
Abstract
Objectives
To compare the Trauma-Specific Frailty Index (TSFI) with an institutional Perioperative Geriatric Score (PGS) for predicting postoperative level of care, discharge disposition, and length of stay in older adults undergoing operative fixation of lower-extremity fractures.
Methods
Design: Retrospective cohort study. Setting: Two hospitals within a single academic health system: an urban level I and a suburban level III trauma center. Patient Selection Criteria: Patients aged ≥65 years who underwent operative fixation of lower-extremity fractures between January 1 and June 30, 2025; nonoperative fractures and encounters lacking primary outcome data were excluded. Frailty was measured with the TSFI (0–1 deficit-accumulation index). Perioperative risk was measured with an institutional PGS combining vasopressor use, blood loss, cardiac comorbidity, case duration, and delay to surgery. Outcome Measures and Comparisons: Primary outcomes were postoperative level of care, discharge disposition, and hospital length of stay; 90-day readmission and mortality were secondary. Multivariable regression adjusted for age, sex, body mass index, and fracture type.
Results
Among 248 patients (median age, 78 years; 64.1% female), higher TSFI values were associated with stepdown admission (odds ratio [OR] 2.43; 95% confidence interval [CI], 1.13–5.21), intensive care unit admission (OR 2.79; 95% CI, 1.16–6.70), discharge to a skilled nursing facility (OR 1.96; 95% CI, 1.11–3.47), and longer length of stay (OR 1.61; 95% CI, 1.19–2.17). The PGS showed weaker associations, reaching significance only for intensive care unit admission (OR 1.16; 95% CI, 1.07–1.26). Ninety-day readmission and mortality were too infrequent for reliable estimates.
Conclusions
The TSFI outperformed an institutional perioperative geriatric triage score in predicting postoperative care escalation and discharge disposition in lower-extremity fracture patients. Incorporation of frailty assessment into orthopaedic trauma workflows may improve risk stratification, counseling, and resource planning.
Introduction
Sustained losses in mobility and activities of daily living are common early after surgery and often persist, reflected by marked declines in health-related quality of life across physical, emotional, and social domains.1,2 Mortality remains elevated for months to years after fracture, and many patients do not return to preinjury function, with a sizable proportion requiring new institutional care.1-3 Against this backdrop, operatively treated lower-extremity fractures represent sentinel events with enduring effects on independence and survival.1,4,5
These injuries are also major drivers of resource utilization. 6 Particularly among older adults, who comprise a growing share of orthopaedic trauma, resource needs are amplified. Advanced age and comorbidity are associated with higher perioperative complication rates, longer hospitalization, and greater short-term mortality.7,8 Length of stay correlates strongly with total inpatient costs, and constraints in postacute placement further extend bed-days and downstream expenditures. 9
Components and Calculation of the Trauma-specific Frailty Index
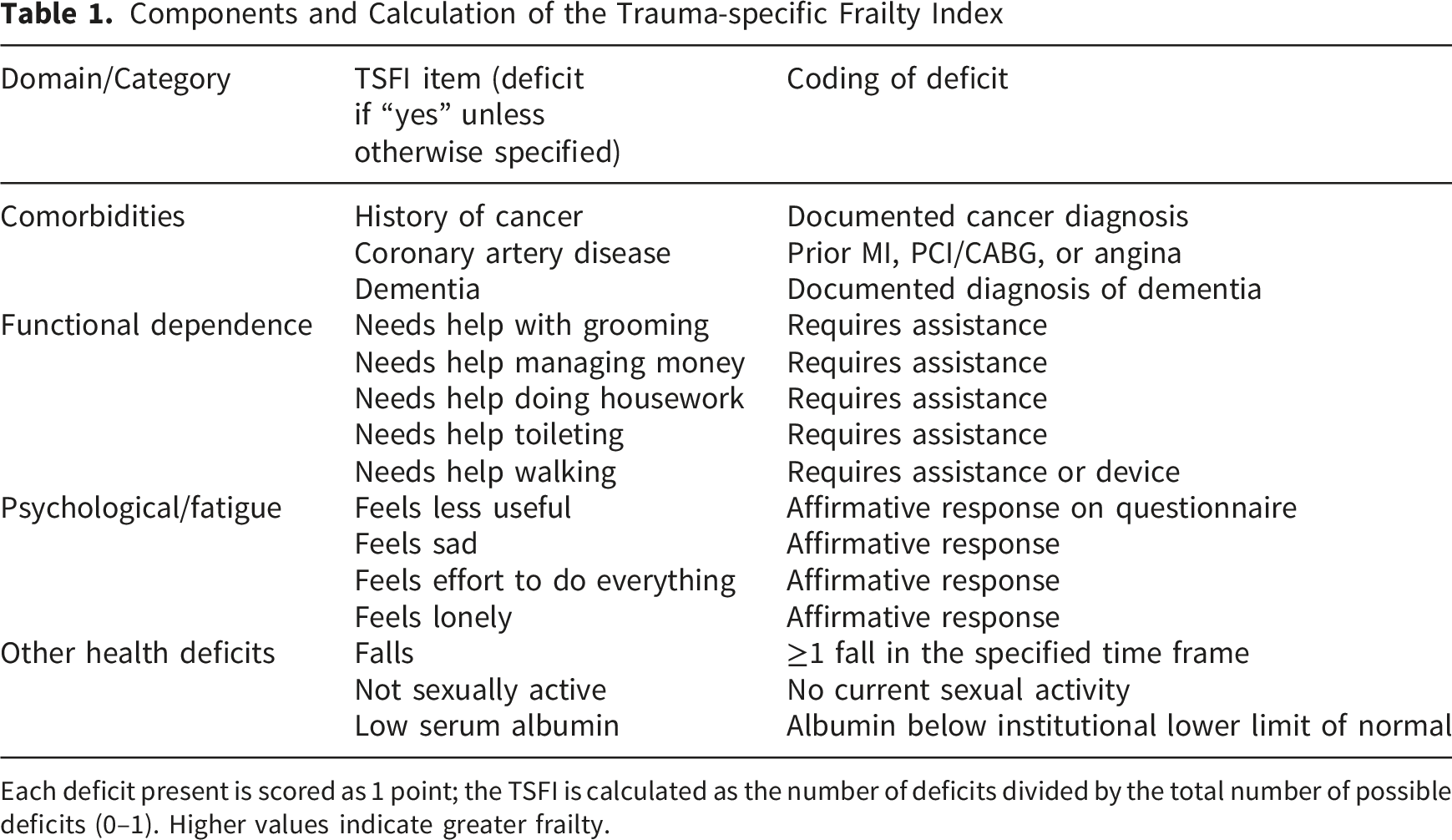
Each deficit present is scored as 1 point; the TSFI is calculated as the number of deficits divided by the total number of possible deficits (0–1). Higher values indicate greater frailty.
Components and Calculation of the Perioperative Geriatric Score
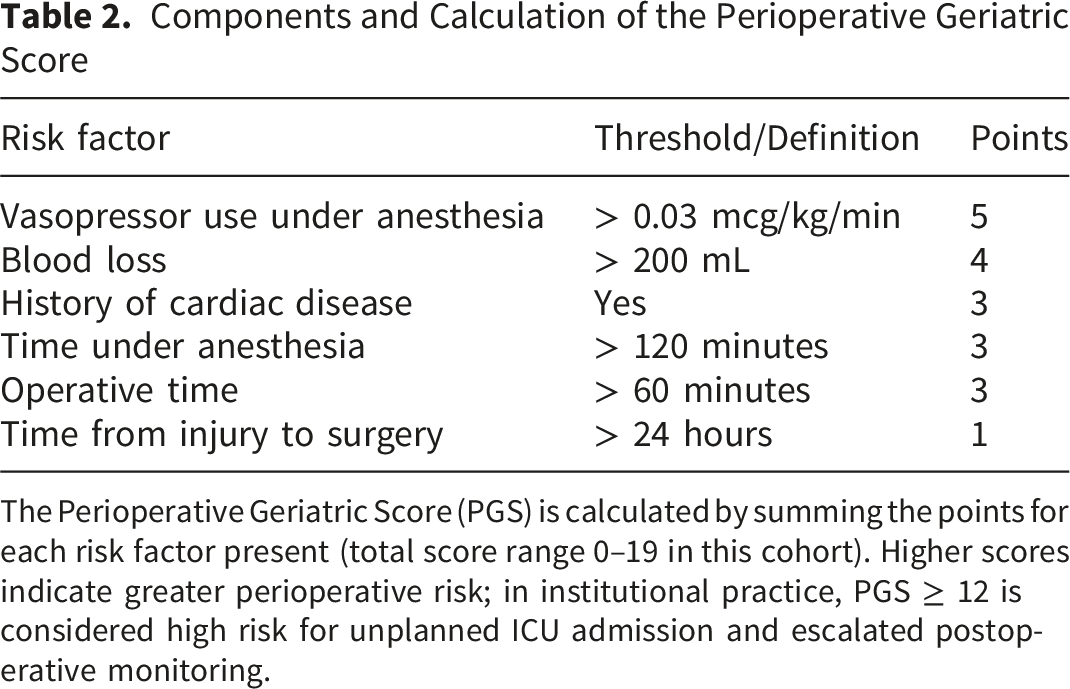
The Perioperative Geriatric Score (PGS) is calculated by summing the points for each risk factor present (total score range 0–19 in this cohort). Higher scores indicate greater perioperative risk; in institutional practice, PGS ≥ 12 is considered high risk for unplanned ICU admission and escalated postoperative monitoring.
Prior work on frailty in orthopaedic trauma often pools elective and urgent procedures, restricts inclusion to single fracture patterns, or employs heterogeneous risk tools, limiting direct comparison between frailty-based and traditional perioperative instruments. 14 Few studies have examined how a trauma-specific frailty index performs against an institutional perioperative triage score for key outcomes such as level of postoperative care, discharge disposition, and length of stay in geriatric lower-extremity fracture patients. To address this gap, we conducted a head-to-head evaluation of the TSFI and the PGS within a contemporary cohort, assessing each tool’s correlation, discrimination, and incremental prognostic value for prespecified clinical and operational outcomes. It is hypothesized that a preoperative frailty index derived from social and functional factors would predict hospital length of stay and discharge disposition in this population.
Methods
Study Design
This retrospective cohort study of consecutively treated older adults undergoing operative fixation of lower-extremity fractures was approved under an orthopaedic retrospective umbrella protocol with waiver of informed consent. Data resided on secure institutional servers and were de-identified for analysis. The sample size was determined by the number of eligible patients treated during the study period; no a priori sample size or power calculation was performed. The study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Setting and Data Sources
Institutional Characteristics and Postoperative Care Capacity
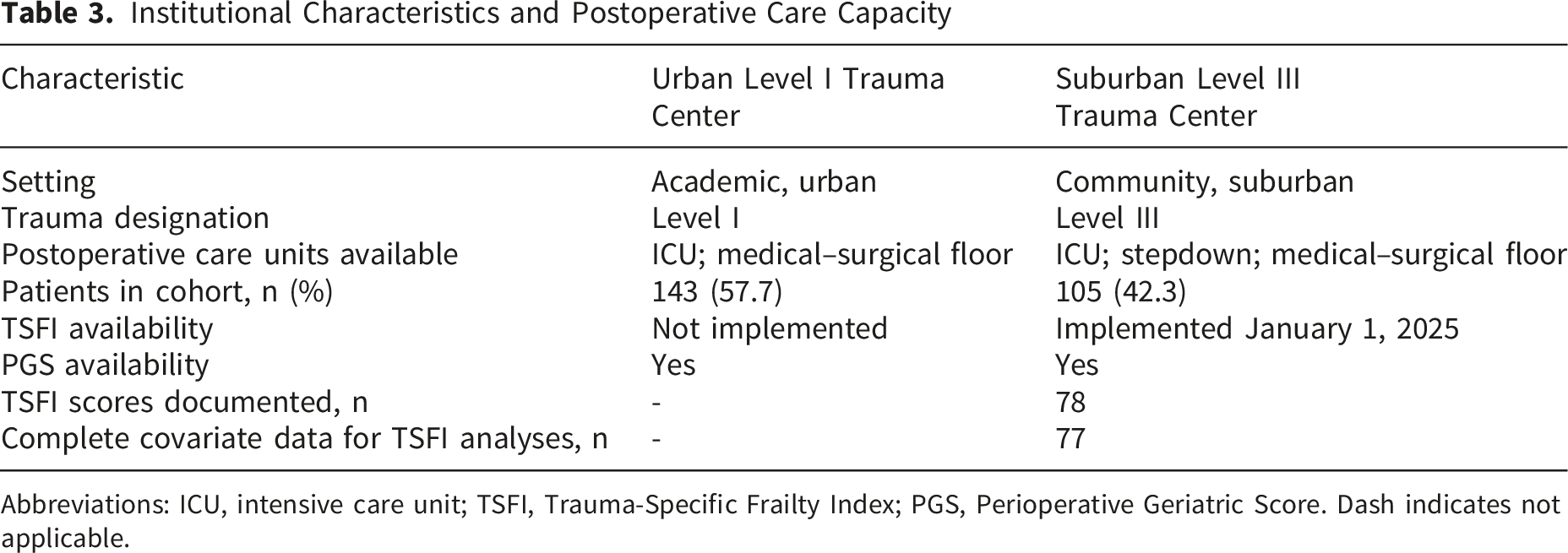
Abbreviations: ICU, intensive care unit; TSFI, Trauma-Specific Frailty Index; PGS, Perioperative Geriatric Score. Dash indicates not applicable.
Participants
Inclusion: patients ≥65 years undergoing operative treatment of an incident lower-extremity fracture (femoral neck/intertrochanteric/subtrochanteric, femoral shaft, distal femur, tibial plateau, tibial shaft, or ankle). Fractures were classified according to the Orthopaedic Trauma Association/AO 2018 Fracture and Dislocation Classification Compendium, corresponding to proximal femur (31; femoral neck/intertrochanteric/subtrochanteric), femoral shaft (32), distal femur (33), proximal tibia (41; tibial plateau), tibial shaft (42), and ankle (44) injuries. 15 Exclusion criteria were age <65 years, nonoperative management of the index fracture, fractures outside the femur–tibia–ankle region, and encounters lacking all primary outcome data. For patients undergoing multiple procedures during a single admission, the first fixation was designated the index procedure.
Demographic Variables
Preoperative variables included age, sex, height, weight, body mass index (BMI), primary diagnosis or fracture type, overall comorbidity profile, and American Society of Anesthesiologists (ASA) physical status classification. Comorbidities were abstracted from chart review and encompassed cardiovascular, metabolic, renal, pulmonary, musculoskeletal, psychiatric, and oncologic conditions commonly encountered in older adults.
Risk Instruments
The institutional perioperative geriatric triage score (PGS) was calculated as a composite measure derived from predefined perioperative risk factors: vasopressor infusion exceeding 0.03 μg/kg/min, estimated blood loss greater than 200 mL, documented cardiac disease, anesthesia duration longer than 120 minutes, operative time greater than 60 minutes, and time from arrival to surgery exceeding 24 hours. Each variable was scored dichotomously, and the total score was generated per the institutional algorithm; in secondary analyses, scores of 12 or higher were classified as high risk.
Frailty was quantified using the TSFI, a deficit-accumulation index calculated as the proportion of predefined frailty characteristics present. These characteristics encompassed select comorbidities including cancer, coronary artery disease, and dementia, dependence in basic or instrumental activities of daily living, indicators of mood and exhaustion, history of falls, mobility limitations, reduced sexual activity, and nutritional markers including serum albumin. The TSFI yields values ranging from 0 to 1, with higher values indicating greater frailty. Consistent with prior literature and local practice, a TSFI value greater than 0.25 was considered high risk in secondary analyses. 16 The TSFI was available only at the hospital where it had been implemented.
Healthcare Utilization
Healthcare utilization outcomes included (1) postoperative level of care immediately after surgery (medical-surgical floor, stepdown, ICU), (2) hospital discharge disposition (home, skilled nursing facility, inpatient rehabilitation, hospice/other), (3) length of stay (LOS) in days, (4) 90-day readmission, and (5) 90-day mortality. Weight bearing as tolerated (WBAT) at discharge and time from admission to surgery were exploratory outcomes. For 90-day endpoints, analyses were restricted to patients with ≥90 days of follow-up or administratively censored at the data-freeze date.
Statistical Analysis
Continuous variables were assessed for normality using the Shapiro-Wilk test and summarized as medians with interquartile ranges or means with standard deviations, as appropriate. Categorical variables were reported as frequencies and percentages. Correlation between the TSFI and the institutional PGS was evaluated using Spearman rank correlation, and linear regression was performed to model their relationship with regression coefficients and R2 values reported.
Multivariable regression analyses evaluated associations between each risk instrument and postoperative outcomes. Multinomial logistic regression modeled postoperative level of care (medical-surgical floor, stepdown, or ICU) and discharge disposition (home, skilled nursing facility, inpatient rehabilitation, hospice/other). Binary logistic regression was used for 90-day readmission and 90-day mortality, using the same covariate structure. Robust linear regression modeled hospital length of stay to account for heteroskedasticity. All models adjusted for age, sex, BMI, and fracture type; the American Society of Anesthesiologists (ASA) classification was analyzed in parallel models as an additional predictor. Both risk instruments were evaluated as continuous measures in all analyses. Given the low frequency of 90-day mortality and readmission events and occasional model non-convergence, these 90-day analyses were considered exploratory and corresponding estimates were interpreted cautiously. All tests were two-tailed with significance defined as p < 0.05. All statistical analyses were conducted using Python (Version 3.10; Python Software Foundation, Wilmington, DE) with the stats models, SciPy, and pandas libraries.
Demographic Characteristics
Baseline Demographic and Clinical Characteristics of the Study Cohort
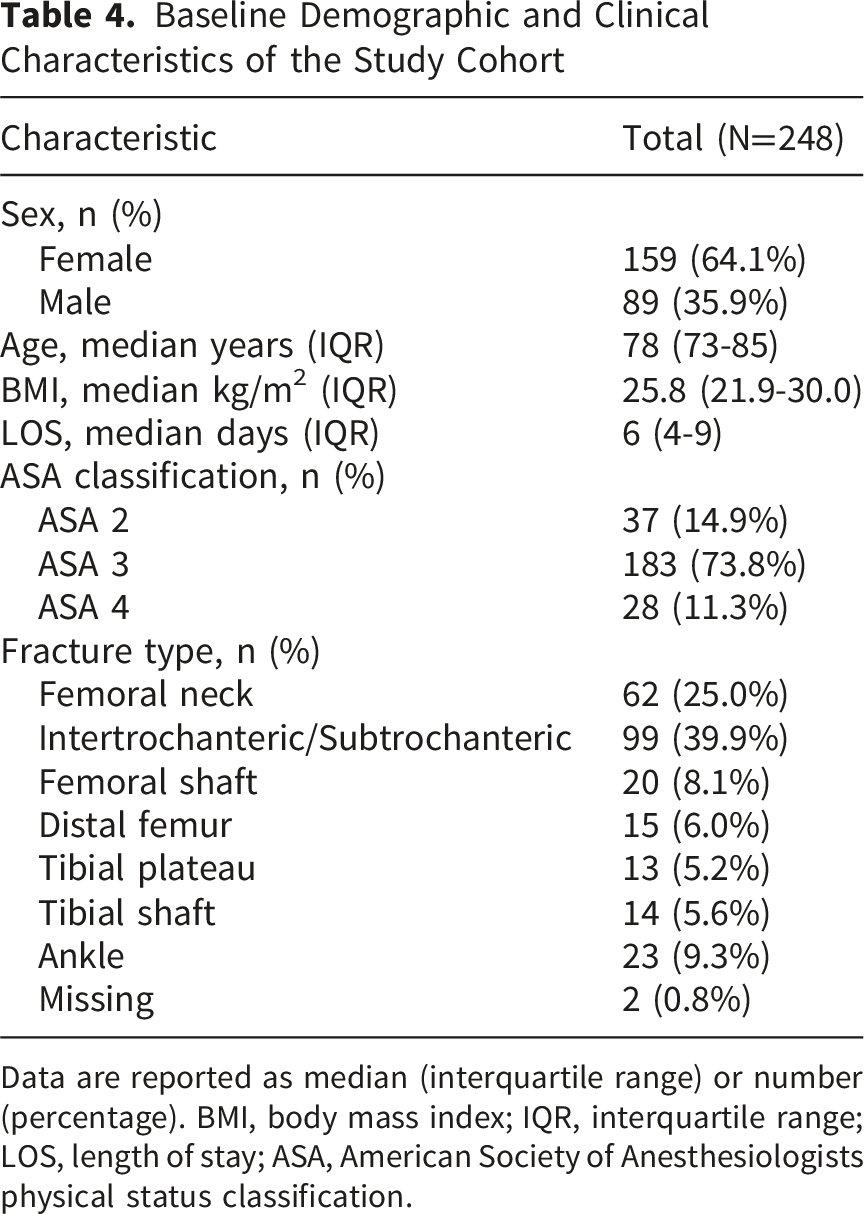
Data are reported as median (interquartile range) or number (percentage). BMI, body mass index; IQR, interquartile range; LOS, length of stay; ASA, American Society of Anesthesiologists physical status classification.
Stepdown Unit
The TSFI demonstrated a significant association with stepdown unit admission (Odds Ratio [OR] 2.43, 95% Confidence Interval [CI] 1.13–5.21; p = 0.023). In contrast, the perioperative geriatric score (PGS) was not significantly associated with stepdown utilization (OR 0.99, 95% CI 0.92–1.06; p = 0.786).
Intensive Care Unit (ICU)
Higher TSFI scores were significantly associated with ICU admission (OR 2.79, 95% CI 1.16–6.70; p = 0.022). The PGS also demonstrated a significant but more modest association with ICU admission (OR 1.16, 95% CI 1.07–1.26; p < 0.001).
Skilled Nursing Facility (SNF)
The TSFI was significantly predictive of SNF disposition (OR 1.96, 95% CI 1.11–3.47; p = 0.021). By comparison, the PGS demonstrated only a borderline and non-significant association (OR 1.03, 95% CI 0.96–1.11; p = 0.452).
Inpatient Rehabilitation (IPR)
The TSFI was not significantly associated with IPR admission (OR 0.69, 95% CI 0.22–2.19; p = 0.529). The PGS showed a modest but non-significant trend toward increased IPR utilization (OR 1.07, 95% CI 0.98–1.17; p = 0.148).
Length of Stay (LOS)
Both frailty indices were significantly associated with increased hospital length of stay. The TSFI was associated with longer LOS (OR 1.61, 95% CI 1.19–2.17; p = 0.002), and the PGS demonstrated a similar significant association (OR 1.18, 95% CI 1.07–1.30; p = 0.001).
Weight-Bearing Status and Time to Surgery
In secondary analyses restricted to patients with complete data, higher TSFI values were not significantly associated with weight-bearing as tolerated at discharge or with time from arrival to surgery greater than 24 hours. The perioperative geriatric score similarly did not demonstrate a clinically meaningful association with either outcome; although its relationship with delayed surgery reached statistical significance, this was expected because delay to surgery is a component of the score itself. These analyses were therefore considered exploratory, and no definitive conclusions were drawn for these secondary endpoints.
Ninety-Day Readmission and Mortality
Ninety-day adverse events were infrequent in this cohort, limiting the ability to generate stable regression estimates. In the readmission model, neither frailty instrument demonstrated a significant association with 90-day readmission, but confidence intervals were extremely wide, reflecting sparse event counts and limited statistical power. For 90-day mortality, the TSFI model showed evidence of quasi-separation and did not converge, precluding meaningful interpretation of effect estimates. The perioperative geriatric score similarly showed no significant association with mortality. Taken together, the low frequency of 90-day events and convergence instability suggest that these analyses should be considered exploratory only, and no definitive conclusions can be drawn regarding the predictive performance of either frailty measure for rare postoperative outcomes.
A Summary of all Model Estimates Is Presented in Table 5
Discussion
Multivariable Model for Stepdown Unit Admission (Multinomial Logistic Regression). Reference Category: Medical-Surgical Floor. Odds Ratios for the TSFI are Reported per 0.1 unit Increment. All Tests Two-Sided; p < 0.05 Considered Significant. Events per Variable = 11.2 (56 Stepdown Events, 5 Predictors). n = 77. Stepdown Contrast From the Multinomial Level-Of-Care Model
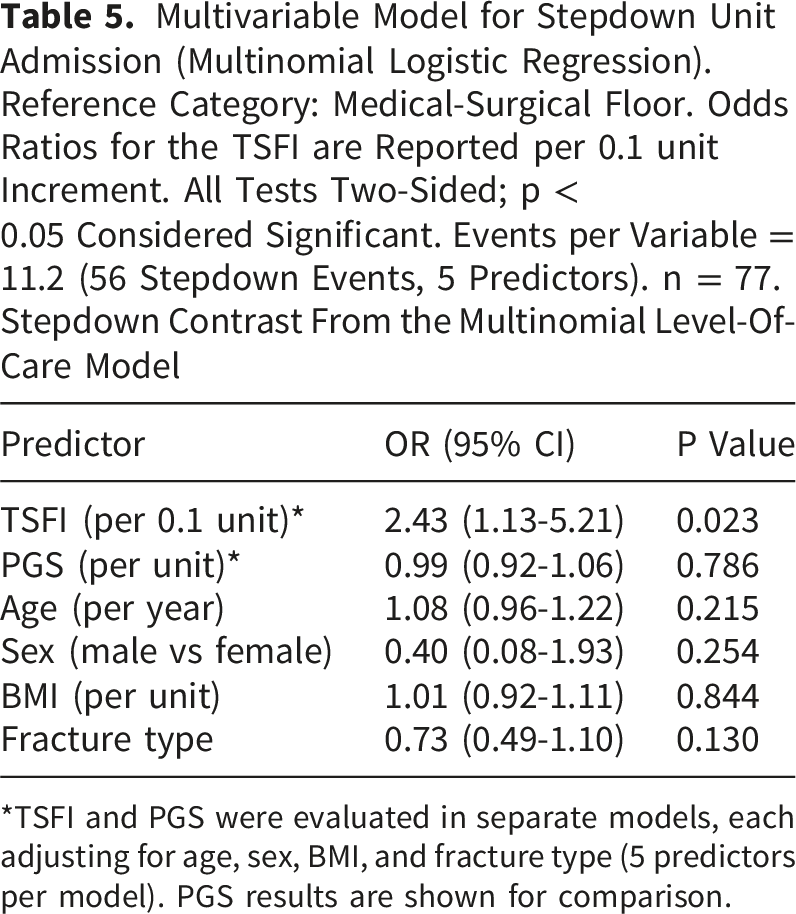
*TSFI and PGS were evaluated in separate models, each adjusting for age, sex, BMI, and fracture type (5 predictors per model). PGS results are shown for comparison.
Multivariable Model for ICU Admission (Multinomial Logistic Regression). Exploratory Analysis. Reference Category: Medical-Surgical Floor. Odds Ratios for the TSFI are Reported per 0.1 unit Increment. Events per Variable = 1.8 (9 ICU Events, 5 Predictors); Estimates Should be Interpreted Cautiously. n = 77. ICU Contrast From the Multinomial Level-Of-Care Model
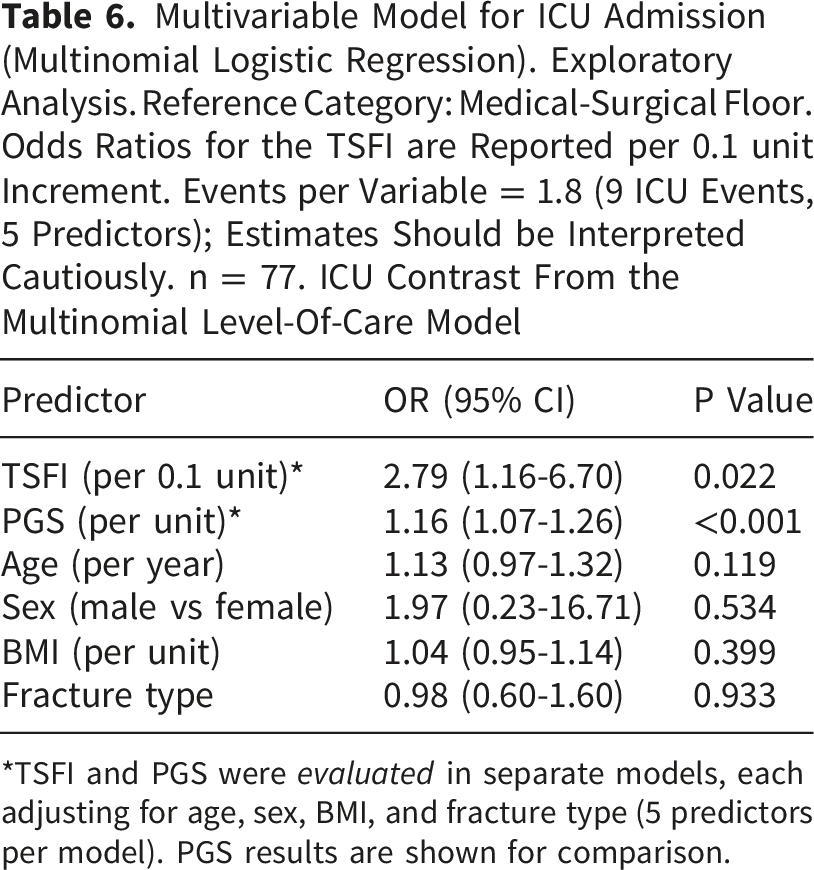
*TSFI and PGS were evaluated in separate models, each adjusting for age, sex, BMI, and fracture type (5 predictors per model). PGS results are shown for comparison.
Multivariable Model for Skilled Nursing Facility Discharge (Binary Logistic Regression). Home Discharge (n = 16) vs Skilled Nursing Facility Discharge (n = 48). Odds Ratios for the TSFI are Reported per 0.1 unit Increment. PGS Evaluated in a Separate Model on the Same Cohort With the Same Covariates. All Tests Two-Sided; p < 0.05 Considered Significant. n = 64. Patients Discharged to Inpatient Rehabilitation (n = 7), Hospice (n = 3), or Other Destinations (n = 4) Were Excluded From This Binary Comparison
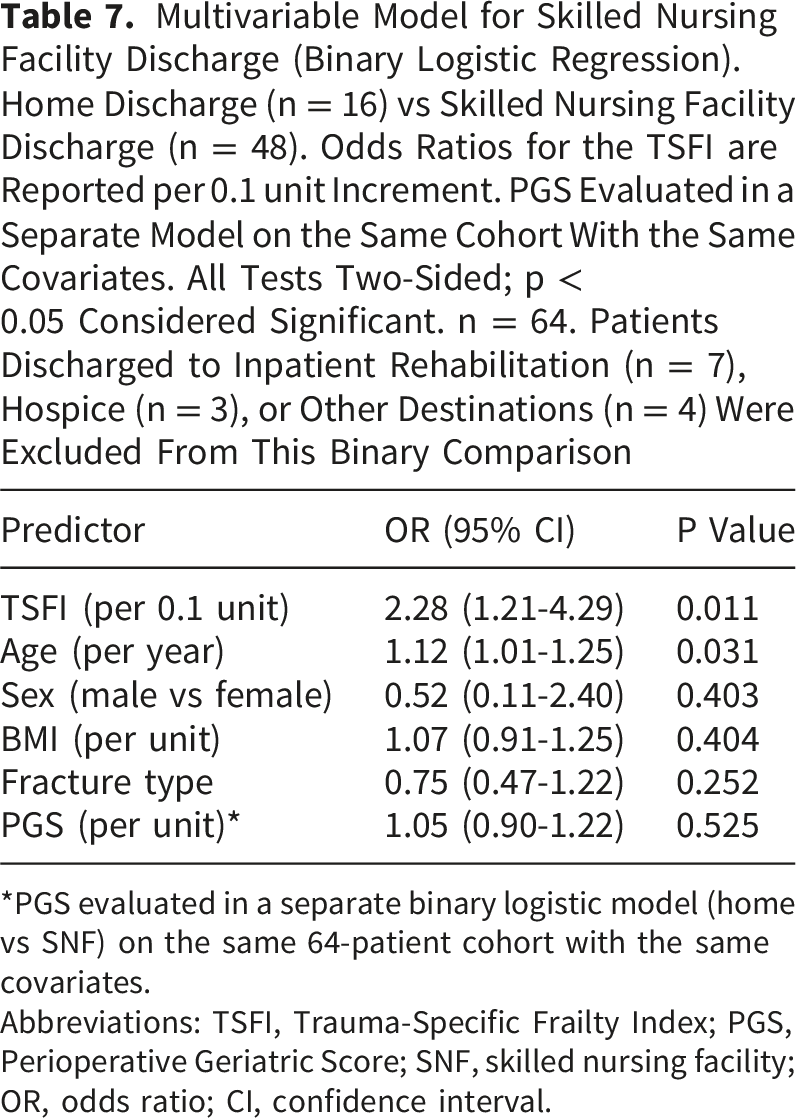
*PGS evaluated in a separate binary logistic model (home vs SNF) on the same 64-patient cohort with the same covariates.
Abbreviations: TSFI, Trauma-Specific Frailty Index; PGS, Perioperative Geriatric Score; SNF, skilled nursing facility; OR, odds ratio; CI, confidence interval.
Multivariable Model for Hospital Length of Stay (Robust Linear Regression). Beta Coefficients Represent the Change in Length of Stay (days) per Unit Change in Each Predictor. All Tests Two-Sided; p < 0.05 Considered Significant. Observations per Predictor = 15.6 (78 Observations, 5 Predictors)
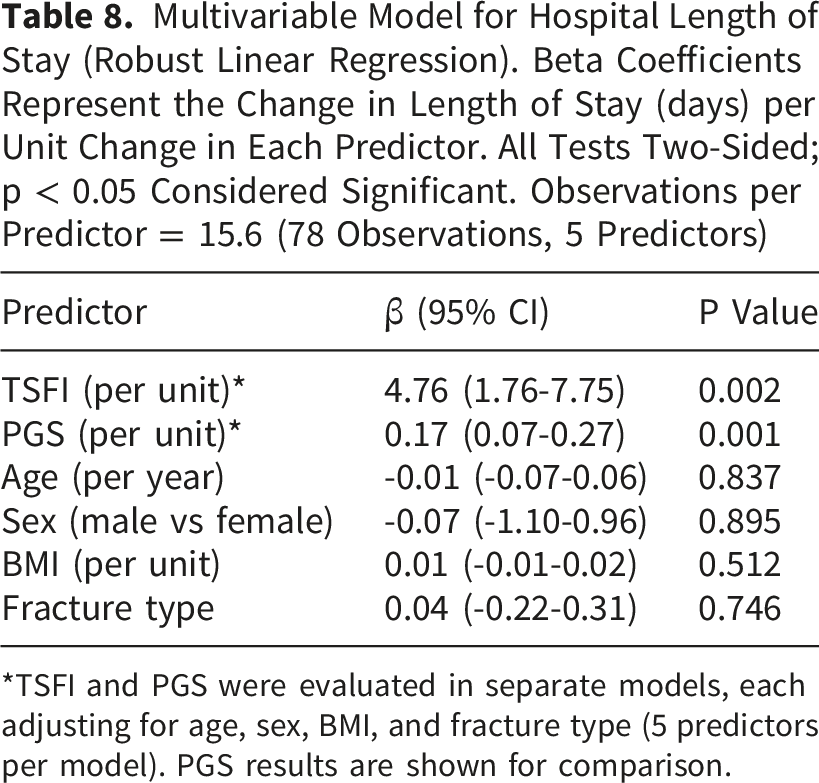
*TSFI and PGS were evaluated in separate models, each adjusting for age, sex, BMI, and fracture type (5 predictors per model). PGS results are shown for comparison.
The present findings align with the current body of literature establishing the TSFI as a robust predictor of discharge to a skilled nursing facility or rehabilitation, prolonged length of stay, major complications, and in-hospital mortality across diverse geriatric trauma populations.16,20-24 Yet, while these outcomes are important markers of long-term recovery and survival, they generally reflect events that occur later in the hospitalization or after discharge. By contrast, the immediate perioperative period, particularly when escalation to a stepdown or ICU is required, represents a pivotal juncture in patient management and influences resource allocation, staffing, and postoperative monitoring intensity. In addition to predicting 90-day healthcare utilization, TSFI scores were also associated with escalation to stepdown and ICU levels of care. In practice, these results may afford clinicians additional predictive utility across the perioperative continuum. The clinical and policy implications of these findings were substantial. Stepdown and ICU utilization drive hospital resource consumption, and early identification of patients likely to require these services enables proactive planning.21,24 Incorporating frailty assessment into initial trauma evaluations may support discussions with patients and families regarding realistic postoperative expectations, guide early consultation with geriatrics and rehabilitation services, and streamline discharge disposition planning. Because Medicare SNF eligibility depends on three qualifying inpatient overnights and timely physical and occupational therapy assessments - which may be difficult to obtain on weekends or after hours - an admission frailty score that predicts SNF disposition could help prioritize early therapy evaluations and insurance precertifications for high-risk patients, allowing transfer to SNF as soon as eligibility criteria are met. From a systems standpoint, embedding frailty tools such as the TSFI into perioperative workflows could help optimize bed utilization, reduce delays in postacute placement, and align with institutional efforts toward value-based care and bundled payment models..16,20,21,23
This study should be interpreted in the context of its limitations. It was conducted within a single academic health system, which may limit generalizability, and the TSFI was implemented at only one clinical site, introducing the possibility of site-related bias. As a retrospective analysis, causal inference cannot be established, and unmeasured confounding remains possible. The sample size, while sufficient to detect several clinically meaningful associations, was modest relative to large trauma registries, and no a priori sample size or power calculation was performed; the study was therefore powered by the available sample, which may have limited the ability to detect associations for less frequent outcomes. This limitation was most evident in the 90-day outcomes, where the low frequency of mortality and readmission events led to wide confidence intervals and model non-convergence; therefore, these analyses should be considered exploratory rather than definitive. Finally, although we compared the TSFI with an institutional perioperative geriatric triage score, future work should evaluate how the TSFI performs relative to other established frailty instruments and in larger, multicenter cohorts.
Conclusion
The TSFI reliably predicted not only discharge to skilled nursing facilities and prolonged hospitalization but also, for the first time, escalation to stepdown and ICU care. Taken together, these findings support a broader role for frailty screening that extends beyond long-term outcomes to immediate perioperative management. Incorporating TSFI into routine trauma workflows may improve risk stratification, strengthen patient counseling, and optimize resource allocation in orthopaedic trauma.
Footnotes
Acknowledgments
The authors thank the orthopaedic trauma registry staff and clinical research personnel at our institution for their assistance with case identification and data abstraction for this project. This study received no external funding.
Ethical Considerations
This study received ethical approval from the University of Cincinnati Institutional Review Board (IRB #2020-0116) on June 23, 2025. This was an IRB-approved retrospective chart review; all patient information was de-identified, and informed consent was waived. Patient data are stored on secure institutional servers and will not be shared with third parties.
Consent to Participate
Informed consent to participate was waived by the University of Cincinnati Institutional Review Board due to the retrospective nature of the study and use of de-identified data.
Consent for Publication
Not applicable. The manuscript does not contain any individual person’s identifiable data, images, or videos.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are derived from institutional clinical and trauma registry databases and contain protected health information. De-identified data may be available from the corresponding author on reasonable request and with appropriate Institutional Review Board and institutional approvals.