
Abstract
Background
Hemiarthroplasty remains the gold standard for hip fracture care in displaced intracapsular fractures. There is now substantial evidence that uncemented femoral stems are associated with higher risk of perioperative fractures. Cemented composite beam (CCB) stems offer some of the lowest overall rates of perioperative fracture risk, but are not widely used in the Irish system, and concern regarding the use of new implants and associated learning curves can act as a barrier to change.
Objectives
We aim to assess our units experience transitioning to a cemented composite beam (CCB) and the associated learning curve and technical pitfalls.
Design
Retrospective, single centre, single blind review identified the first 140 cases of CCB stems.
Methods
Post-operative radiographs on all cases were assessed for perioperative fracture and stems were classed as being varus or valgus if the stem alignment was >3 degrees from the anatomical axis. A cemented taper slip (CTS) stem, which was in use for over 10 years in the unit, provided a control group.
Results
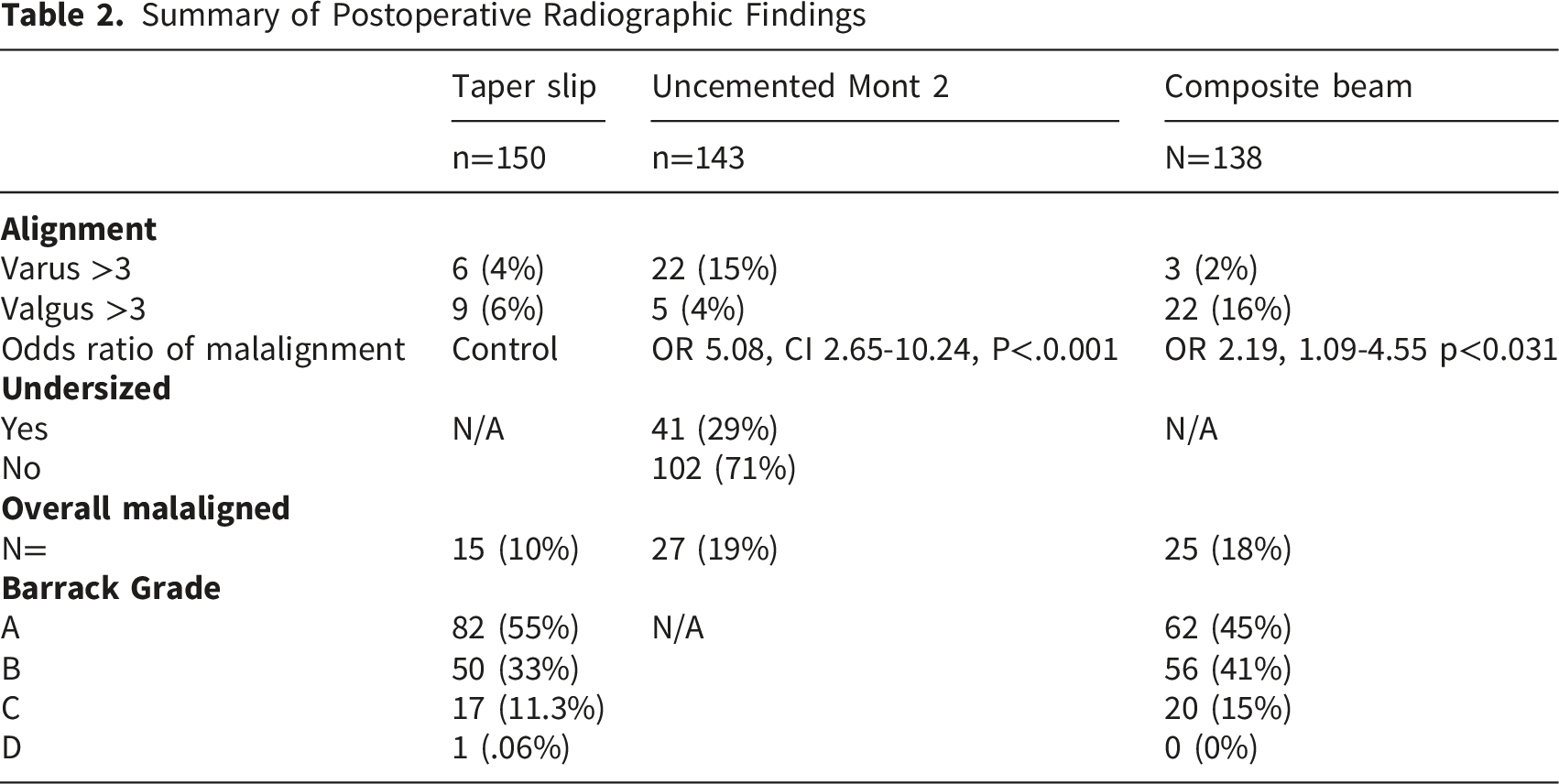
Following introduction, higher odds of malalignment were experienced with the CCB stem (OR 2.19, 1.09-4.55 p<0.031), relative to CTS. However, compared to overall rate of malalignment in the CTS group (9.3%), the learning curve for the CCB stem was short, with rates of malalignment returning to in line with our control CTS cohort within 46 cases (Cases 1-46 32% malaligned, cases 47-92 10.86% malaligned, cases 93-138 4.34% malaligned). There was no increased risk of periprosthetic fracture demonstrated with introduction of the new stem.
Conclusions
We have shown a relatively short learning curve associated with transitioning to a CCB stem for fragility fracture hemiarthroplasty. We highlight some of the early technical issues experienced and corrected.
Introduction
As global populations age, rates of proximal femoral fractures are projected to rise over the coming decadess 1 While advances in surgical and medical management have improved overall care, proximal femoral fractures continue to cause mortality and morbidity in elderly populations 2 resulting in a reduction in quality of life 3 and considerable individual and societal socioeconomic burdenn 4 Approximately half of these fractures are intracapsular, with arthroplasty based procedures (hemi or total) representing the accepted gold standard of managementt 5
Surgeons may choose to use uncemented femoral stems for hemiarthroplasty in order to reduce both operative time and bone cement implantation syndrome. Furthermore, surgeon familiarity with uncemented stems from elective total hip arthroplasty procedures may play a role in prosthesis choice. However, recent high quality evidence including systematic reviews,6,7 large scale database studies 8 as well as randomised controlled trails comparing cemented to uncemented hemiarthroplasty 9 have shown no increase in mortality with cemented femoral stems. Further, improved quality of life and reduced rates of periprosthetic fractures have been reported in cemented stems. 10 This has resulted in a move back towards cemented stems in this cohort of patients in a number of jurisdictions.11,12 This evidence is also reflected in the most recent iterations of consensus guidance documents from both the National Institute for Health and Care Excellence (NICE) 13 and the American Academy of Orthopaedic 14 Surgeons (AAOS). 15 Despite this, rates of uncemented hemiarthroplasty remain high globally. In the most recent Irish hip fracture registry 23% of hemiarthroplasty patients received uncemented components 16 and the use of uncemented implants in the US and Canada remains widespread. 8
As evidence continues to mount, we believe surgeons should move towards cemented stems for hip hemiarthroplasty. Concurrently, evidence on cemented stem design would suggest that composite beam stems are associated with lower risk of peri-prosthetic fracture when compared with taper slip designs.15,17,18 In the fragility fracture cohort this becomes increasingly significant. 19 For this reason, surgeons should consider composite beam stems if switching to a cemented stem for hemiarthroplasty, while those using a taper slip cemented stem may consider switching to a composite beam stem for this fragility cohort. One potential barrier to change is the recognition of learning curves associated with adoption of new stem designs. 20 Over the last number of years, our unit transitioned from a cemented taper slip (CTS) design to an uncemented Mont B2 (UM2) type stem in 2020/2021 and more recently back to a cemented composite beam (CCB) stem design. The aims of this study were to report on the learning curve and fracture rates and explore technical pitfalls associated with transitioning between stem design for hip hemiarthroplasty.
Methods
This was a single blinded, retrospective single centre comparative study. The study was deemed exempt from ethical approval due to its retrospective, radiographical and non-interventional nature. The study was carried out in a tertiary referral university hospital comprising eleven orthopaedic surgeons on the subspecialist register, five of which are fellowship trained in lower limb arthroplasty. For approximately 12 years a cemented taper slip stem design (Trilliance, B. Braun, Tuttlingen, Germany) was routinely used for hemiarthroplasty. From January 2020 to January 2021, the unit went through a trial period of using an uncemented, Mont 2, hydroxyapatite coated stem (Corail, DePuy, Warsaw, Indiana, USA) which was routinely in use for elective total hip arthroplasty within the department. This was also in response to anaesthetic concerns regarding bone cement implantation syndrome, and a desire for reduced operative times in the context of the ongoing COVID 19 pandemic. In response to emerging evidence with regards to fracture risk, a return to cemented stems took place in 2022. In 2024 the whole unit converted to using a composite beam cemented design (Excia, B. Braun, Tuttlingen, Germany) in place of the previous taper slip design.
We carried out a retrospective review of theatre logbooks from the above periods and identified the first 140 cases of both composite beam and Mont 2 uncemented stems implanted between 1st December 2024 and 1st December 2025. All hemiarthroplasty cases carried out via a lateral approach in this period were included. Total arthroplasty cases and those performed via a direct anterior approach were excluded. The cutoff of 140 was set as this was the total number of uncemented cases available following exclusion criteria. In addition, 140 cases of the cemented taper slip stem which had been in use for 12 years were selected to be used as a control cohort and establish a baseline level of stem malalignment.
Baseline demographics including age and gender were recorded from theatre logbooks. Pre and post-operative radiographs were accessed via our local imaging system. Pre-operative radiographs were used to assess Dorr classification, which was based off the non-fractured hip. 21 Anteroposterior (AP) radiographs are taken on all patients in recovery using a standardised protocol. Post-operative radiographs on all cases were assessed for alignment of the stem using the system previously described by Khalily and Lester, 22 ascertained using the post-operative alignment tool on TraumaCad® (Brainlab AG, Munich, Germany) software. Stems were classed as being varus or valgus if the stem alignment was >3 degrees from the anatomical axis of the femoral shaft, in keeping with prior research on stem alignment.22,23 Radiographs were also assessed for evidence of intra operative fracture (ie. cable or plate fixation). Barrack grading of cement fixation was carried out on cemented stems. 24 Uncemented stems were classified as adequately or under sized using the method described and validated by McConnell et al. 25
Ten cases from each cohort were randomly selected and repeat radiographic assessment was carried out by one of the senior authors in order to quantify inter rater variability on stem alignment and sizing measurements and Dorr classification.
Categorical variables were described by counts and proportions, while continuous variables were described by medians and ranges. Logistic regression models were used to compare the odds of mal-alignment and post-operative fracture, respectively, in the each of the UM2 and CCB cohorts to those in the CTS cohort, and the reported learning curve was projected based on this analysis. Model estimated odds ratios are reported with 95% confidence intervals based on profile likelihoods and two-sided p-values based on Wald tests. All analyses were conducted using the R statistical programming language (V 4.2.2;). 26
Baseline demographics, Dorr Classification and Fellowship Status of Supervising Surgeon

Results
Summary of Postoperative Radiographic Findings
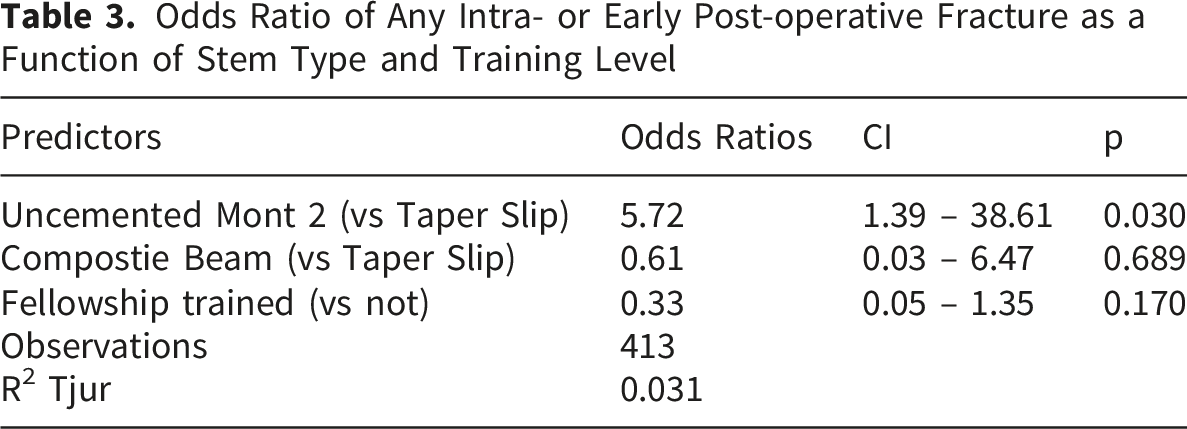
Odds Ratio of Any Intra- or Early Post-operative Fracture as a Function of Stem Type and Training Level
Inter-rater variability was low overall for alignment (varus/valgus), with 96.7% agreement for stem alignment and 90% agreement for UM2 sizing. Agreement for Dorr classification was 76.7%.
Discussion
The evidence-practice gap in orthopaedic surgery has been well documented.27-29 As the rate at which orthopaedic research is produced continues to rise, 30 surgeons must ensure that evidence based medicine is being appropriately implemented within units- and in a timely manner. It is well documented that changes to practice can be slow even when high levels of evidence such as randomised controlled trials exist, and the reasons for this are multi factorial. 31 While surgeon and elective practice preferences can play a role in femoral stem selection, this should not be the dominant factor in hip fracture care as evidence continues to grow against the use of uncemented prostheses in this cohort.6,9,10 It is the author’s belief that in light of this evidence, more units should endeavour to switch towards cemented stems, with our preference being composite beam design cemented stems based on the current evidence.15,17
Learning curves are associated with any alteration in operative technique, and as such may act as one such barrier to change.32,33 Particularly when prolonged operative times may be associated with increased rates of complications. 34 However, while it is responsible for orthopaedic surgeons to be cognisant of learning curves and their impact on outcomes, it would be remiss to allow them to prevent implementation of changes in response to evidence. In this study, we share our units experience with changing stems on two occasions, initially from a cemented taper slip design to an uncemented Mont 2 type stem and finally to a cemented composite beam. The results of our study show a relatively short learning curve associated with introduction of a composite beam design cemented stem. However we noted an overall high and sustained rate of complications and malalignment of uncemented stems. Of note, this was independent of whether or not the surgeon was arthroplasty fellowship trained or not, despite the fact that all five arthroplasty surgeons in the unit routinely use both cemented and uncemented stems in their elective arthroplasty practice. This reenforces the point that stem choices in elective practice should not influence fracture care. Our malalignment rates for the CTS stem and CCB stem beyond the initial learning curve are in keeping with published literature.23,34 Of note, our rates of malalignment of the UM2 stem is also reflected within available literature, with varus malalignment also recorded in high volume centres.35,36
We also highlight the technical considerations associated with each stem. The main issues encountered with the uncemented stems were undersizing and resultant varus or valgus malalignment of the stem, as well as an increased risk of periprosthetic fracture intraoperatively. Undersizing may reflect a less aggressive approach to femoral broaching as surgeons try to avoid fractures. In the composite beam stems, we observed a tendency for implantation in significant valgus angulation in the first 46 cases, after which this rate returned to baseline. Reasons for this are hypothesised to be surgeon’s familiarity with a straight taper slip stem, which necessitates a more lateral broach entry point when compared to the curved, force closed composite beam design.
Additionally, our study highlights the importance of regular local audit of practice to allow for quality control and early identification of areas for concern. Clinical audit represents a cornerstone of governance, and as such is a core tenet of guidelines for good clinical practice. 37 Our unit consists of 11 surgeons, five of which are arthroplasty fellowship trained, with the remaining six surgeons subspecialised in other areas within orthopaedics. This layout reflects the majority of publicly funded units in Ireland and the United Kingdom. An audit of all trauma cases is carried out on a weekly basis. We believe this audit contributed to the early identification of technical implantation errors with the new stem designs, and allowed for collective rather than individual learning and adaptation of new technology, thus shortening the learning curve for individual surgeons. The benefit of regular morbidity and mortality reviews are also well documented. 38 In our unit this also allowed for prompt identification of increased fracture rates in the uncemented cohort and prompted cessation of the routine use of this stem pending departmental review.
Finally, while our study was not pre-powered to assess for fracture rates in uncemented hemiarthroplasty, our results are in line with the current available evidence on the topic, 9 showing a higher rate of intraoperative periprosthetic fracture in this cohort. Unlike the total hip arthroplasty cohorts, the frailty inherent to the fracture cohort is a cause for concern when using uncemented stems. 39 Thus, in our unit, the rate of intraoperative fracture in the uncemented cohort resulted in cessation of the use of this stem for routine hemiarthroplasty cases. It is also important to note that large, registry based studies will often only detect periprosthetic fractures in cases where components have been revised. 40 As such, while registry based data aims to give a more generalisable overview of practice when compared to RCTs often carried out in specialist centres, they may under-report rates of fracture due to constraints on data collection methodology. 41
Limitations
There are a number of limitations to this study. This is single centre, non blinded retrospective study and as such is inherently subject to bias.
Secondly in our unit, hemiarthroplasty patients do not have routine post-operative clinical or radiographic follow up and as such only post operative supine radiographs taken in recovery are available. While these are taken according to a standardised protocol, there is higher variation in the quality of the radiographs compared to departmental films.
Another limitation of this study is the small overall numbers in each cohort, however we believe that these numbers are adequate to describe the learning curve as well as key technical considerations when introducing a new femoral stem to a unit.
Our unit has extensive previous experience with cementation and cemented taper slip stems. Some of this experience including later generation cementing techniques is transferrable to composite beam implantation. The authors acknowledge that the learning curve may differ in units where only uncemented stems have been in use. However we believe that our sharing of our common technical pitfalls in the adoption of this stem will still serve to help such units in early recognition and correction of these errors.
In this study a risk of bias exists in the inability to blind investigators to the stem used during radiographic analysis. We aimed to limit this by using a post operative stem alignment software rather than simple angle measurements.
Conclusions
There is growing evidence against the use of uncemented stems in hip fracture care. As units make the switch to cemented stems, the current evidence base supports the use of a composite beam design. We have shown a relatively short learning curve associated with transitioning to this stem design, and highlight some of the early technical issues experienced and corrected.
Footnotes
Ethical Considerations
The study was deemed exempt from ethical approval by local board due to its retrospective, radiographical and non-interventional nature.
Author Contributions
Orla Hennessy, Kieran Field and Sean Flynn contributed to conceptualisation as well as data collection, synthesis and analysis, writing of the first and second drafts and revision. Darren Dahly contributed data analysis including statistical modelling and 1st draft of manuscript. F Rowan, E Pomeroy, T Murphy and M Cleary provided conceptualisation, project supervision, editing and revision of the first draft and revised draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Upon request.