
Abstract
Measles is a highly contagious, vaccine-preventable infectious disease. The incidence of measles has been rising due to a confluence of factors, including international travel and vaccine hesitancy. The purpose of this Pharmacotherapy Update was to examine and appraise preventive measures and treatment options, both pharmacotherapy and supplements, used in measles management. Topics included ribavirin, measles-mumps-rubella vaccine post-exposure prophylaxis, immune globulin, antibiotics, vitamin A, and cod liver oil supplements. Parents, caregivers, and policymakers considering these interventions are recommended to consult with health care providers and seek guidance from professional organizations regarding the effectiveness and safety of these treatments. Vaccination with the measles-mumps-rubella vaccine remains the most effective intervention to prevent measles, and efforts are urgently needed to achieve the requisite 95% vaccination rate to improve public health, confer herd immunity, and eradicate measles.
Introduction
Since 2022, there has been a dramatic global increase in measles infections. Reported cases surged by 224% between 2022 and 2023, from 205,173 to 663,795. 1 The World Health Organization (WHO) reported cases in its European Region in 2024 were the highest they have been since 1997 and continued to increase worldwide. 2 In 2024, measles cases and outbreaks occurred in 27 of the 33 member states in the WHO European region, many of which had previously declared measles eliminated. 3 To combat measles epidemics over the last two decades, several European countries implemented policies mandating routine and catch-up vaccines and engaged and educated local communities to improve vaccine knowledge and access and reduce mistrust.4–6
Measles, declared eliminated in the United States (US) in 2000, has also seen outbreaks return over the past decade, primarily due to cases brought in by travelers and a lack of immunity within the population.7,8 From September 30, 2018, to July 15, 2019, a total of 649 measles cases were reported in the US, with 49 hospitalizations and no deaths. 9 This outbreak marked the highest number of cases recorded since 1992 and since measles was declared eliminated in 2000. However, as of November 5, 2025, there have been a total of 1,681 cases of measles in 42 states reported, including 203 hospitalizations and three deaths. 10 The resurgence of measles infection is multifactorial including declining global immunization rates, international travel, and vaccine hesitancy. Vaccine hesitancy is a major contributor, often stemming from unfounded fears about vaccine safety, particularly the disproven link between vaccines and autism, concerns about overwhelming the immune system, complacency regarding the risk of contracting the illness, and issues with vaccine convenience and access.11,12 The coronavirus disease-2019 (COVID-19) pandemic exacerbated these challenges, causing disruptions to routine immunization programs and leading to a decrease in vaccination rates, especially among infants born during 2020–2021. 13 This decline in vaccination coverage undermines herd immunity and increases the risk of outbreaks. The dangers of measles, including severe complications and mortality, are averted by adequate vaccination.
Measles is a highly infectious illness caused by an RNA paramyxovirus spread through large respiratory droplets from infected individuals. 14 Droplets can remain airborne for up to 2 h, increasing the risk of nonimmunized individuals contracting the infection. For household contacts, up to 90% of susceptible people will develop illness with measles. Measles typically presents with a prodromal phase characterized by fever, cough, coryza, and conjunctivitis, indicating the onset of the disease without the characteristic rash of a measles infection. 15 The prodromal phase presents 2–4 days prior to the rash in which the measle virus is most contagious, making rapid diagnosis critical to prevent spread. During the prodromal phase, up to 70% of patients present with Koplik’s spots, described as small, bluish-white spots on the buccal mucous membrane primarily on the inside of cheeks and on the lips. 16 Following the prodromal phase, the characteristic maculopapular rash begins with the initial appearance of the rash on the face and neckline, progressing to the trunk and extremities. The rash may persist from 3 to 5 days with resolution occurring in the same manner of appearance. In uncomplicated cases of measles, the infection typically resolves within 1 week. In some cases, a cough can persist for 10 days. 17
Because the measles virus targets epithelial cells and infects multiple organs, complications have been reported in all organ systems. 17 The most common complications from a measles infection in the respiratory tract are otitis media and pneumonia. Other less common but severe complications include encephalitis, subacute sclerosing panencephalitis, and acute disseminated encephalomyelitis, which may lead to severe neurologic impairments or death. The most common cause of death is due to pneumonia due to the measles virus with or without another viral infection or a bacterial superinfection. 18
Infants, children less than 5 years old, and adults are at high risk of complications. Infection during pregnancy may lead to miscarriage, preterm delivery, low neonatal weight, and maternal fatality. In individuals with immunosuppression involving T-cells (eg, congenital T-lymphocyte dysfunction, bone marrow transplant, chemotherapy, immunosuppressive doses of corticosteroids), the fatality rate approaches 55%. 17 Overcrowding and malnutrition, which are widespread globally, increase the risk of complications from infectious diseases.
Before the introduction of the highly effective measles vaccine, nearly everyone in the population was infected by adolescence. With such a high number of cases, complications were frequently seen, including approximately 48,000 hospitalizations, 1,000 cases of encephalitis, and 400–500 deaths. The highly effective measles vaccine transformed the situation, providing 93% protection from the first dose and 97% after the recommended second dose. A live attenuated vaccine is generally safe with rare adverse events like febrile seizures (occurring in 1 case per 200–4,000 vaccinated children) or immune thrombocytopenia (occurring in 1 case per 40,000 vaccinated children), which are significantly less common and severe than complications from the natural infection itself. Achieving herd immunity, which protects vulnerable individuals including infants who may have waning maternal antibodies, requires approximately 95% of the population to be immune. In 2023, the measles vaccine coverage rates worldwide were 83%, while the coverage rates in the US were 92.7% for school-aged children.6,19,20 In the US, the recommended measles vaccine schedule is two doses: the first between 12 and 15 months and the second at 4–6 years. 21 The WHO recommends the first measles vaccine dose at 9 months and the second dose between 15 and 18 months in countries with ongoing transmission to reduce infant mortality. 22 The vaccine comes in two forms, MMR (measles, mumps, rubella) and MMRV (measles, mumps, rubella, and varicella), which are similarly effective. 21
Treatment for measles remains largely supportive, as limited data are available demonstrating conclusive effectiveness and safety.
Pharmacotherapy
Antivirals
Among the antivirals currently available, none have demonstrated clinical efficacy against measles infections and thus are not approved by the US Food and Drug Administration (FDA) or endorsed by any guidelines. Ribavirin, which is used off-label for respiratory syncytial virus (another paramyxoviridae virus), has been investigated as a potential treatment option due to its relatively broad activity against both DNA and RNA viruses. 23
In vitro data indicate successful inhibition of measles replication, 24 but clinical data are limited to two randomized, placebo-controlled trials in the pediatric population.25,26 In the first, conducted by Pal and colleagues, 100 patients diagnosed with measles and ranging from 6 months to 47 years of age were treated with either ribavirin or placebo along with supportive care. 25 Pediatric patients received a syrup formulation at a dose of 20 mg/kg/day in four divided doses; no further information on study design or quantity of pediatric patients was provided. Compared to the placebo group, those treated with ribavirin had a reduction in duration of constitutional symptoms (mean 3.2 ± 0.6 days compared to 7.3 ± 0.8 days), a reduction in duration of rash (2 ± 1 day compared to 5 ± 1 day), and a decreased incidence of respiratory, gastrointestinal, and encephalitis complications (zero compared to 22 respiratory, 16 gastrointestinal, and 3 encephalitis) noted, although no statistical analyses were performed. No information was provided regarding ribavirin’s tolerability.
The second study was a double-blind trial conducted by Uylangco and colleagues in 40 patients ranging from 1 to 12 years of age. 26 Each was diagnosed with measles, but those with complications, a history of asthma or obstructive lung disease, or who received gamma globulin were excluded. Patients received either ribavirin 10 mg/kg/day in four divided doses for 7 days or a matching placebo. Investigators noted a difference in fever duration in those on ribavirin compared to placebo (2.35 ± 1.01 days compared to 3.7 ± 1.19 days). The development of respiratory complications in those on ribavirin occurred in 20% compared to 35% in those taking placebo. However, statistical analyses were not performed. Lab abnormalities, either hematological or chemical, were not observed in any patient.
The inconsistency in dosing strategies and incomplete study design reduced the applicability of this evidence to the general pediatric population. Furthermore, ribavirin is associated with significant hematological abnormalities: neutropenia (incidence as high as 40%), anemia (35%), and thrombocytopenia (8%). It carries a boxed warning for hemolytic anemia and is a known teratogen. 23 A final consideration is the availability of ribavirin formulations. While 200 mg capsules and tablets are commercially available, an oral suspension would need to be compounded to provide ease of administration and accurate weight-based doses to pediatric patients. 27 An intravenous formulation is available via an emergency investigational new drug application through the US FDA.
At the time of this writing, no clinical trials are underway for antiviral measles treatment. As such, prevention with routine vaccinations must remain a mainstay of controlling the virus.
Post-exposure prophylaxis
For those in whom the vaccine is contraindicated, such as in severe immunosuppression, or those in whom vaccination has not been performed or is incomplete, the use of post-exposure prophylaxis (PEP) can be considered to reduce the risk of infection development or alter the course of infection. 28 PEP may consist of administration of the MMR live attenuated vaccine or passive immunity with immune globulin (IG). These methods have estimated effectiveness rates of 83.4% to 100% for the MMR vaccine and 76% to 100% for IG. 29
MMR vaccine
Individuals who are unvaccinated or who have only received one dose may receive benefit if the MMR vaccine can be administered within 72 h of exposure in limited contact settings, such as schools, daycares, and medical offices. Such a high rate of effectiveness is not maintained in more intense contact settings, such as households. For individuals over 6 months old who are not immunocompromised or pregnant, either the MMR or MMRV vaccine is the preferred method for PEP. Of note, the MMR vaccine is recommended in those living with HIV with a CD4 count over 200 cells/mm3 due to a lack of data with the MMRV vaccine in this population. 28
In the event of a measles outbreak, immunization guidance allows for more aggressive administration in cases of ongoing exposure. Initiating the MMR vaccine can be considered in infants as young as 6 months of age, rather than 12 months of age, which is typically recommended. Should an infant receive their first dose prior to 12 months of age, they would still need a 2-dose series beginning at 12 to 15 months of age. 8 In those who are at least 1 year of age and have received only one dose, a second dose can be administered if at least 28 days have elapsed since the first dose, rather than waiting until 4 to 6 years of age.14,28
Immune globulin
For those who miss the 72-h window for vaccine PEP, immune globulin (IG) can be considered. IG is also indicated for severe immunocompromise (eg, HIV), pregnant persons who are not vaccinated, or infants less than 6 months of age. 28 Infants in this age group lack sufficient humoral immune maturity to mount an adequate response to vaccination and are expected to have waning maternal antibodies. This is particularly relevant when maternal immunity is secondary to immunization as opposed to past infection, which provides a more robust immunological response.14,28
IG can be administered via the intramuscular, intravenous, or subcutaneous routes, but the intravenous route is recommended. The intravenous immune globulin (IVIG) must be administered within 6 days of exposure. 29 Of note, the potency of IG products has waned over time due to collection from donors whose antibodies are harvested from vaccine-exposed populations instead of those with a history of measles infection, which provides higher antibody titers. As such, higher IG doses are needed to confer similar protection. 28 This caveat has decreased the utility of intramuscular IG in older children, as the recommended dose of 0.5 mL/kg will exceed the maximum volume for administration (15 mL) to a child who weighs 30 kg or more. 30 Subcutaneous IG requires pump administration and multiple weekly doses. Thus, IVIG is recommended at a dose of 400 mg/kg with close monitoring for infusion-related reactions. 14 Those who have received at least one dose of the MMR vaccine should not need IG, as they are thought to have sufficient immunity to have a relatively low risk of measles infection and associated complications unless severely immunocompromised.
Antibiotics
Administration of antibiotics to prevent secondary complications after measles infection also lacks strong evidence. A systematic review focusing on children was performed in 2013 and found that nearly all studies on this topic were performed prior to 1970 using inadequate research methods and prescribed antibiotics that are either no longer used as empiric therapy for respiratory infections or avoided in pediatric patients based on age (eg, penicillin, tetracycline, sulfamethoxazole/trimethoprim). 31 Additionally, the risk of developing antibiotic resistance cannot be overstated. Monitoring for the development of bacterial complications, such as otitis media and pneumonia, for prompt treatment should remain a significant component of the management of measles.
Vitamins and supplements
Given the lack of data supporting the effectiveness of antivirals and antibiotics, the brief eligibility period to administer vaccine PEP, and the practical limitations of IVIG, patient, caregiver, and policymaker interest in vitamins and supplements to treat and prevent measles has garnered media attention. 32 Some entrepreneurs market vitamins and supplements to vaccine-hesitant populations, offering products as alternatives to vaccinations. 5 Importantly, vitamins and supplements do not prevent measles infection; the most effective preventive measure is vaccination.
Vitamin A
Vitamin A is a fat-soluble vitamin necessary for growth and development, vision, and immunity. 33 Retinoids (ie, retinol and retinal) are forms of vitamin A, and common dietary sources include dairy, fish, and orange- and green-colored fruits and vegetables. 34 Plants synthesize carotenoids (ie, beta-carotene), which are converted to vitamin A after ingestion. Malnutrition, including vitamin A deficiency, is a risk factor for severe measles. Measles may deplete stored vitamin A in the liver, or vitamin A release from the liver may be insufficient (too slow) to meet homeostasis during infection. 35 Though vitamin A deficiency may be asymptomatic, some children will present with xerophthalmia and anemia.
The WHO and American Academy of Pediatrics (AAP) recommend vitamin A treatment for children with measles.14,20 Doses and clinical considerations are presented in Table 1. Summarily, one daily dose for 2 days is recommended for most children, though a third dose (2–6 weeks following the second dose) is recommended if vitamin A deficiency is diagnosed. Depending on the manufacturer and formulation, the active ingredient of vitamin A differs from product to product (eg, beta carotene 25,000 units versus retinyl palmitate 8,000 units); clinicians and caregivers alike must review the product label to determine the amount of vitamin A per supplement serving size. Vitamin A treatment is well-tolerated. 34 Children who are also using retinoids for the treatment of acne (ie, tretinoin, isotretinoin, adapalene) are at risk for hypervitaminosis A, and thus these medications should be withheld during concomitant vitamin A treatment and for 7–14 days thereafter. 36
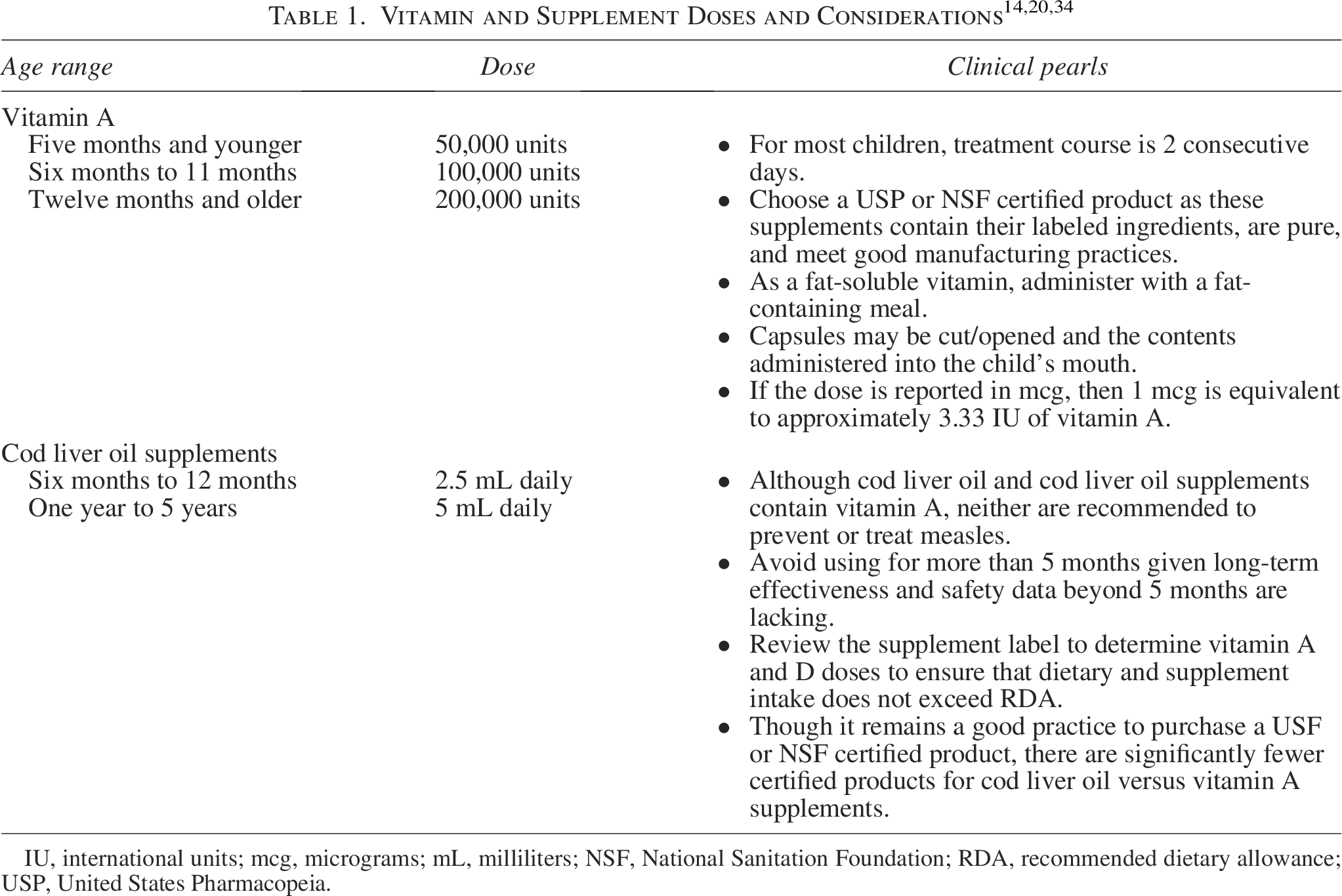
IU, international units; mcg, micrograms; mL, milliliters; NSF, National Sanitation Foundation; RDA, recommended dietary allowance; USP, United States Pharmacopeia.
America’s Poison Centers have reported a 38% increase in vitamin A exposures and overdoses in 2025 compared to 2024. 37 Chronic vitamin A use (at doses recommended to treat measles) is not recommended because it increases the risk for hypervitaminosis A and all-cause mortality. 34 Signs and symptoms of vitamin A overdose include gastrointestinal distress, headache, visual changes, and ostealgia. Parents and caregivers should not administer vitamin A to treat measles in the absence of physician consultation and oversight.
Though the WHO and AAP recommend vitamin A, the current body of evidence suggests vitamin A possibly reduces mortality in children less than 2 years (RR: 0.57, 95% CI: 0.25–0.66) and the incidence of croup (RR: 0.53, 95% CI: 0.29–0.89).14,20,35 Vitamin A does not prevent measles, and its use should be restricted to only children who have contracted measles.
Cod liver oil
Cod liver oil is oil from the liver of Atlantic cod (fish); it should not be confused with fish oil, which is oil from the body of fish and/or shellfish. Though cod liver oil also contains omega-3 fatty acids, docosahexaenoic acid and eicosapenaenoic acid, cod liver oil supplements should not be confused with or considered analogous to omega-3 fatty acid supplements because most cod liver oil supplements do not contain omega-3 fatty acids. 34
As a food, cod liver oil itself is replete with vitamins A, D, and E and omega-3 fatty acids; however, cod liver oil supplements generally contain vitamins A and D, but amounts vary substantially between products. The United States Pharmacopeia estimates that every 1 gram of cod liver oil supplement may contain between 600 and 2,500 units of vitamin A and 60 and 250 units of vitamin D, and every 5 mL of cod liver oil may contain between 2,700 and 11,250 units of vitamin A and 270 and 1,125 units of vitamin D. Neither the WHO nor AAP recommends cod liver oil or supplements as preventive therapy or treatment for measles, though supplements may be an acceptable source of vitamins in children whose diet lacks these nutrients. Safe doses of cod liver oil supplements in children are presented in Table 1. Cod liver oil supplements are well-tolerated and side effects are mostly limited to gastrointestinal complaints. 34
Though cod liver oil supplements contain vitamin A, they should be avoided as a source of vitamin A to treat measles given the overdose potential attributable to the other components (ie, vitamin D and inactive ingredients) in the supplement.
Conclusion
Measles is a highly infectious, vaccine-preventable disease with no evidence-based effective treatment. Vaccination is the most effective intervention to prevent infection in children and at-risk populations; however, recent trends have resulted in unvaccinated individuals. Other preventive strategies available once exposed include vaccine PEP or IG in severe immunocompromise people, pregnant people, or infants less than 6 months of age. Vitamin A is recommended to treat measles, though it should occur under the supervision of a physician or health care professional given the risks for vitamin A toxicity. Though cod liver oil supplements contain vitamins A and E, cod liver oil supplements should not be used to prevent or treat measles. Given measles’ contagiousness and sequelae, all suspected and confirmed cases of measles must be managed by supervising health care professionals.
Authors’ Contributions
M.M.O.: Writing—original draft; writing—review and editing; S.B.: Writing—original draft; writing—review and editing; P.M.B.: Conceptualization; writing—original draft; writing—review and editing; supervision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This Pharmacotherapy Update was unsupported by funding.