
Abstract
Patients with pathogenic variants of lipopolysaccharide-responsive beige-like anchor protein (LRBA) are known to present with autoimmune diseases, inflammatory bowel disease, lymphoproliferative disorders, allergies, immunodeficiency, and malignancies. This condition, characterized by widespread infections that impact multiple systems, has various radiological findings reported in the literature. These include computed tomography (CT) findings indicating lung involvement and magnetic resonance imaging (MRI) findings showing neurological system involvement. However, F-18 fluorodeoxyglucose positron emission tomography-CT (FDG PET-CT) imaging findings in LRBA deficiency have not yet been described in the literature. This report presents multiple organ involvements detected by F-18 FDG PET-CT in a case with an LRBA gene variant. FDG PET-CT findings for diagnostic and primary focus evaluation were reviewed in a 17-year-old male patient with a pathogenic LRBA variant, prompted by multiple hypoechoic nodular appearances identified on abdominal ultrasonography. In this patient, who carried a pathogenic LRBA variant (c.3396-3397delAC, p.D975Yfs*15) and was treated with abatacept for liver involvement, FDG PET-CT revealed a wide range of system involvements. These included the lungs, liver, intestines, bone, bone marrow, and lymph nodes, as well as multiple joints and tendons. In immunodeficiency diseases with such extensive multisystem involvement, whole-body imaging techniques like F-18 FDG PET-CT can serve as valuable tools for physicians to comprehensively assess the disease and formulate effective treatment strategies.
Keywords
Introduction
Lipopolysaccharide-responsive beige-like anchor (LRBA) deficiency is a congenital immunodeficiency disorder caused by biallelic pathogenic variants in the LRBA gene, which result in the loss of protein expression. 1 In cases with deficient LRBA protein expression, LRBA has been identified as a post-translational regulator of cytotoxic T lymphocyte—associated protein 4 (CTLA-4), preventing its degradation in lysosomes; subsequently, germline heterozygous loss-of-function pathogenic variants in the CTLA4 gene were found to cause a monogenic disorder with a clinical phenotype similar to LRBA deficiency. 2
These pathogenic variants lead to defects in B lymphocyte activation, organomegaly, enteropathies, inflammatory bowel diseases, multiple autoimmune disorders involving activated T cells, and recurrent infections.1,3 The symptoms display significant phenotypic variability, differing in age of onset, severity, multi-organ involvement, and disease progression.
A thorough physical examination and advanced imaging techniques are crucial for identifying these diverse phenotypic manifestations. Given that clinical presentations, symptoms, and laboratory findings often overlap with degenerative processes, autoimmune-allergic events, sterile inflammatory conditions, and infections, whole-body imaging—particularly F-18 fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET-CT)—plays a pivotal role. FDG PET-CT is invaluable for differential diagnosis, assessing the extent and severity of the disease, and identifying the optimal biopsy site by pinpointing areas of highest activity.4,5 F-18 FDG PET-CT is an advanced functional and anatomical imaging modality that offers critical insights across a wide range of medical disciplines. In oncology, it plays a pivotal role in tumor staging and restaging, evaluating treatment response, identifying optimal biopsy sites, planning radiotherapy, and guiding numerous other clinical decisions. In cardiology, it assists in assessing the viability of chronically ischemic or infarcted myocardial tissue. In neurology, it contributes to the evaluation of the location and severity of neurodegenerative disorders and epilepsy. In addition, it is highly effective in identifying the underlying cause of fever and pinpointing sites of infection.
Functional whole-body imaging techniques such as F-18 FDG PET-CT are particularly valuable in oncology and inflammatory diseases with multi-system or diffuse involvement. 6 Their capacity to visualize all affected organs and systems enables clinicians to map the complex pathways from abnormal laboratory findings to clinical manifestations. This facilitates the early detection of lesions—prior to the development of chronic changes or sequelae—and supports the accurate planning and implementation of therapeutic strategies. In contrast, diffuse organ and system involvement is often difficult to detect using conventional morphological imaging methods.
This report highlights the first documented case of multisystem involvement detected using F-18 FDG PET-CT in a patient with LRBA deficiency.
Case
Written informed consent was obtained from the individual’s parents for participation in the study and publication. All procedures were conducted in accordance with the ethical standards of institutional and national research committees.
A 17-month-old boy, initially presenting with recurrent infections and Evans syndrome accompanied by elevated double-negative T lymphocytes, was clinically diagnosed with autoimmune lymphoproliferative syndrome (ALPS) in 2011. 7 Genetic analysis later identified an LRBA pathogenic variant (c.3396-3397delAC, p.D975Yfs*15), making the patient the 15th case included in the multicentric study titled “Abatacept as a Long-Term Targeted Therapy for LRBA Deficiency,” published in 2019 by Kiykim A. and colleagues. 8
A 17-month-old boy, who initially presented with recurrent infections and Evans syndrome accompanied by elevated double-negative T lymphocytes, was clinically diagnosed with autoimmune lymphoproliferative syndrome (ALPS) in 2011. Lymphocyte subset analysis revealed that double-negative T cells (CD3+, CD4−, CD8−) accounted for 16% of the total lymphocyte population. Subsequent genetic testing identified a pathogenic LRBA variant (c.3396_3397delAC, p.D975Yfs*15), and the patient was later included as the 15th case in the multicenter study titled “Abatacept as a Long-Term Targeted Therapy for LRBA Deficiency,” published in 2019 by Kiykim A. and colleagues.
In 2017, after the discovery of multiple liver nodules on abdominal MRI, a liver biopsy revealed “hemophagocytosis” and “active hepatitis” (positive for CD68 histiocytes and negative with EBER ISH). The patient experienced frequent infections, pneumonia, and diarrhea, necessitating intravenous immunoglobulin treatment. By 2018, the patient was diagnosed with LRBA deficiency, complicated by bronchiolitis obliterans organized pneumonia (BOOP), and was subsequently started on abatacept therapy (CTLA4-Ig—Orencia®, Bristol Myers Squibb, Princeton, NY). 8
In September 2022, the patient was admitted to Erciyes University Faculty of Medicine Hospital with complaints of high fever, diarrhea, abdominal pain, and shortness of breath, presenting to the pediatric hematology-oncology outpatient clinic. Physical examination revealed hepatomegaly and pulmonary crackles on auscultation. Some laboratory tests are shown in Table 1.
Biochemical Values of the Patient with LRBA Pathogenic Variant
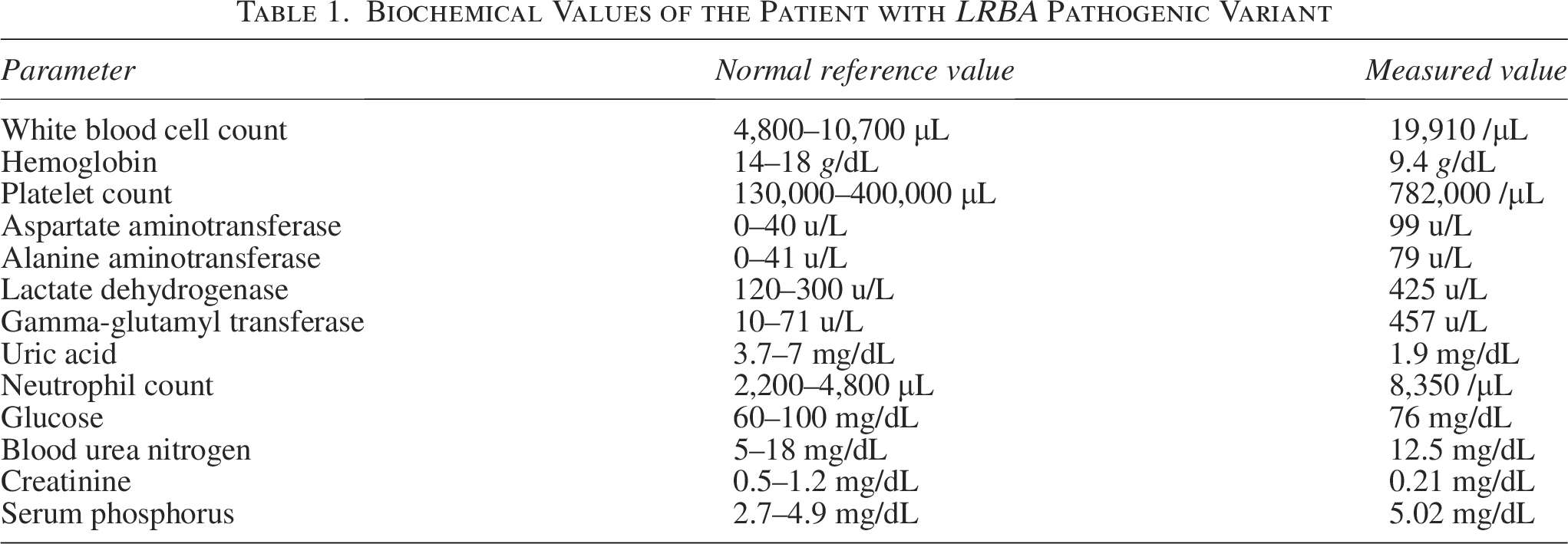
All other measured values were within normal limits.
Abdominal ultrasonography revealed multiple hypoechoic nodular appearances in the liver, suspected to indicate metastases, as well as multiple conglomerate lymph nodes, the largest measuring 36 × 13 mm, located in the hilum of both kidneys, the paraaortic area, and the mesenteric root. As a result, the patient was referred to the nuclear medicine clinic for FDG PET-CT to assess systemic involvement and rule out concomitant malignancy.
The PET-CT scan was performed as a whole-body imaging study, 55 min after intravenous administration of 3.48 mCi of F-18 FDG (Medicheck Nuclear Products Industry and Trade Inc., Istanbul). The patient had fasted for 8 h prior to the scan, and their blood glucose level was recorded as 102 mg/dL at the time of F-18 FDG injection. Scanning was conducted in 3-dimensional mode using a PET-CT scanner (GE Healthcare, Milwaukee, WI).
In the F-18 FDG whole-body PET-CT study, multiple nodular density increases with unclear borders were observed in different segments of both lung parenchyma, accompanied by interlobular septal thickenings and reticular density increases. The largest nodule measured 8 × 6 mm, with some showing minimal metabolic activity.
The liver was larger than normal, with heterogeneous density. Widespread hypodense lesions were noted across all segments, the largest being 41 × 25 mm in segment 4 b. These lesions had faint contours, with some appearing slightly hypermetabolic and others merging, indicative of hepatitis associated with the primary disease.
The colon walls were diffusely thickened and edematous, showing intense hypermetabolism (SUV max: 8.9), particularly at the cecum, consistent with colitis related to the primary disease. Multiple lymph nodes with varying degrees of hypermetabolic activity were identified in the bilateral paraaortic area, iliac chains, around the pancreatic head, between duodenojejunal loops, the pericecal region, among all intestinal loops, and the right inguinal region. The largest lymph node measured 20 × 11 mm, suggesting nodal involvement linked to the primary disease.
Bone trabecular structures in the skull, vertebral column, ribs, sternum, and pelvic bones were diffusely sclerotic. Mild hypermetabolism was present across the axial skeleton, with heterogeneous hyperdense-sclerotic appearances in the intramedullary regions of both scapulae, iliac wings, and proximal metaphyseal regions of the humerus and femur. Multiple sclerotic lesions were also identified in the intramedullary area of the right femur’s distal metaphyseal region, the largest being 8 × 6 mm, though without significant metabolic activity. These findings supported bone and bone marrow involvement in the primary disease (Fig. 1).
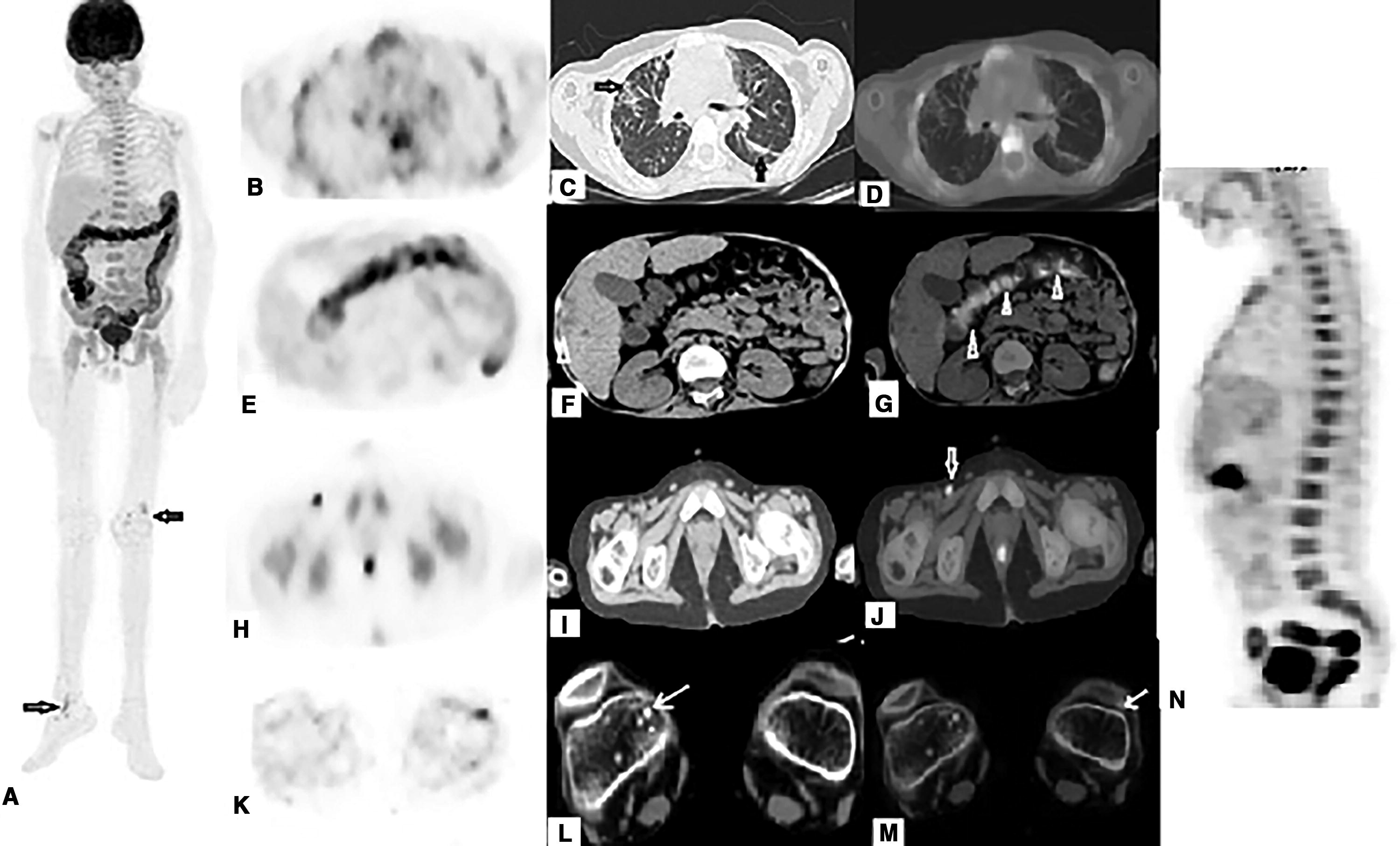
The F-18 fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET-CT) whole-body scan (
Endoscopic biopsies performed in October 2022, 4 days after the PET-CT scan, revealed “active ileitis and diffuse active colitis” in samples taken from the terminal ileum, cecum, ascending colon, sigmoid colon, and rectum. In addition, a lung biopsy obtained via thoracotomy 1 week after the PET-CT scan was diagnosed as BOOP. Immunohistochemical staining of the lung biopsy showed positive results for leukocyte common antigen, negative results for cytomegalovirus, and positive results for Masson’s trichrome in areas containing Masson bodies.
Discussion
Recently, with advancements in next-generation high-throughput DNA sequencing technologies, various human inborn errors of immunity have been identified. Among these, LRBA deficiency is classified as a primary immune regulatory disorder. It belongs to a subgroup of diseases characterized by autoimmunity, lymphoproliferation, autoinflammation, and malignancy.
LRBA protein functions as a T cell regulator, protecting it from lysosomal degradation by facilitating the transport of cytotoxic T-lymphocyte protein-4, a potent inhibitory immune receptor, to the cell surface. Patients with LRBA deficiency often exhibit a tendency toward hemophagocytosis.7,8 Pathogenic variants in the LRBA gene are known to cause humoral immunodeficiency, lymphoproliferation, and autoimmune diseases. Treatments for this disorder include hematopoietic stem cell transplantation (HSCT) and various immunosuppressive agents.3,4,9 However, careful management is essential due to complications associated with immunosuppressive therapies and the high mortality rate linked to HSCT.
Since there is no clear genotype-phenotype correlation in LRBA deficiency, it is understandable that physicians often require more detailed information when planning treatments. Key considerations include the optimal duration and combinations of immunosuppressive drugs, as well as the appropriate timing for transitioning to HSCT.
To date, detailed radiological and molecular imaging findings in LRBA deficiency have not been extensively documented. A meta-analysis of 109 cases of LRBA deficiency—93 with homozygous pathogenic variants and 16 with compound heterozygous pathogenic variants, derived from 45 eligible articles—revealed a broad spectrum of clinical manifestations. These included immune disorders, autoimmune diseases, organomegaly, chronic diarrhea, and recurrent infections. 1 In a study by Gamez-Diaz L et al. examining the phenotypes of 22 patients with LRBA deficiency, the primary clinical complications were immune dysregulation (95%), organomegaly (86%), recurrent infections (71%), and hypogammaglobulinemia (57%). 10 However, our literature review did not identify any F-18 FDG PET-CT imaging findings in LRBA pathogenic variant cases.
F-18 FDG PET-CT is an emerging and effective imaging technique, increasingly used in the assessment of inflammatory and degenerative processes, prolonged unexplained fever, autoimmune-allergic events, rheumatologic conditions, sterile inflammatory processes, and infectious diseases. Since clinical examinations, symptoms, and laboratory findings in such conditions often overlap, whole-body imaging—particularly F-18 FDG PET-CT—plays a critical role in differential diagnosis and in assessing the extent and severity of the disease. Furthermore, it serves as an essential guide for determining biopsy sites, highlighting areas of active involvement when a definitive diagnosis cannot be achieved.4,5
In rare multisystem diseases such as LRBA deficiency, determining glucose receptor expression levels in lesions and identifying diffusely involved tissues and systems through FDG PET-CT can provide valuable insights for clinicians. Consequently, this imaging method allows for a detailed evaluation of disease dissemination, severity, and unexpected areas of involvement in primary immunodeficiency disorders with multisystem involvement.
In this case, featuring a pathogenic LRBA variant, F-18 FDG PET-CT revealed involvement across numerous systems, including lymphoproliferative, lung, liver, bowel, bone, bone marrow, joint, and tendon involvements. This underscores the utility of FDG PET-CT in comprehensively understanding and managing such complex conditions.
This study has certain limitations. Notably, there was no histopathological evaluation of some system involvements identified on F-18 FDG PET-CT. However, the observed foci of increased metabolic activity—unusual for this age group—were interpreted as findings associated with LRBA deficiency. Evaluation of central nervous system involvement should ideally have been conducted using MRI. Additionally, because the F-18 FDG PET-CT scan was performed on a previously diagnosed patient undergoing immunomodulatory treatments, the activity-uptake characteristics of the lesions in different systems may not fully reflect their true metabolic activity.
In newly diagnosed patients, PET-CT imaging performed both before and after treatment initiation could uncover variability in the glycolytic phenotype, offering valuable insights into disease behavior and the predictive power of molecular imaging.
Conclusions
In cases of LRBA deficiency with a broad clinical spectrum, the F-18 FDG PET-CT method offers significant value to patient management. It enables detailed assessment of disease spread and severity, facilitates treatment planning, monitors treatment response, and demonstrates multisystem involvement. This imaging modality holds great potential in guiding comprehensive care for such complex disorders.
Authors’ Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Footnotes
Acknowledgments
The authors thank the patient and his family for their continued enthusiasm and willingness to enable this case report and the Erciyes University Genetics Department for their guidance and work.
Author Disclosure Statement
No competing financial interests exist. All authors declare that they have no conflicts of interest that are relevant or could be considered relevant to the article.
Funding Information
No specific grant was received for this research from any public, commercial, or not-for-profit sector funding agency.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the parents of the individual for participation in the study and the publication. All procedures performed were in accordance with the ethical standards of the institutional and national research committee.
Data Deposition and Access
Because of the identifiable nature of this rare disease, data from this project may be available on request from the corresponding author.