
Abstract
Background:
The Ehlers–Danlos syndromes (EDSs) are a group of connective tissue disorders characterized by skin laxity and hypermobile joints. EDS is associated with many comorbidities that often necessitate multidisciplinary care. Adults with EDS report more atopic conditions such as allergic rhinitis and asthma; however, gaps exist around the prevalence of atopic conditions in pediatric patients with EDS. The objective of this study was to determine the prevalence of atopic conditions (allergies, asthma, and atopic dermatitis) in pediatric patients with hypermobile EDS (hEDS) and compare it to the general pediatric population in the United States.
Methods:
A convenience sample of 149 patients aged 8–22 years, with a diagnosis of hEDS and atopic disease was evaluated. Atopic conditions and medication use were reviewed.
Results:
Patients were mostly females (85%) and Caucasian (89%) with an average age of 15.5 years (standard deviation: 3.1). Many patients had allergic rhinitis (46%); medication allergies (44%), with antibiotics as the most common; and asthma (39%), mild intermittent as the most common severity. All prevalences were higher compared to the general United States pediatric population except for atopic dermatitis.
Conclusions:
There was an increased prevalence of atopic conditions in pediatric patients with hEDS compared to the United States pediatric population. Due to the increased prevalence of atopic conditions, health care providers should be aware of and monitor for signs of atopic and allergic conditions in pediatric patients with hEDS. Allergy and pulmonology specialists should be considered in the management of pediatric patients with hEDS if symptoms are present.
Introduction
The Ehlers–Danlos syndromes (EDSs) are a group of heritable connective tissue disorders defined by hyperextensible, fragile skin and hypermobile joints. There are 14 different subtypes that are identified by distinct clinical features and genetic abnormalities, however, the hypermobile subtype does not have a known genetic abnormality. 1 Hypermobile EDS (hEDS) is believed to be autosomal dominant due to identified inheritance patterns; however, the lack of a monogenic abnormality has led to the belief that hEDS is likely multifactorial. 2 hEDS is diagnosed with the 2017 International Classification of the EDS when an individual meets criteria for generalized joint hypermobility per the Beighton score, has supportive skin and musculoskeletal features and no other underlying condition has been identified to explain the clinical features. 3 Of all the subtypes, hEDS is the most common with a prevalence of 1 in 500 people, 4 however, it is still underdiagnosed due to lack of awareness by medical providers. 5 Furthermore, care for individuals with hEDS can be complex due to the high prevalence of comorbid symptoms and conditions that include fatigue and sleep disfunction, 6 chronic pain, 7 gastrointestinal disorders, 8 dysautonomia 9 and headaches. 10 The abundance of comorbid symptoms and conditions has been shown to have a negative impact on quality of life for people with hEDS,6,11 which has led to the development of the Spider questionnaire (31 items across 8 domains [pain, fatigue, neuromusculoskeletal, cardiac, urogenital, gastrointestinal, anxiety, and depression]), which has been validated in adolescents with hEDS to recognize the presence and impact of symptoms and conditions, 12 and recommendations to provide comprehensive, multidisciplinary health care to support and manage patients with hEDS. 13
Studies of atopic conditions in adults with EDS show that asthma is one of the most common comorbidities associated with EDS, 14 and atopic disease was seen in a higher prevalence of patients with EDS when compared to controls. 15 Food allergies have also been reported at a higher prevalence in adults with EDS compared to those without EDS, 16 while atopic dermatitis is present in 23% of adult patients with EDS compared to 10% of the general adult population without EDS.13,14 While studies show that atopic disease is prevalent in adults with EDS, gaps in knowledge exist around the prevalence of atopic disease in pediatric patients with EDS. For children without EDS atopic conditions are prevalent, with 25% of children that have at least 1 allergic condition, 15 while 6% have food allergies, 19% have seasonal allergic rhinitis, 11% have atopic dermatitis, and 6% have asthma.15,16 While atopic conditions are prevalent in the pediatric population of the United States and adults with EDS, the prevalence of atopic conditions in pediatric patients with EDS has not been determined. The objective of this study was to determine the prevalence of atopic conditions (allergies, asthma, and atopic dermatitis) in pediatric patients with hEDS and compare it to the general pediatric population in the United States.
Materials and Methods
As part of a longitudinal study of 232 patients, aged 8–22 years, that took place in a multidisciplinary EDS clinic in the Midwest United States (that evaluates and treats hEDS), a convenience cohort of 149 patients was identified between January 2018 and 2023 that met inclusion criteria, which included a previous diagnosis of at least 1 “atopic condition” (as defined by a diagnosis of food allergies, allergic rhinitis, asthma, or atopic dermatitis) and a confirmed diagnosis of hEDS (as defined by the 2017 International Classification for Ehlers Danlos Syndromes 3 ) The diagnosis of hEDS was made or confirmed in the multidisciplinary EDS clinic by a geneticist and genetic counselor during the study time period, and the study took place prior to the development of the pediatric generalized joint hypermobility framework. 17 Chart review was conducted, and patient data was extracted from medical records, which included symptoms, co-morbid diagnoses, subspecialty care received, and current medication usage. Demographic information was obtained. Atopic condition information was extracted from allergy and dermatology clinic notes to confirm diagnoses. Asthma information and severity were extracted from pulmonology clinic notes, and if no diagnostic severity was indicated, asthma severity was determined based on the extracted symptoms and medication list using a reference sheet from the National Heart, Lung, and Blood Institute. 18 This study was reviewed and approved by the local institutional review board (IRB: 00001628), and verbal consent and assent were obtained prior to enrollment in the study.
Statistical analysis
Numerical variables were summarized as means and standard deviation (SD), while binary and categorical variables were summarized as frequencies and percentages. Chi-square tests of independence were conducted to assess significant associations between the diagnoses of EDS and food allergies, allergic rhinitis, asthma, and atopic dermatitis. Chi-square statistics, degrees of freedom, and P value were computed to assess statistical significance. The significance level was set at α = 0.05. The effect size was calculated using a phi coefficient. The parameters used were small (0.1), medium (0.3), and large (0.5). The Mann–Whitney U test was performed to compare the prevalence of atopic diseases between pediatric patients with EDS and the United States pediatric population. All statistical analysis was completed using Microsoft Excel version 16.94.
Results
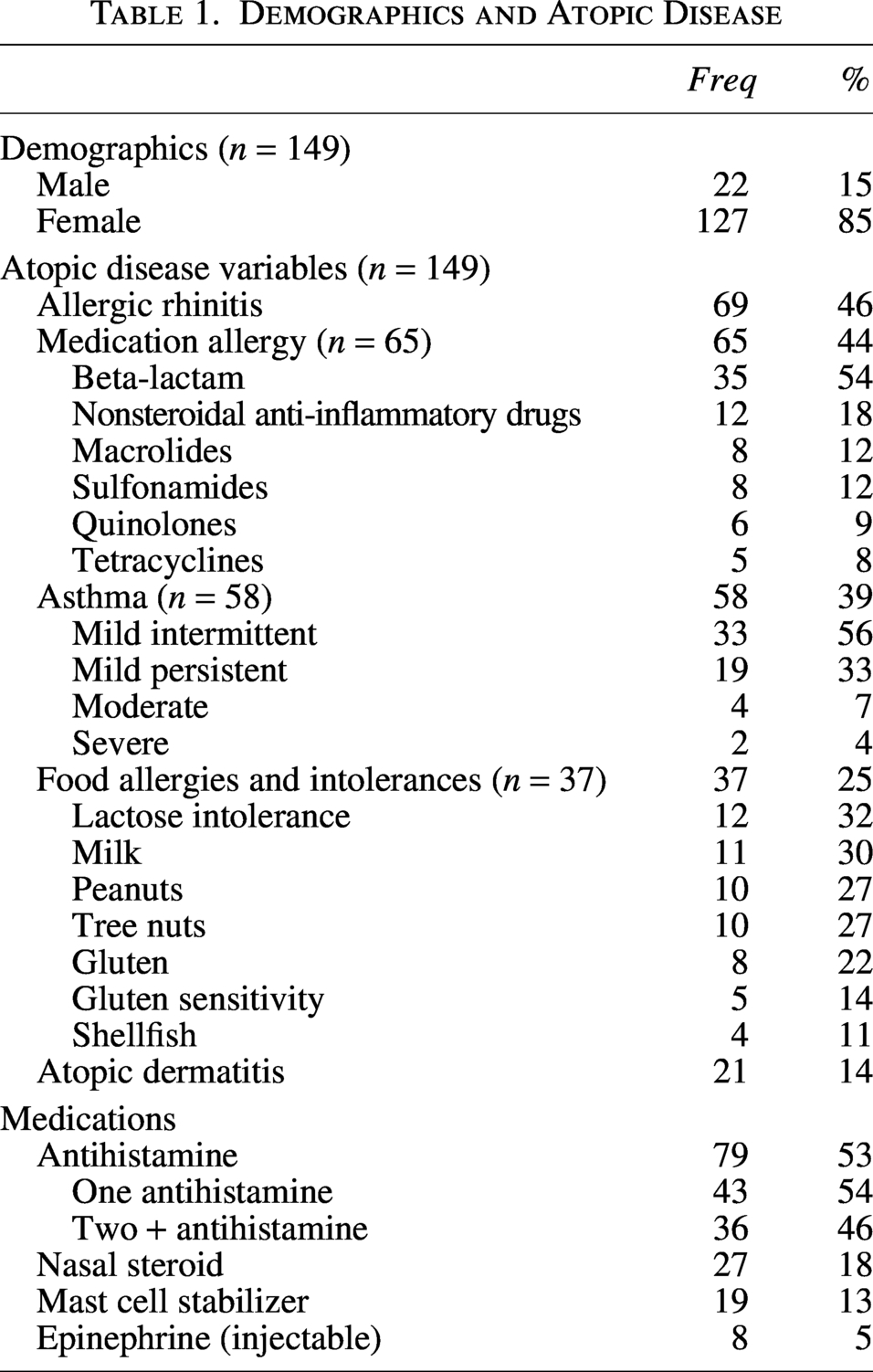
Of 232 patients, 149 met study inclusion criteria and had an average age of 15.5 years (SD: 3.1; range 8–22 years). Most patients identified as female (85%) and Caucasian (89%). Briefly, 7 patients identified as multiracial (5%) and Hispanic (5%), and 1 identified as Black (1%). Almost half (46%) of the pediatric patients with hEDS had allergic rhinitis, while 39% were diagnosed with asthma. Of those with asthma, mild intermittent asthma was the most common severity (56%), followed by mild persistent asthma (33%), moderate persistent asthma (7%), and severe (4%; Table 1). Food allergies were present in 25% of patients, with milk allergy (30%) being the most diagnosed, followed by peanut and tree nut allergy (27% each). Lactose intolerance was also seen in 32% of patients (Table 1 and Supplementary Table S1). Atopic dermatitis was present in 14% of patients, while almost half the cohort (44%) had a medication allergy. Of those with medication allergy diagnoses, most were due to beta-lactams (54%), followed by nonsteroidal anti-inflammatory drugs (18%), macrolides (12%), and sulfonamides (12%; Table 1 and Supplementary Table S1). Over half (53%) the patients were on antihistamine therapy, with 46% on 2 or more antihistamines, while nasal steroids were used in 18%, mast cell stabilizers in 13%, and 5% with injectable epinephrine prescribed (Table 1). Of the 149 patients with hEDS in this study 2 patients (1%) had a previous diagnosis of mast cell activation syndrome (MCAS).
Demographics and Atopic Disease
There was a significant, moderate association between pediatric patients with hEDS and concomitant diagnoses of allergic rhinitis (χ2 [1, N = 249] = 19.5, P < 0.001, Φ = 0.28), asthma (χ2 [1, N = 249] = 28.0, P < 0.001, Φ = 0.34), and medication allergies (χ2 [1, N = 249] = 32.1, P < 0.001, Φ = 0.36). There was a significant, small association between pediatric patients with hEDS and diagnosis of food allergies (χ2 [1, N = 249] = 10.4, P = 0.001, Φ = 0.02), while there was no significant relationship between patients and atopic dermatitis (χ2 [1, N = 249] = 10.4, P = 0.47). Of the atopic conditions identified in this cohort, all prevalences were higher (with a large effect size [r = 0.79]) compared to the general US pediatric population19,20 (U = 25, Z = 2.65, P = 0.008; Fig. 1).
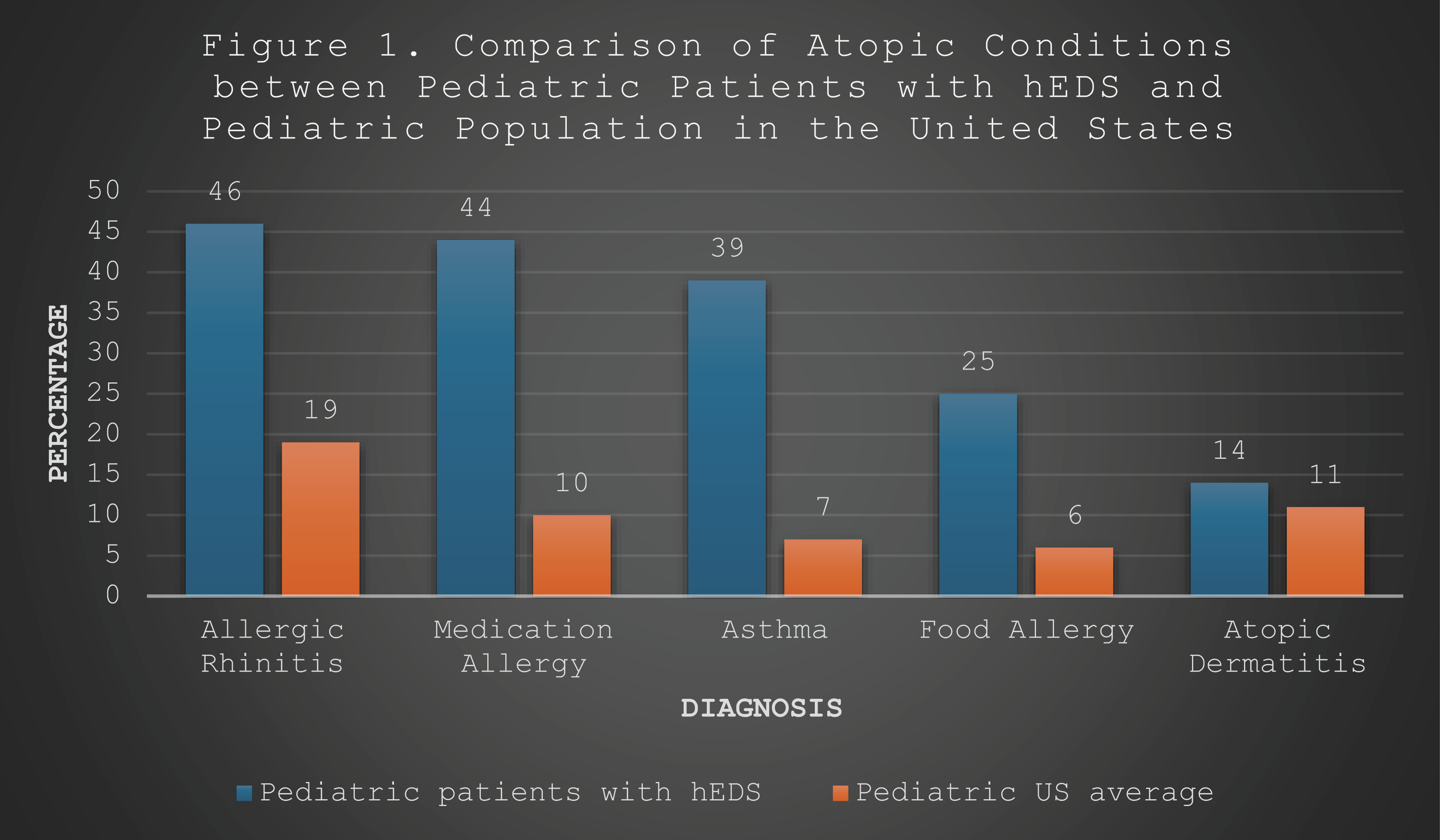
Comparison of atopic conditions between pediatric patients with hEDS and the pediatric population in the United States. hEDS, hypermobile Ehlers–Danlos syndromes.
Discussion
The objective of this study was to determine the prevalence of atopic conditions in pediatric patients with hEDS and determine how it compares with the general pediatric population in the United States. This study looked at documented atopic conditions and allergies (allergic rhinitis, asthma, atopic dermatitis, and food and medication allergies) in pediatric patients with hEDS and found there is a large prevalence of all atopic conditions and allergies evaluated, and all are more prevalent in the pediatric patients with hEDS compared to the general pediatric population in the United States.
Allergic rhinitis was the most prevalent atopic condition identified in this cohort of pediatric patients with hEDS and is significantly more prevalent in this population compared to the general pediatric population in the United States (13%–19%).15,17 A previous report of children with hEDS shows a significantly higher risk for children with EDS to develop allergic rhinitis compared to children without EDS. 21 While the cause of the high risk and prevalence are unclear, there is consideration that the symptoms may be due to MCAS, which may manifest clinically as allergic inflammation and has been linked to EDS. 22
Asthma was also found to be more prevalent in pediatric patients with hEDS compared to reported data for children in the United States, and most of the patients in this study had mild intermittent asthma, with only a few having severe asthma, which is similar to what is seen in the national US population. 16 The patients in this cohort were evaluated and diagnosed by pediatric pulmonology specialists, but a previous case series of 5 pediatric patients diagnosed with EDS (2 with classical EDS and 3 with hEDS) and asthma showed that only 2 (both with hEDS) of the 5 patients had asthma while the others had alternative explanations for their respiratory symptoms, which included vocal cord dysfunction. 23 Due to the number of respiratory symptoms and potential for misdiagnosis, providers need to carefully pursue respiratory symptoms in children with EDS to ensure accurate diagnosis. Further investigation is needed to evaluate the prevalence of asthma in children with EDS to determine accurate prevalence.
Food and medication allergies were also more prevalent in this cohort of pediatric patients with hEDS compared to pediatric-aged patients in the United States. 15 The most common food allergies reported in this study are dairy, peanuts, and tree nuts, which is consistent with reports in the general pediatric population. 18 Additionally, the most common medication allergy reported in this population was antibiotics, which is also similar to what has been previously reported in children. 24 The food and medication allergy types are similar between those with and without hEDS, but why those with hEDS have a higher prevalence is unclear. There have been reports that suggest people with EDS have more adverse effects or worse symptoms with different classes of medication; 25 however, more work is needed to evaluate medication efficacy and intolerance in patients with EDS.
Atopic dermatitis in children with hEDS was seen at a similar prevalence to US national averages (14% and 11%, respectively). Patients with EDS do have more skin fragility issues such as easy bruising, atrophic scarring, striae, and poor wound healing, but atopic dermatitis does not seem to be more prevalent, and there was no association seen between patients with hEDS and atopic dermatitis.
Over half (53%) of the patients in this study were on antihistamine medications, with almost half (46%) of those on multiple antihistamines. While not surprising given the large number of patients in this study with allergic rhinitis and asthma, it may indicate that the atopic disease is more severe or patients are less responsive to the medication and require additional therapies. Unfortunately, our study was not designed to evaluate this question, but future studies should consider these questions.
Study limitations
This study has several limitations that may limit generalizability, as it was conducted at 1 site that has a multidisciplinary EDS clinic, which may bias the sample toward a more impaired or impacted group of individuals with EDS that are seeking multidisciplinary care; however, most reported cohorts are predominantly Caucasian females, which is similar to the demographics for this study. Additionally, the results of this study may not be generalizable, as the prevalence of atopic disease varies between ethnicities and genders. 19 This study would benefit from the participation of other genders and more diverse ethnicities, which may be challenging due to the predominate Caucasian demographics of cohorts with EDS. The atopic conditions and medications were extracted from the patient’s medical records, and so condition acuity and chronicity, state of treatment, and previous treatment are not all clearly defined. While information was confirmed through subspecialty evaluation documentation, details were not obtained about specific tests that were performed that led to each diagnosis. Additionally, this study took place in the Midwest United States, which has well-documented seasonal changes and increased allergens that may affect people differently, and future work should include a larger cohort across a more diverse geographical area.
Conclusions
Pediatric patients with hEDS have a higher prevalence of allergic rhinitis, medication and food allergies, and asthma but not atopic dermatitis when compared to the pediatric population of the United States. The medication and food allergies are mostly the same as the general population, with antibiotics and dairy as the most common medication and food allergies, but those with hEDS have higher overall prevalence compared to the pediatric population of the United States. Children and adolescents with hEDS have many unique comorbid conditions, and atopic and allergic conditions are prevalent. Medical care for pediatric patients with hEDS should include evaluation for atopic and allergic conditions with a low threshold to refer to allergy and pulmonology specialists. Future work is needed to determine the degree and impact of these conditions on overall health and how they may be related to other comorbidities seen in patients with EDS.
Authors’ Contributions
J.T.J.: Conceptualization, formal analysis, investigation, methodology, project administration, supervision, writing—original draft, and writing—review and editing. K.G.C.: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, and writing—review and editing. A.L.: Data curation, investigation, resources, software, and writing—review and editing.
Data Availability Statement
Data will be made available upon reasonable written request.
Supplemental Material
sj-docx-1-pai-10.1177_2151321X261467509 — Supplemental material for Prevalence of Atopic Disease in Pediatric Patients with Hypermobile Ehlers–Danlos Syndrome
Supplemental material, sj-docx-1-pai-10.1177_2151321X261467509 for Prevalence of Atopic Disease in Pediatric Patients with Hypermobile Ehlers–Danlos Syndrome by Jordan T. Jones, Kathleen G. Click, and Ashley Lytch
Footnotes
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.