
Abstract
Background
Osteoporotic fractures represent a major public health problem, particularly in older adults. Distal femur fractures, although less frequent, have also been associated with substantial mortality, with rates approaching those of hip fractures. However, direct comparisons between both entities remain limited and heterogeneous, and it is unclear whether distal femur fractures carry a comparable prognostic burden.
Methods
We conducted a retrospective observational cohort study including surgically treated patients aged ≥65 years with proximal or distal femoral fractures between 2013 and 2019. Distal fracture cases were compared with a proximal femoral fracture cohort. Cases were identified using ICD codes and validated through clinical record review. The primary outcome was all-cause mortality at 30, 90, and 365 days after surgery. Survival was analyzed using Kaplan-Meier curves, compared with the log-rank test. Cox proportional hazards models were used to assess the association between fracture type and mortality, adjusting for relevant clinical variables.
Results
A total 234 proximal and 74 distal femoral fractures patients were included. One-year mortality was similar between groups (27.4% vs. 35.6%, p=0.176). However, mortality was significantly higher in distal fractures at 30 days (16.2% vs. 7.7%, p = 0.031) and 90 days (24.3% vs. 14.1%, p = 0.039). Kaplan-Meier analysis showed significant differences at 30 and 90 days but not at 365 days. In multivariable Cox regression, fracture type was not independently associated with mortality, while rurality was associated with lower mortality.
Conclusion
Although distal femoral fractures were associated with higher short- and mid-term mortality, fracture type was not an independent predictor of mortality after multivariable adjustment. Rurality emerged as an independent predictor of survival, warranting further investigation. These findings suggest that distal femur fractures may require a similar level of clinical attention.
Keywords
Introduction
Osteoporotic fractures are a serious health problem and a condition with a very high incidence due to the increase in life expectancy of the population. 1 Of all fragility fractures, those that have received the most attention are proximal femur fractures, given their serious repercussions in terms of morbidity and mortality. 2 Mortality rates following hip fracture are high, predominantly affecting older adults,3,4 and represent one of the leading causes of death in this population, 5 with one-year mortality rates ranging from 20% to 30%.6,7
Their clinical severity is partly explained by specific anatomical and physiological factors. In particular, femoral neck fractures are characterized by a precarious vascular supply8,9 which often necessitates early surgical intervention to prevent complications and avoid reoperations that would markedly increase morbidity and mortality in this vulnerable population. 10
Another type of osteoporotic fracture is distal femur fractures, which also have a high incidence. 11-13 These fractures, as well as proximal femoral fractures, often occur as a result of a low-energy mechanism, most commonly a fall from standing height in older adults2,3,11,12. Although less frequent than proximal femoral fractures, various studies show that they have a significant clinical impact in terms of mortality. 14 Studies have demonstrated mortality rates of 16% at 6 months, increasing to 30% at one-year follow-up. 15
Distal femur fractures may present either as periprosthetic fractures or as native fractures, unrelated to any implant. The latter have received considerably less attention compared with periprosthetic fractures.
Several studies have shown the characteristics of distal femur fractures in the older population. 15 They often settle in the distal metaphysis of the femur with proximal and distal extension and also affect the knee joint. It is necessary to achieve adequate reduction to prevent deformity and firm osteosynthesis to allow early mobilization and weight bearing, avoiding prolonged immobilization and joint stiffness. 16
Treatment of distal femur fractures consists of osteosynthesis with either a plate or intramedullary nail. 17 In some complex cases, prosthetic replacement of the distal femur has been proposed. 18 As with proximal femoral fractures, surgical treatment should be performed early.
Despite the well-established clinical relevance of proximal femoral fractures, distal femur fractures remain comparatively under-characterized in older adults, distal femur fractures are less frequent but are increasingly recognized as a serious condition in elderly patients. Several studies have reported substantial mortality following distal femur fractures, with rates approaching those observed after hip fractures. For instance, Streubel et al reported a one-year mortality rate of approximately 25% in older adult patients with distal femur fractures. 12
However, direct comparisons between distal and proximal femoral fractures remain limited and heterogeneous, and it is still unclear whether distal femur fractures represent a condition with a comparable prognostic burden. This lack of clarity has important clinical implications. While proximal femoral fractures benefit from well-established orthogeriatric care pathways, distal femur fractures are not consistently managed within the same framework, despite potentially similar outcomes.
Therefore, a direct comparison between both entities is necessary to better understand their relative impact in terms of survival and clinical characteristics, and to determine whether distal femur fractures should be considered within a similar paradigm of clinical urgency and multidisciplinary management.
We hypothesized that surgically treated distal femoral fractures in older adults would show survival outcomes comparable to those observed after proximal femoral fractures.
The aim of this study was to compare survival between surgically treated patients aged 65 years and older with proximal and distal femoral fractures using Kaplan-Meier analysis at 30, 90, and 365 days of follow-up. Additionally, we aimed to assess the association between fracture type and mortality using Cox proportional hazards models adjusted for relevant clinical variables.
As secondary objectives, we sought to characterize and compare the baseline clinical profiles of patients in both groups, including comorbidity burden and perioperative variables.
Material and Methods
Study Design and Setting
After ethical approval from the Reference Ethics Committee (Ref. PI 2020 01 420). We conducted an observational, longitudinal, retrospective cohort study including surgically treated patients aged 65 years and older with a primary diagnosis of proximal or distal femoral fracture between August 10, 2013, and December 13, 2019. Proximal femoral fractures were identified using ICD-9 code 820.x. Distal femoral fractures were identified using ICD-9 code 821.x and ICD-10 codes S72.3–S72.4, according to the coding system in use at the time of admission and subsequently confirmed based on clinical and anatomical classification.
All available distal femoral fracture cases were accrued over the full study period, from August 2013 to December 2019, for a total of 88 cases. The proximal femoral fracture cohort was derived from a previously historical reference cohort from the same institutional setting, collected from December 2013 to July 2014. Accordingly, the study was designed as a comparison between an accrued distal femur fracture cohort and a historical proximal femur reference cohort. Given the higher incidence of proximal femoral fractures, it was considered appropriate to use a larger reference cohort, with a 1:3 ratio relative to the distal femoral fracture cohort, in order to ensure a sufficiently large comparison group without compromising analytical feasibility. 19 The proximal and distal fracture cohorts were mutually exclusive. No patient belonged to both cohorts.
Patients were identified from the hospital administrative database, managed by the Clinical Documentation Department, after a formal request, using diagnostic codes from both ICD-9 and ICD-10 classification systems, according to the coding system in use at the time of admission. Once the dataset was obtained, to minimize potential inconsistencies, a direct clinical verification procedure was used instead of relying solely on automatic mappings between coding systems. Patients were classified as having proximal or distal femoral fractures by cross-checking the administrative code against the clinical diagnosis recorded in the medical record by the geriatricians.
Patient selection and data validation followed a structured multistep process. First, the initial identification of cases using ICD-9 and ICD-10 codes by the Clinical Documentation Department. Second, cases were screened according to the predefined inclusion and exclusion criteria (Figure 1). Third, a manual review of the clinical diagnosis recorded in the medical record, including data cleaning procedures such as the identification and removal of duplicate records, verification of date consistency, and assessment of missing or implausible values in key variables. Finally, the classification of each type of fracture (proximal or distal) according to the clinically described anatomical location. Missing data were minimal, with 98.7% of values available. Analyses were conducted using all available data for each variable, given the low proportion of missing values. Flow diagram of patient selection and inclusion in the study cohort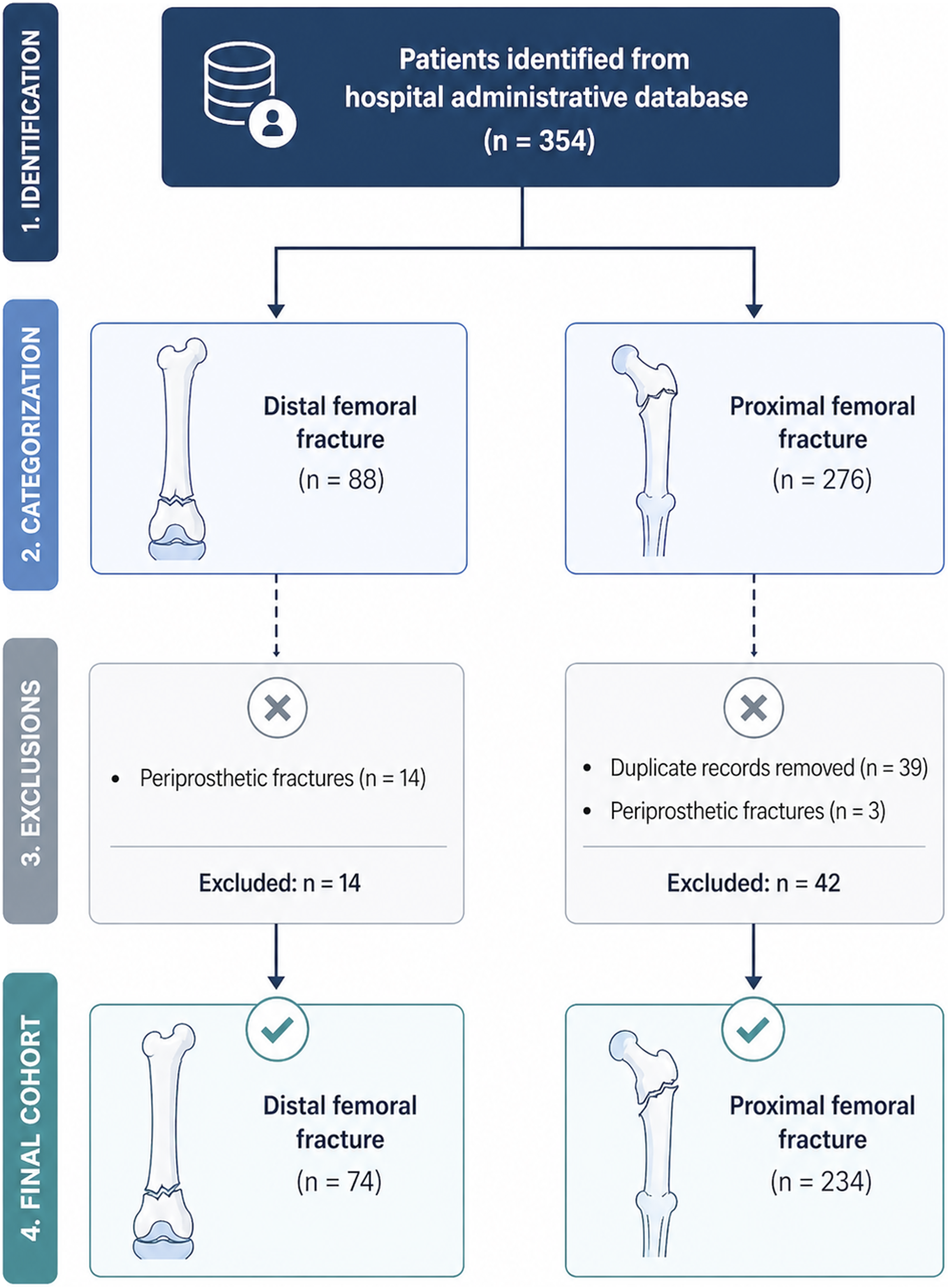
The clinical categories used for classification were, for proximal femoral fracture: subcapital, basicervical, pertrochanteric and subtrochanteric, broadly corresponding to AO/OTA 31A, 31B and 32-a patterns. The recorded distal femoral fracture categories were supracondylar, distal third diaphyseal and unicondylar fractures, broadly corresponding to AO/OTA 33A, 32-c and 33B fracture patterns, respectively.
In the analysed dataset, differences between coding systems primarily concerned the inclusion of additional details, such as lateralization or other specifications, without affecting the primary anatomical classification of the fracture.
Selection Criteria
Inclusion criteria were patients aged 65 years or older with non-periprosthetic femoral fracture caused by a low-energy trauma, such as a fall from a standing height. Fractures caused by high-energy mechanisms or those related to tumour pathology or other etiologies, such as atypical fractures related to bisphosphonate use, were excluded.
Data Sources and Variable Measurement
Once the raw dataset was received, the research team refined and analyzed the following variables categorized into the following groups:
Patient sociodemographics: age, sex, rurality, and date of birth were extracted from administrative records.
Baseline clinical and preoperative risk variables: To assess the burden of comorbidity at the time of injury, the Charlson Comorbidity Index (CCI) was calculated for each patient based on comorbidities obtained from patient clinical records. The CCI is calculated by adding the coefficients assigned to comorbidities present at enrolment. 20 Also, the American Society of Anesthesiologists (ASA) grade was obtained from the preoperative anesthetic assessment recorded in the electronic medical records. Polypharmacy status, antiplatelet therapy, and anticoagulant therapy were considered too.
Comorbidities: Comorbidities were obtained from the dataset based on previously documented diagnoses recorded in the electronic medical records. These included diabetes mellitus; digestive and hepatobiliary conditions (such as gastroesophageal reflux disease, hiatal hernia, chronic gastritis, diverticulitis, gastric ulcer, diarrhea, and pancreato-biliary disease); cardiac comorbidities (including chronic heart failure, valvular heart disease, arrhythmia, and ischemic heart disease); renal comorbidities (including chronic kidney disease and urinary tract infection); pulmonary diseases (such as chronic obstructive pulmonary disease, pulmonary embolism, and asthma); and history of cancer (including digestive, pulmonary, gynecological, endocrine, hematological malignancies, bone metastases, and renal cancer).
Injury and Surgical Characteristics: We recorded the fracture type and its anatomical location (proximal vs. distal).. For distal fractures, we confirmed the use of lateral locked plating (osteosynthesis), while for proximal fractures, the type of surgery, osteosynthesis or prosthetic replacement, was noted. The time from admission to surgery (in days) and the length of hospital stay were also recorded.
Outcome Variable: The primary outcome was all-cause mortality at 30, 90, and 365 days after surgery. Mortality status and date of death were obtained from the hospital’s electronic medical records. Time-to-event was calculated from the date of surgery to the date of death or last follow-up. Complications were registered too as postoperative outcomes: postoperative seroma, postoperative bleeding, mechanical complications, renal complications, cardiac complications, and respiratory complications, as well as prosthetic infection.
Study Sample Size
To ensure the reliability of our sample, a posteriori calculation of the sample size was done to verify that the number of subjects was sufficient to detect a significant difference in mortality. According to previous studies 21 , the mortality rates were estimated at approximately 38% for the distal femoral fracture cohort and around 18% for the proximal femoral fracture cohort. Taking these rates into account, we performed a post hoc sample size calculation with a power of 80%, a two-sided significance level of 5%, and a 1:3 ratio, using the Sample Size Calculator from the Cleveland Clinic Risk Calculator Library. 22 The calculation indicated that an optimal sample size would be 61 subjects in the distal cohort and 183 in the proximal cohort.
All patients received surgical treatment. All distal femoral fractures were treated with osteosynthesis, particularly with plate fixation. Proximal femur fractures were managed with osteosynthesis or with prosthetic replacement, depending on fracture type and patient characteristics.
Statistical Methods
Statistical analysis was performed using the software IBM SPSS 23. A descriptive analysis was carried out using frequencies and contingency tables for qualitative variables, and for describing quantitative variables, the mean and the standard deviation were used. In addition, the normality was studied using the Kolmogorov-Smirnov test (Lilliefors corrected).
According to the inferential analysis, the chi-square or Fisher’s exact test, was used to analyse the relation between qualitative variables, as appropiate, and the Mann-Whitney test for quantitative variables. Then, a survival analysis was performed using Kaplan-Meier curves. Group comparison by a factor for patients’ survival was done using the Log-Rank test. Cox regression was used to assess the independent effect of clinical and demographic variables on survivorship, adjusting for potential confounders: age, gender, CCI, rurality, type of fracture and time to surgery, selected based on their role in the relationship between fracture type and mortality. Hazard ratios (HRs) with 95% confidence intervals were calculated, and statistical significance was set at a two-tailed p ≤ 0.05.
Results
Participants and Descriptive Analysis
A total of 308 patients were included in the study, 234 with proximal femur fractures and 74 with distal femur fractures. Within one year of follow-up, 64 patients (27.4%) with proximal femoral fractures died during this period of time and 26 patients (35.6%) with distal femoral fractures.
The mean age was 85.6 years (range 65–103) in the proximal group and 85.5 years (range 65–103) in the distal group. Men were significantly more frequent among patients with distal fractures (53.4%) and the distribution between urban and rural residence did not differ significantly.
Comparison of Baseline and Clinical Characteristics
Baseline Characteristics of the Study Population
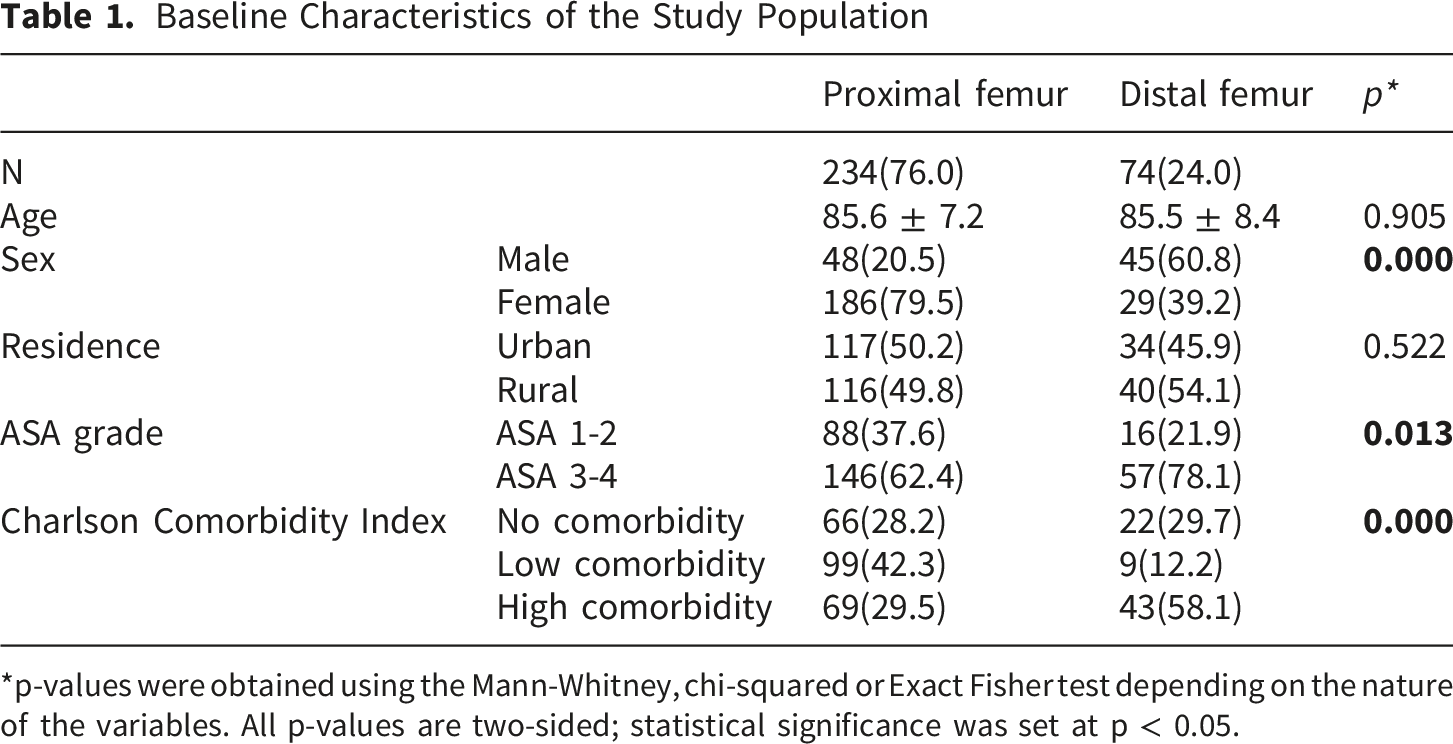
*p-values were obtained using the Mann-Whitney, chi-squared or Exact Fisher test depending on the nature of the variables. All p-values are two-sided; statistical significance was set at p < 0.05.
Clinical Variables
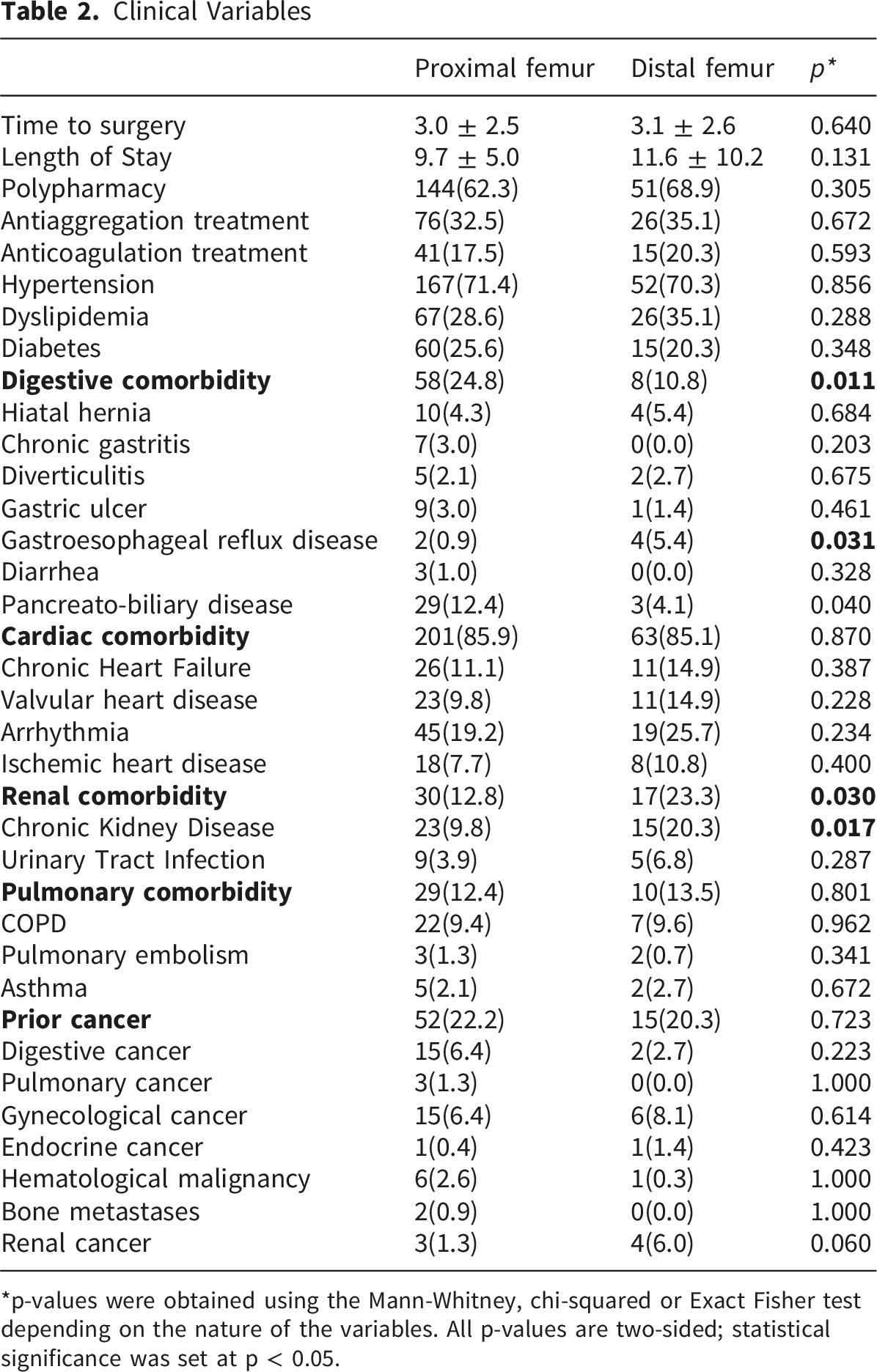
*p-values were obtained using the Mann-Whitney, chi-squared or Exact Fisher test depending on the nature of the variables. All p-values are two-sided; statistical significance was set at p < 0.05.
The prevalence of polypharmacy, antiplatelet therapy and anticoagulant therapy was similar between groups. Patients with distal fractures had a significantly higher prevalence of renal comorbidity (23.3% vs. 12.8%, p = 0.030). Within this category, chronic kidney disease was also significantly more prevalent in this group (20.3% vs. 9.8%, p = 0.017).
In contrast, digestive comorbidity was significantly more prevalent in patients with proximal femur fractures (24.8% vs. 10.8%, p = 0.011) and within this category, gastroesophageal reflux disease was significantly more frequent (5.4% vs. 0.9%, p = 0.031). This latter finding should be interpreted with caution due to the low number of cases.
No significant differences were observed for cardiac, pulmonary, or overall cancer history between the two groups.
Postoperative Complications
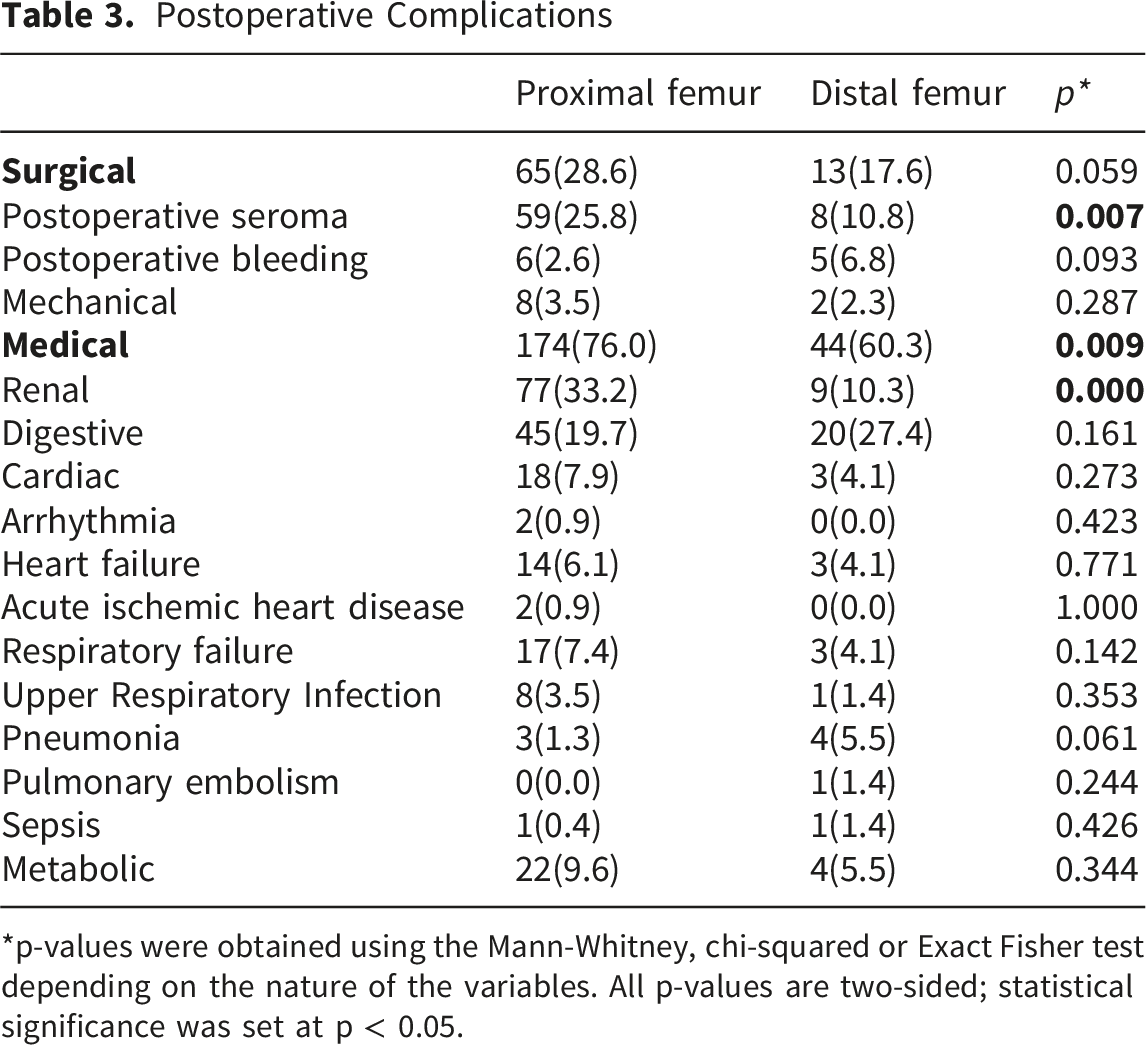
*p-values were obtained using the Mann-Whitney, chi-squared or Exact Fisher test depending on the nature of the variables. All p-values are two-sided; statistical significance was set at p < 0.05.
Mortality Rates According to the Type of Fracture
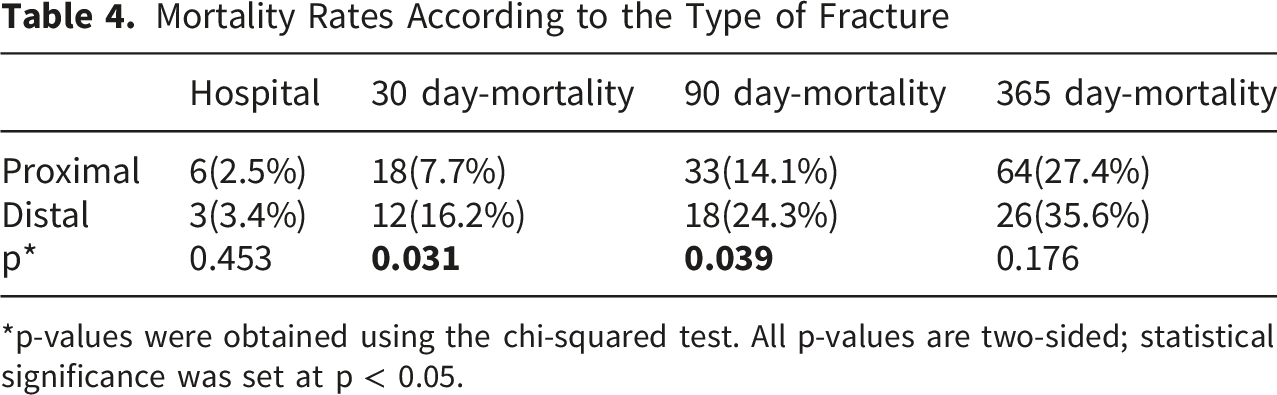
*p-values were obtained using the chi-squared test. All p-values are two-sided; statistical significance was set at p < 0.05.
Mortality and Survival Analysis
In our study, in-hospital and 365-day mortality rates did not differ significantly between distal and proximal fractures (p = 0.453 and p = 0.176, respectively). However, mortality rates were significantly higher in patients with distal femur fractures at 30 days of follow-up (16.2% vs. 7.7%, p = 0.031) and 90 days of follow-up (24.3% vs. 14.1%, p = 0.039).
Kaplan-Meier curves (Figure 2) showed a steeper early decline in survival in patients with distal femur fractures. When survival was analyzed separately at different follow-up horizons, significant differences between survival curves were observed at 30 days (p = 0.025) and 90 days (p = 0.028), but not at 365 days (p = 0.122). Kaplan-Meier survival curves comparing cumulative survival in patients with proximal or distal femur fractures at 30, 90, and 365 days of follow-up, with Log-Rank p-values displayed. All p-values are two-sided; statistical significance was set at p < 0.05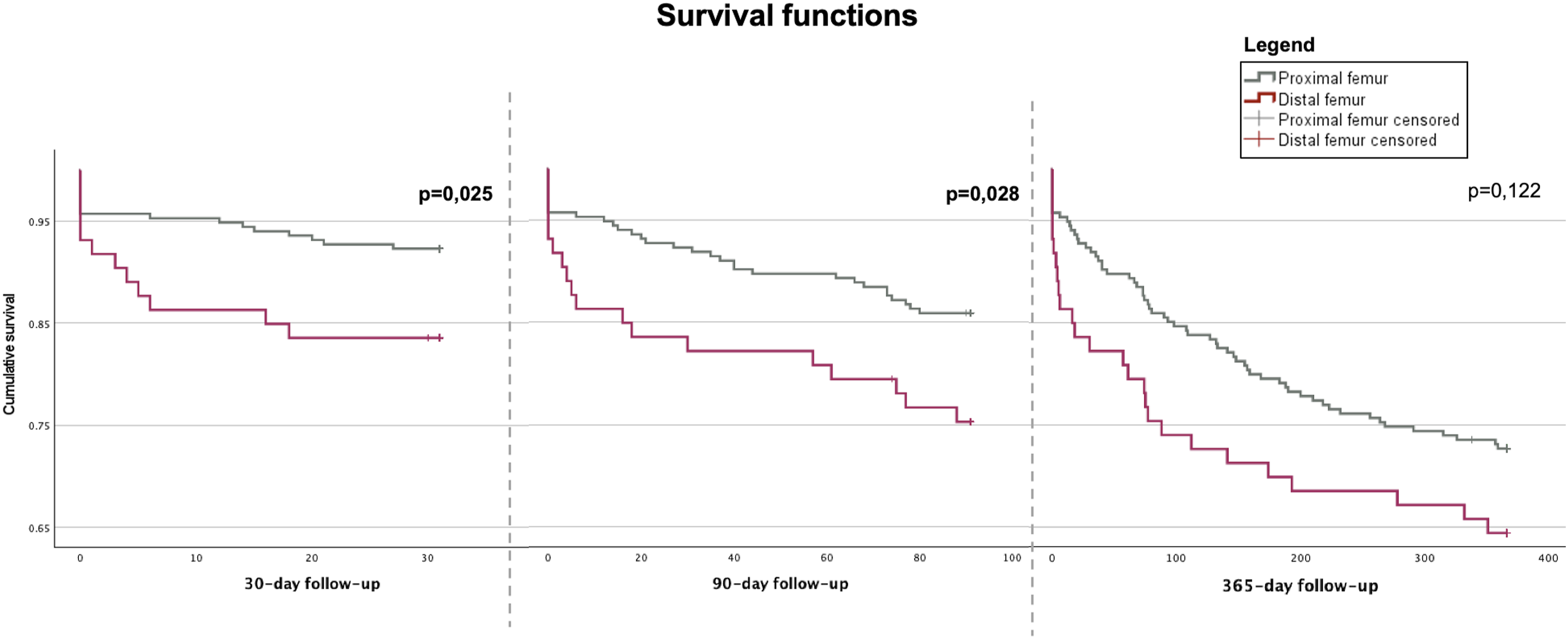
Multivariable Cox regression analysis showed that rurality was independently associated with survival, with patients from rural areas showing a lower risk of mortality at 90 days (HR 0.48; 95% CI 0.27–0.85; p = 0.012) and at 365 days (HR 0.65; 95% CI 0.43–1.00, p = 0.042).
No statistically significant association was observed for fracture type, proximal vs distal. Age, sex, and Charlson Comorbidity Index showed a trend toward increased mortality risk, although these associations were not significantly associated with mortality at 30, 90, or 365 days.
Discussion
Key Results and Interpretation
The main finding of this study is that survival among surgically treated patients for distal and proximal femur fractures was similar in long-term, with no significant differences observed at 365 days of follow-up. However, early mortality at 30 and 90 days was significantly higher in patients with distal femoral fracture. In contrast, after adjusting a Cox regression model, fracture type was not independently associated with mortality at any time point.
In this context, patients with distal femur fracture, presented a significantly worse baseline clinical profile, including higher CCI scores and higher proportion of ASA III and IV. However, these variables were not independently associated with mortality in the multivariable model. Although baseline comorbidity differs between groups, these indices do not reflect association of these variables in explaining mortality differences. Instead, the observed early mortality excess in distal fractures may reflect residual confounding, unmeasured variables, or acute perioperative factors not captured in the dataset, such as frailty, functional status, or early postoperative complications.
Notably, rurality raised as the only independent predictor of survival, with rural patients showing a lower risk of mortality. This aspect has been barely studied, particularly in distal femur fractures. However, the available evidence from hip fracture populations, suggests that differences between urban and rural settings may influence mortality outcomes. These differences, tend to emerge during follow up but not in the early stages. 23 A similar pattern was observed in our cohort, in which the effect of rurality became more evident after the first month. Previous studies such as23,24 have suggested that these differences may be related to variations in baseline health status, living alone, access to rehabilitation, follow-up care, levels of physical activity and social support networks. However, the underlying mechanisms remain unclear and warrant further investigation, particularly in distal femur fracture cohorts. It should also be noted these studies included patients aged 50 or older, younger than those considered older adults, which may limit the direct comparability with our findings.
Our results are consistent with Streubel et al, 12 who in their study compared native distal femur fractures with proximal femoral fractures; they found a similar behaviour of mortality rates in both groups, as observed in our present study. Similar findings were shown in large case series obtained from the Swedish Fracture Register. 25 A recent meta-analysis estimated a 30-day mortality of 8% and a one-year mortality of 26%. 26 In Spain, Merino-Rueda et al 27 reported a one-year mortality of 23% although they included surgically treated patients and non-surgically treated patients in the series. However, other studies have reported higher mortality rates of 38% at one year in distal femur fractures, reflecting the heterogeneity of the available literature. 28 When comparing our results, early (16.2%) and one-year (35.6%) mortality rates were higher than those reported in most previous studies, with the exception of Jordan et al, who described a one-year mortality of 38%. 28
Meyers et al 14 reported low mortality rates, although it may be taken into account that the population they included is patients older than 60 years. In our study, patients aged 65 years and older were included, as this threshold is widely used to define older adult populations; this group is characterized by increased vulnerability to adverse outcomes such as mortality and disability, as shown by Fried et al 29 This may limit comparability. These same authors relate the time of the surgery to its possible outcome in prognosis and survival. They concluded that a delay of more than two days after admission incurs a mortality increase.
In contrast, other comparative studies between distal and proximal femur fractures have reported longer time to surgery and higher mortality in distal fractures,13,27 findings that differ from those observed in our cohort, where time to surgery was not independently associated with mortality. These authors, in contrast with our findings, found longer times to surgery and a higher mortality in distal fractures.
Regarding baseline comorbidities, patients with distal femur fractures showed a significantly higher prevalence of renal comorbidity, particularly chronic kidney disease, which is consistent with the overall worse clinical profile observed in this group. In contrast, digestive comorbidity, mainly gastroesophageal reflux disease, was more frequent in patients with proximal femur fractures, although its clinical relevance in relation to survival outcomes appears limited. Postoperative renal complications were more frequent in the proximal fracture group.
Limitations
This study has several limitations that should be considered. First, its single-center design may limit the generalizability of the findings. Second, although multivariable analysis was performed, the possibility of residual confounding cannot be excluded. Relevant variables such as postoperative weight-bearing status, rehabilitation protocols, and discharge destination were not available, which may influence outcomes and limit the interpretation of differences between groups. Additionally, the heterogeneity of both proximal and distal femur fractures, including differences in fracture patterns and surgical management, was not fully captured in the analysis. The absence of a detailed classification system or stratified analysis may introduce bias and limits the ability to account for variability in treatment approaches and clinical complexity.
Additionally, the retrospective design of the study may introduce information bias, and some variables, particularly specific comorbidities and complications, had a low number of events, which may affect the robustness of these findings. The use of both ICD-9 and ICD-10 coding systems may introduce a potential risk of misclassification, although this was minimized through manual validation of clinical records.
Finally, although the study period spans years in which coding systems evolved, detailed harmonization procedures between classification systems were not specifically analyzed, which may represent a potential source of misclassification bias.
Generalisability
Regarding external validity, our study population reflects a real-world cohort of older adult patients undergoing surgical treatment for distal and femoral fractures in a tertiary care setting. However, the single-center design and the use of a historical reference cohort for proximal fractures may limit the generalizability of our findings to other settings or healthcare systems. Additionally, variations in surgical management and institutional practices should be considered when interpreting these results.
Conclusions
In conclusion, patients with distal femoral fractures showed higher mortality at short and mid-term follow-up compared with proximal femoral fractures, whereas no significant differences were observed at one year. However, this association was not maintained after multivariable adjustment, suggesting that fracture type itself may not be an independent predictor of mortality. Future studies should investigate in greater depth the influence of rurality, fracture pattern, and other unmeasured clinical and healthcare- related factors on survival outcomes following distal femoral fractures in older adults.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Clinical Documentation Unit of the University Healthcare Complex of Salamanca (CAUSA) for their valuable assistance in managing medical records and facilitating the data extraction process for this study.
Ethical Considerations
This study was approved by the Salamanca Research Ethics Committee (approval no. PI202001420; February 2020). All procedures were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Consent to Participate
Written informed consent was obtained from all participants before inclusion in the study.
Author contributions
Study concept and design: JFB. Acquisition of subjects and/or data: CdC, JMH, CP, AG. Methodology: DBB, JFB. Statistical and data analysis: DBB. Design of tables and figures: DBB. Interpretation of data: DBB, JFB. Writing of the document in its initial format: DBB, JFB, CdC. Writing of the final draft: DBB, JFB. Final approval of manuscript: all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are available from the corresponding author upon reasonable request.