
Abstract
Background:
Drug-induced anaphylaxis is increasingly reported in children, and multiple drug allergy syndrome (MDAS) poses therapeutic challenges. Desensitization may be considered when no alternative therapy exists. Nitrofurantoin is widely used for uncomplicated urinary tract infections (UTIs); however, anaphylaxis related to it has been rarely described, and no cases of desensitization have been reported.
Case Presentation:
We present the case of an 8-year-old girl with recurrent UTIs and MDAS who had experienced anaphylaxis to amoxicillin and nitrofurantoin, as well as urticaria associated with aminoglycosides and cephalosporins. After isolation of Escherichia coli resistant to multiple antibiotics but sensitive to nitrofurantoin, a rapid 12-step oral desensitization protocol was implemented under close monitoring. The procedure was well tolerated without systemic reactions, and nitrofurantoin prophylaxis was successfully initiated.
Conclusions:
To the best of our knowledge, this is the first reported case of successful nitrofurantoin desensitization in a child with MDAS, providing a potential therapeutic option for similarly high-risk scenarios.
Introduction
Drug-induced anaphylaxis has been increasingly reported in children in recent decades and represents an important cause of anaphylaxis-related mortality. 1 It is estimated that 5% of pediatric anaphylactic reactions in Europe between 2007 and 2015 were drug related. 2 A multicenter study from Turkey demonstrated that drugs were the leading triggers in 21% of childhood anaphylaxis cases. 3 Moreover, the incidence of drug-induced anaphylaxis was shown to be significantly higher in children aged 7 years and older compared with infants and younger children. Multiple drug allergy syndrome (MDAS) is defined as hypersensitivity to two or more structurally and pharmacologically unrelated drugs and has been primarily documented in adult populations. 4 In low-risk populations without a history of hypersensitivity, the prevalence of MDAS is ∼1.2%, whereas it ranges from 0% to 36% among individuals with known or suspected drug allergies. Drug desensitization is considered when no suitable alternative therapy is available. 5
Nitrofurantoin is widely used for the treatment of uncomplicated urinary tract infections (UTIs) owing to its high efficacy and low rates of antimicrobial resistance. 6 Although rare, nitrofurantoin-induced anaphylaxis has been reported, most often in women. 7 Nitrofurantoin is also known to cause acute pulmonary toxicity, a rare but often fatal hypersensitivity reaction in adults. In addition, long-term use, particularly in patients with renal dysfunction, may lead to chronic pulmonary toxicity and pulmonary fibrosis.6,8 In both scenarios, discontinuation of the drug represents a first-line intervention; however, to the best of our knowledge, nitrofurantoin desensitization has not yet been reported. Therefore, we describe the first reported case of successful oral nitrofurantoin desensitization in a child with MDAS. 9
Case
An 8-year-old girl with a history of recurrent UTIs and multiple drug allergies, including two prior episodes of anaphylaxis to amoxicillin and nitrofurantoin, was referred to our pediatric allergy and immunology clinic for further evaluation and treatment after the growth of Escherichia coli in her urine culture.
Her medical history revealed that an initial prophylactic regimen with cefuroxime-axetil had been started by the pediatric nephrology department at another city. She tolerated for ∼18 months until she developed acute urticaria within minutes of administration. Four months later, she was hospitalized and treated with intravenous amikacin after E. coli was again cultured; however, she developed acute urticaria shortly after the first dose, prompting immediate drug discontinuation and antihistamine therapy. Prophylaxis was subsequently switched to nitrofurantoin, but the patient developed a truncal rash within minutes after the initiation of therapy, followed by dyspnea ∼20 min later. She was transferred to the emergency department, though treatment details were unavailable. Amoxicillin prophylaxis was then recommended by her nephrologist. Before treatment commencement, due to her past relevant drug allergy history, she was referred to the pediatric allergy clinic at the same center, where skin prick testing with penicillin G and ampicillin, followed by an oral provocation test with phenoxymethylpenicillin were performed, with both resulting negatively. Following these procedures, an oral provocation with amoxicillin was initiated but resulted in biphasic anaphylaxis. A subsequent urine culture revealed E. coli growth that was sensitive to amikacin, gentamicin, and cefixime. Owing to its structural similarity to cefuroxime, a rapid desensitization protocol with cefixime was performed successfully, and the patient was maintained on cefixime prophylaxis.
Her past medical history was otherwise unremarkable. However, her family history revealed that her father, aunt, and some of her cousins had experienced difficulties tolerating various medications, although they could not explain either the medications or the reactions, and there was no official medical documentation of their reactions.
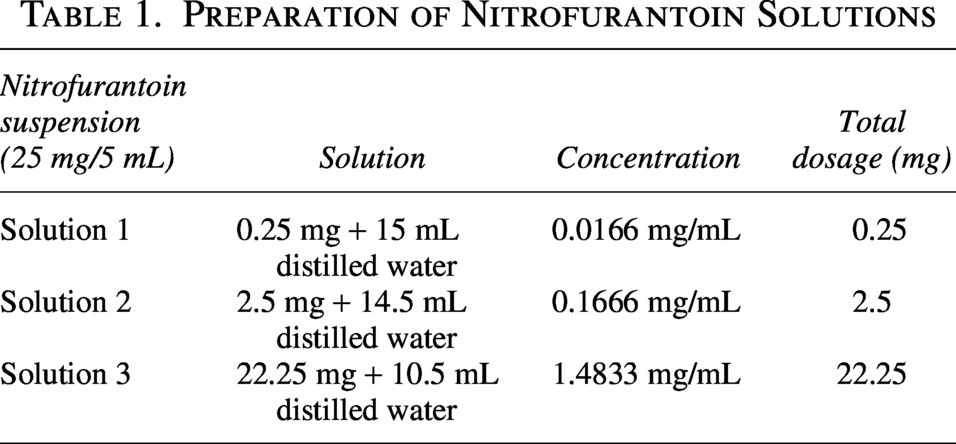
The patient was referred to our clinic after cefixime-resistant E. coli was isolated in her urine culture within 1 year of follow-up. We initially performed a single-dose graded challenge test with gentamicin successfully, and her treatment was completed with gentamicin. Subsequently, her prophylaxis regimen was switched to trimethoprim–sulfamethoxazole (TMP–SMX). Despite having been on prophylaxis for 2 months, an E. coli growth sensitive to ciprofloxacin, levofloxacin, ertapenem, piperacillin–tazobactam, gentamicin, and nitrofurantoin, and resistant to ampicillin, amoxicillin, cefazolin, cefixime, and TMP–SMX was detected in her urine culture. Considering that ciprofloxacin can be used both orally and prophylactically, we decided to administer a single-dose graded challenge test with intravenous ciprofloxacin (13 mg/kg). Within minutes of initiating this, a rash developed on her upper body, spontaneously regressing without any treatment in a few minutes. She had no other systemic symptoms, and her blood pressure remained stable. Serum tryptase level was within normal limits. Rashes were observed on her trunk while applying ciprofloxacin on numerous occasions. While under treatment with ciprofloxacin on the 11th day, the patient’s urine culture grew ciprofloxacin-resistant E. coli, and the treatment was completed in 14 days. As the microorganism remained sensitive to gentamicin, a graded challenge test with gentamicin (1.5 mg/kg/dose) was successfully completed, and therapy was switched to gentamicin accordingly. After completing medication and sterilizing the urine culture, voiding cystourethrography revealed grade III vesicoureteral reflux in the left collecting system, along with bladder dysfunction. Following consultation with the pediatric nephrology department, nitrofurantoin was selected because the patient’s urine cultures showed resistance to both cefixime and TMP–SMX. Nitrofurantoin was chosen specifically due to the low rates of bacterial resistance reported in the literature for this agent. We initiated a 12-step rapid oral desensitization protocol to reach a maintenance dose of 2 mg/kg/day, starting with an initial dose of 1 mg/kg. Informed consent was obtained from the patient’s caregivers. On the day prior to testing, she was premedicated with systemic methylprednisolone (1 mg/kg at −13, −7, and −1 h) and hydroxyzine (−1 h). The patient was monitored at each step, and her vital signs were checked, and emergency equipment was kept ready in case of a systemic reaction.
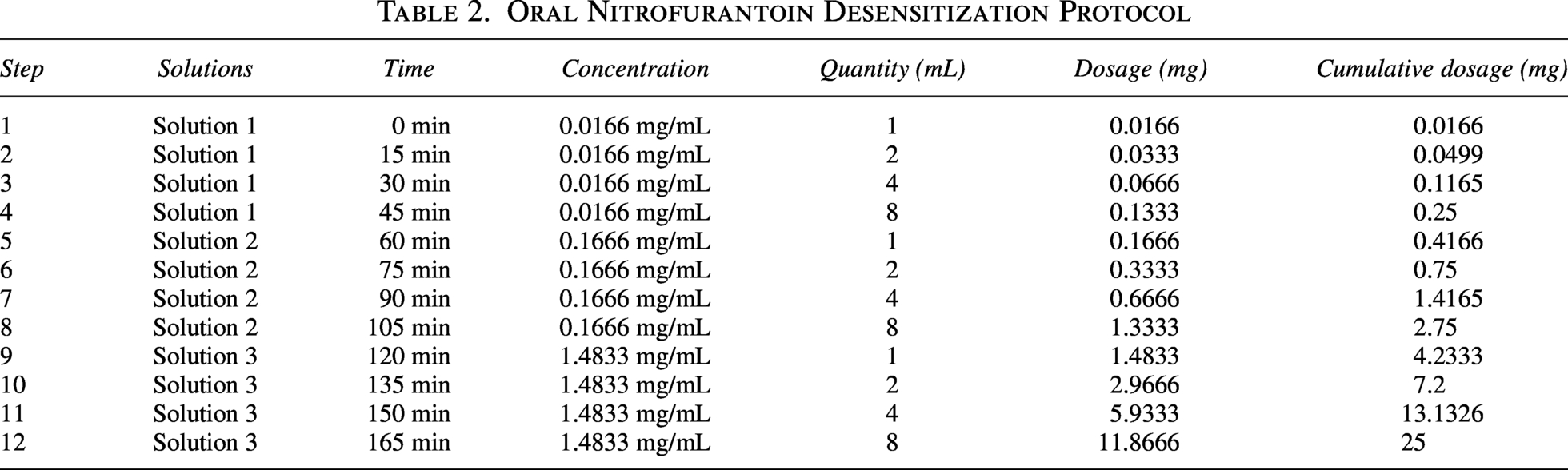
The preparation of nitrofurantoin solutions is summarized in Table 1, and the desensitization protocol is presented in Table 2.
Preparation of Nitrofurantoin Solutions
Oral Nitrofurantoin Desensitization Protocol
A timeline summary of the patient’s drug allergy history is provided in Figure 1.
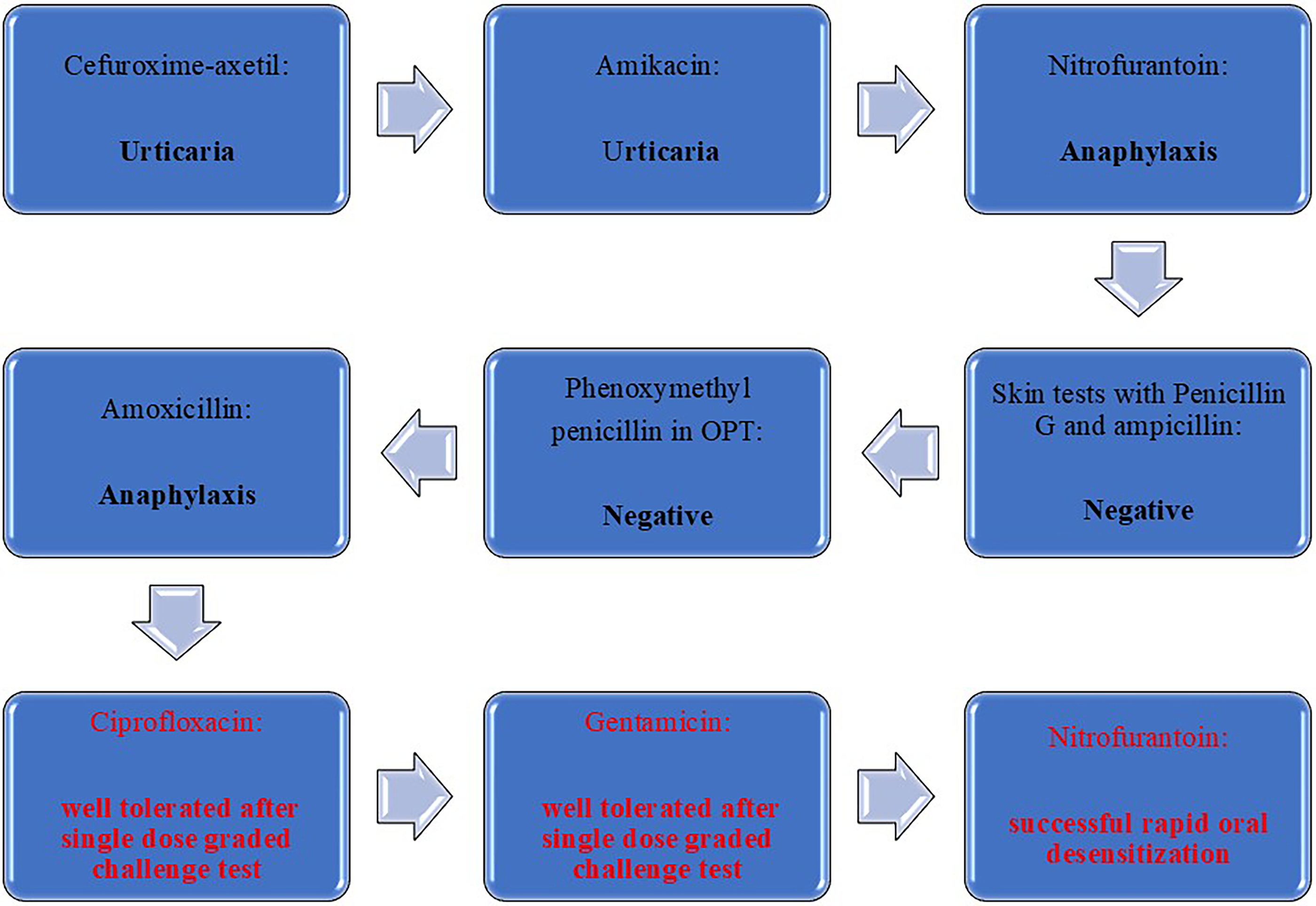
Timeline shows the patient’s reactions and test results: black text indicates previous history of allergies, and red text indicates procedures performed in our center.
The protocol was completed, and desensitization was carried out successfully. Subsequently, the patient was started on regular nitrofurantoin prophylaxis twice daily, and she has been continuing treatment without any reaction.
Discussion
In patients diagnosed with drug allergy, desensitization to the culprit drug is considered when no suitable alternative therapy exists, particularly in cases involving multidrug-resistant infections.
10
However, pediatric desensitization protocols remain limited and are commonly adapted from adult studies. Candidates for desensitization typically include patients with type I and certain mild-to-moderate type IV hypersensitivity reactions, such as fixed drug eruptions and maculopapular eruptions.
11
In contrast, desensitization is contraindicated in type II cytotoxic reactions, type III serum sickness
To the best of our knowledge, this is the first documented case of successful nitrofurantoin desensitization in a child with a history of anaphylaxis to both amoxicillin and nitrofurantoin, for whom nitrofurantoin prophylaxis was ultimately deemed essential due to recurrent UTIs. Several factors contributed to the decision to pursue desensitization: the recognition that nitrofurantoin represented the only viable prophylactic option to improve the patient’s clinical course, the experience of the treatment team in managing pediatric drug hypersensitivity, and the cooperation of the patient and her caregivers. This case emphasizes the importance of individualized decision-making in pediatric desensitization, particularly when rare agents such as nitrofurantoin are involved.
Conclusion
Drug hypersensitivity reactions, particularly anaphylaxis, may prevent patients from receiving optimal therapy. Patient-specific desensitization protocols—implemented after careful patient selection, individualized risk–benefit assessment, and informed consent—can provide access to the most effective treatment. It is essential, though, to be prepared for both early and delayed hypersensitivity reactions that may occur during and after the procedure and ensure their prompt recognition and appropriate management. Each reported case of drug desensitization contributes valuable insights that help select suitable candidates, guide the standardization of pediatric protocols, and expand therapeutic options for children with limited alternatives.
Ethics Approval and Consent to Participate
According to institutional policies, ethics committee approval was not required for this case report. Written informed consent for publication was obtained from the patient’s legal guardian.
Consent for Publication
Written informed consent for publication was obtained.
Authors’ Contributions
Y.O. participated in the clinical management of the patient, drafted the article, and coordinated the submission and revision process. A.S. assisted during the preparation and administration of the desensitization protocol and monitored the patient for adverse reactions. E.C. previously followed the patient in the allergy clinic and initiated prophylactic treatment under close outpatient monitoring, participated in the patient’s follow-up at our center, and contributed to the administration of the desensitization protocol. C.U. and E.B. participated in the preparation and administration of the desensitization solutions, contributed to the acquisition of clinical data, and monitored the patient throughout the protocol. P.G. was primarily responsible for the patient’s clinical management, evaluated therapeutic alternatives, made the decision to proceed with oral nitrofurantoin desensitization, developed the desensitization protocol, performed the literature review, contributed to the conceptualization and presentation of the article, and critically revised the article for important intellectual content. C.A. contributed to the design of the desensitization protocol and critically revised the article for important intellectual content. All authors reviewed, approved, and agreed to be accountable for all aspects of the work.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.