
Abstract
Background
The aim of this study was to evaluate patients over 65 years old treated with an angled blade plate (ABP) for distal femoral fractures and determine if the use of ABP was reasonable in this specific population who are prone to complications.
Methods
Consecutive patients with distal femoral fracture who had undergone open reduction and internal fixation with ABP plate between January 2010 and December 2023 were retrospectively analyzed. Medical records were reviewed for age, sex, follow-up, injury characteristics, fracture pattern, and complications, such as malunion, non-union and infection. Clinical evaluation of patients was performed using the international Knee Documentation Committee (IKDC) score.
Results
Twenty-one (18 female; 85.7%) patients were included, with a median (range) age of 78.5 (65-92) years. Mean follow-up was 17 months. Four of the patients sustained high-energy trauma fractures and the remainder fractured because of a simple fall; five were admitted due to the nonunion and three because of complications related to intramedullary nail. Most (85%) had periprosthetic fracture. Only 2/21 (9.5%) had nonunion and implant failure and were revised again with ABP and iliac crest autograft. Furthermore, only 1 (4.8%) with superficial infection needed surgical debridement in the early postoperative period. After a minimum of 12 months follow up the mean IKDC score was 37 (range 21-72).
Conclusion
ABP appears to be a reliable device for the treatment of distal femoral fractures in patients over 65 years, including those with osteoporotic and periprosthetic fractures, and non-unions, with a 90% union rate.
Background
Surgical treatment is a standard method for distal femoral fractures in the adult population. This provides alignment and allows early motion of the knee joint and so improves function of the extremity. 1 There is no consensus about which fixation device is optimal for distal femoral fractures. The 95-degree angled blade plate (ABP) was initially designed for proximal femoral fractures in the 1960s and then found increasing use for distal femoral fractures. However, most of the companies stopped producing this plate and extra effort is required to obtain these ABPs today. Locking condylar plates (LCP) and retrograde intramedullary nail (IMN) are the most commonly used devices currently. A locking plate provides multiple points of fixed angle contact by locked screws and provides increased rigidity, especially in osteoporotic bone or in periarticular fractures with a small distal segment. However, indications for use of a locking plate have not been completely clarified and failures have been reported.2-5 Furthermore, there is a concern about increased stiffness and possible risk of non-union when using locking implants.6-8 Retrograde IMN has been used, especially with extra-articular fractures and periprosthetic fractures. Although, several studies have suggested that retrograde nailing can be used in intraarticular fractures,9-12 iatrogenic comminution and insufficient fixation were reported as potential complications. Moreover, not all prosthetic designs are suitable for nailing if there is a periprosthetic fracture. Even double fixation (double plate or plate and nail together) has also been suggested, especially for complicated fractures in the elderly population. 13
The first choice in our institution for distal femoral fractures is the ABP, even in complicated cases, despite the supply difficulties. The aim of this study was to evaluate patients over 65 years old treated with ABP for distal femoral fractures and determine if the use of ABP was reasonable for this age group who are prone to complications. Variables considered included the rate of healing, alignment, need for secondary surgery, and complications. Our hypothesis was that ABP fixation provided good clinical results in this elderly population for the treatment of distal femoral fractures, even in complicated cases such as non-unions and periprosthetic fractures.
Methods
Approval for this study was granted by the local ethics committee. In addition, a comprehensive agreement for academic use of information such as type of treatments, treatment progress or any other data acquired during their treatments was obtained from the patients by the hospital at the time of their hospitalization. Consecutive patients with distal femoral fracture who had undergone open reduction and internal fixation with ABP plate between January 2010 and December 2023 were retrospectively analyzed. Patients younger than 65 years-old, who had less than one-year follow-up, and whose x-rays and other clinical documents were not available were excluded. All surgery and clinical and radiological evaluations were performed by the authors.
ABP is a standard surgical method in our institution for all distal femoral fractures including cases of non-union and periprosthetic fractures, with the exception of open fractures, widely comminuted, intra-articular high energy fractures, fractures with insufficient lateral cortex for blade insertion and coronal plane (Hoffa) fractures. Medical records were reviewed for age, sex, follow-up, injury characteristics, fracture patterns, complications such as malunion defined as more than 5-degree varus or valgus malalignment, non-union defined as persistent pain and incomplete cortical healing on at least three cortices on plain radiograph within six months, and infection.
All patients underwent surgery with lateral approach in the supine position. After open reduction, Kirchner wires and clamps were used for provisional fixation, supplementary lag screws used for intra-articular fragments and then the ABP was applied under fluoroscopic control. Iliac crest autograft was used for cases of non-union. Non-weight bearing was recommended for eight weeks postoperatively. As a routine, follow-up visits were scheduled at two weeks, four weeks, two months, three months, six months, one year postoperatively and then annually. Radiographic measurements were made by an orthopaedic surgeon who was not a treating surgeon. Postoperative clinical evaluation of patients was performed using the International Knee Documentation Committee (IKDC) score at least 12 months after the surgery.
The collected data were statistically analyzed using IBM SPSS, version 22 (IBM Inc., Armonk, NY, USA). The fit of the quantitative parameters to the normal distribution was evaluated with the Shapiro Wilks test and it was found that the parameters did not show normal distribution. Descriptive statistical methods including mean and standard deviation, and frequency and percentage (%) are given and quantitative data were compared with the Mann Whitney U test.
Results
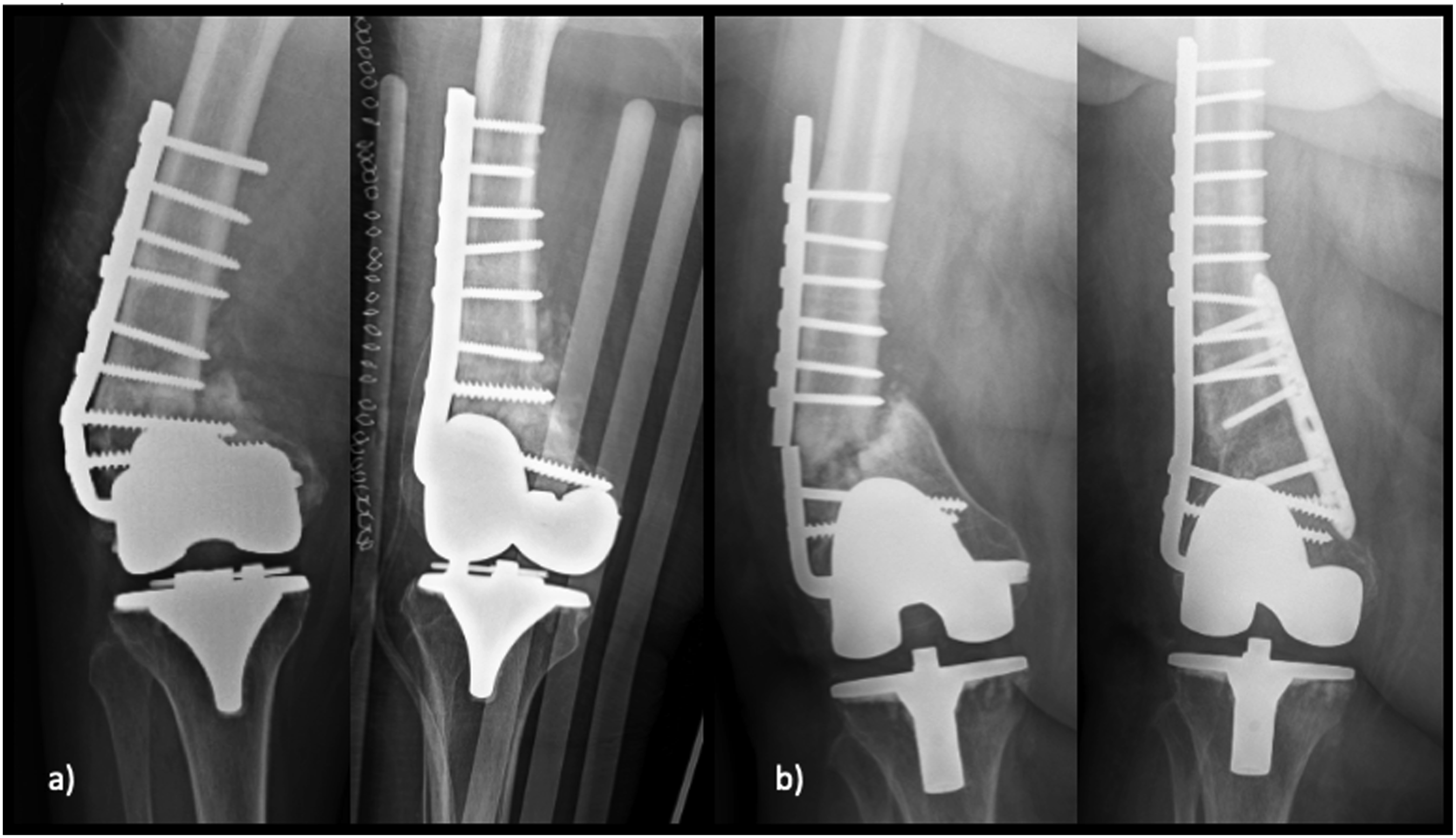
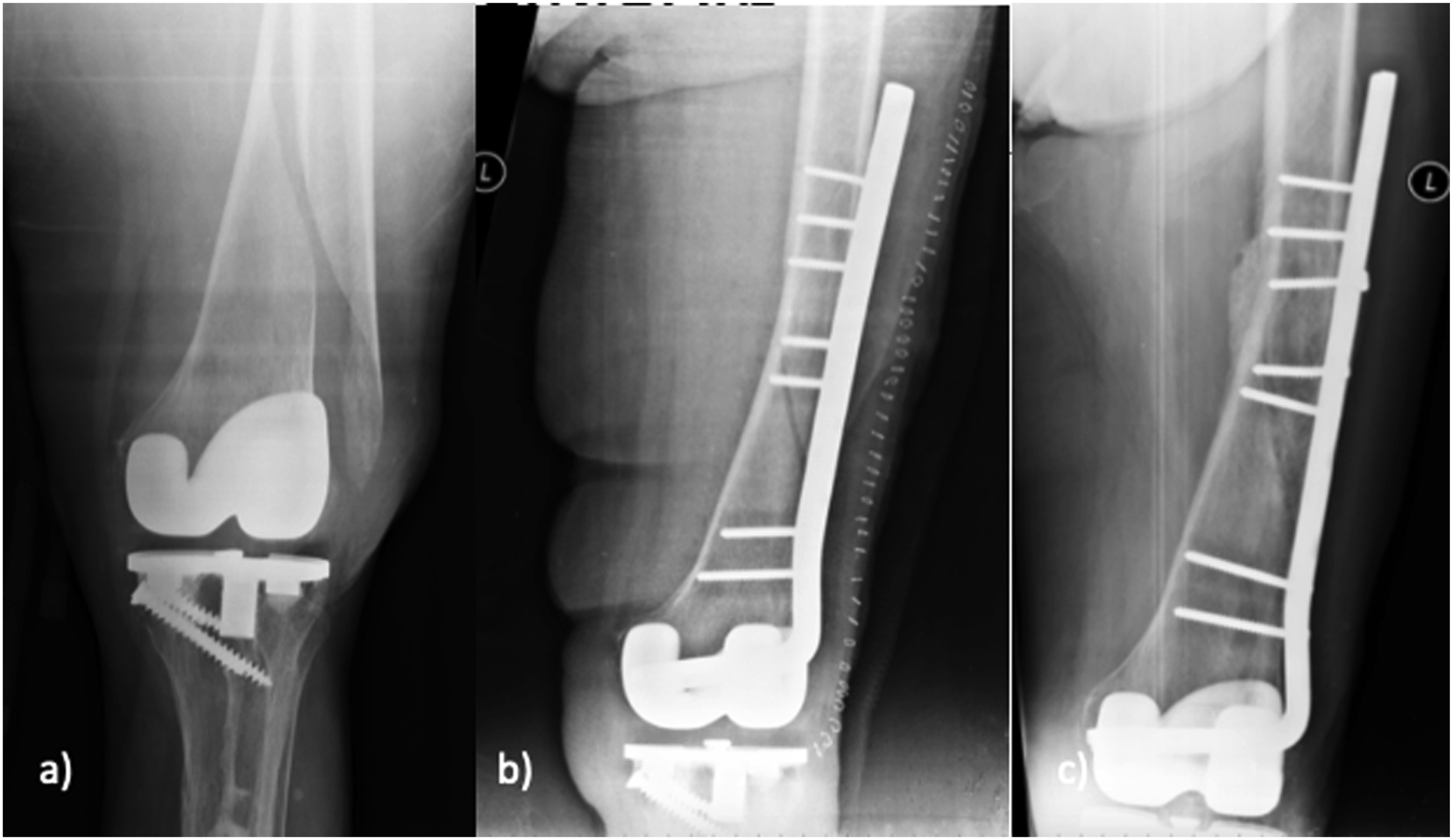
Sixty-six patients were identified as having been treated with ABP. However, 46 were excluded due to either insufficient follow-up and/or incomplete medical records and/or being younger than 65 years of age. Thus, 21/66 (31.8%) of all patients treated with ABP were included. The median (range) age was 78.5 (65-92) years and 18 (85.7%) were female. Median follow-up was 17 (12-26) months. Four (19.1%) of the patients had sustained high energy trauma (motor vehicle accident), and the remaining 17 (80.9%) had fracture as a result of simple fall. Of these 21 patients, 5 (23.8%) were admitted due to non-union because of failure of a LCP (Figure 1) and 3 (14.3%) had complications related to IMN and who were operated in different institutions (Figure 2). Eighteen (85%) of the patients had periprosthetic fracture. Only 2/21 (9.5%) had non-union and implant failure and had to undergo revision with ABP and iliac crest autograft (Figure 3). Four (19.1%) of the patients had varus malalignment when compared with their other knee at the last follow-up, and there was 1 (4.8%) valgus malalignment (Figure 4). Of note, only 1 (4.8%) with superficial infection needed surgical debridement in the early postoperative period. After a minimum of 12 months follow up the median IKDC score was 37 (range 21-72), which indicated residual dysfunction and was an expected result because of population characteristics. Radiographs of five different patients (A) had non-union and implant failure (B) after revision with angled blade plate Radiographs of the patients who had an intramedullary nail and was treated with angled blade plate. (A) Supracondylar fracture distal to the antegrade intramedullary nail, (B) non-union of the distal femoral fracture after treatment with an intramedullary nail, (C) supracondylar femoral fractur in a patient who has total knee prosthesis and intramedullary femoral nail Two patients who were treated with an angled blade plate and had subsequent non-union Union achieved in a distinct varus position

Discussion
This study found that ABP was a reliable option for distal femur fractures in patients over 65 years-old. A 90% union rate was achieved with only two non-unions and one superficial infection in this osteoporotic elderly population, including patients with non-union and periprosthetic fractures (Figure 5). Complicated 90 years old patient: (A) Postoperative radiograph after collum femoris fracture, (B) debridement and replacement of the prosthesis with a spacer because of prosthetic infection, (C) distal femoral fracture during prosthesis removal and osteosynthesis with an angled blade plate, (D) removal of the spacer and prosthetic reconstruction with a trochanteric plate, (E) periprosthetic fracture 2 months after surgery, (F) after achievement of the distal femoral union, removal of the angled blade plate and osteosynthesis with a femoral shaft plate
ABP was a traditional method for open reduction and internal fixation for distal femoral fractures. LCP and retrograde IMN subsequently gained popularity and most of the companies stopped producing ABP, although there are current published studies that advocate the superiority of ABP. LCP supplies multiple points of fixed-angled contact in distal femur and increases the rigidity. Therefore, it appears superior to the ABP, which has only one fixed angled portion, especially in osteoporotic bone or fractures with a small distal segment. However, there is a concern about the effect of increased rigidity on fracture healing14,15 and many failures related to the use of LCP have been reported.2-5
Limited soft tissue damage and preservation of fracture hematoma are the main advantages of retrograde IMN, especially for extra-articular fractures. 16 Although there are several studies that reported better results with IMN than LCP for distal femoral fractures, even in intra-articular fractures, difficulties in practice and complications related to the fixation of articular fragments were highlighted.9-12,17 There are several factors that explain the popularity of LCP and retrograde femoral IMN for the treatment of distal femoral fractures. These were introduced more recently and easy to obtain. Surgical technique may be less demanding for IMN and LCP and young surgeons are not familiar with the classical ABP because of the fall from favor of this rudimentary device.
Although the ABP is a historically used device and its use is now limited, there are current biomechanical and clinical advantages. Even prospective randomized studies have advocated the superiority of ABP over LCP and retrograde IMN. Heather et al compared ABP and the LCP for the treatment of distal femoral fractures. 8 They assessed complications including infection, non-union and malunion, and secondary procedures in fractures suitable to treatment with either implant. They retrospectively evaluated 70 patients with 71 fractures. Thirty-two fractures were treated with ABP and 39 were treated with the LCP. These authors reported that patients treated with LCP had more complications and non-unions and requiring more secondary procedures. Vandenbussche et al evaluated outcomes after ABP fixation and after fixation using condylar screw plate, retrograde IMN and LCP. 18 They reviewed two multicenter studies, one prospective and the other retrospective, and compared four groups. There was no significant difference in terms of complication rates, need for bone grafting, non-union rates and IKDC values. The early surgical revision rate was lower in the ABP group than the other three groups (p=0.02). A 2020 prospective randomized study by Patterson et al compared LCP with ABP for distal femoral fracture amenable to either device. Forty-five patients were treated with LCP and 34 patients treated with ABP. It was reported that ABP had superior performance to LCP for union rate and need for secondary procedure. 19 Besides acute fracture, ABP has been suggested as a rescue surgical option in revision surgeries in many clinics. 18 Patterson et al reported that they used ABP for distal femoral non-unions but not for acute fractures and even criticized themselves about why they did not use it in the first place, even though it was four times cheaper than LCP. 19 Amorosa et al examined the results of the use of ABP in proximal and distal femoral non-unions. The healing rate for aseptic, non-unions using the ABP was 91.2%.
There are also biomechanical studies evaluating the best device for distal femoral fractures. 20 Batista et el. compared ABP with LCP for distal femoral open wedge osteotomy. ABP achieved higher stiffness mean values than LCP for both axial compression and torsion loads and was suggested as an alternative fixation method for supracondylar open wedge osteotomy. 21 Higgins et al also biomechanically compared ABP and LCP for distal femoral fractures in cadaveric femurs. They found that LCP was stronger than ABP during cyclic loading and ultimate strength but they tested only axial loading, while torsional stiffness and bending were not tested and was acknowledged as a limitation in their study. 22 Although ABP has fallen from favor as an initial fixation device for distal femoral fractures, it appears that ABP is effective, and even may be superior to other devices.
However, there is no published information about the use of ABP in elderly, osteoporotic patients whose treatment is more challenging. Chen et al reported that complication rate after fixation with femoral nail and locking plate was 15-20% in periprosthetic distal femur fractures, so osteoporotic patients need modified fixation methods to strength the construct. They used experimental and finite element methods and compared LCP, retrograde IMN and their modifications. Retrograde IMN was supported with a spiral blade at the distal portion of the nail and LCP was used with a strut allograft. These authors recommended an allograft and LCP combination for the periprosthetic fractures in osteoporotic patients. 23 In a 2020 study, Stoffel et al highlighted the difficulty of stable fixation in complex distal femur fractures and advocated the use of double fixation constructs as a solution. They defined complex fractures as high energy open fractures, osteoporotic fractures in the elderly and periprosthetic fractures and reviewed studies using double fixation, such as double plate (medial and lateral) and retrograde IMN with lateral plate. They concluded that there is a growing need for double fixation constructs for complex distal femoral fractures13,24 In the current study, we evaluated patients over 65 years old treated with ABP for distal femoral fractures, including osteoporotic patients, periprosthetic fractures and non-unions. Efficacy of the ABP on the treatment of distal femoral fractures was shown several times in the literature but there was no information about its use in this age group.
Conclusion
In conclusion, although there are limitations of the current study, such as retrospective design and lack of control group, it was demonstrated that ABP was a reliable device for the treatment of distal femoral fractures in patients over 65 years old, including osteoporotic and periprosthetic fractures and nonunions, achieving a 90% union rate. Orthopaedic surgeons should consider the use of an ABP, a simple and cheap device, as an alternative to complicated solutions, such as using double fixation or modifying standard techniques for these complicated fractures.
Footnotes
Ethical Considerations
Approval for this study was granted by the local ethics committee with the approval number of 2025/662 and the decision number KÜ GOKAEK-2025/25/27.
Consent to Participate
Informed consent about being part of a study obtained from all patients before surgery as a part of university clinical routine.
Author Contributions
All authors contributed to the study conception and design. SD and CE write the manuscript, SE an MU collected data and prepared figures, EI and CCK did final revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.