
Abstract
Background
Postoperative constipation (POC) is common in older adults after hip fracture surgery and may be influenced by perioperative care and nutritional status. Serum albumin is an imperfect nutrition marker, whereas the Geriatric Nutritional Risk Index (GNRI) combines albumin with body weight and may better reflect nutritional reserve. The association between preoperative GNRI and POC after fixation of AO/OTA 31-A extracapsular hip fractures remains unclear. We evaluated the association of preoperative GNRI with POC and compared discrimination with other preoperative markers.
Methods
We conducted a single-center retrospective cohort study of patients aged ≥65 years undergoing proximal femoral nail fixation for AO/OTA 31-A extracapsular hip fractures. POC was defined as no spontaneous bowel movement for ≥3 postoperative days or laxative/enema use within 72 hours. Multivariable logistic regression adjusted for age, sex, BMI, diabetes, prior stroke/TIA, Parkinson’s disease, time to first mobilization (≥48 h), and total opioid dose (morphine-equivalent dose, MED). Discrimination was assessed using ROC AUC; analyses were complete-case.
Results
Among 230 patients, 152 (66%) developed POC. In the expanded model, higher GNRI was associated with lower odds of POC (adjusted OR 0.86 per 1-unit increase, 95% CI 0.81–0.91; P<0.001). Higher BMI (OR 1.18, 95% CI 1.05–1.33; P=0.005), mobilization ≥48 h (OR 2.43, 95% CI 1.22–4.83; P=0.011), and opioid exposure (OR 1.52, 95% CI 1.24–1.85; P<0.001) were associated with higher odds. Model AUC increased from 0.758 to 0.822 after adding perioperative factors. In single-marker ROC analyses, GNRI showed modest discrimination for POC (AUC 0.724, 95% CI 0.650–0.789), higher than serum albumin (AUC 0.689), BMI (AUC 0.539), and age (AUC 0.545).
Conclusions
POC was common after fixation of AO/OTA 31-A extracapsular hip fractures in older adults. Preoperative GNRI provided prognostic information, and perioperative variables further improved discrimination. GNRI may help identify patients who could benefit from proactive bowel management, opioid-sparing strategies, and early mobilization.
Introduction
Postoperative constipation (POC) is frequently encountered in older adults following hip fracture surgery, yet it often receives insufficient clinical attention. 1 This complication can cause considerable discomfort, delay mobilization, impair nutritional intake, and predispose patients to secondary problems such as delirium or respiratory infections. 2 Among perioperative factors, the influence of opioid analgesics is well recognized. By binding to peripheral μ-opioid receptors, these drugs slow intestinal transit and diminish the defecatory reflex; symptoms typically arise within the first three postoperative days.3,4
The likelihood of POC is also shaped by patient-related characteristics, including advanced age, limited mobility, and suboptimal nutritional status—all of which are common in geriatric orthopedic populations. 5 Older patients with hip fractures often present with reduced physiological reserve, acute inflammatory stress, poor oral intake, and impaired mobility before and after surgery. These factors may act together to reduce gastrointestinal motility and delay the recovery of normal bowel function. Therefore, identifying preoperative markers that reflect the patient’s nutritional and functional vulnerability may help clinicians recognize patients at increased risk before constipation becomes clinically apparent.
Although serum albumin is a traditional marker of nutrition, it is affected by inflammation, hydration status, and acute illness, and may not fully capture nutritional reserve in older surgical patients. To address these limitations, the Geriatric Nutritional Risk Index (GNRI) was introduced, integrating albumin levels with body weight relative to ideal values. 6 GNRI has demonstrated prognostic value for adverse outcomes such as infections, pressure ulcers, functional decline, and mortality in elderly cohorts.7,8 However, its relationship with gastrointestinal complications such as POC has yet to be clearly defined. Existing studies on constipation after hip fracture surgery have mainly focused on general clinical risk factors or postoperative care variables, whereas evidence regarding preoperative nutritional risk, particularly GNRI, 9 remains limited.
Previous studies on POC have generally grouped hip fractures into a single category, overlooking distinctions between intracapsular and extracapsular hip fractures in surgical management, anesthesia, 10 analgesic exposure, and rehabilitation pathways.9,10 AO/OTA 31-A extracapsular hip fractures are commonly treated with internal fixation using proximal femoral or cephalomedullary nails and may be followed by delayed mobilization, a factor that may heighten the risk of constipation.11,12 Limiting the study cohort to this subgroup can improve the uniformity of patient characteristics and strengthen the clinical relevance of findings.
In light of these considerations, the present study explores whether preoperative GNRI is associated with postoperative constipation in older adults undergoing fixation of AO/OTA 31-A extracapsular hip fractures, 13 while accounting for relevant perioperative confounding factors, including opioid exposure and delayed mobilization. We also compared the discriminatory performance of GNRI with routinely available preoperative markers, including serum albumin, BMI, and age. We postulate that lower GNRI scores, reflecting greater nutritional risk, correspond to an increased probability of developing POC in this setting.
Methods
This retrospective cohort study was conducted at a tertiary hospital between January 2022 and January 2025. The study was approved by the institutional ethics committee, and informed consent was waived due to the retrospective design and use of anonymized data. All research procedures adhered to the ethical standards of the institutional and national research committees, as well as to the principles of the Declaration of Helsinki (1964) and its later revisions. This study was reported in accordance with the STROBE statement, and the completed STROBE checklist is provided as Supplementary Material.
Inclusion and Exclusion Criteria
We retrospectively reviewed the records of consecutive patients aged ≥65 years who were admitted with an AO/OTA 31-A extracapsular hip fracture and underwent surgical fixation.
Inclusion criteria were as follows: 1. Radiographically confirmed unilateral AO/OTA 31-A extracapsular hip fracture, including 31-A1, 31-A2, or 31-A3 patterns. 2. Surgical fixation performed with a proximal femoral nail. 3. Availability of complete perioperative data, defined as serum albumin, body weight, and height measured within 48 hours before surgery, along with nursing documentation of bowel movements and analgesic use for at least the first 72 postoperative hours. In this study, the term “extracapsular hip fracture” refers specifically to AO/OTA 31-A fractures treated with proximal femoral nail fixation. Subtrochanteric fractures, femoral neck fractures, pathological fractures, and other extracapsular fracture patterns were not included.
Exclusion criteria were: 1. A pre-existing diagnosis of chronic constipation meeting Rome IV criteria or another gastrointestinal motility disorder. 2. Regular use of laxatives (more than three doses per week for ≥1 month before admission). 3. Pathological or periprosthetic hip fracture. 4. Multiple injuries with an Injury Severity Score >16 or a requirement for intensive care. 5. Death or discharge within 72 hours after surgery. 6. Missing key baseline data, including serum albumin, body weight, or height.
Data Collection
Demographic variables included age (years), sex, and body mass index (BMI, kg/m2). Comorbidities were extracted from the medical record. Parkinson’s disease, which may affect bowel motility, was recorded separately. Preoperative nutritional status was assessed within 48 hours before surgery by measuring serum albumin (g/L), body weight (kg), and height (cm), and calculating the Geriatric Nutritional Risk Index (GNRI).
Surgical variables included anesthesia type (spinal or general), operative duration (minutes), and estimated intraoperative blood loss (mL). All patients with AO/OTA 31-A extracapsular hip fractures underwent internal fixation with a proximal femoral nail, thereby minimizing variability in surgical method.
Postoperative variables included total opioid consumption within the first 72 hours, expressed as morphine-equivalent dose (MED); time to first mobilization (<48 or ≥48 hours); bowel function (spontaneous bowel movements within 72 hours and use of laxatives or enemas); and length of hospital stay (days).
Postoperative constipation (POC) was defined as the absence of spontaneous bowel movement for ≥3 consecutive days after surgery or the need for pharmacologic intervention (e.g., laxatives or enemas) within the first 72 hours postoperatively. Postoperative bowel function was assessed as part of routine nursing care, including documentation of spontaneous bowel movements and the use of rescue laxatives or enemas. No universal prophylactic laxative protocol was applied to all patients during the study period. Laxatives/enemas were recorded when used for treatment (rescue) rather than routine prophylaxis. Diagnosis was confirmed through review of nursing records and medication administration charts.
Statistical Analysis
Analyses were performed in IBM SPSS Statistics v26.0. Two-sided P < 0.05 was considered significant. Continuous variables were summarized as mean ± SD or median (IQR) and compared with the t test or Mann–Whitney U test as appropriate; categorical variables were expressed as n (%) and compared with the χ2 or Fisher’s exact test. Because this was a retrospective cohort study, all eligible patients treated during the study period were included, and no formal a priori sample size calculation was performed. The available sample included 230 patients with 152 POC events; with nine prespecified covariates in the expanded logistic regression model, the number of outcome events was considered acceptable for exploratory multivariable analysis.
Binary logistic regression was performed with GNRI modeled continuously, and effects were expressed per 1-unit increase. Covariates were specified a priori: age, sex, BMI, diabetes mellitus, prior stroke/TIA, Parkinson’s disease, total opioid dose (morphine-equivalent), and first mobilization ≥48 h. Multicollinearity among covariates was assessed using variance inflation factors (VIFs) and tolerance values, with VIF >5 or tolerance <0.20 considered indicative of potential multicollinearity. Results are reported as adjusted odds ratios (ORs) with 95% CIs. Model discrimination was assessed using the receiver operating characteristic area under the curve (ROC AUC). To avoid relying on discrimination alone, model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test and the Brier score. All analyses used complete cases.
Results
Baseline Characteristics by Postoperative Constipation Status
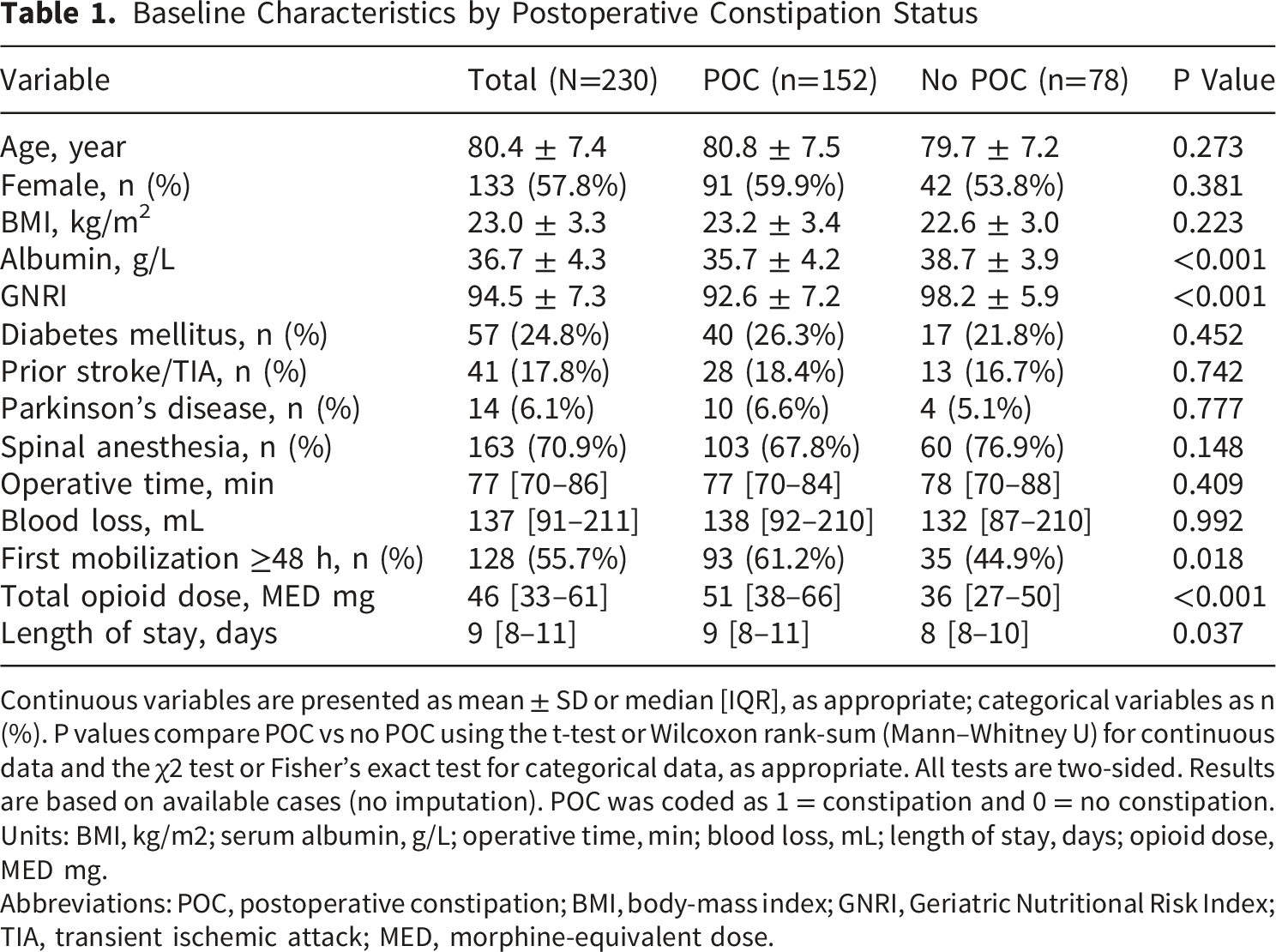
Continuous variables are presented as mean ± SD or median [IQR], as appropriate; categorical variables as n (%). P values compare POC vs no POC using the t-test or Wilcoxon rank-sum (Mann–Whitney U) for continuous data and the χ2 test or Fisher’s exact test for categorical data, as appropriate. All tests are two-sided. Results are based on available cases (no imputation). POC was coded as 1 = constipation and 0 = no constipation. Units: BMI, kg/m2; serum albumin, g/L; operative time, min; blood loss, mL; length of stay, days; opioid dose, MED mg.
Abbreviations: POC, postoperative constipation; BMI, body-mass index; GNRI, Geriatric Nutritional Risk Index; TIA, transient ischemic attack; MED, morphine-equivalent dose.
Multivariable Logistic Regression Analysis of Factors Associated With Postoperative Constipation
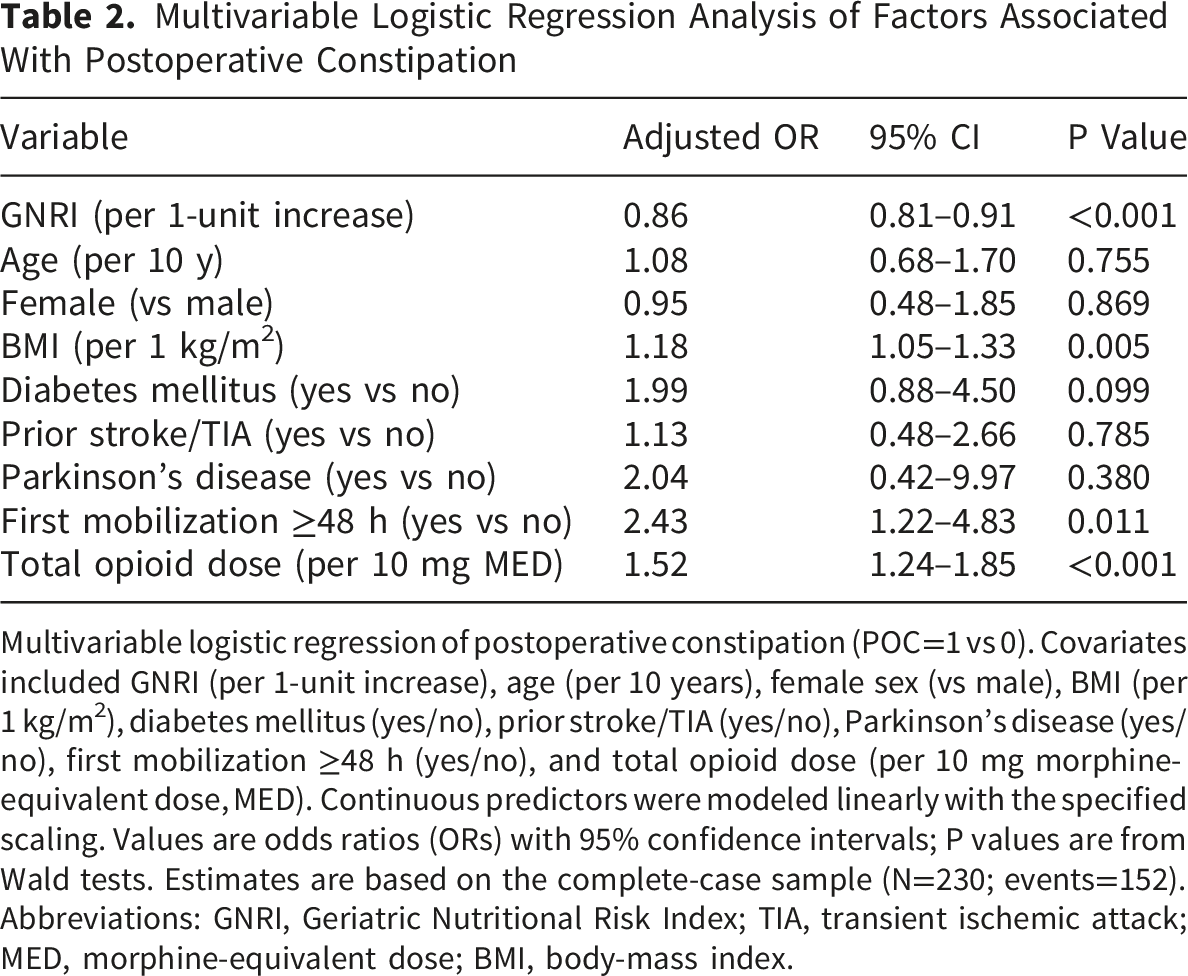
Multivariable logistic regression of postoperative constipation (POC=1 vs 0). Covariates included GNRI (per 1-unit increase), age (per 10 years), female sex (vs male), BMI (per 1 kg/m2), diabetes mellitus (yes/no), prior stroke/TIA (yes/no), Parkinson’s disease (yes/no), first mobilization ≥48 h (yes/no), and total opioid dose (per 10 mg morphine-equivalent dose, MED). Continuous predictors were modeled linearly with the specified scaling. Values are odds ratios (ORs) with 95% confidence intervals; P values are from Wald tests. Estimates are based on the complete-case sample (N=230; events=152). Abbreviations: GNRI, Geriatric Nutritional Risk Index; TIA, transient ischemic attack; MED, morphine-equivalent dose; BMI, body-mass index.
After accounting for baseline characteristics and comorbidities, lower GNRI, higher BMI, delayed mobilization (≥48 h), and greater opioid exposure were the principal correlates of postoperative constipation. The preoperative model showed moderate discrimination for POC (AUC 0.758), and discrimination improved after adding perioperative factors, including mobilization ≥48 h and opioid consumption, to the expanded model (AUC 0.822). These AUC values indicate risk-stratification performance rather than diagnostic certainty. For the expanded model, calibration assessment showed no evidence of poor model fit by the Hosmer–Lemeshow test (P = 0.668), and the Brier score was 0.159, indicating acceptable overall prediction error.
On the common complete-case subset (N=230, events=152), GNRI showed modest discrimination for postoperative constipation (AUC 0.724, 95% CI 0.650–0.789), which was numerically higher than serum albumin (AUC 0.689, 95% CI 0.617–0.755), BMI (AUC 0.539, 95% CI 0.461–0.617), and age (AUC 0.545, 95% CI 0.470–0.618). ROC curves for all four preoperative markers were constructed on the same individuals to ensure comparability (Figure 1). These findings suggest that GNRI may provide modest incremental risk-stratification information beyond serum albumin alone, but it should not be interpreted as a standalone diagnostic test for postoperative constipation. Receiver operating characteristic curves for GNRI, serum albumin, BMI, and age in discriminating postoperative constipation. AUC values were interpreted as measures of discrimination for risk stratification rather than as standalone diagnostic performance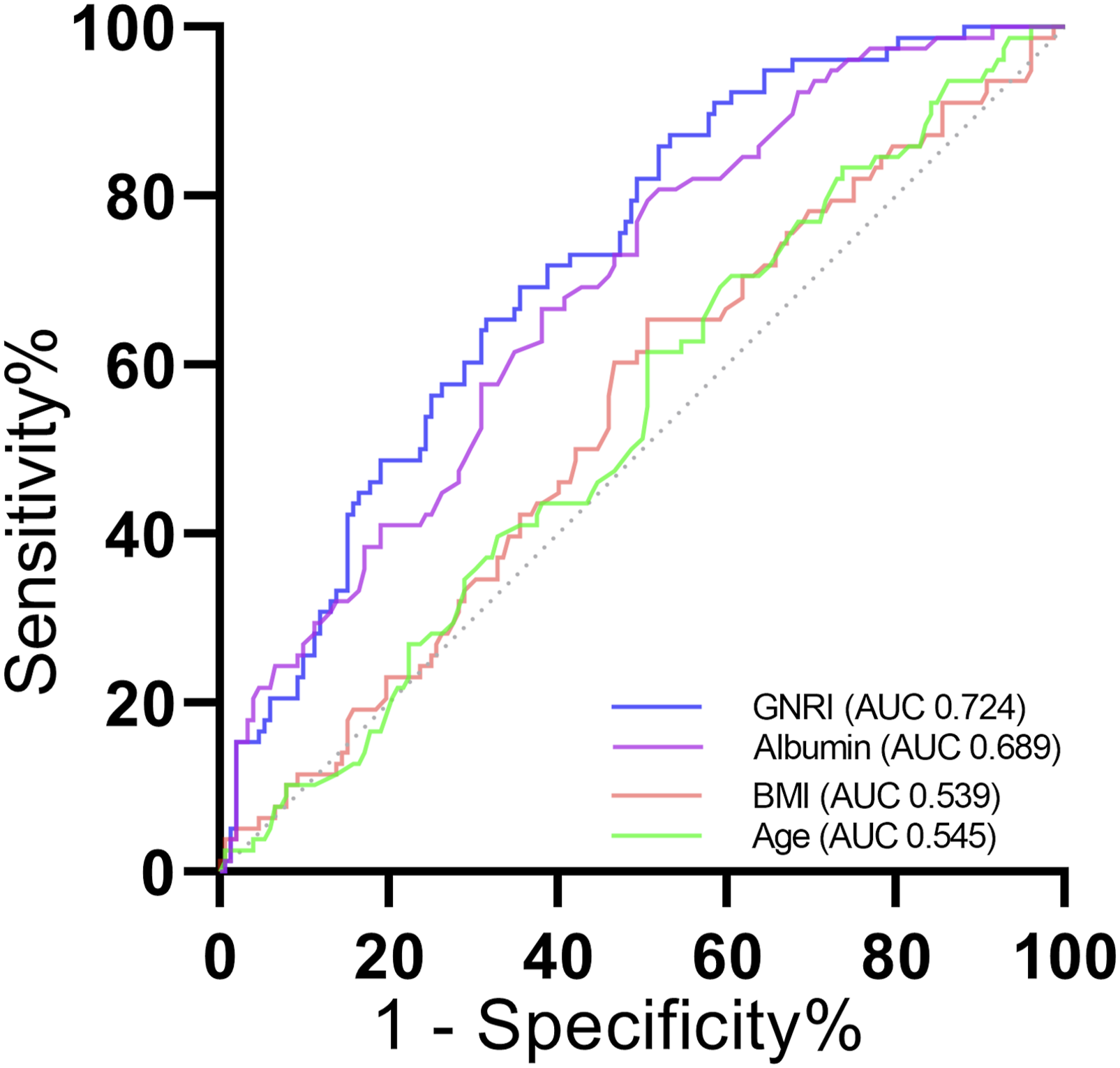
Discussion
In this cohort of older adults undergoing fixation of AO/OTA 31-A extracapsular hip fractures, postoperative constipation was common and appeared to reflect both baseline nutritional vulnerability and modifiable perioperative factors.13 Lower preoperative GNRI was independently associated with a higher risk of POC after adjustment for demographic characteristics, comorbidities, delayed mobilization, and opioid exposure. GNRI also showed modest but more favorable single-marker discrimination than serum albumin, BMI, or age, suggesting that a composite nutritional index may provide additional risk-stratification information beyond routinely available single measures. Importantly, delayed mobilization and greater opioid exposure were also associated with POC, highlighting potentially modifiable targets for perioperative bowel management.
Several studies have linked preoperative nutritional deficits to poorer postoperative recovery, including delayed gastrointestinal function and other complications.14-17 In this context, our data suggest that GNRI—a composite index—discriminates constipation risk better than serum albumin alone, likely because it captures both body mass and protein status rather than a single laboratory value. Differences in effect sizes across studies may reflect variation in patient mix, surgical approach, analgesic regimens, and mobilization practices, all of which can influence bowel motility. The associations we observed for higher opioid exposure and delayed mobilization align with opioid-related gastrointestinal hypomotility and with evidence supporting early ambulation in ERAS pathways.18-20 Taken together, these findings support the clinical plausibility of our results and highlight GNRI as a practical preoperative screening measure.
The association between lower GNRI and constipation is biologically plausible. Poor protein–energy reserves are linked to sarcopenia, reduced abdominal and pelvic floor strength, and slower colonic transit. 21 Hypoalbuminemia may also reflect systemic inflammation and fluid shifts that can impair enteric function. These factors may increase opioid requirements and delay mobilization, which could partially mediate the observed association.22,23 Importantly, GNRI remained associated with constipation after adjustment for opioid dose and time to first mobilization, suggesting that the relationship is not fully explained by perioperative management alone. GNRI was modeled as a continuous variable, and we observed no clear departure from linearity; therefore, effects are reported per 1-unit increase. Residual confounding (eg, dietary fiber intake, baseline bowel habits, or unmeasured frailty) cannot be excluded.
From a clinical standpoint, GNRI can serve as a quick preoperative screen to identify patients who may benefit from proactive bowel management. A pragmatic threshold based on ROC analysis could be used to trigger a standardized bundle—opioid-sparing analgesia, early ambulation targets, hydration and fiber optimization where feasible, and scheduled (rather than PRN) laxatives. Because GNRI is available before surgery, risk discussions and order sets can be prepared in advance, while the perioperative factors identified here (opioid dose and time to first mobilization) remain actionable during admission. In resource-limited settings, GNRI offers a low-cost approach to prioritizing enhanced recovery measures without additional testing, and implementation can be audited using routine metrics (eg, time to first walk and daily opioid totals). Discrimination improved after adding perioperative variables, suggesting that modifiable perioperative factors may add risk-stratification information. However, AUC alone does not establish clinical usefulness, and the model should be interpreted alongside calibration performance and validated in independent cohorts before clinical implementation.
This study has several limitations. First, it was a single-center, retrospective observational study with a relatively modest sample size and no formal a priori sample size calculation; therefore, causality cannot be inferred, statistical power for detecting weaker associations may have been limited, and residual confounding, such as baseline bowel habits and dietary factors, may remain despite adjustment. Second, POC was determined from routine clinical documentation and may be subject to misclassification. Third, analyses were complete-case; although the sample size (N=230; events=152) provided an acceptable number of outcome events for the prespecified expanded model, the findings should be interpreted as exploratory and may not be directly generalizable to other institutions, perioperative pathways, or patient populations. GNRI was modeled as a continuous predictor and appeared approximately linear on the log-odds scale; alternative functional forms produced similar results, but these analyses cannot substitute for external validation. Finally, discrimination was assessed in the derivation cohort, so some optimism is expected; calibration and clinical utility should be evaluated in independent and ideally prospective cohorts. Despite these limitations, the study included a clearly defined AO/OTA 31-A extracapsular hip fracture cohort treated with proximal femoral nail fixation, prespecified covariates with clinical rationale, and consistent findings across multivariable regression and single-marker ROC analyses.
Key next steps include external validation and implementation testing. Multicenter datasets should evaluate discrimination and calibration and assess whether performance is consistent across different analgesic and mobilization practices. Pragmatic studies could test whether using GNRI to trigger a simple perioperative bundle (opioid-sparing analgesia, early ambulation targets, and a scheduled bowel regimen) reduces constipation-related morbidity, rather than improving prediction metrics alone. Prespecified subgroup analyses (eg, age ≥80 years, fracture pattern, and anesthesia type) may help identify settings in which GNRI-guided pathways are most effective. Finally, reporting the full model equation would facilitate independent validation and prospective benchmarking.
Conclusions
Postoperative constipation was common in this cohort of older adults undergoing AO/OTA 31-A extracapsular hip fracture fixation. Higher preoperative GNRI was independently associated with lower odds of constipation, and adding perioperative variables (opioid exposure and time to first mobilization) improved discrimination beyond a preoperative model. Together, these findings suggest that GNRI may be a useful preoperative screening tool and highlight opioid stewardship and early mobilization as modifiable targets to reduce risk.
Supplemental Material
Supplemental Material - Preoperative GNRI Predicts Postoperative Constipation after Fixation of Extracapsular Hip Fractures in Older Adults
Supplemental Material for Preoperative GNRI Predicts Postoperative Constipation after Fixation of Extracapsular Hip Fractures in Older Adults by Lan Guo, Youwei Tian, Ying Liu, Yanan Fu, Zhanbei Ma and Chong Nan in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Ethical Considerations
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Baoding No.1 Central Hospital (Approval No. [2024]105).
Consent to Participate
The requirement for informed consent to participate was waived by the Ethics Committee due to the retrospective design and use of de-identified data.
Author Contributions
Lan Guo: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft. Youwei Tian: Investigation, Data curation, Writing – review and editing. Ying Liu: Validation, Visualization, Writing – review and editing. Yanan Fu: Investigation, Data curation, Writing – review and editing. Zhanbei Ma: Resources, Investigation, Writing – review and editing. Chong Nan: Conceptualization, Supervision, Methodology, Writing – review and editing, Project administration, Funding acquisition. All authors critically revised the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the S&T Program of Baoding (2441ZF051).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.