecting the reliability of the findings and the overall model performance. Single-center study with small sample size: The study was conducted at a single center with a relatively small sample size of 165 children, which may limit the generalizability of the results. Future research should aim to replicate these findings in larger and more diverse populations to confirm the diagnostic value of the FEF50/0.5FVC ratio across different pediatric asthma cohorts. Lack of long-term outcome evaluation: This study did not evaluate the long-term outcomes of employing the FEF50/0.5FVC ratio in clinical practice. Furthermore, research is needed to determine if this ratio can predict disease progression or response to treatment. Retrospective design of the study: The retrospective design of the study may introduce biases related to data collection and interpretation. Prospective studies with longitudinal follow-up would provide stronger evidence of the clinical utility of the FEF50/0.5FVC ratio in managing asthma in pediatric population.
In conclusion, this study highlights the diagnostic value of the FEF50/0.5FVC ratio in detecting OVD in asthmatic children. By offering a more sensitive and specific marker for airflow limitation compared to traditional spirometric measures, this ratio has the potential to improve early detection and management of pediatric asthma. Furthermore, research is needed to confirm these findings in larger populations and explore the broader applications of the FEF50/0.5FVC ratio in pediatric respiratory medicine.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.